
Abstract
Madura foot is a chronic, progressively destructive bacterial or fungal infection of the subcutaneous tissues, which may affect skin, muscle, and bone. It is endemic in tropical and subtropical areas known as the “Mycetoma belt” between latitude 30°N and 15°S. Mycetoma is prevalent in the poor population living in remote areas of developing countries that lack proper reporting system and management. The World Health Organization recognized mycetoma as a neglected tropical disease back in 2016. Though the diagnosis is challenging, early detection and proper treatment can reduce morbidity and provide a promising outcome. We report a case of chronic painless, multiple papulo-nodular skin lesions at the foot that resembles mycetoma infection which was detected early and recovered with a satisfactory outcome with proper treatment.
Introduction
Madura foot or pedal mycetoma is a debilitating suppurative infection that involves the subcutaneous tissues and extends into deeper tissues. Though the foot is the commonest site, mycetoma infection can occur at other sites like hand, knee, scalp, neck, chest, abdomen, arm, buttock, perineum, and shoulder. 1 Mycetoma is more far-reaching than previously estimated. It has been reported in 102 countries. 2 However, it is endemic in tropical and subtropical areas known as the “Mycetoma belt” between latitude 30°N and 15°S, which includes the Bolivarian Republic of Venezuela, Mexico, Chad, Ethiopia, India, Mauritania, Senegal, Somalia, Ethiopia, Sudan, Thailand, and Yemen. 1 A systemic meta-analysis on the global burden of human mycetoma conducted by van de Sande 3 revealed 7 different actinomycetes responsible for actinomycetoma and 18 different fungal species as the causative agents for eumycetoma. A definite diagnosis of the causative agent is necessary as the treatment of the 2 etiologies is entirely different. Though the diagnosis is challenging, early detection and proper treatment can reduce morbidity and improve treatment outcomes. 2 Mycetoma is more common among the poor population. Living in remote areas of developing countries makes proper reporting and management more difficult. Moreover, the lack of trained staff, health care facilities, proper diagnostic tools, and treatment make the cases even worse. The World Health Organization recognized mycetoma as a neglected tropical disease back in 2016. 4 As mycetoma is not endemic in Malaysia, little is known about its prevalence in Malaysia where it prevails in sporadic form and causes diagnostic challenges.
We report a case of chronic painless, multiple papulo-nodular skin lesions at the foot resembling mycetoma infection which was detected early and recovered with a satisfactory outcome with treatment.
Case Study
A 60-year-old Malay lady was referred to our orthopedic clinic with multiple papulo-nodular lesions at the right foot for 2 months. The skin lesion was spreading in all directions despite the treatment in the local general practitioner clinic. She was a known case of diabetic mellitus and chronic kidney disease (CKD) and was on regular dialysis. She was on oral antibiotics and topical antibacterial and steroid ointment for 1 month. She came from a village with a poor socio-economic background, and she used to like working in her house garden barefooted. Her husband had a similar infection 1 year back and had undergone a below-knee amputation to control the infection. But he subsequently succumbed following the complications of the surgery. Initially, she was provided telemedicine service and advised for referral with an oral broad-spectrum antibiotic and topical antifungal cream.
The patient was very anxious at presentation. On examination, multiple papules and nodules were noted at the back of her right heel, around the ankle joint, and mostly at the medial side of the foot. There was a localized, 3 × 3 cm, slightly elevated fissured and cracked area at the medial aspect of the heel at the margin of the dorsum and the sole (Figure 1). There was no local pain. The affected area had normal skin temperature and was hyperpigmented. Nodules were firm on palpation and mildly tender on deep palpation. Some vesicular lesions were also present. The discharge came out from the nodules following the crush. The discharge was like the characteristic granular grains. But there was no discharging sinus. X-ray of the ankle joint, crushed swab of the nodules for culture and sensitivity (CS) were taken at the first visit. X-ray was normal. A crushed swab CS study was done for Gram-negative, Gram-positive, and fungal culture. There was a growth of Staphylococcus aureus which was sensitive to Cloxacillin but there was no growth of fungus. Tablet Cloxacillin along with topical antifungal cream was added to her treatment regimen. However, there was no sign of improvement even after 1 month of antibiotics and topical antifungal therapy.

Clinical picture of the patient at presentation.
Then tissue biopsy was taken under local anesthesia (Figure 2). Histopathology report showed skin tissue with pseudo-epitheliomatous hyperplasia and focal hyperkeratosis of the epidermis. There was mild to moderate intraepithelial lymphocytic and neutrophilic infiltrate. The dermis was densely infiltrated by lymphoplasmacytic infiltrates. There were scattered multinucleated giant cells and small granulomas formed by epithelioid histiocytes. Focal neutrophilic infiltrates were observed (Figure 3). Periodic acid–Schiff (PAS) stain was negative for fungal bodies and Ziehl–Neelsen (ZN) stain was negative for acid-fast bacilli. Histopathological diagnosis was suggestive of suppurative granulomatous inflammation. Histopathologists commented that although PAS and ZN stains were negative for microorganisms, correlation with the clinical, microbiological, and histopathological investigation was recommended to ascertain the etiology of this suppurative granulomatous inflammation.

Clinical picture after the tissue biopsy.
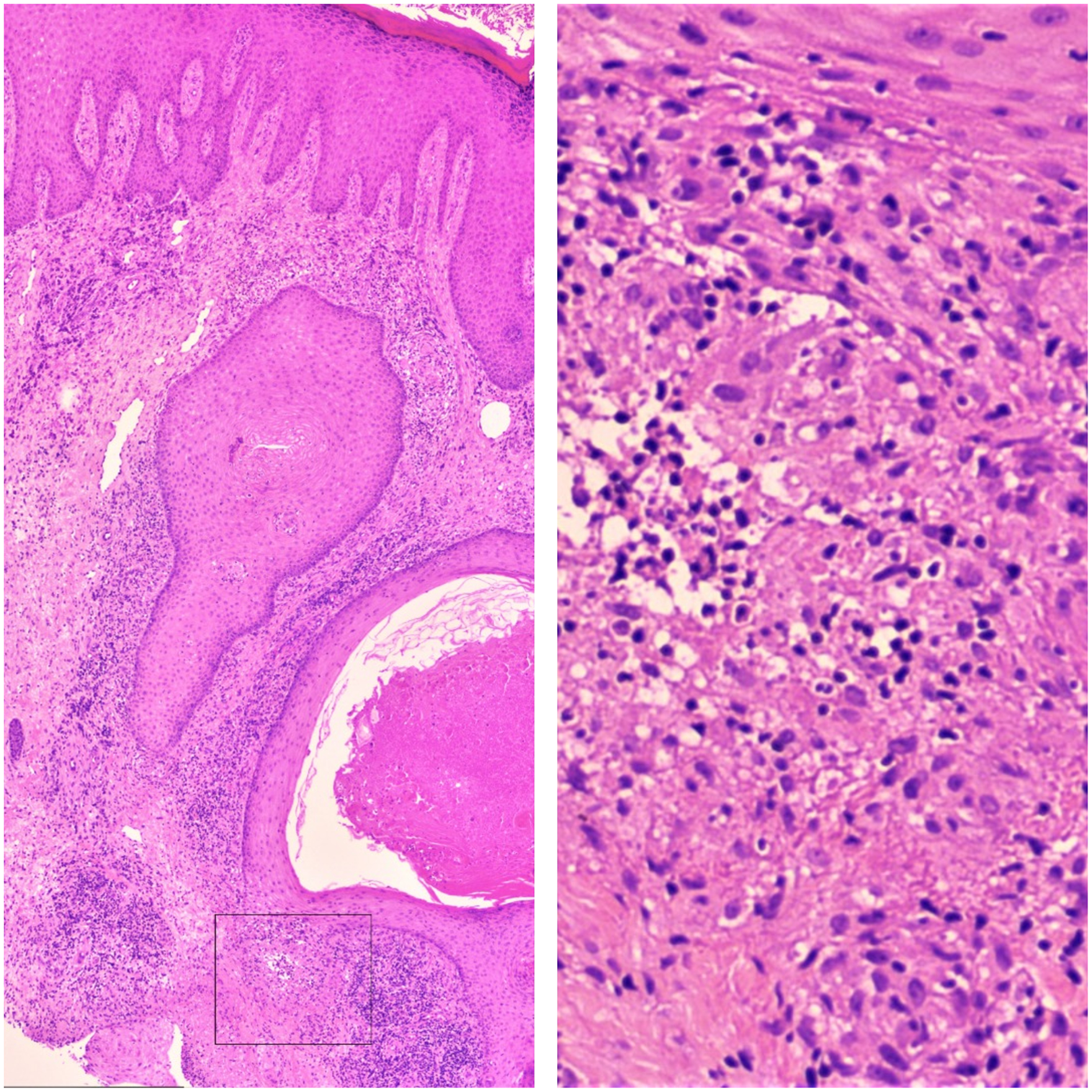
Histopathological slide.
After getting the tissue biopsy report, the joint board considered it as a fungal infection and started tablet itraconazole. After 1 month of the oral antifungal treatment, there were signs of improvement of the lesion (Figure 4) and we continued the antifungal medication along with the regular dressing of the wound for another 3 months. After 6 months, skin lesions were completely resolved (Figure 5). We followed up the case for another 6 months and there was no relapse or recurrence of the infection. The patient was discharged with the advice not to walk barefooted in the garden.

Clinical picture after 1 month of the treatment.

Clinical picture after 6 months of the treatment.
Discussion
Mycetoma is characterized by a combination of painless, firm subcutaneous mass, multiple sinuses, and purulent or serosanguinous discharge containing grains. It usually involves the skin, deep structures, and bone, culminating in deformity, destruction, and loss of function. 5
It was first reported in the mid-19th century in Madurai, India. Since then, it has been reported from all over the world with irregular consistency. The highest number of cases being reported from the “mycetoma belt.” Due to its slow progression, painless nature, lack of awareness of the disease, and scarcity of medical and health facilities in the endemic areas, many patients present late with advanced infection. The time between initial infection and consultation has been found to vary from 3 months to 50 years. This makes the existing suboptimal treatment strategy even more complicated leaving amputation as a last resort. 2 Moreover, diabetes, advanced age, and other immunocompromised conditions make the management even more challenging. Our patient was referred within 2 months of the appearance of the skin lesion. Thus, we can consider it as an early diagnosis.
Eumycetoma is predominant in tropical and subtropical regions of Asia (Mid-East, India) and Africa (Sub-Saharan Africa), whereas actinomycetoma is predominant in North Africa, Central, and South America and a few Asian countries. Though the disease is not contagious, relatives of an individual with mycetoma living in the same locality have an increased likelihood of developing mycetoma. Shared environmental factors and genetic or immunological predisposition are hypothesized to have a role in increasing the susceptibility to the disease. 5 Disease transmission occurs when the causative organism enters the body through minor trauma or a penetrating injury, commonly thorn pricks. Therefore, there is a clear association between mycetoma and individuals who walk barefooted and are manual workers. 3 Our patient had a history of working in the house garden barefooted with her husband. Her husband had a similar skin infection at the foot 1 year back which ended up with an amputation. This raised the suspicion that our patient was suffering from mycetoma infection of the foot.
During the initial phases, a hard, painless papule forms that increases in size to form mycetoma: a tumor-like growth. With time a chronic inflammation and a granuloma with zones of grains surrounded by neutrophils, macrophages, lymphocytes, plasma cells, and foreign body giant cells are formed which slowly destroys tissues and provides shelter for the organism. 5 Cell-mediated immunity plays a critical role in the immunity against mycetoma, with T-lymphocytes playing a central role by destroying the fungi and producing an immuno-protective status against the infection. To date, there are limited data available on the immune response to mycetoma infection and how patients can modulate their response against Madurella mycetomatis. However, patients who develop mycetoma seem to be deficient in their cell-mediated immunity. 5 T-helper (Th) type 1 lymphocyte responses provide protective immunity against mycetoma, whereas the progression of the disease is favored by the Th2 immune response (interleukin [IL]-4, IL-5, IL-6, and IL-10) in mycetoma patients. 6 As diabetic patients usually have compromised Th-1 response, they are vulnerable to develop a worse form of mycetoma. Usually, 3 host tissue reactions occur in mycetoma infection: neutrophil adherence, degranulation, and disintegration of grains; replacement of neutrophils with macrophages which engulf grain and neutrophil debris; and formation of epithelioid granuloma. As the tumor grows, sinus tracts form, soft tissue gets extensively involved and eventually, it involves down into the bone-producing osteomyelitis. Our patient had all the risk factors for developing complicated Madura foot as she was a diabetic patient with CKD. However, as she was diagnosed early, she recovered completely with treatment.
Secondary bacterial infection can occur in mycetoma, commonly with S aureus, Streptococcus pyogenes, or Proteus mirabilis. These coexisting deep-seated infections could contribute to the poor response to various antifungals and antibiotics. Elimination of these concomitant infections shortens the duration and improves the outcome of the treatment. Our patient was also presented with a concomitant S aureus infection.
The clinical presentation of eumycetoma and actinomycetoma is very much similar, with subtle differences. Therefore, the proper diagnosis of the cause is important as misdiagnosis may lead to the failure of the treatment. Ultrasound, Gram or PAS staining of discharge or crushed swab, fine-needle aspiration, or biopsy are preferred clinical investigations. X-ray, computed tomography scan, and magnetic resonance imaging are also useful to see the extent of the lesion and the invasion of structures. 5 In our case, PAS staining, and culture were not positive for fungus, but the histopathological report showed resemblance to mycetoma infection.
This disease is often diagnosed and treated by clinical observation. Early management of mycetoma when the lesion is small has a better prognosis. However, with time the treatment becomes complicated, time-consuming, and expensive. Moreover, recurrence is also common due to noncompliance to the treatment, and inadequate or the absence of response to antifungals and surgery. The azole class of antifungals and antibiotics is used to treat eumycetoma and actinomycetoma, respectively. 1 Our case responded well with 4 months of treatment with itraconazole and there was no relapse or recurrence after 6 months of the complete cure.
Prevention of mycetoma infection is difficult, but people living in or traveling to endemic areas should be advised not to walk barefooted as a preventive measure.
Conclusion
As mycetoma is prevalent among the poor population residing in remote areas of developing countries with inadequate reporting and management systems, they are advised to avert walking or working barefooted particularly in the garden. Early detection and proper treatment along with regular follow-up can manage this neglected problem efficiently with a promising outcome.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Acknowledgement
The authors acknowledge the department of histopathology for providing the pictures of the histopathological slides.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.