
Abstract
The aim of this single-center, retrospective study is to demonstrate the effectiveness of distally based peroneus brevis muscle flap as first therapeutic option for infections after Achilles tendon open repair. We retrospectively analyzed 14 consecutive patients with complete Achilles tendon rupture and developing surgical site infection after an attempt of open surgical repair. Every patient was reconstructed with distally base peroneus brevis muscle flap. The primary outcome was the return to work and the initiation of full weight-bearing. Secondary outcomes were complication rate and time needed to return to work. A review of the literature was conducted to better define the actual standard treatment. Each patient returned to work. No flap necrosis occurred. Two minor healing delays and one hematoma were reported. Median time to wound healing was 17 days (interquartile range [IQR] = 13-20). Median time to full weight-bearing was 52 days (IQR = 47-55). Median follow-up (FU) was 21 months. Distally based peroneus brevis flap is a safe treatment for surgical site infections after Achilles tendon rupture repair. Patients regained full weight-bearing after a median time of 52 days from the surgical reconstruction. No major complications were observed. This flap clearly emerges as first reconstructive option for complications after surgery of Achilles tendon region.
Introduction
Open repair after Achilles tendon ruptures can complicate with infection, 1 presenting with skin and tendon necrosis. Exposure of suture stitches and tendon augmentation adjuncts often follows. These complications significantly lengthen healing time and might hinder return to full weight-bearing. While defined techniques exist for the primary repair of Achilles tendon rupture, treatment protocol for its complications is not yet defined. 1
Secondary intention healing, with multiple debridement and negative pressure wound therapy, implies patient discomfort and long healing time, with no predictable result. 1 Skin graft succeeds only on a clean, viable wound bed and is not indicated in presence of infection 2 : in this case, regional or distant flaps are considered the best option, fasciocutaneous and muscle flaps being equally effective on local infection control.3,4 Propeller flaps have higher partial necrosis rates, while free flaps have higher infection and coverage defect rates. 4
Distally based peroneus brevis (PB) muscle flap is a feasible reconstructive option for ankle and foot defects.5-9 The PB is located in the lateral leg compartment, deep and anterior to the peroneus longus. It originates from the middle third of the fibula and inserts on the base of the fifth metatarsal. Innervated by the superficial peroneal nerve, it pronates and extra-rotates the foot. Its function can be easily replaced by the peroneus longus.
Its use as flap was first described by Pers and Medgyesi. 10 The proximal two thirds of the muscle are vascularized from the anterior tibial artery whereas the distal third from the peroneal artery. 11 It is considered a type IV according to Mathes and Nahai muscle flap classification. 12 Initially described as a proximally based flap, 13 today it is frequently described as a distally based flap for foot and ankle coverage. 14
To further understand the role of the PB muscle flap, we performed a literature review. Because of very few total flap losses described, the PB muscle flap has already proven to be a safe solution for primary reconstruction of the Achilles region. We show for the first time its additional effectiveness for complicated soft tissue defects of the above-mentioned anatomical zone.
Materials and Methods
After the Local Ethics Committee approval, we retrospectively reviewed clinical data of 14 consecutive patients referred to our department from 2013 to 2018 affected by a surgical site infection (SSI) occurred after Achilles tendon open repair.
Inclusion criteria were clinical diagnosis of SSIi complicated by skin and tendon necrosis after complete Achilles tendon rupture open repair as well as the presence of a positive microbiological swab. The exclusion criterion was a previous history of surgical intervention other than the primary surgical repair.
On admittance, detailed personal and surgical history was taken for each patient. A physical examination was performed by the senior author LV, with focus on clinical conditions of the Achilles region wound and recording preoperative active and passive range of motion (ROM).
The chief surgeon (senior author LV) performed surgical debridement followed by an immediate coverage with distally based PB muscle flap in each patient. A cefazolin-based preoperative antibiotic prophylaxis was administered and continued for 5 days during the postoperative period.
The primary outcome was the rate of full weight-bearing and return to work. Secondary outcomes were the postoperative complication rate and the days needed to return to work.
Surgical Technique
The surgical technique is well described in the literature.12,13,15 The patient is supine, with the affected limb internally rotated (with a sandbag under the ipsilateral buttock). Under general anesthesia with a thigh tourniquet, the first essential step is always represented by a careful debridement of the tendon and eventual prosthetic material removal (Figure 1).
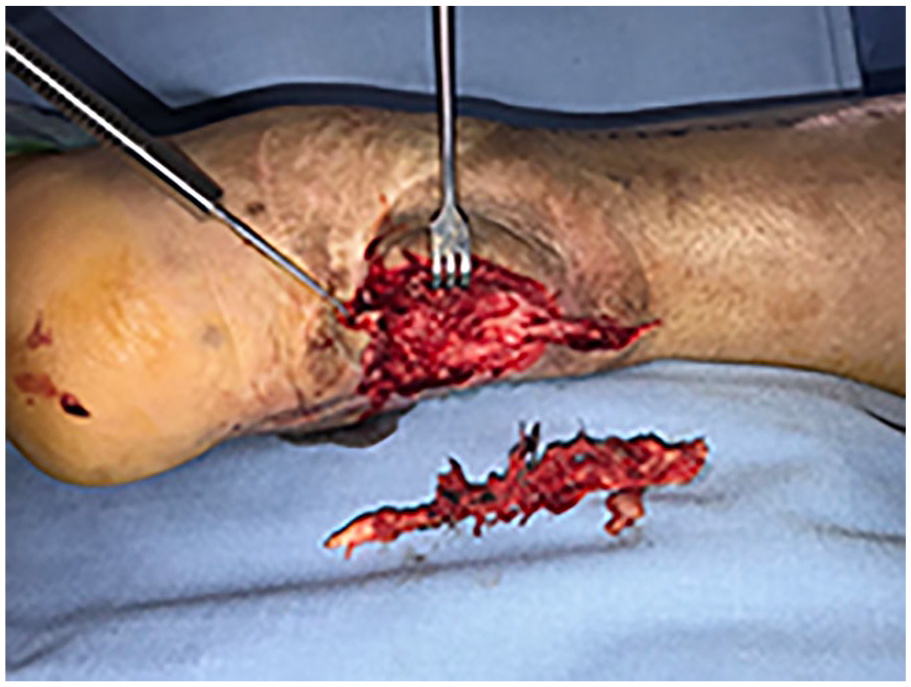
Left Achilles tendon with exposed synthetic mesh. A left Achilles tendon previously repaired with a Gore-Tex mesh. The patient developed an infection with exposure of the mesh. At the time of the first debridement, the mesh was excised.
After that, you can proceed with the flap harvesting. Skin and fascia are incised from 4 cm distally to the fibular head to 3 cm proximally to lateral malleolus; this incision is performed 1 cm posteriorly to the fibular line. Extreme care is taken to preserve the superficial branch of the peroneal nerve. The peroneus longus lies superficial and posterior to the PB: once retracted, the PB muscle is exposed. Muscle insertions are detached from the fibula and the posterior intermuscular septum and the dissection proceeds subperiosteally from proximal to distal. Dissection stops when you encounter a suitable perforator vessel running through the posterior septum, usually within 8 cm from the lateral malleolus (Figure 2). The flap is tunneled under the skin and distally rotated (Figure 3A and B). Eventually, the muscle flap is covered with a split-thickness skin graft, and the donor site is restored by means of a primary closure. A cast is applied to avoid temporary flexion-extension of the ankle.

Left peroneus brevis isolated. Complete isolation of a left, distally based, peroneus brevis muscle flap. To notice the extension of the muscle belly till the proximal third of the leg, allowing complete coverage of the Achilles region once distally rotated.
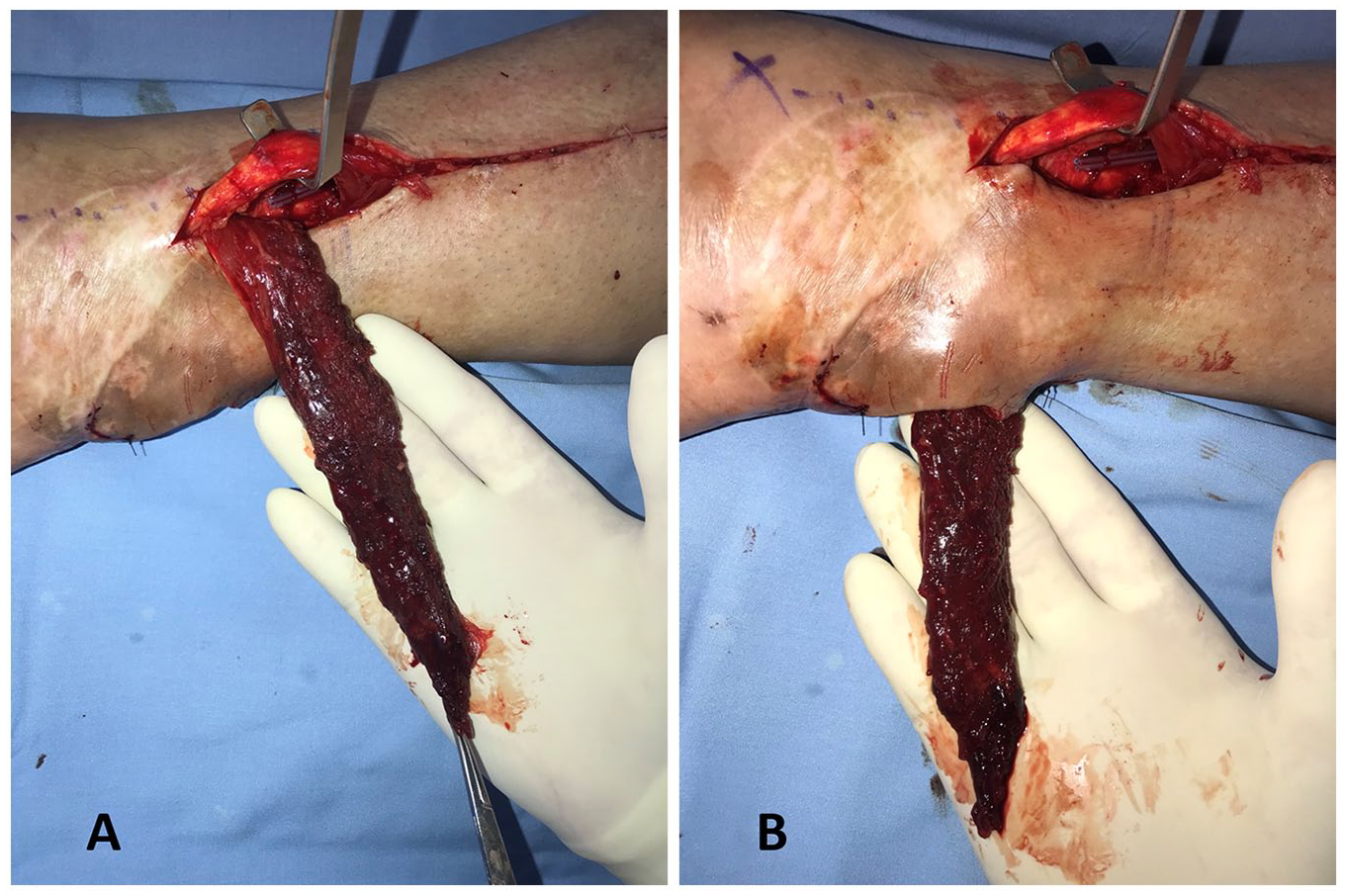
Tunneling of the distally based peroneus brevis (DBPB) under the lateral malleolus skin. (A) The DBPB is completely isolated and the arc of rotation is firstly assessed with the muscle overlying the skin of the ankle. (B) Once the complete coverage of the Achilles tendon is demonstrated, the flap is tunneled under a skin bridge posterior to the lateral malleolus, to reduce the skin grafted area.
Postoperative Management
The patient may be discharged the day after the surgical intervention, keeping the affected limb unloaded in non–weight-bearing. The first clinical FU and dressing change is performed after 5 days. The cast is maintained at least for 4 weeks. Full weight-bearing is permitted not earlier than the fourth week after surgery. Ankle active and passive ROM was assessed in every patient at the initiation of the full weight-bearing and after 6 months from the operation.
Literature Review
MEDLINE, Embase, and the Cochrane Library Database were searched for “peroneus brevis muscle” from inception to December 2019 by 2 independent expert doctors (authors FA and GC). A total of 2305 citations were restituted. Books, letters, case reports, and case series with less than 4 patients were excluded from our review. After removal of duplicates, a total of 18 studies were included in the review.
Results
Three female and 11 male patients were included in the study. Median age was 54 years (interquartile range [IQR] = 43-59). Right Achilles tendon was involved in 11 patients. Six patients were active smokers. Patient characteristics are shown in Table 1.
Patients Characteristics and Main Outcomes.
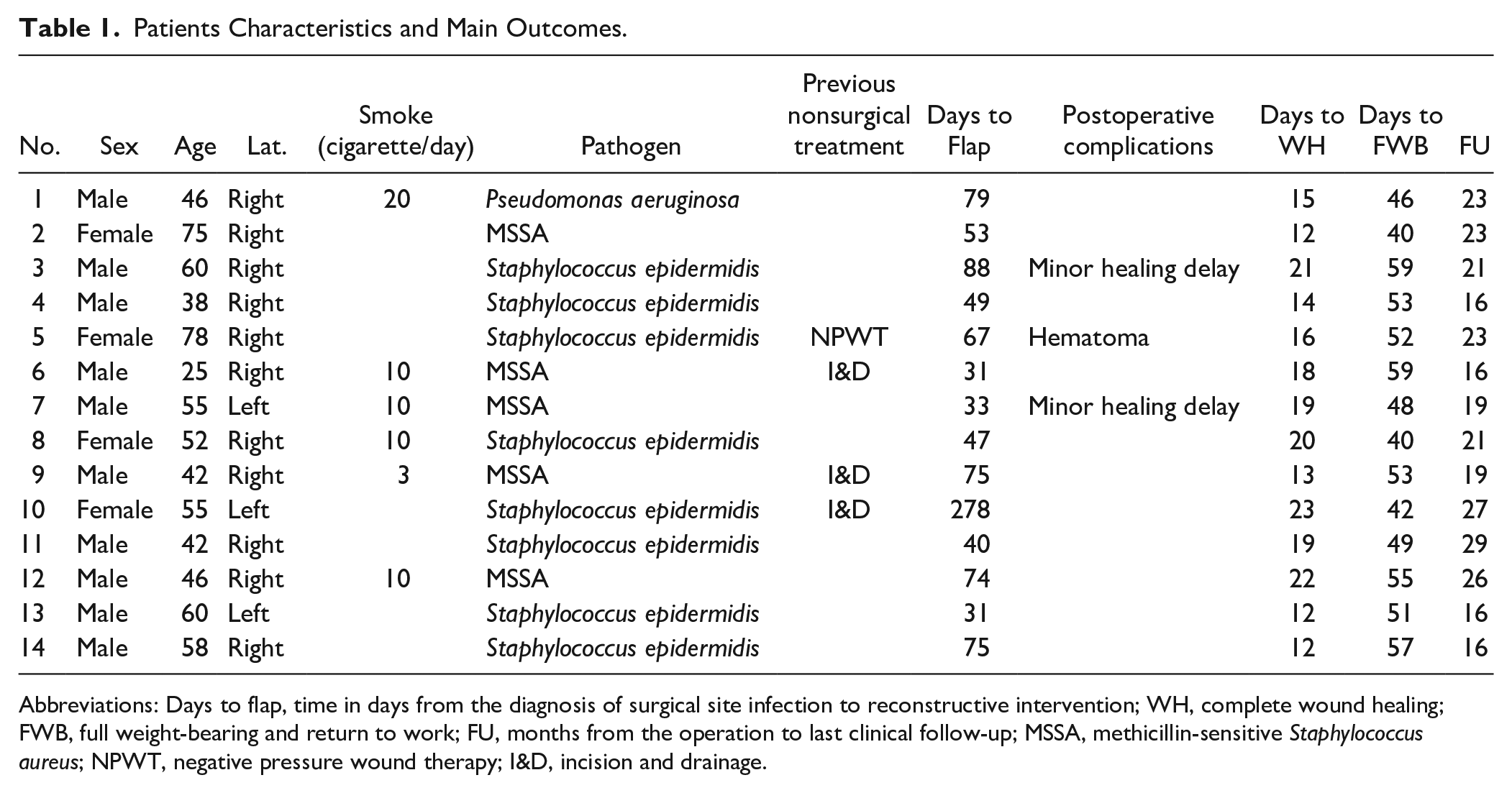
Abbreviations: Days to flap, time in days from the diagnosis of surgical site infection to reconstructive intervention; WH, complete wound healing; FWB, full weight-bearing and return to work; FU, months from the operation to last clinical follow-up; MSSA, methicillin-sensitive Staphylococcus aureus; NPWT, negative pressure wound therapy; I&D, incision and drainage.
The median time between the clinical diagnosis of complicated SSI and our surgical intervention was 60 days (IQR = 42-75). Microbiological swab tests reported methicillin-sensitive Staphylococcus aureus in 5 cases, Staphylococcus epidermidis in 8 cases, and Pseudomonas aeruginosa in 1 case. We found an exposed and infected Gore-Tex mesh, previously used for tendon augmentation, in 1 patient (#3). This last patient was 1 of the 2 cases who developed a partial skin graft loss.
Each of our patients was able to return to work. Median FU was 21 months (IQR = 17-23). (Figure 4, case #3: complete flap recovery; and Figure 5A and B, case #3: complete dorsiflexion recovery of the foot after 57 days.)

Complete healing after a distally based peroneus brevis + skin graft. The showed healing is achieved after 57 days from the operation. No hypertrophic scar or functional impairment is noticeable.

Range of motion after Achilles tendon reconstruction with distally based peroneus brevis. The patient achieved almost complete plantar-flexion (A) and dorsiflexion (B) of the foot after reconstruction of the Achilles tendon with the peroneus brevis flap.
No lower extremity functional deficits were observed. All flaps survived, without any reoperation. No major complications occurred, including tendon re-rupture, infection relapse, or flap loss. Minor complications were observed in 3 patients (21%): 2 partial skin graft necrosis (we think because an excessive friction on the cast) and 1 hematoma. Interestingly, the skin graft often appeared hyperpigmented at the first FU appointment resembling a partial loss.
Median time to reach a complete wound healing was 17 days (IQR = 13-20). Full weight-bearing and return to work were reached after a median of 52 days (IQR = 47-55). Median passive ankle ROM was 0° to 45° for plantar flexion and 0° to 15° of dorsiflexion; median active ROM was 0° to 40° of plantar flexion and 0° to 10° of dorsiflexion.
Discussion
Achilles tendon open repair complications commonly require long healing time. 1 Unfortunately, the inability to bear weight on affected limb for prolonged periods increases patient’s discomfort and decreases the affected joint’s mobility. Thus, a reconstruction with minimal morbidity and high reliability is strongly encouraged.
In our case series, we demonstrate the effectiveness of the PB muscle flap as treatment for infection after Achilles tendon open repair. After “reverse” PB muscle flap reconstruction, we showed a median time of 52 days to reach a full weight-bearing on affected limb and to return to work. Despite a single hematoma, there were no other major complications, reoperations, or flap losses.
A total of 426 cases in 18 studies regarding the PB muscle flap for foot and ankle reconstruction has been identified (Table 2). Total flap losses were described in 14 cases, showing the average rate of PB muscle flap failure to be less than 1%. Partial flap loss and other minor complications (ie, skin graft necrosis, healing delay, hematomas without the need for reoperation) were described in 9% and 13% of cases, respectively. The overall rate of complications has been estimated to be 21%. Compared with our series, we did not have total flap losses; our minor complication rate was 21%, exactly matching results emerged from the literature analysis.
Details Regarding Studies Included in the Literature Review.
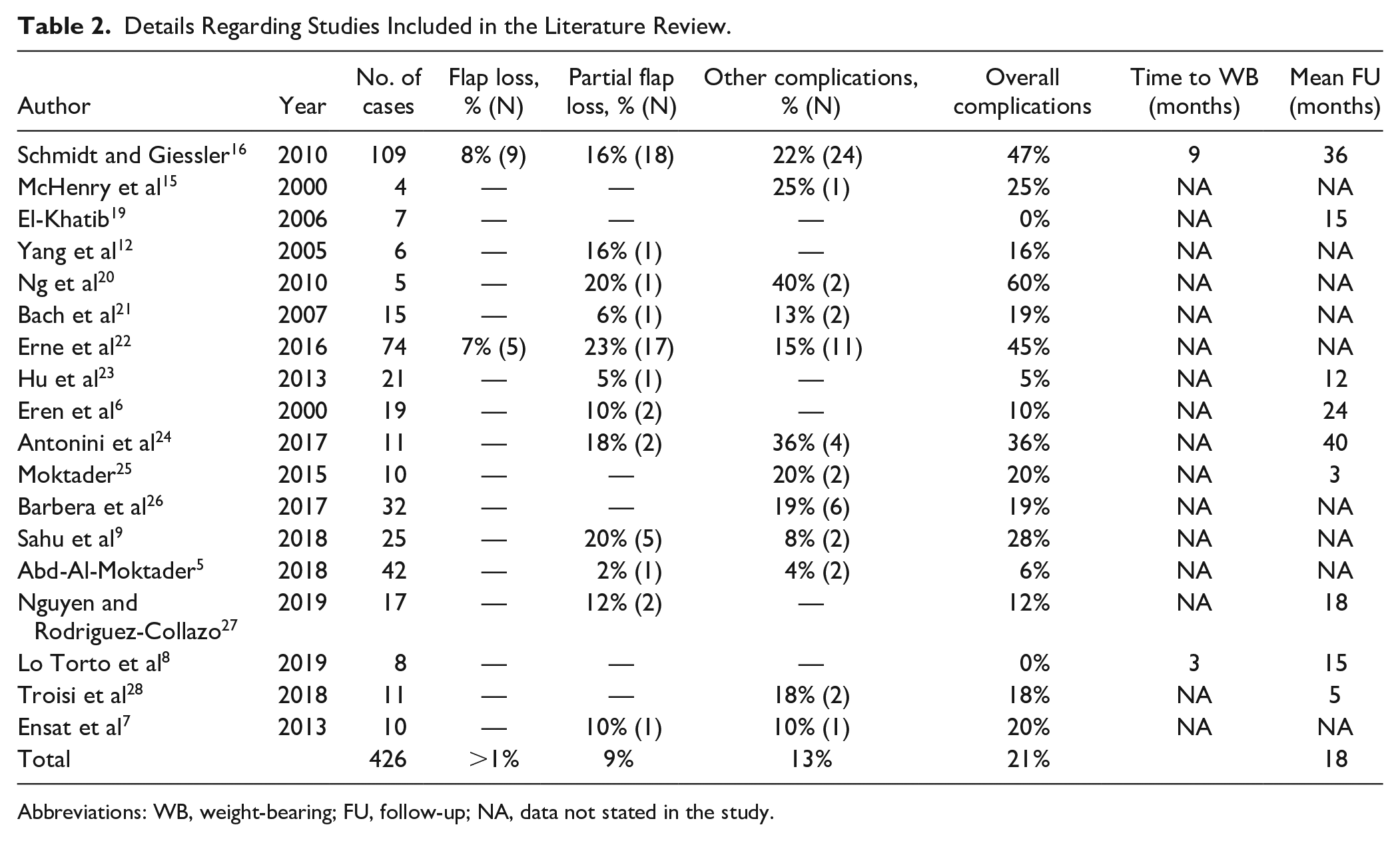
Abbreviations: WB, weight-bearing; FU, follow-up; NA, data not stated in the study.
Even if Schmidt and Giessler 16 describe the use of a composite osteomuscular PB flap in the largest case series known so far, in their series, the PB muscle flap is used only twice after elective orthopedic surgery complications. Our results only refer to complicated previous attempts of Achilles tendon reconstruction.
Interestingly, among the 18 selected studies, only the studies by Schmidt and Giessler 16 and Lo Torto et al 8 evaluated the time needed to recover a full weight-bearing, being 9 and 3 months, respectively; the average FU (only 9/18 studies divulged it) was 18 months.
It can be argued that the use of pedicled propeller flaps 17 might be a better option compared with PB muscle flap, being less invasive and sparing the muscle. 18 Nevertheless, local fasciocutaneous flaps showed a complication rate of 25.2% in the meta-analysis performed by Bekara et al, 4 with a 3.5% of total flap loss and 10.2% of partial flap loss.
A direct comparison study between pedicled fasciocutaneous flaps and local muscle flaps for the foot and ankle reconstruction is not yet available. Thus, a reliable comparison between their safety and efficacy is not possible. In our series, the sacrifice of the PB muscle did not impair ankle dorsiflexion or supination, without clinically significant functional reduction. Moreover, no complications of donor sites were recorded.
Our study, though, is the first to show the efficacy of PB muscle flap in complicated reconstruction of the Achilles tendon area, and we, therefore, consider it as a good first-line reconstructive option for SSIs of open Achilles tendon repair.
We well know the main limitations of our study: small sample size, lack of validated outcome measures, and study design, with case series having low level of evidence. However, all the 18 studies included in our literature review were case series. For this reason, we advocate further studies comparing PB muscle flap with pedicled-propeller fasciocutaneous flaps in the treatment of Achilles tendon surgical repair complications.
We consider the distally based PB muscle flap a reliable solution for Achilles tendon repair complications, leading to weight-bearing on affected limb in less than 2 months and with no significant morbidity.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.