
Abstract
Soft tissue management in lower limb poses a considerable challenge to a reconstructive plastic surgeon. Perforator-based propeller flaps can cover large wounds without sacrificing a major vascular axis and allows reconstruction using nearby similar tissues, thereby following the principle of replace like with like. This study was undertaken with the objective to look for the results of propeller flap in lower limb reconstruction and how the results can be improved. This was a retrospective study on 40 patients who underwent the reconstruction of soft tissue defects of lower limb with propeller flap. All the relevant data were collected and analyzed. Patients with soft tissue defect anywhere in the leg were included, but patients who had history of degloving injury, peripheral vascular disease, and diabetes mellitus were excluded. All these patients were divided in 2 groups according to the angle of rotation of propeller flap. Group I had 20 patients in which the flap was rotated by 150° to 180°. Group II had 20 patients, and the flap was rotated by 90° to 150°. Postoperatively, the first 2 cases in Group I showed total flap congestion and had complete necrosis, which were debrided and an alternate method was used to reconstruct. Thereafter, no patient had total flap necrosis. Minor complications were seen in 3 patients who showed transient venous congestion of the flap. Group II had no flap necrosis except for mild dehiscence, which was managed by secondary suturing. In most cases, the aesthetic result was acceptable and patients were completely satisfied. When parameters of the defect are suitable for treatment with a propeller-based local flap, this technique may be considered as the first option for surgical reconstruction. Proper planning, location of perforator with preoperative and intraoperative audio Doppler, and use of magnification would make this procedure more successful and definitely decrease the use of long-duration microvascular surgery.
Introduction
Soft tissue defect in the lower limb has always been known to present a difficult reconstructive challenge to the plastic surgeon. The principles of surgical management of lower extremity soft tissue defects, in the last few years, have changed with the introduction of new models of local flaps. Since the innovative work by Koshima and Soeda, 1 improvements in anatomical knowledge on cutaneous, subcutaneous, and intramuscular vessels originating from major vascular axis of the lower limbs have allowed development of various types of perforator flaps, which are commonly being used in clinical practice these days.2-4
According to the Gent consensus 2003, perforator flaps are constituted by cutaneous and subcutaneous tissue areas nourished by perforator arterial branches originating from major vascular axis with an intramuscular (musculocutaneous perforator flap) or intraseptal (septocutaneous perforator flap) course. The Tokyo consensus 5 2011 on propeller flaps defines a perforator propeller flap as “a perforator flap with a skin island made of two paddles, one larger and one smaller, separated by the nourishing perforating vessel that corresponds to the pivot point.”
Taylor et al 6 , based on their experimental studies, gave the angiosome concept and reported that a single perforator may safely supply its proper angiosome and up to half of the adjacent perforator vascular territory. This theory is favored by vascular adoption directed toward the periphery that occurs by means of increased vascular pressure in the perforator artery after ligature of collateral subcutaneous and intramuscular arterial branches.6,7
Perforator-based propeller flaps are safe and reliable and represent an important step forward in reconstructive plastic surgery of the lower limb. Whenever possible, surgical intervention and donor-site morbidity ought to be limited to a single body region, and the use of propeller perforator flaps can concretely widen options for lower limb defects reconstructive. 8
In this study, we assessed the planning, advantages, and complications of propeller flaps and also evaluated the donor site morbidity and methods to improve the success rates of this procedure. We also aimed to determine if the outcome between the 2 groups was affected by the angle of rotation and present a rather simplified operative technique.
Materials and Methods
This was a retrospective study on 40 patients who presented to the Department of Plastic Surgery with soft tissue defects of leg. All these patients had reconstruction of the defect with a propeller flap. Appropriate data were collected and analyzed. Patient inclusion criteria were the following:
Patients with soft tissue defect anywhere in leg
Post-injury, post-infective debridement, or post-contracture release defects
Post-burn defects, especially deep electric burn
Nonhealing ulcers
Implant-exposed wounds or post-dehiscence wounds
Exclusion criteria were the following:
Patients who had history of degloving injury
Patients with critical limb ischemia: prior ischemic changes in the distal extremity with ankle-brachial index <0.4
Patients who are known cases of peripheral vascular disease and have underwent any procedure such as chemical or lumbar sympathectomy
Diabetes mellitus
The flaps were planned using planning in reverse method and perforators were located by audio Doppler in all cases preoperatively. All these patients were divided in 2 groups according to the angle of rotation of propeller flap. Group I had 20 patients in which the flap was rotated by 150° to 180°. Group II also had 20 patients and in this group the flap was rotated by 90° to 150°.
Operative Technique
Surgery mostly was performed by the qualified plastic surgeons with at least 3 years of experience in plastic surgery, with the patient under spinal anesthesia. General anesthesia was used only when indicated. Preoperative localization of the nearest perforator was done by hand-held audio Doppler with the help of 8 MHz transducer. The dimensions of the flaps were drawn after debridement of the defect and localization of appropriate perforator(s) from the adjacent healthy and non-degloved skin. The shape of the flaps was according to that of the created defect. In group I, the long axis of the flap was orientated along the long axis of the limb so that the resultant flap is oriented 150° to 180° to the defect. To the distance between the perforator and the distal edge of the defect 1 to 2 cm are added, and the resulting value is transposed proximally to the skin, which will cover the defect, ensuring the flap’s comfortable inset, without any tension on the pedicle. Similarly, to the width of the defect is added 0.5 to 1 cm to allow the closure without tension. Group II had planning according to the degrees of rotation. In group II, the perforators were located near or distal to the distal margin of the defect so that the rotation is around 90° to 150° approximately. In our few initial cases we also marked the alternate pedicled flap, which was considered as plan “B,” if somehow the perforator is not seen or injured inadvertently during the dissection.
To start with, only one edge of the future flap is incised, which was common to both plans “A” and “B.” The incision was made up to the deep fascia and is followed by subfascial dissection under loupe magnification, and all the identified perforators are preserved and the peri-perforator area was dissected to increase the mobility of the vessels.
All throughout dissection, the perforators were humidified with lidocaine to prevent spasm. We prefer using lidocaine 15% spray, which was directly instilled over the perforator. If 2 adjacent perforators with same characteristics are found, we kept both of them until the flap’s dissection is completed and the tourniquet released. Then, after alternative clamping and repeated checking of vascularity of the flap, it was possible to ligate one of them. Once the best perforator is chosen, the definitive design of the flap was accomplished according to its location, size, suitability to sustain the flap, number of venae commitantes, course, and orientation.
Then, after enlarging the perforator foramen using a longitudinal fascial incision, the chosen perforator is cleared retrograde, of all muscular branches and fascial strands for at least 2 cm, but no longer than needed for optimal flap’s rotation. Now, the incision around the flap and harvesting was completed, and the flap was rotated into defect for final insetting.
The donor site was closed without tension, to prevent reduction of the flap’s blood supply by compressing the source vessel, and also can induce swelling of the distal leg. If primary closure was not possible, the donor site was grafted with split thickness skin graft and bolster dressing applied.
The flap was examined every 2 hours on the day of operation, and if any doubt was there, then scratching was done with 23-gauge needle to look for the oozing of blood. If there was dark blood then a few sutures were removed to relieve the tension, and if the flap was still found to be congested then it was derotated for 1 day. The next day vascularity was examined and again the flap was rotated back into the defect.
Results
This retrospective study was conducted on 40 patients operated between January 2014 and December 2016 in the Department of Plastic Surgery (Figures 1-4).
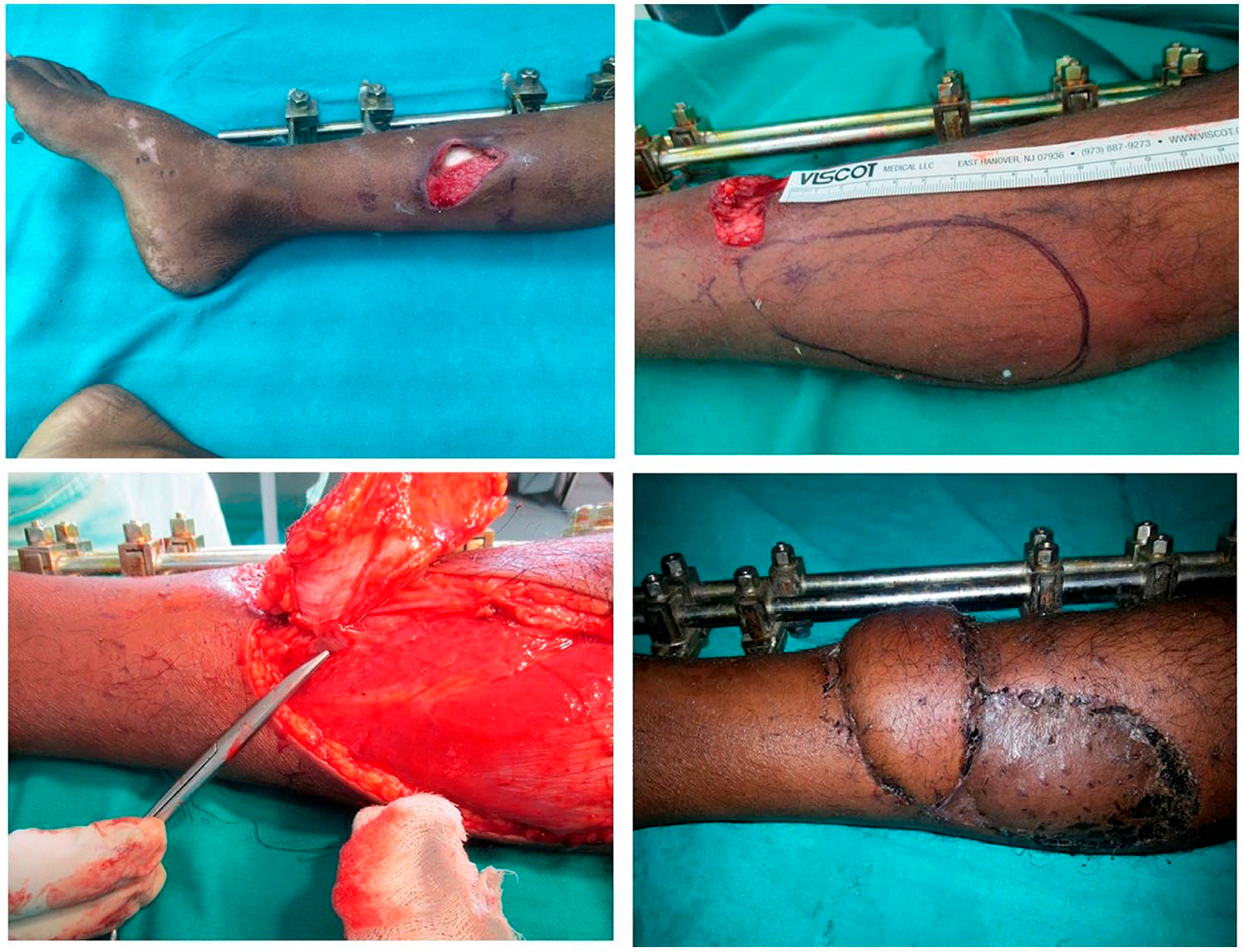
Propeller flap based on posterior tibial vessels and rotated by 90°. (Top left) Posttraumatic defect with exposed tibia and external fixator applied for reduction of tibial fracture. (Top right) Propeller based on posterior tibial vessels marked and perforator located with audio Doppler. (Bottom left) Propeller based on posterior tibial vessels raised with perforator vessels pointed out by scissors. (Bottom right) Postoperative photograph after stitch removal (14th day).

Propeller flap based on posterior tibial vessels and rotated by 90°. (Top left) Posttraumatic defect with exposed tibia. (Top right) Propeller based on posterior tibial vessels raised. (Bottom left) Immediate intraoperative picture showing flap inset over the defect and donor area covered with STSG. (Bottom right) One month postoperative photograph showing good flap and excellent graft take on donor area.

Propeller flap based on posterior tibial vessels and rotated by 90°. (Top left) Post electric contact burn defect with exposed tibia. (Top right) Propeller based on posterior tibial vessels being raised with vessel loop around the vessels. (Bottom left) Intraoperative picture showing flap being inserted over the defect, which was created after debridement of dead exposed bone. (Bottom right) One month postoperative photograph showing good flap and excellent graft take on donor area.

Propeller flap based on posterior tibial vessels and rotated by 180°. (Top left) Defect over the tibia after excision of Marjolin’s ulcer. (Top right) Propeller based on posterior tibial vessels raised. (Bottom left) Immediate intraoperative picture showing flap inset over the defect and donor area covered with STSG. (Bottom right) One month postoperative photograph.
Age and Sex Distribution
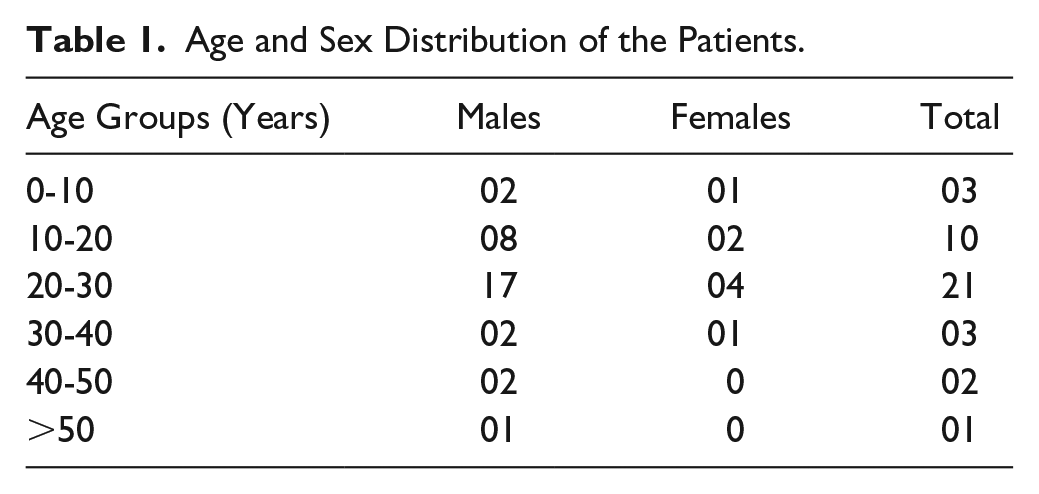
The mean age of patients in this study was 25.4 (11.47) years. Most of the patients were in the age group of 20 to 30 years. The youngest patient was 8 years old, while the oldest patient was 60 years old. Males accounted for 32 (80%) patients and the females for 8 (20%) of the study population (Table 1). This data were comparable between the 2 groups.
Age and Sex Distribution of the Patients.
Etiological Distribution
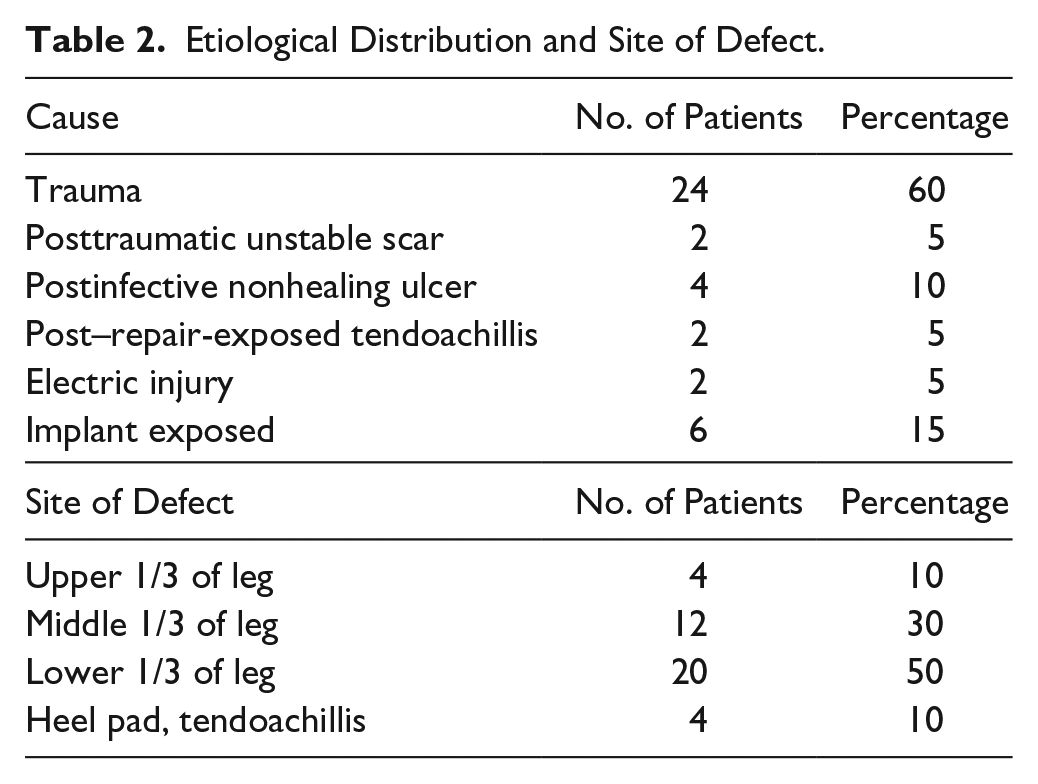
Trauma was the most common cause of injury in 24 (60%) patients. This was followed by postinfective nonhealing ulcer accounting for 15%. Other group comprised posttraumatic unstable scar and post–repair-exposed tendoachillis with 2 patients (5%) each. Electrical injury was responsible in 2 (5%) patients. Implant-exposed wound was present in 6 patients (Table 2). There was no significant difference between the 2 groups regarding the etiological distribution.
Etiological Distribution and Site of Defect.
Timing of Operation After Injury
Eight patients (20%) were operated within 1 week after sustaining injury, while 22 patients (55%) were operated between 1 and 2 weeks. Four (10%) patients were operated between 2 and 3 weeks after sustaining injury and 6 (15%) patients were operated after 3weeks of sustaining injury due to late reporting in our department after getting discharged from other departments (Table 2).
Site of Defect in the Leg, Angle of Flap Rotation, and Size of Wound and Their Corresponding Flaps
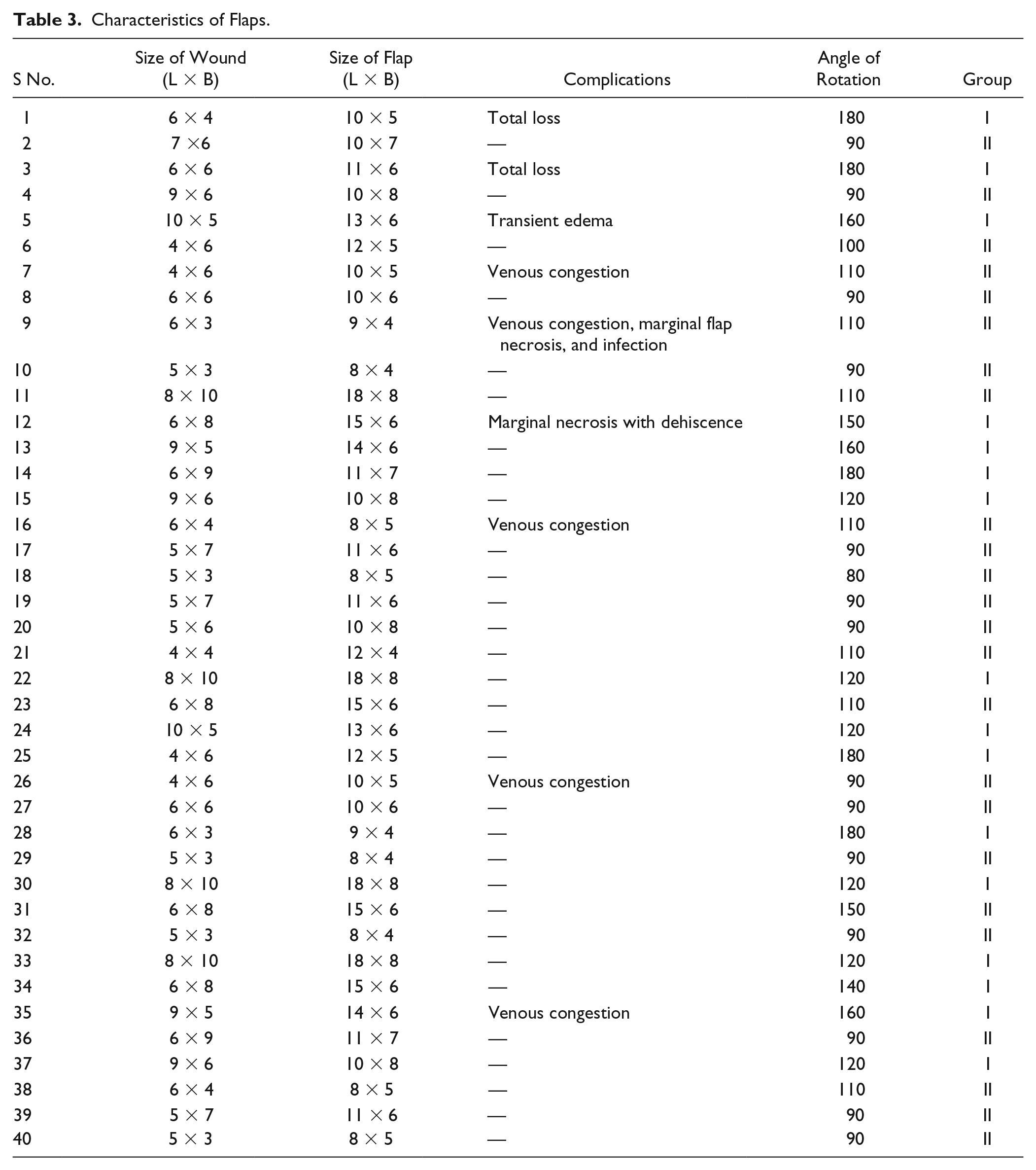
Lower 1/3 leg defect was the most common area and it comprised 20 (50%) of the patients. Twelve (30%) patients were with middle 1/3 leg defect. Four (10%) patients had defect over the upper 1/3 of leg. Four patients (20%) had injury in tendoachillis and heel pad region. Group I had 20 patients in which flap was rotated by 150° to 180°. Group II also had 20 patients and the flap was rotated by 90° to 150° (Table 3). Maximum size of the flap in our study was 18 cm × 8 cm and smallest flap was of size 8 cm × 4 cm (Table 3).
Characteristics of Flaps.
Main Artery Giving Perforator
The most common artery giving perforators was posterior tibial artery, giving perforator in 26 patients (65%). Other arteries were anterior tibial, peroneal artery, and medial sural artery, 6 (15%), 4 (10%), and 4 (10%), respectively. Peroneal artery and posterior tibial artery perforator-based flaps were mostly used for lower leg coverage. Medial sural artery perforators were used for planning flap for upper third of leg.
Complications
Overall complication rate was 10% (4/40) in our study. The most common complication in our study was venous congestion, comprising 5 patients. Venous congestion was reversed after careful postoperative leg elevation. Partial flap necrosis, wound infection, and transient edema were seen in 2 patients only (one in each group). Two patients (5%) needed another flap procedure after total flap loss (in group I). The complication rates were higher in group I as compared with group II (Tables 3 and 4). The differences were not statistically significant once we take all types of complications (major and minor necrosis). There were no gross donor site morbidity except for marginal graft loss, which healed by dressings only. In 3 cases, donor site was closed primarily. All the patients had no specific complaints regarding the donor area.
Comparison of Outcome and Complications Between the 2 Groups.
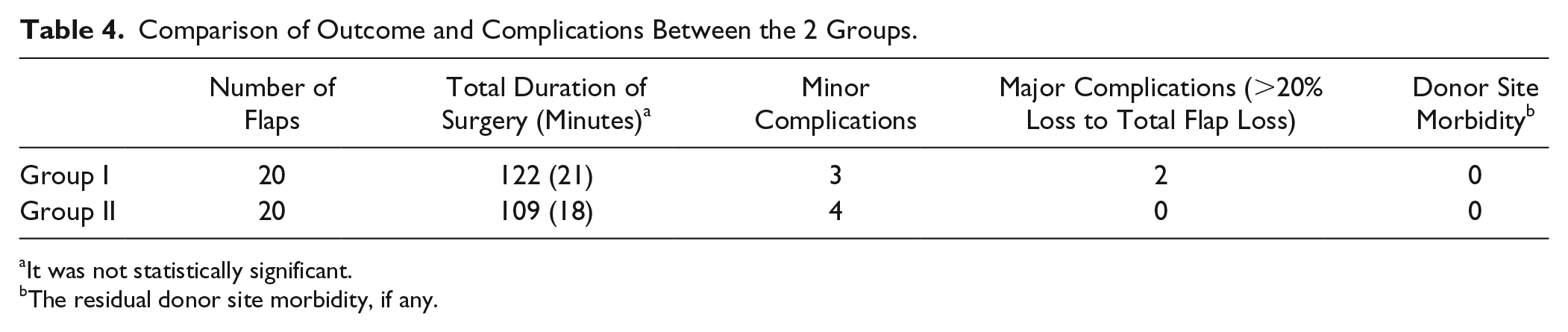
It was not statistically significant.
The residual donor site morbidity, if any.
Discussion
The reconstruction of complex distal extremity defect is quite challenging with both cosmetic and functional considerations. The basic principle in lower extremity reconstruction is utilization of the simplest option and should replace like with like tissue, minimize the morbidity of the donor site, preserve the main vascular axis, and reduce operating and hospitalization time. The propeller flaps in the last few years has gained great popularity for soft tissue defect reconstruction of different parts of the body, and surgical technique has been refined from time to time by several authors. Perforator propeller flaps are based on a reliable vascular pedicle and can undergo wide mobilization and rotation. They allow for an ample freedom in design and choice of the donor site, based on the quality and volume of soft tissue required and on scar orientation and hence they are very versatile. The development of perforator-based propeller flaps in reconstructive surgery has been helped by improved knowledge of the vascular basis of flap perfusion and anatomical studies on lower limb vascular supply provided the basis for local perforator flap design in treating lower limb defect.2,3,9 The propeller flap as a model of local perforator flap was first described by Hyakusoku et al 10 for the treatment of periarticular skin retractions around the elbow secondary to burn injury. In this the flap was harvested around a cutaneous perforator arterial branch by twisting the vascular pedicle and rotating the skin paddle like a propeller up to a maximum of 180° angle. These flaps are particularly suitable for complicated soft tissue defects of the lower third of the leg, foot, heel, and ankle, where local flap options have previously not been available. The flap may be rotated for up to 180°, and the distal perforators in particular can be used for coverage of defects. 11
The subdermic vascular network is rich and allows the elevation of thin skin flaps. One single perforator vessel located may support a large skin area because of the opening of potential vascular territories, which vascularizes the peripheral border of the flap. The process of vascular adaptation is promoted by the increase of blood flow pressure, which occurs in the perforator artery after interruption of subcutaneous and intramuscular branches during flap harvesting.
Many authors pointed out the utility of these flaps in covering medial and lateral malleolar areas and of the heel and tendoachillis region with several advantages:
As they are tissue adjacent to the defect they have similar skin texture and color to the injury zone.
As microvascular anastomosis is not needed the operation time is shorter than a microsurgical transfer.
The surgical intervention can be performed under a regional anesthesia.
Rotation and hence transfer is quite tailor made in comparison to pedicled flaps, which produces dogears or are interpolated.
Over the last few years, several clinical studies reported on the application and results of perforator-based propeller local flaps in lower-limb reconstruction.12-16 Masia et al 8 did reconstruction with propeller flaps in 35 of 59 patients operated on with perforator flaps for defects related to oncological surgery, trauma, and unstable scars. They reported 4 flap losses and observed partial necrosis with secondary healing in 4 propeller flaps performed in heavy smokers (3) or diabetic (1) patients. We noticed 2 total flap losses, which needed another local transposition flap, and 2 marginal flap losses, which healed after debridement and dressings. These were our first 2 cases where the flaps were rotated by 180°. We were hesitant to skeletonize the vascular pedicle and perhaps it led to kinking of vessels during rotation. From then onward the vessels were meticulously dissected and freed to ease the rotation and prevent kinking. In a study by Jakubietz et al, 12 they treated 8 patients with defects in the malleolar region with 90° to 180° propeller flaps based on perforators from the tibial and peroneal vessels. Our range of angle of rotation was from 90° to 180°.
The main limitations of our study were that the sample size was small and it involved various heterogeneous sites. In our experience, perforator-based propeller flaps fulfilled the preoperative expectations. All patients had good healing, and no further surgical procedure was required except for local transposition flaps in 2 patients. In most cases, the aesthetic result was very good and majority of the patients were fully satisfied. The favorable results reported in the literature, as well as the results of our personal experience for lower limb reconstruction, are encouraging. We believe that when the characteristics of the defect are suitable for treatment with a propeller-based local flap, this technique should be regarded as one of the possible reconstructive options.
Conclusions
Perforator-based propeller flaps are safe and reliable and represent an important step forward in reconstructive plastic surgery of the lower limb, especially leg. Perforator flaps are aesthetically better as the donor is from the adjacent area, donor site morbidity is minimized, less time is taken for flap harvest as compared with free flaps, less blood loss in comparison with other options, procedure requires only spinal anesthesia as opposed to general anesthesia in free flap surgery (good option in non–tertiary care centers), decreased hospital stay, and does not require sophisticated monitoring devices after the flap is transferred to the recipient area. The only drawback is that the raising of these flaps requires a certain amount of skill, which in time most surgeons are able to master.
The use of propeller perforator flaps can concretely widen the reconstructive options for lower limb defects. These flaps are particularly reliable in the distal leg and at the ankle region where the defects are often small but difficult to treat by means of other local flaps and there is presence of robust perforators.
Research Data
dataset for A Study of Clinical Applications of Perforator-Based Propeller Flaps in Leg Reconstructive Surgery: A Single-Center Experience of 40 Cases
dataset for A Study of Clinical Applications of Perforator-Based Propeller Flaps in Leg Reconstructive Surgery: A Single-Center Experience of 40 Cases by Shahab Faria Shahabuddin and Mohammed Fahud Khurram in The International Journal of Lower Extremity Wounds
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent was obtained from all individual participants included in the study.