
Abstract
Several wound classification systems are used to assess diabetic foot wounds. The recommendations for their use depend on the authors and foot associations. In this study, we compared Saint Elian score system, WIfI classification and Texas in 101 patients with foot wounds, and we followed them for a median of 149 days, finding differences both in the assigned risk and in the association with major amputation and wound healing. Saint Elian and WIfI scores match when Saint Elian is low or high risk but not when it is moderate. WIfI stages correlate with major amputation and wound healing. Saint Elian III correlates with major amputation. Prevalence of major amputations was 41% for WIfI 4 and 83% for Saint Elian III. WIfI 1 and 2 and Saint Elian I had a rate of wound healing of 80% to 85%. Stages 1 and 2 of WIfI score behave similar with regard to wound healing, 82% and 80% (P = .71), and major amputation, 0% and 10% (P = .68). Stages I and II of Saint Elian have the same rates of major amputation, 0% and 8% (P = .66), but not of wound healing, 85% and 51% (P < .05). The optimal cut point for detecting major amputation in Saint Elian is 18, with a sensitivity of 90.9 and specificity of 84.9, but there is no recommended cut point for wound healing. These classifications are validated for their use in diabetic foot wounds and to assess amputation risk, helping physicians make decisions and talk to the patients about prognosis.
Introduction
Several wound classification systems have been proposed to describe diabetic foot wounds, and there are different recommendations about their use depending on the authors, the foot societies, and the countries. Actually, clinicians, surgeons, and nurses from different countries discuss what the best classification system for diabetic foot ulcers is. Some authors suggest that a clinically relevant classification has to be easy to use, reproducible, and effective to communicate the extent of the foot lesion and perhaps the prognosis. It should also be applicable for investigation, education, and communication between all care providers and the multidisciplinary team. 1 Others think that the more easy to use the classification, the less details it gives about the wound and the less accurate for the prognosis and evolution is. 2
There are various classifications used among countries. One of the oldest is Wagner, which uses 6 grades in classifying foot ulcers. It has been widely used in several investigations and in clinical practice for years. It neither takes into account peripheral vascular disease as an independent risk factor for amputation nor assesses adequately the severity of infection. 1
This classification considers vascular perfusion only when gangrenous changes appear and infection when osteomyelitis is present. This makes it useless to evaluate ischemia or infection grade as independent risk factors for amputation. However, an increase in the severity score of Wagner classification correlates with the increase in the amputation risk. 3
Texas University classification is about a 4 × 4 table, with 16 cells and 4 grades and 4 stages. It takes into account ischemia, infection (but not its grade), and extent of the ulcer. It predicts outcomes and is validated, although some authors consider it difficult to apply in clinical practice because of its complexity. 1 It does not consider the presence of gangrene, 4 which increases the risk for amputation in different studies, although the patients who had infection and/or ischemia had higher rates of amputation,3,5 making the classification useful for predicting outcomes. It does not consider infection severity.
Extension, infection, perfusion, depth, and neuropathy are components of PEDIS classification system, but some authors consider this classification difficult to use in clinical practice because of its complexity. 1 PEDIS system has been validated as a set of predictors of lower extremity amputation. 2
In 2010, an article was published presenting a new classification named Saint Elian Wound Score System, based on a score that takes into account different aspects of the wound. This score categorizes the patient in 3 grades: low risk of amputation with high probability of cicatrization when the score is less than 10 (Grade I), moderate risk that threatens part of the foot between 11 and 20 (Grade II), and high risk of major amputation for patients with more than 21 points (Grade III). 1 The presence of ischemia, more than one affected zone, area (size), and neuropathy were predictors of major amputations. This classification has external validation. 6 One of its benefits relates to the possibility of reclassifying the lesions, allowing the physician to make decisions based on the good or bad results after the first treatment, reevaluating and correcting the therapy as needed to improve outcomes. 7
Fontaine and Rutherford classifications should not be applied for patients with diabetes and do not take into account wound characteristics nor infection grade. 8 Infectious Diseases Society of America (IDSA) classification 9 does not take into account ischemia or other aspects of the lesions. Saint Elian, PEDIS, and Texas address ischemia, infection, and wound size, but exclude gangrene from the analysis. 4
Wound, Ischemia and foot Infection (WIfI) classification 4 is based on 3 prognostic factors that affect clinical management and amputation risk. These factors are as follows: wounds, that are stratified or graded from grade 0 to 3, based on size, depth, and severity; ischemia, graded considering ankle brachial index (ABI) or toe brachial index and infection, which score is based on IDSA classification. 9 This new classification is intended to permit more meaningful analysis of outcomes for various forms of therapy for the diabetic foot and to create a guide with prognostic value that correlates with the natural history and risk of amputation, being useful to make decisions about the patients’ treatment, in particular those of revascularization. However, WIfI is not enough to make acute decisions about the treatment only by itself, because there are more factors that affect the progress of the lesions, including the comorbidities, the clinical condition of the patient, and so on.
Current recommendations about using classifications vary based on the societies, the countries, the availability of procedures, and so on. The objective of this study was to determine whether the patients with diabetic foot categorized by Texas, WIfI, and San Elian scores had same risk for major amputation and if they correlated with outcomes after a follow-up period.
Experimental Section
This is a prospective observational analytic study.
Patients older than 18 years who consulted at Hospital Nacional Profesor Alejandro Posadas Diabetic Foot Unit for the first time for the diabetic foot lesion that was going to be studied (new lesion) between January 1, 2019, and September 1, 2019, were enrolled in a prospective database designed to track wound and patients characteristics. Patients with broad dorsal wounds that impeded making procedures for measuring ABI or those who had been hospitalized and discharged for that lesion were excluded.
Measures of ABI and 3 classifications (Saint Elian, Texas, and WIfI) were performed for each patient. ABI was measured with a portable duplex ultrasound Contec with an 8 MHz probe. Saint Elian classification was calculated according to the Saint Elian score, 1 Texas using the corresponding 4 × 4 table, 5 and WIfI calculated by the mobile application SVS. The toe brachial index or transcutaneous oxygen pressure was not used to calculate WIfI score because of the lack of that technology. Patients were treated by a multidisciplinary team in a tertiary care hospital that includes clinician diabetologist physician, a vascular surgeon, an orthopedist surgeon, a physiatrist, an infectologist, podiatrist, and nurse. Patients were treated ambulatory or hospitalized depending on the severity of the wound according to the recommendations of international guidelines for diabetic foot management from different societies (D-foot international 10 , IDSA guidelines 9 and Nice guidelines 11 ). If the wound was clinically infected, microbiological cultures were taken and empirical antibiotic therapy was initiated guided by local germs. If the patient had severe ischemia, the medical team ordered angiography and revascularization that was carried out in the same hospital. Decisions on major or minor amputation were taken by the team guided by international guidelines and clinical judgement. Wound cleansing was carried out using physiological solution or water for noninfected wounds and chlorhexidine 4% if they required antisepsis. Surgical or chemical debridement was performed as needed, and collagenase, hydrogel, and alginate were used. Wound dressings were used when available. Patients were followed-up in further consultation until February 2020.
Statistical Analysis
Categorical variables are presented as absolute values and percentage. Continuous variables are presented as median and standard deviation. For comparison between categorical variables, χ2 was used, and for continuous variables, median comparisons were performed with Student’s test for normal distribution and Mann-Whitney test for asymmetrical distribution. Kruskal-Wallis test was used to determine if there were differences between 2 or more groups of an independent variable on a continuous or ordinal dependent variable. Infostat, MedCalc, SPSS, and VCCstat were used for the statistical analysis. Significance was considered as P < .05. Values for χ2 with Yates correction or the Fisher’s exact test with 2 × 2 tables and of variance ratios for natural and treatment analysis of variance were calculated.
Results
One hundred one patients were included in the study. Median age was 59.2 years (29-92 years), and 27% were female. Eighty-nine percent had type 2 diabetes. From 101 patients initially included for descriptive analysis, 4 (3.9%) were excluded from outcome analysis because one of them finally had a melanoma and the other 3 were lost to follow-up. Then, outcomes of 97 patients were analyzed from the initial cohort. Patients were followed-up for a median of a 139-day period.
Description and Comparison of Classifications
Distribution of Patients by Saint Elian, WIfI, and Texas Scores
When Saint Elian classification was used, 12.9% (95% confidence interval [CI] = 7.3-21.4) of patients were in category I (likely successful wound healing, mild), 80.2% (95% CI = 71.1-87.5) in category II (condition with partial foot threatening) and 6.9 % (95% CI = 2.81-13.77) in category III (limb and life-threatening condition). Most patients (n = 52, 51.5%; 95% CI = 41.4-61.5) were classified as grade 3 of Texas score because they had a wound that penetrated bone, with infection, ischemia, or both. Distribution of patients by Saint Elian, WIfI, and Texas classification systems are described in Figure 1.
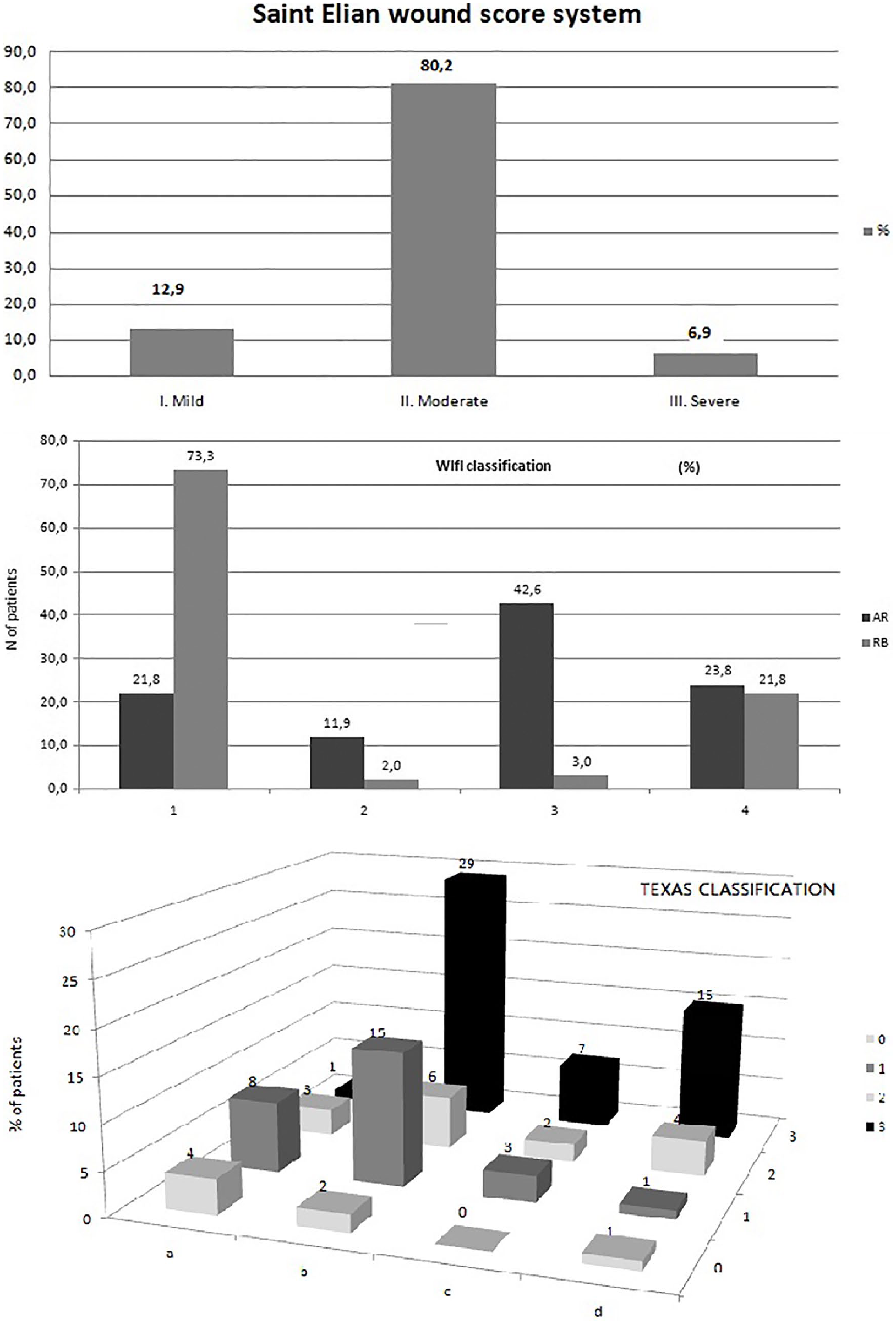
Distribution of patients by the 3 scores: (a) Distribution of patients by Saint Elian Wound Score System. I = mild: likely successful wound healing; II = moderate: condition with partial foot threatening; III = severe: limb and life-threatening condition. (b) Proportion of patients in stages of Wound, Ischemia and foot Infection (WIfI) classification system by AR (amputation risk) and RB (revascularization benefit). 1= very low AR/very low RB; 2= low AR/low RB; 3= moderate AR/moderate RB; 4= high AR/high RB. (c) Distribution of patients by Texas Classification.
Comparison Between Classifications
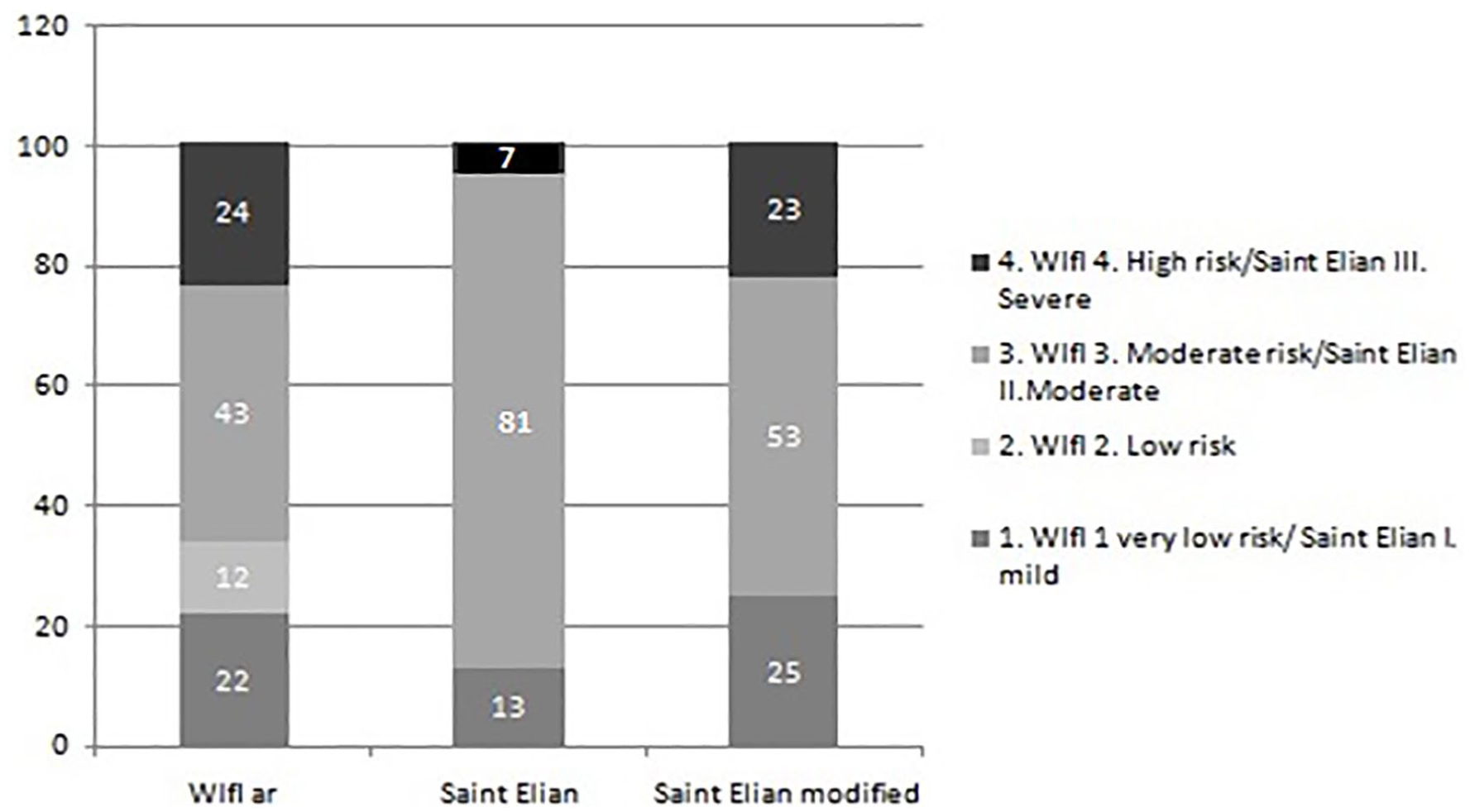
For high-risk categories, Saint Elian category III (severe) accounted for 7 patients (6.9%) and WIfI 4 for 24 patients (23.7%), P < .001.
For low-risk patients, Saint Elian described 13 patients (12.9%) and WIfI 34 patients (33.7%) taking into account low and very low risk (P < .01).
From all patients classified as category 4 of WIfI classification system (high amputation risk), 70.8% (n = 17) were classified as moderate (II) and 29.1% (n = 7) as severe (III) in Saint Elian score. Lowering the cut point of Saint Elian score for III Severe Category to include more patients with high risk for WIfI score implies that more patients with lower categories for WIfI (2 and 3) are categorized as Severe in Saint Elian score. Otherwise, when the patient had a lesion classified as Saint Elian III (severe), it corresponded to WIfI 4 score in 100% of cases (Table 1 and Figures 2 and 3).
Number of Patients in WIfI Amputation Risk Stages 1 to 4 That Would Be Included in Category III of Saint Elian Score (Severe) if Cut Point Lowers for High-Risk Patients.
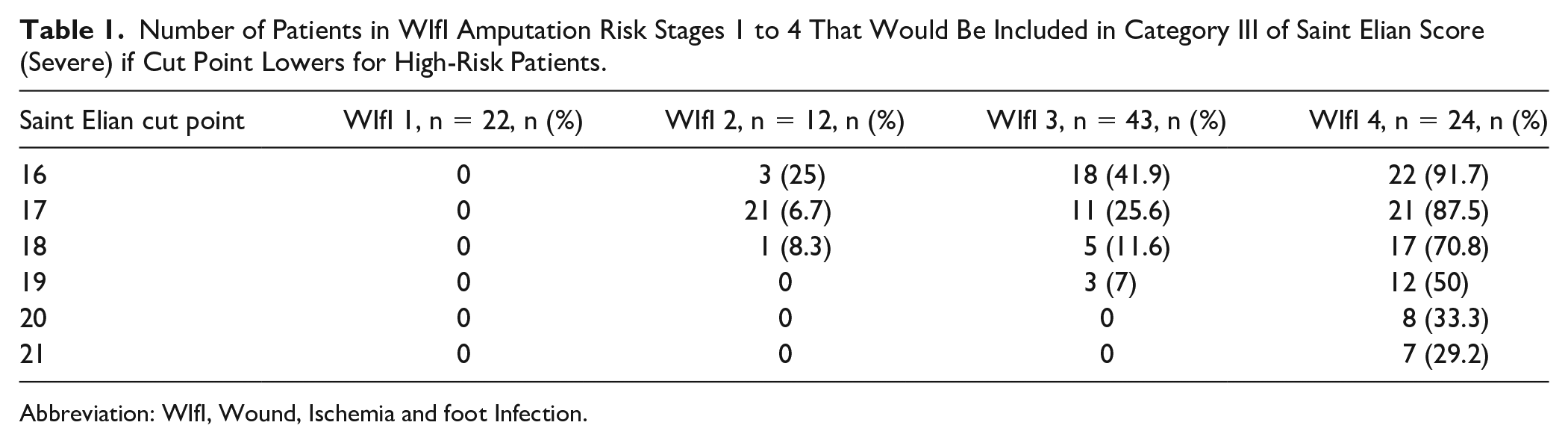
Abbreviation: WIfI, Wound, Ischemia and foot Infection.
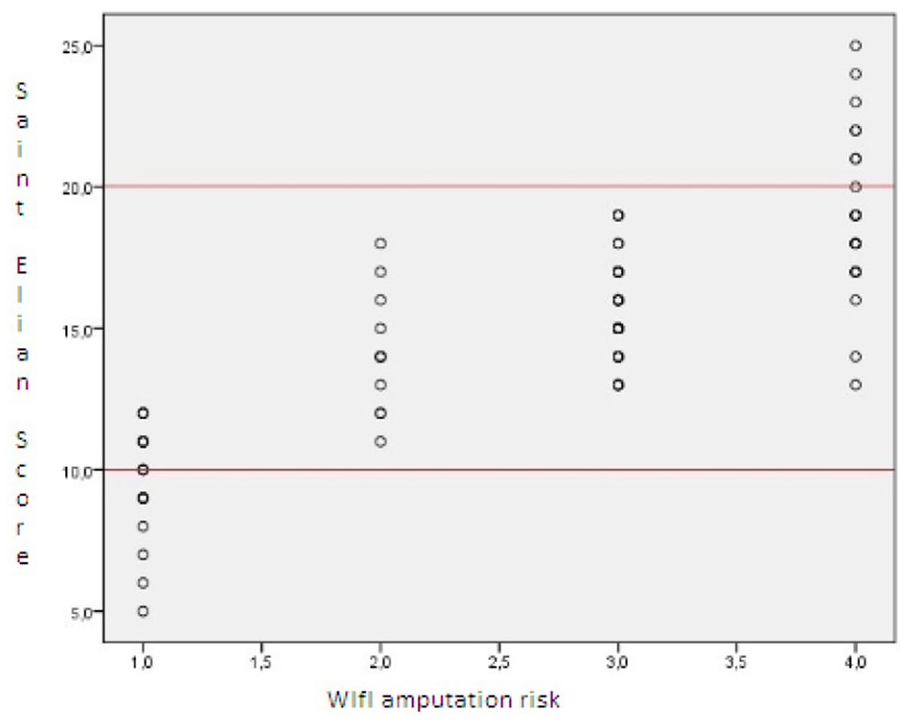
Distribution of patients classified by Saint Elian in relation to Wound, Ischemia and foot Infection (WIfI) score.
Distribution of patients by Wound, Ischemia and foot Infection (WIfI) amputation risk and Saint Elian Wound Score System (number of patients). In the third column is shown the distribution of patients by Saint Elian score system if cut point changes to ≤12 for mild and ≥18 for severe category.
All patients with low to moderate risk in WIfI score (2 and 3) are included in the grade II (moderate) of Saint Elian score system (Figures 2 and 3).
Patients with low risk for Saint Elian score (I) were classified as WIfI 1 (very low amputation risk) in 100% of cases. From all the patients in WIfI 1 category, 59.1% were in the lowest risk category or Saint Elian score I and the rest (40.9%) in the moderate category II. For low-risk patients, if the cut point of Saint Elian score had been 12 instead of 10, all patients in WIfI 1 category should have met the criteria for Saint Elian I (mild; Table 2 and Figure 3).
Number of Patients With WIfI Amputation Risk Stages 1 to 4 That Would Be Included in Category 1 of Saint Elian Score if the Cut Point for Low Risk Rises.
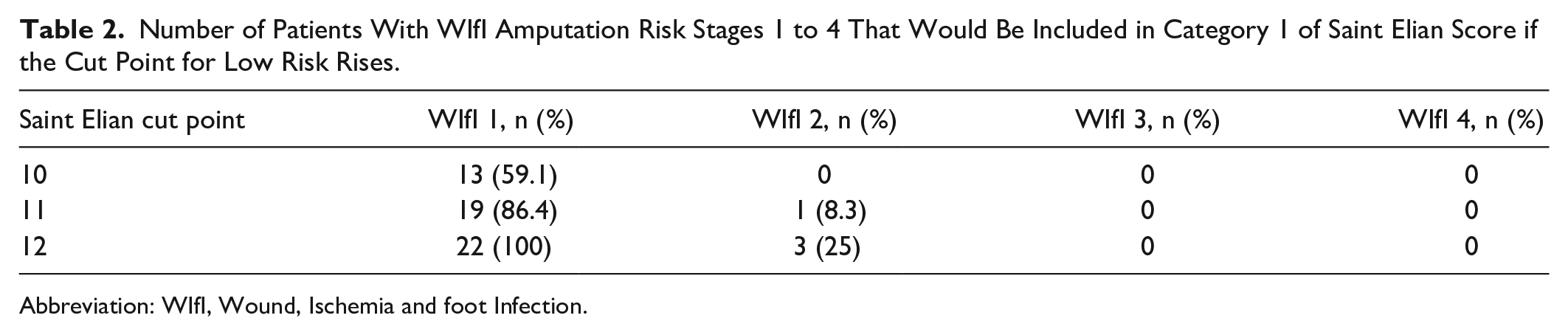
Abbreviation: WIfI, Wound, Ischemia and foot Infection.
When comparing Texas and Saint Elian Score System, there was a linear increasing tendency for Saint Elian Score related to Texas amputation risk (Figure 4).
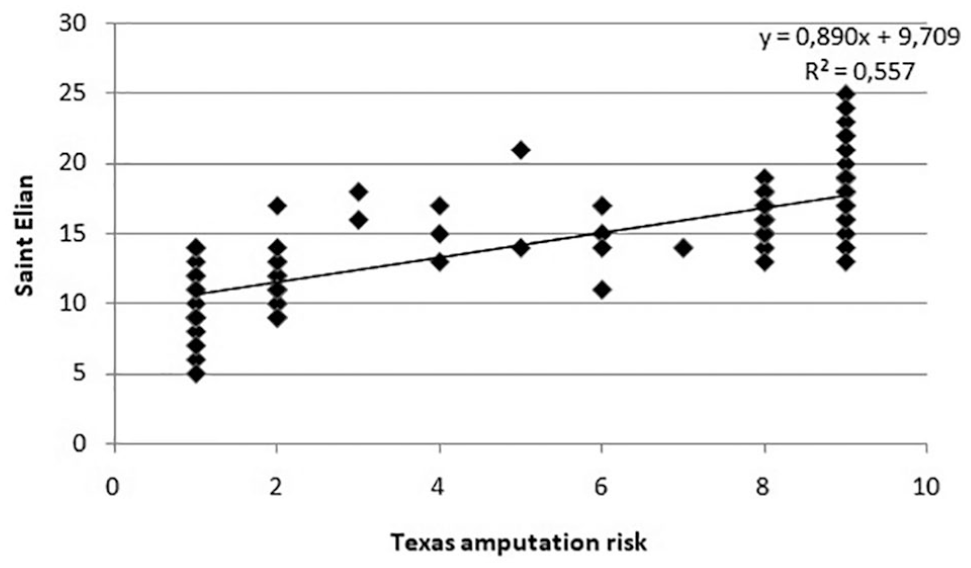
Saint Elian score related to Texas risk amputation. For this comparison, the amputation risk table published in the original article of Texas University classification 5 was categorized by risk from 1 (0% risk) to 9 (100% risk).
Outcomes
After a median follow-up of 149 days, 97 patients were analyzed from the initial cohort. Eleven patients (11.3%; 95% CI = 5.8-19.4) had a major amputation; 52 patients (53.6%; 95% CI = 43.1-63.8) had a complete wound healing; and 34 (35.1%; 95% CI = 25.6-45.4) had a persistent open wound at the time of the last visit. Median follow-up period was 145, 165, and 122 days for the patients with each outcome. Thirteen patients (13.4%; 95% CI = 7.3-21.9) required a minor amputation.
Patients who underwent a major amputation had a lower ABI than the other patients, with a median of 0, compared with patients with complete healing (median of 1.17) and patients with persistent open wounds (median of 1.10), P < .01. ABI was lower for Saint Elian III patients (a median of 0, compared with 1.10 and 1.13 for Saint Elian I and II, respectively), P < 0.01, and for WIfI 4 (0.17, significantly lower than 1.20 for WIfI 1, 0.57 for WIfI 2, and 0.61 for WIfI 3), P < .001.
The final evolution of patients is described in Table 3 (for WIfI and Saint Elian) and Table 4 (for Texas).
Outcomes Related to Both WIfI and Saint Elian Classification a .
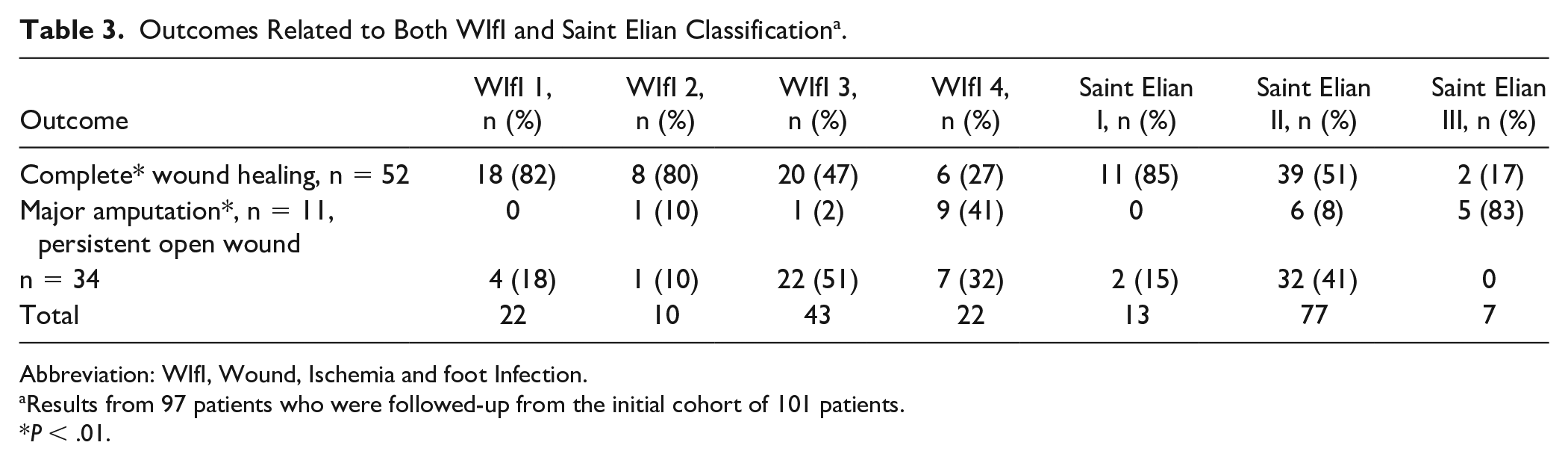
Abbreviation: WIfI, Wound, Ischemia and foot Infection.
Results from 97 patients who were followed-up from the initial cohort of 101 patients.
P < .01.
Outcomes Related to Texas Classification a .
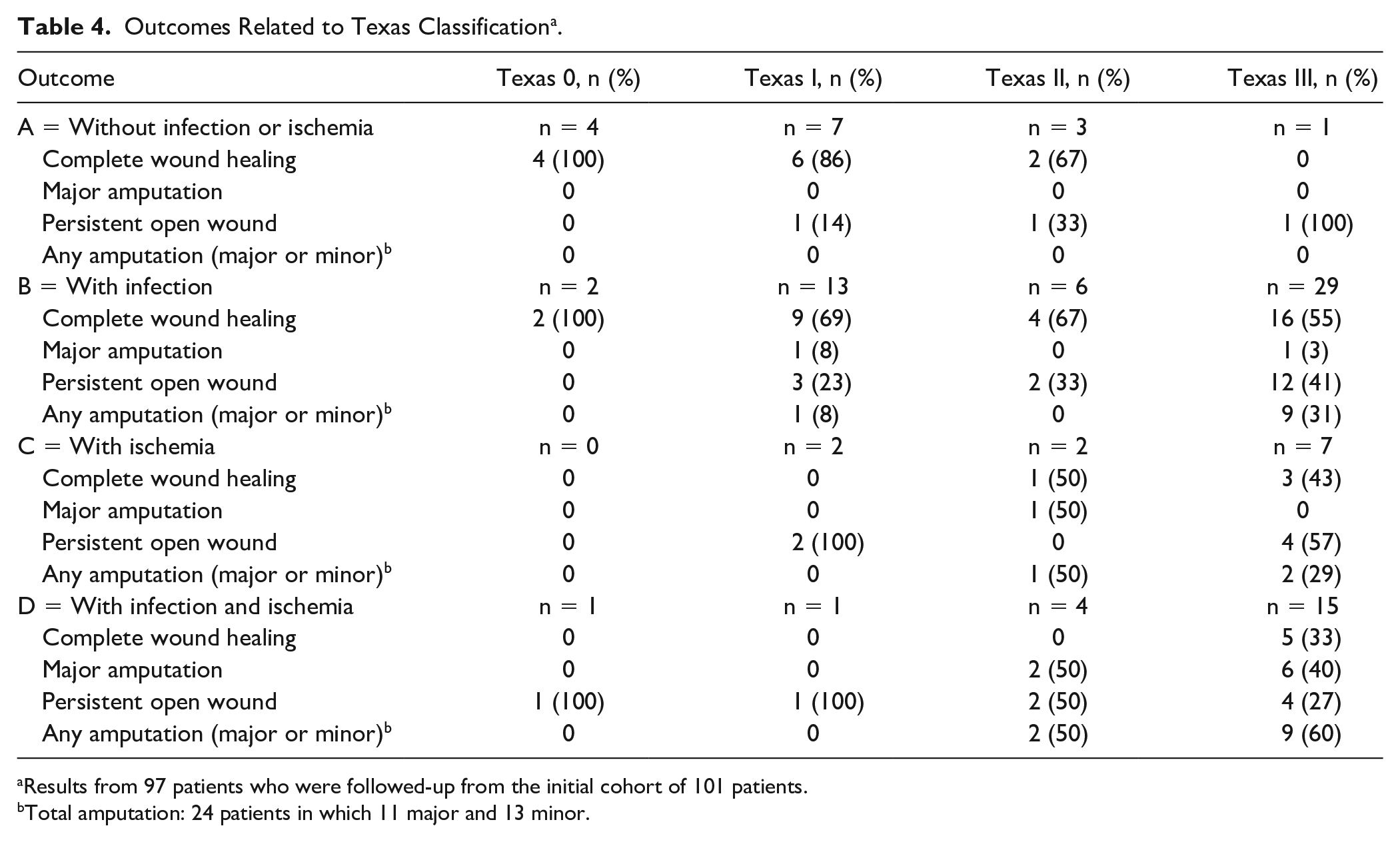
Results from 97 patients who were followed-up from the initial cohort of 101 patients.
Total amputation: 24 patients in which 11 major and 13 minor.
Kaplan-Meier survival curves for major amputation and wound healing for WIfI and Saint Elian classifications are shown in Figures 5 and 6. Patients who had their wounds classified as WIfI 4 and Saint Elian III had higher rates of major amputations than the other patients (P < .01) and lower rates of wound healing, statistically different for WIfI (P < .01) but not for Saint Elian (P = .32). The rate of wound healing was similar for WIfI 1 and 2, 82% and 80%, respectively (P = .71), and so was the rate of major amputation, 0% and 10% (P = .68). This was not true for Saint Elian I and II, which had no significant difference in major amputation rate (0% and 8%,s respectively; P = .66) but had significantly different rates for wound healing, 85% and 51%, respectively (P < .05). Saint Elian I had higher rates of wound healing than the other categories (P = .03).
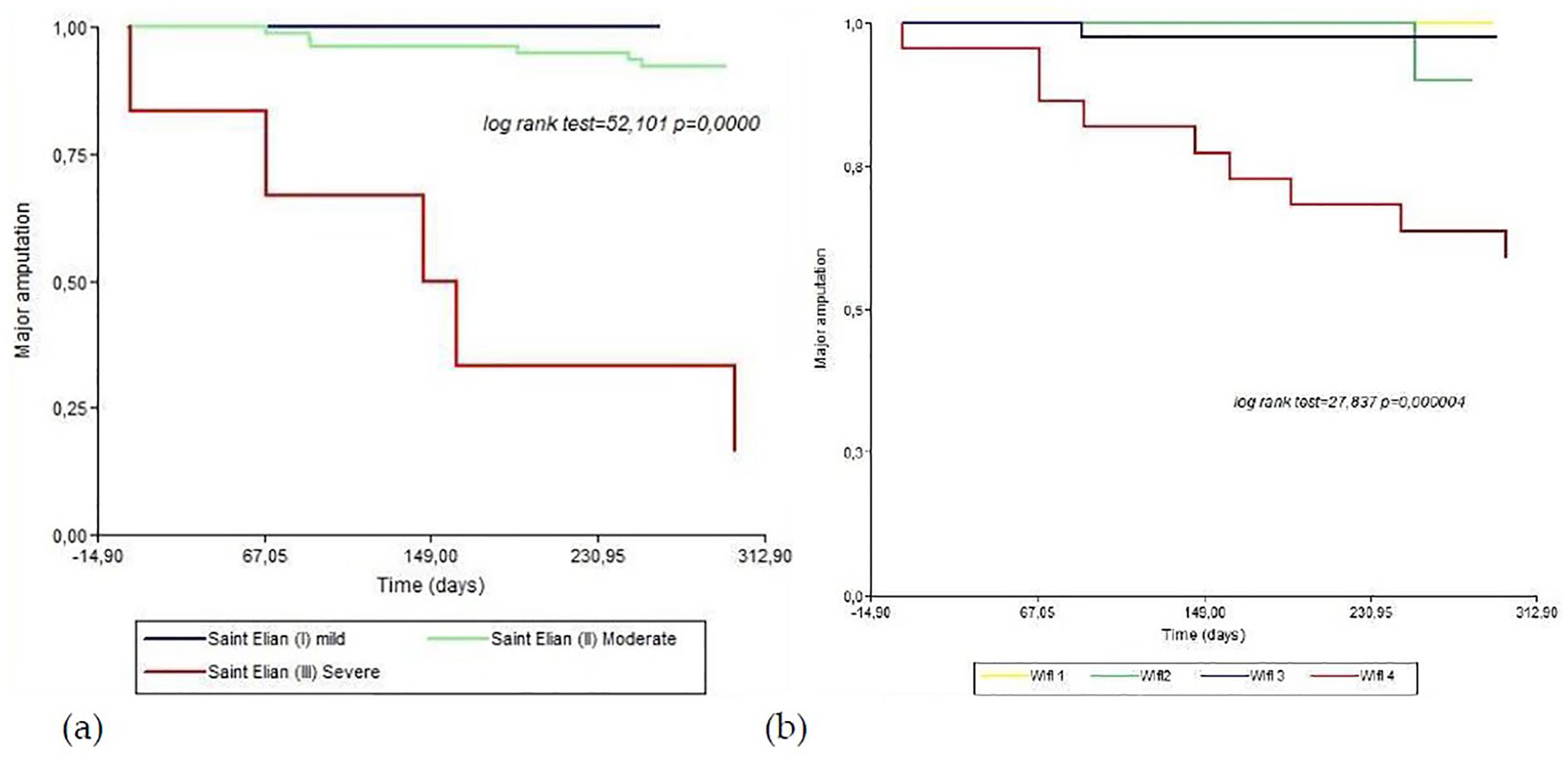
Kaplan-Meier survival curves for major amputation for Saint Elian score (a) and Wound, Ischemia and foot Infection (WIfI) score (b).
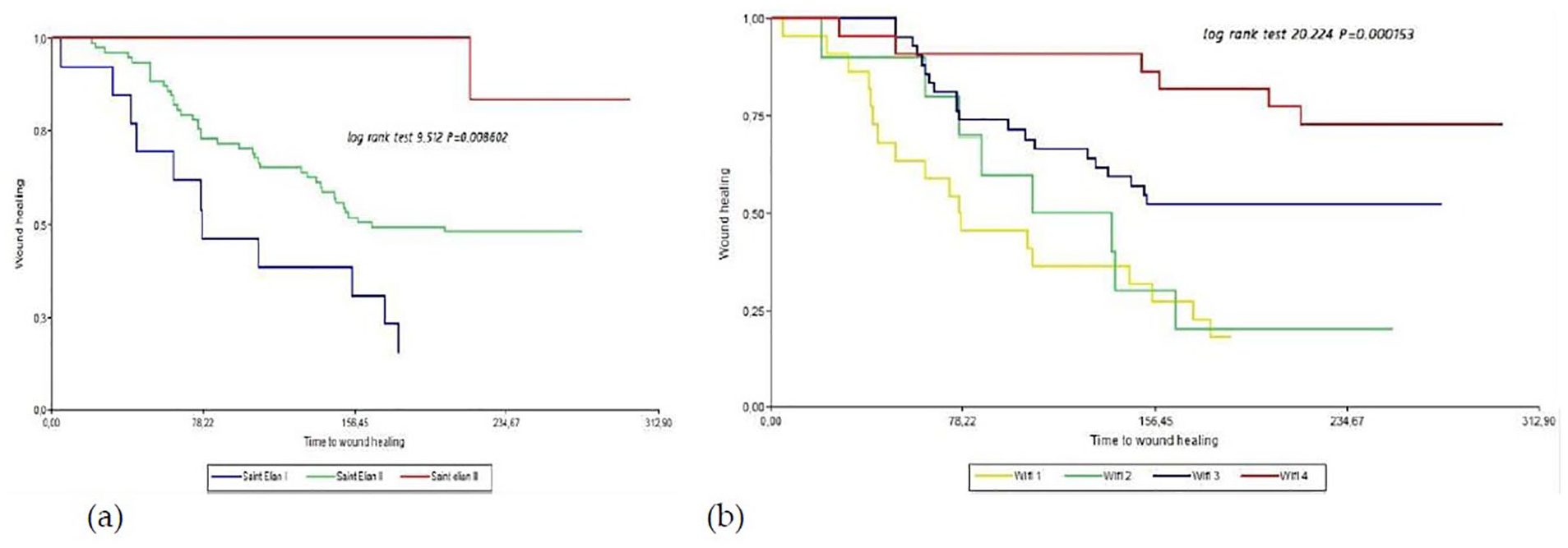
Kaplan-Meier survival curves for wound healing for Saint Elian score (a) and Wound, Ischemia and foot Infection (WIfI) score (b).
Receiver operating characteristic curve for Saint Elian score shows that the cut point with the best sensitivity and specificity for major amputation is higher than 17.5 with 90.9% and 84.9%, respectively (Figure 7 and Table 5).
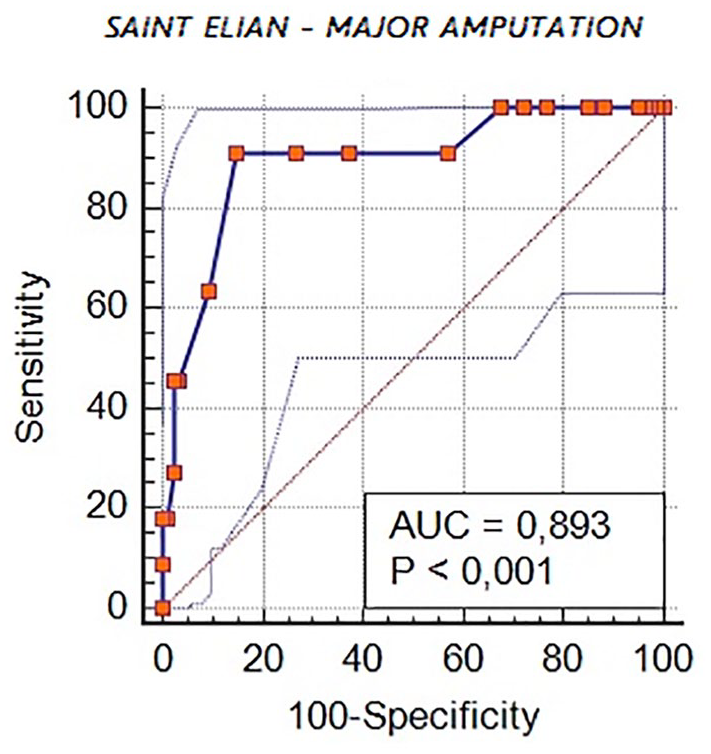
Receiver operating characteristic curve for major amputation in Saint Elian Score.
Sensitivity and Specificity for Major Amputation for Different Cut Points in Saint Elian Score.
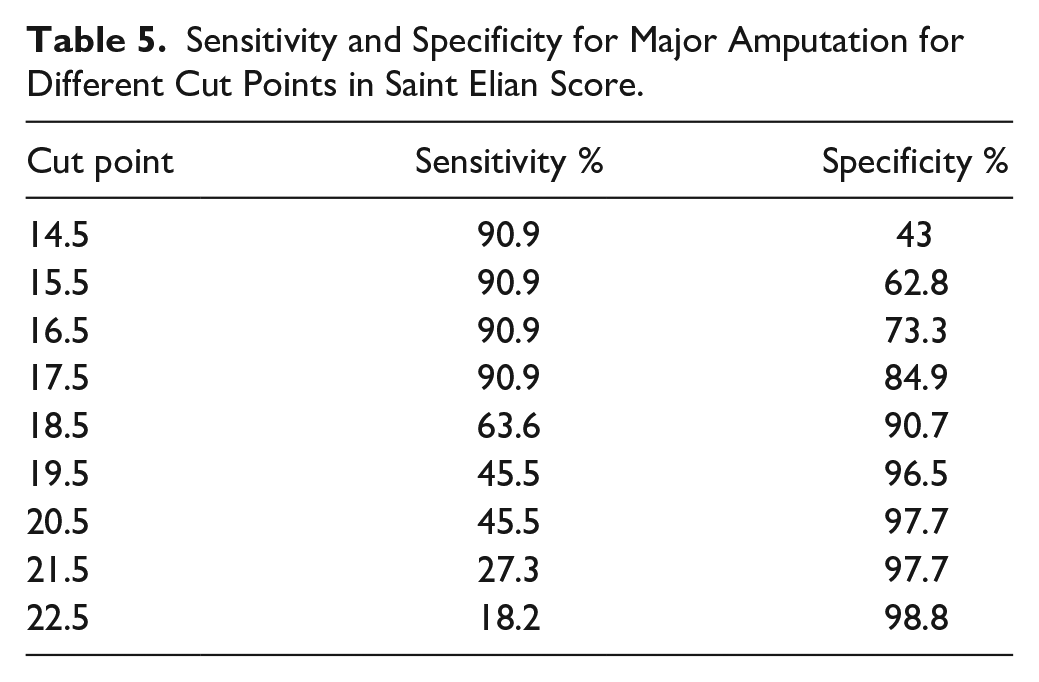
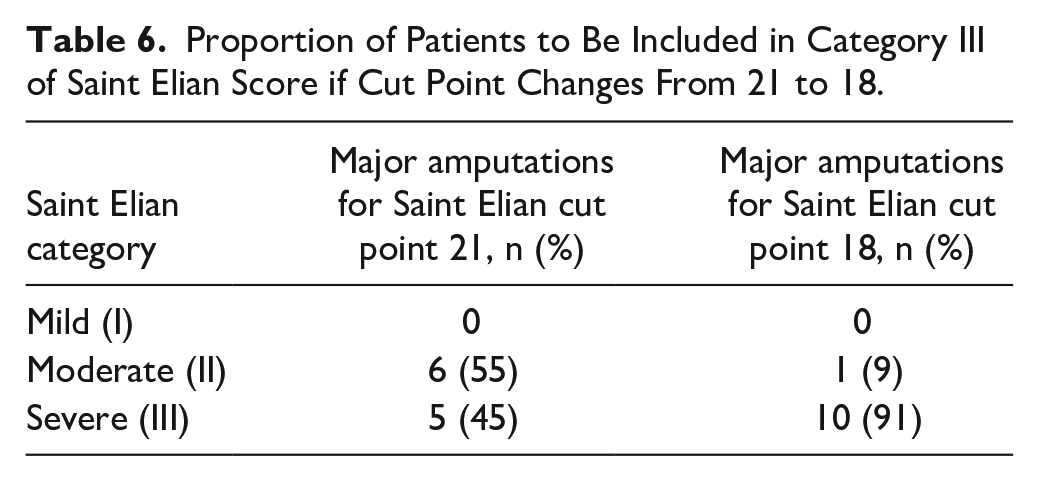
Changing Saint Elian’s cut point for severe category (III) to 18, 91% of major amputations are included in this category (Table 6).
Proportion of Patients to Be Included in Category III of Saint Elian Score if Cut Point Changes From 21 to 18.
There is no point for wound healing with enough sensitivity and specificity in Saint Elian Score.
Discussion
A wound classification system must be able to provide diagnostic precision and predict prognosis in an early stage, helping physicians avoid skipping important prognostic factors during the evaluation of the patient and the wound, considering opportune derivation, medical intervention, more aggressive treatment, and justifying cost-benefit strategies. Wagner and Texas have been extensively used, but they are poor in the description of the wound and do not include aspects as infection grade, wound size, or vasculopathy severity.
There is a growing debate regarding the use of foot ulcers’ classifications. Physicians who care for patients with diabetic foot ulcers are concerned about the use of one score or another, about which classification is recommended and what is the evidence for the use of these scores. Moreover, they discuss about the usefulness of these classifications, whether they should influence the decisions on the diagnosis and treatment or if they are only a tool for prognosis or audit. 1 In this study, we focused on 3 classifications: WIfI risk stratification score, 4 University of Texas Wound Classification System, 5 and Saint Elian Wound Score System, 2 and we intended to compare them to each other and to clinical outcomes, trying to augment the existing evidence on their usefulness.
There are differences between Saint Elian and WIfI classifications when they are compared with each other. Saint Elian category II (moderate risk) includes 80.2% of patients in our study, similar to the original article of Saint Elian score where the proportion was 76%. 2 The fact that most patients are included in moderate category could be a weakness of this classification, because there is a wide variety of lesions, with different grades of ischemia, infection, locations, and wound size, and therefore different outcomes. Lowering the cut point to 18 for severe lesions, 22.8% of all patients will be part of this category, including 90% of those who underwent major amputation and 70.1% of WIfI 4 patients, and this could imply a more accurate assessment of foot lesions and their prognosis by including a more homogeneous population of patients in Saint Elian categories. In our study, 18 is the cut point with higher sensitivity and specificity for major amputations. When we choose cut point of 12 for mild category in Saint Elian score instead of 10, it correlates better with WIfI 1 and 2 (very low and low risk) but has no good sensitivity and specificity for wound healing. Other challenge to implement this classification is the fact that it has too many points to evaluate, making it difficult and laborious as it takes time for its completion. However, Saint Elian takes into account various aspects of the wound not considered in other classifications, such as wound size, location, and number of affected zones that have been risk factors for major amputation in Saint Elian’s study. 2 The score has been built under the evidence of one observational study, and more evidence is necessary for external validation. The authors of this study emphasizes the importance of Saint Elian score to follow-up the wound healing progress and therapeutic impact, and encourage physicians to use the classification in each visit to evaluate evolution of the wound. 7
When analyzing Texas wound classification study, 5 there was a significant trend toward a higher prevalence of amputations (major and minor) for increasing depth and stage, and this was also true in our study, where 92% of major amputations corresponded to categories II and III with infection, ischemia, or both. We found a higher proportion of major amputations and more lesions that penetrated bone (51.4%) than in Texas study (30.3%). Texas classification is a 4 × 4 table easy to perform but gives not much information about wound characteristics such as degree of ischemia, wound extent, or location. It may be easy and fast to perform as it requires few aspects to evaluate, but lacks information about details, and because of its 16 categories, it is difficult to validate for major amputation or wound healing as the sampling size should be large enough.
WIfI risk stratification score was published in 2014, with the aim of creating an updated classification system after new technologies had risen, particularly endovascular procedures that made previous schemes obsolete. 4 This score was created taking into account 3 aspects of the lesion (wound characteristics, ischemia, and infection) and dividing the results into 4 grades based on clinical observations. The risk for each stage was assigned by a 12-member panel of experts on limb ischemia. Each member was asked to assign a limb threat clinical stage to the 64 categories that arise from the combination of the 3 risk factors. This procedure has defined the stages of WIfI for limb amputation risk and revascularization benefit. The WIfI classification system is not meant to function as a stand-alone clinical decision-making tool but as a guide for appropriate stratification of patients in clinical trials. Some reports have demonstrated good correlation between WIfI and both amputation risk and wound healing.12,13 However, more recently, these correlations have been questioned because other reports showed similar wound healing and major amputation rates for all WIfI stages. 14 WIfI classification takes into account ischemia, infection grade, and wound size, but it lacks information about localization, number of affected zones, and neuropathy that appear to be risk factors in Saint Elian study. 2 WIfI gives information about prognosis and revascularization benefit and has been validated in various studies with different results.12-21 Stages 1 and 2 behave in the same way as it was shown in our study and in the study of Zhan et al, 18 so these 2 stages could be unified. Although the information given by this classification is more complete than that of Texas, it is more difficult to implement because it requires an Android application or a table to calculate the stage.
A systematic review and meta-analysis was published in 2019 with the aim of summarizing the current evidence on the prognostic value of WIfI classification system in clinical practice. 19 This study shows that WIfI can predict major amputation after 1 year but is not sufficient for helping in clinical decision-making. The search yielded 12 studies comprising 2669 patients and included diabetic and nondiabetic patients. This meta-analysis concludes that major amputation risk rises with increasing WIfI stage, as it is shown in an article published in 2017 15 and in our study too.
Some issues may have affected the results of our study. For example, there is 1 patient who underwent a major amputation that was classified as Texas IB, Saint Elian 14, and WIfI 2, and this fact could bias the results because it corresponds to low risk for Texas and WIfI and moderate risk with a low score for Saint Elian. The lesion started as a small and punctiform finger ulcer and progressed into necrosis and ischemia that could not be revascularized in time. As patients were treated in a tertiary hospital in a developing country, there may be some procedures not available for advanced wound healing treatment such as negative-pressure wound therapy or growth factors, and this can potentially result in nonidentical outcomes to other studies.
There are still many differences in the results of the studies regarding the correlation of classifications with wound healing or major amputation. This may be due to the availability of treatments in each center and countries and the heterogeneity of the samples in the studies. It is important to design new investigation studies to conclude whether one classification is better than the others or if its usefulness depends on the necessities of the multidisciplinary team, patients, country, and health system.
Some studies analyzing WIfI and Saint Elian score are summarized in Table 7.
Results and Comparison of Studies.
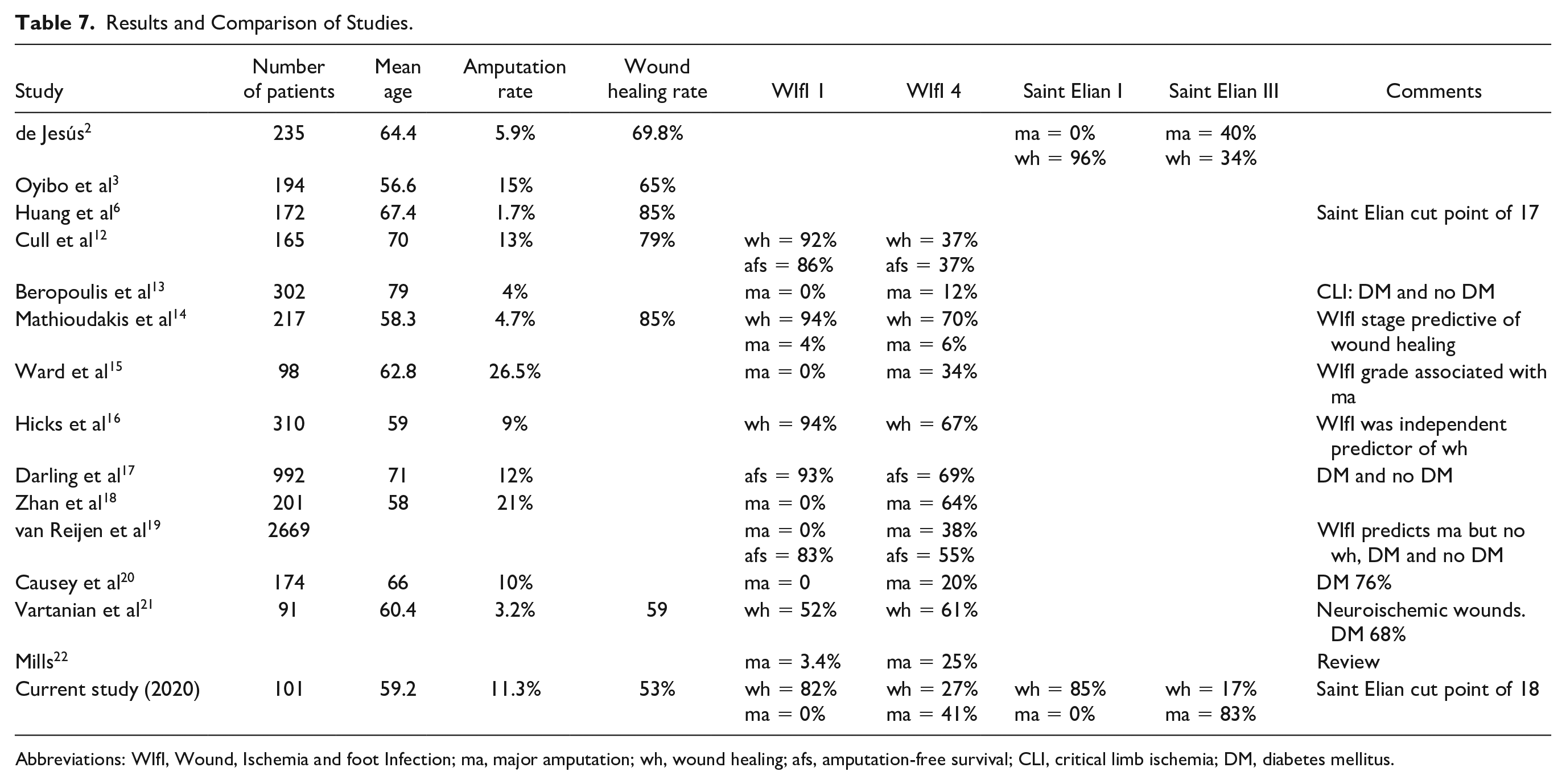
Abbreviations: WIfI, Wound, Ischemia and foot Infection; ma, major amputation; wh, wound healing; afs, amputation-free survival; CLI, critical limb ischemia; DM, diabetes mellitus.
Conclusions
WIfI and Saint Elian do not correlate well in the descriptive analysis. They match when Saint Elian is at low or high risk but not when it is moderate. The correlation improves if Saint Elian cut point for high risk is 18 and if cut point for low risk is 12.
WIfI 4 behaves different from the other categories in the follow-up analysis, not only for wound healing but also for major amputation. Saint Elian III patients had higher rates of major amputation and less rates of wound healing than the other categories.
WIfI stages correlate with major amputation and wound healing. Saint Elian III correlates with major amputation. The optimal cut point for detecting major amputation is 18, but there is no recommended cut point for wound healing. Saint Elian I has higher rates of wound healing than other categories.
Ninety-two percent of amputation had been performed in patients with Texas II and III, B, C and D.
Stages 1 and 2 of WIfI score behaves similar with regard to wound healing and major amputation. Stages I and II of Saint Elian have the same rates of major amputation but not of wound healing.
Footnotes
Acknowledgements
Authors would like to thank Dr. Carlos Eghi and Marcela Mariano from Investigation and Research Department, and Dr. Matías Baldini from Ethics Committee.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.