
Abstract
Eccrine syringofibroadenoma (ESFA) is a rare adnexal tumor deriving from the acrosyringeal portion of the eccrine duct. Five subtypes of ESFA were described including a reactive form. Reactive ESFAs are associated with inflammatory and neoplastic dermatoses. In this article, we report the case of a 90-year-old woman presenting with 3 leg ulcers evolving for 2 years surrounded by large verrucous and eczematous lesions. Multiple skin biopsies showed anastomosing epithelial cords connected to the epidermis consistent with ESFA. We identified 8 cases of ESFA associated with chronic leg ulcers in the literature and reviewed their main clinical and histological features.
Introduction
Eccrine syringofibroadenoma (ESFA) is a rare adnexal tumor originally described by Mascaro in 1963. 1 This adnexal tumor is derived from eccrine duct cells. ESFA usually presents as a single lesion with a predilection for acral sites. Based on the classification of French 2 published in 1997, one of the major clinical subtypes of ESFA is reactive ESFA, which is frequently associated with neoplasia or inflammatory dermatoses such as squamous cell carcinoma and bullous pemphigoid.3,4
We report the case of a 90-year-old woman who presented eccrine syringofibroadenomatosis associated with chronic venous leg ulcers.
Case Report
A 90-year-old woman was initially referred for a 2-year history of venous leg ulcers. The patient’s past medical history included atrial fibrillation, arterial hypertension, and hypothyroidism. Clinical examination showed 3 bilateral perimalleolar leg ulcers and well-defined peripheral eczematous lesions. Contact dermatitis was suspected and patch testing was performed with the European battery series, Revidal-Gerda battery series, and lower leg, cosmetic, and excipient battery series. Patch tests were positive for several allergens including Myroxylon pereirae (balsam of Peru), benzalkonium chloride, linalool hydroperoxide (fragrance), budesonide, and cetostearyl alcohol (emulsion stabilizer of emollient included in betamethasone cream). Additional patch tests with corticosteroid battery and repeat open application test with betamethasone used by the patient were negative. Peripheral lesions continued to enlarge despite eviction of the allergens, applications of topical steroids (diflucortolone), and topical tacrolimus ointments. Histological examination of a skin biopsy taken from the surrounding eczematous lesions showed perivascular lymphocytic infiltrate with hyperkeratosis spongiosis and epidermal hyperplasia, without signs of malignancy, consistent with a diagnosis of subacute and chronic eczema. A Doppler ultrasound of the lower limbs showed patent deep venous incompetence with pronounced reflux. The eczematous lesions continued to worsen during the following months despite the use of elastic compression bandages and prolonged applications of topical corticosteroids.
The patient was then referred to our Dermatology Department after 2 years of evolution of skin lesions. Clinical examination showed 3 ulcers with raised borders measuring 2 × 1 cm on the internal surface of the right leg, 4 × 1 cm and 2.5 × 1 cm on the internal and external surface of the left leg, respectively. These ulcers were surrounded by infiltrated verrucous plaques associated with eczematous lesions extending from the dorsum of the feet to the lower part of the leg (Figure 1). There were no peripheral lymph nodes. Multiple biopsies were performed in the hypothesis of squamous cell carcinoma. Histological examination showed thin cords developing from the epidermis into the dermis surrounded by a lymphocytic infiltrate (Figure 2). Based on the long duration of these lesions, their clinical features, and the histological picture, a diagnosis of reactive ESFA associated with chronic venous ulcers was made. Surgical excision was not performed due to the extent of reactive ESFA. The patient was treated with compression therapy and wound dressing (lipidocolloid dressing). A partial improvement was observed after 1 year of follow-up.

Ulcerations of the external (A) and internal surface (B) of the left lower leg surrounded by verrucous and infiltrated lesions. Ulceration of the internal surface of the right lower leg (C).
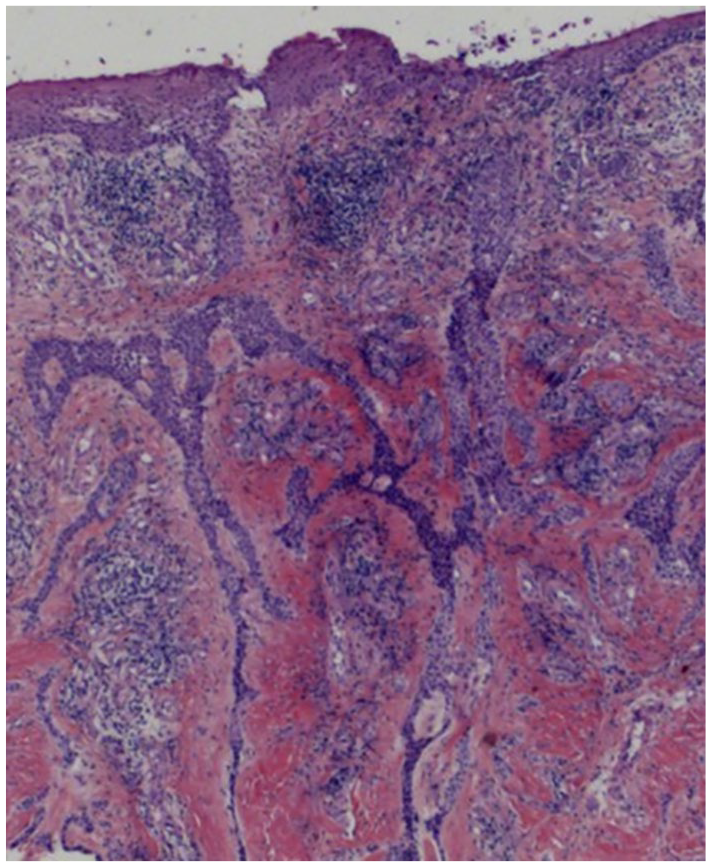
Thin anastomosing reticulated cords of small epithelial cells extending from the basal layer of epidermis into dermis were observed (hematoxylin-eosin-saffron, original magnification ×2.5).
Discussion
Based on Starink’s classification 5 modified by French, 2 ESFA is classified into 5 subtypes: (1) solitary ESFA, (2) multiple ESFA with ectodermal dysplasia syndrome (Clouston’s syndrome and Schöpf-Schulz-Passarge’s syndrome), (3) multiple (diffuse, zosteriform, linear) ESFA without associated cutaneous findings, (4) nonfamilial unilateral linear ESFA, and (5) reactive ESFA. The reactive subtype ESFA is associated with skin neoplasia such as squamous cell carcinoma, 6 basal cell carcinoma, 7 and pilomatricoma. 8 Reactive ESFA has also been reported to be associated with inflammatory skin disorders such as palmoplantar eczema, 9 bullous pemphigoid, 10 erosive lichen planus, 11 primary cutaneous amyloidosis, 12 peristomal dermopathy, 13 and chronic ulceration.
Around 40 cases of reactive ESFA have been reported in the literature, including 8 cases occurring in patients with chronic leg ulcers (Table 1).14 -21 Patients’ mean age was 64.5 years (range = 50 to 78 years). The average duration of lesions before diagnosis was 2 years (range = 6 months to 5 years). All cases were localized on the extremities of the lower limbs. Clinical manifestations were variable, ranging from pinkish papules to large verrucous plaques. Three cases were associated with leprosy14 -16; one case was related to diabetes mellitus. 17 In these 4 cases, lesions were localized on the sole of the foot, likely favored by polyneuropathy due to leprosy or diabetes mellitus, which was evidenced in these 4 patients. Reactive ESFA has also been reported in the absence of neuropathy. Two cases were described secondary to chronic traumatic injury,18,19 including one case of reactive ESFA, which occurred within 6 months after the onset of an ulcer of the right sole. 19 ESFA typically occurs on chronic nonhealing ulcers but can also be associated with long-lasting wounds. Ichikawa et al 20 reported a case of verrucous lesions consistent with reactive ESFA developing on a burn scar. In accordance with the present case, reactive ESFA was described in a patient who presented fleshy verrucous plaques with a history of chronic venous ulcers and severe peripheral vascular disease. 21
Review of Reported Cases of Reactive Eccrine Syringofibroadenoma Associated With Chronic Ulcer.
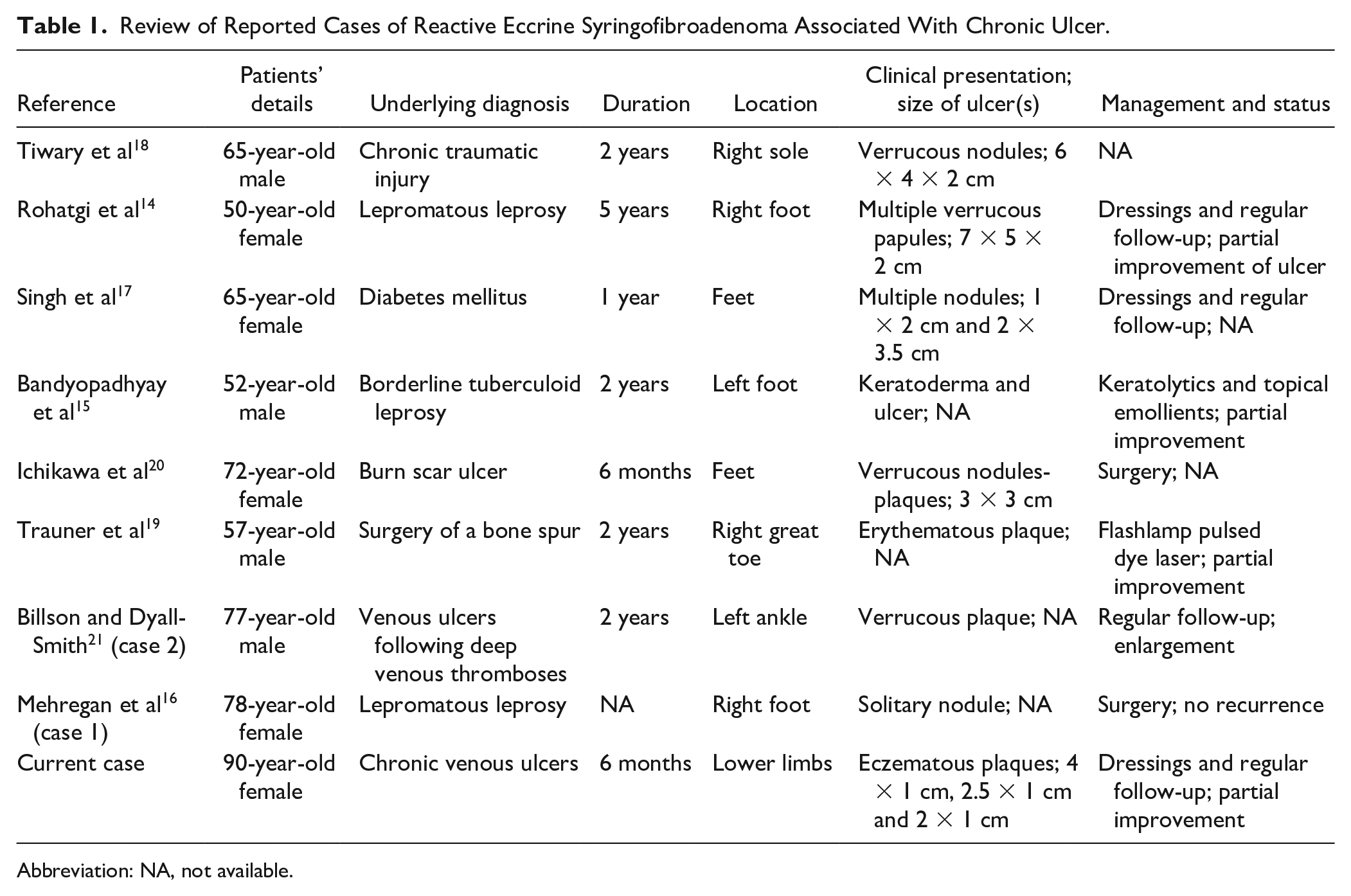
Abbreviation: NA, not available.
Surgical excision is the mainstay of treatment for localized forms of ESFA.16,20 Treatment of extensive forms is limited to wound care and regular follow-up.14,21 Pulsed dye laser was proposed in a recalcitrant case of ESFA, which did not previously respond to cryotherapy and electrodessication. 19
Regarding the literature, 8 cases of reactive ESFA were associated with chronic ulcers, but only one was a case of localized form of ESFA associated with venous leg ulcer. To our knowledge, we described the first case of bilateral reactive ESFA associated with chronic venous leg ulcers. Overall, despite its rarity, a diagnosis of reactive ESFA must be proposed in patients with nonhealing verrucous lesions surrounding chronic venous ulcers as an alternative diagnosis to squamous cell carcinoma.
Footnotes
Acknowledgements
The authors are grateful to Nikki Sabourin-Gibbs, Rouen University Hospital, for her help in editing the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent to publication was obtained from the patient.