
Abstract
This study investigated the effect of early rehabilitation on gait restoration, wound healing, and home discharge in patients with lower extremity (LE) chronic wounds. This multicenter, retrospective cohort study included 233 Japanese inpatients who received treatment for LE chronic wounds from April 2012 to March 2015. A multivariate analysis was conducted using outcomes of gait restoration, wound healing, and home discharge as dependent variables. Other survey items were used as independent variables. Early rehabilitation was extracted as an independent factor with gait restoration (hazard ratio [HR] 1.82, P < .01) and home discharge (HR 1.77, P < .001) as dependent factors by the stepwise method in Cox proportional-hazards regression analysis, but it was not extracted as an independent factor with wound healing as the dependent factor by the stepwise method as well as the forced entry method (P = .44). A significant relationship between the presence of gait restoration and home discharge was observed in the chi-square test (P<.001), and the duration from admission to gait restoration was significantly correlated to the duration from admission to home discharge (Pearson's product-moment correlation coefficient; r=.89, P<.0001). Early rehabilitation was a positive factor for gait restoration and home discharge in chronic LE wound patients.
Keywords
Introduction
Lower extremity (LE) chronic wounds impair the patient’s quality of life and restrict activities of daily living because the feet are crucial for walking and standing.1,2 Diabetes is the main cause of LE chronic wounds, with worldwide patient numbers estimated to be more than 400 million and 8.5% of the adult population; 1 out of 4 diabetes patients will develop LE chronic wounds. 3 Therefore, LE chronic wound healing and the patient’s future life need to be regarded by medical professionals to extend longevity. Troublingly, patients with LE chronic wounds commonly have metabolic function and/or microcirculatory system diseases, such as diabetes and peripheral arterial diseases,2,4 and their average age is reported to be over 70 years in Japan. 5 Physical inactivity subsequently causes disuse syndrome, inclusive of muscle atrophy in the LEs and decreased physical endurance, leading to the loss of gait ability and restriction in community life. In addition, the loss of gait ability delays the patient's home discharge, 6 which further accelerates the decline in physical performance, as well as causes cognitive and psychological problems. 7 To prevent this, an early rehabilitation intervention is needed to stimulate the LE skeletal muscles for chronic wound patients. While external forces on the wound site impair healing, 8 various materials and devices such as formed orthotic insoles, leg-length walking cast boots, and total contact casting have been recently utilized in the clinical setting to offload foot ulcers,8,9 enabling the patient to continue using the skeletal muscles in the wounded LE. Therefore, early rehabilitation interventions are expected to coincide with wound treatments for patients with LE chronic wounds. However, the effect of early rehabilitation on physical performance and wound healing has not been reported in these patients. We, therefore, analyzed the relationships between early enforcement of a rehabilitation intervention with gait restoration, wound healing, and home discharge in LE chronic wound patients in a multicenter, retrospective study.
Methods
Study Design and Participants
This retrospective cohort study was conducted in 233 consecutive Japanese inpatients admitted to 6 hospitals of Oita Oka Hospital, Kasukabe Central General Hospital, Kita-Harima Medical Center, Shin-Suma Hospital, Yao Tokushukai General Hospital, or Yokohama General Hospital for the treatment of LE chronic wounds from April 2012 to March 2015. In order to analyze wide kinds of data on rehabilitation initiation to clarify the effect on each outcome, we selected a multicenter investigation. The study included patients who were hospitalized for the treatment of LE chronic wounds arising from peripheral arterial disease and/or diabetes on the plantar surface of the foot, underwent rehabilitation during hospitalization and walked daily without a foot prosthetic before the ulceration. Patients who had ulcers associated with lymphedema or venous stasis; those who developed an infection after peripheral revascularization or wound surgery, including amputation; those who had a persistent infection after debridement of an infected lesion; those who had an amputation above the Lisfranc joint; and those who died during hospitalization were excluded. The therapeutic strategy for wound healing was determined via discussion between the medical doctors, nurses, physical therapists, occupational therapists, and prosthetists in all the hospitals. Basically, the necrotic and/or infected tissues were surgically debrided, and revascularization procedures were conducted for ischemic wounds to promote healing and avoid major amputation. Standard wound care was ensured by the doctors and well-trained nurses. During rehabilitation, patients performed exercises under the supervision of physical and/or occupational therapists, and the duration of intervention was determined by the medical staff depending on the patient’s condition each day.
Investigation
Patient characteristics and clinical parameters representing relationships between wound healing and physical function were investigated.10–15 These included age (binarized by the median); sex; height; body weight; comorbidity; examination of blood albumin (binarized by 3.0 g/dL), C-reactive protein (binarized by 5 mg/L), and white blood cells (binarized by 10,000/μL); history of undergoing wound care; time duration after wound occurrence (binarized by 1 week before hospitalization); independence in activity of daily living indoors before hospitalization; the presence or absence of chronic obstructive pulmonary disease; cerebral vascular accident (CVA); dementia; malignancy; cardiac disorder; dialysis; psychiatric disorder; critical limb ischemia (CLI); diabetes; diabetic neuropathy; foot deformity; lower limb amputation; infection requiring tissue removal; osteomyelitis; deep wound (full-thickness dermis ulcer); multiple wounds and wound location (forefoot or other); and start date of rehabilitation. The following outcomes were investigated: the presence or absence of gait restoration during hospitalization and the date when gait restoration was achieved (Investigation I); the presence or absence of wound closure during hospitalization and the day when all wounds healed in each patient (Investigation II); and home discharge (Investigation III). All data were collected from medical records in each hospital.
Determination of Gait Restoration and Wound Healing
The patient's gait was considered restored when they could walk in the hospital ward with/without a walker or cane,16,17 as recorded by the physical therapists or occupational therapists. To evaluate the effects on wound healing, wound closure was identified by Board Certified Specialists of Plastic & Reconstructive Surgery at each hospital.
Definition of Early Rehabilitation
Early enforcement of the rehabilitation intervention refers to its commencement prior to the median of the initiation date. We determined the initiation date of the rehabilitation intervention to be when patients started standing exercises, which included standing up and wheelchair transfer using their LE, under the supervision of the physical or occupational therapists. This was to differentiate the rehabilitation intervention from nonactive exercises on the bed only and to minimize the effect of different exercise prescriptions customized for each individual. The date determined by this criterion reflected the earliest date of active exercise for each patient because, to prevent falls, the patients were not allowed to perform movements in the hospital ward that were more difficult than those performed during training with the physical therapist or occupational therapist. As for the rehabilitation process, physical therapists are involved in rehabilitation in order to regain basic motions like sitting-up and standing-up, while occupational therapists are mainly involved in activities of daily living like eating, toilet, and bathing activity. These 2 kinds of therapists assist the patient's rehabilitation in cooperation, and the motions of gait and wheelchair transfer can be considered as a basic motion as well as an activity of daily living. 17 Therefore, we investigated the initiation date of the rehabilitation intervention by physical therapists or occupational therapists. These therapies were generally prescribed concurrently, and each therapy was conducted for 40 to 60 min, resulting in 1 to 2 h rehabilitation a day. This duration and strength were gradually increased and flexibly adjusted with consideration for the patient's medical condition and endurability. Basically, patients were firstly encouraged to acquire the motions of sitting up and standing, followed by aerobics exercises like gait and bike. Off-loading devices were applied for patients for whom the necessity was deemed by medical doctors, physical and occupational therapists, and prosthetists/orthotists.
Analysis
A multivariate analysis (stepwise method) was carried out using the outcomes of gait restoration, wound closure, and home discharge as dependent variables. Other survey items were used as independent variables. Gait restoration, wound closure, and home discharge were analyzed by a multivariate Cox proportional-hazards regression model. The relationships among dependent variables were analyzed by the chi-square test and Pearson's product-moment correlation coefficient. Logistic regression analysis was additionally used to investigate the relationship among survey items. The necessary sample number was calculated to be 200 since the sample number of 10 should be included per an independent variable in both groups of the event and nonevent group in Cox proportional-hazards regression model. 18 We estimated the factors which would be extracted by the stepwise method as 5 to 10 items, hence selecting the 8 for the estimated number of independent items, and estimated the ratio of the number in the event and the nonevent group was 4:6, resulting in 200 patients. EZR (Saitama Medical Center, Jichi Medical University) 19 was used for the statistical analysis, and the significance level was P < .05.
Ethics
This research was approved by the ethics committee of the Kobe University Graduate School of Health Sciences, and informed consent was obtained by the opt-out method on each hospital website (patients who did not want researchers to use their medical data had to opt-out; otherwise, consent was implied).
Results
Patient Characteristics and Starting Date of Rehabilitation
The number of eligible patients was 233. Patient characteristics and clinical parameters are shown in Table 1. A total of 231 patients underwent the rehabilitation intervention, and the median of the starting date was day 13 after admission. Hence, we defined the beginning of the rehabilitation intervention within 2 weeks after admission as early rehabilitation and added this as an independent variable in the following analysis.
Demographics and Clinical Parameters of the Enrolled Patients.
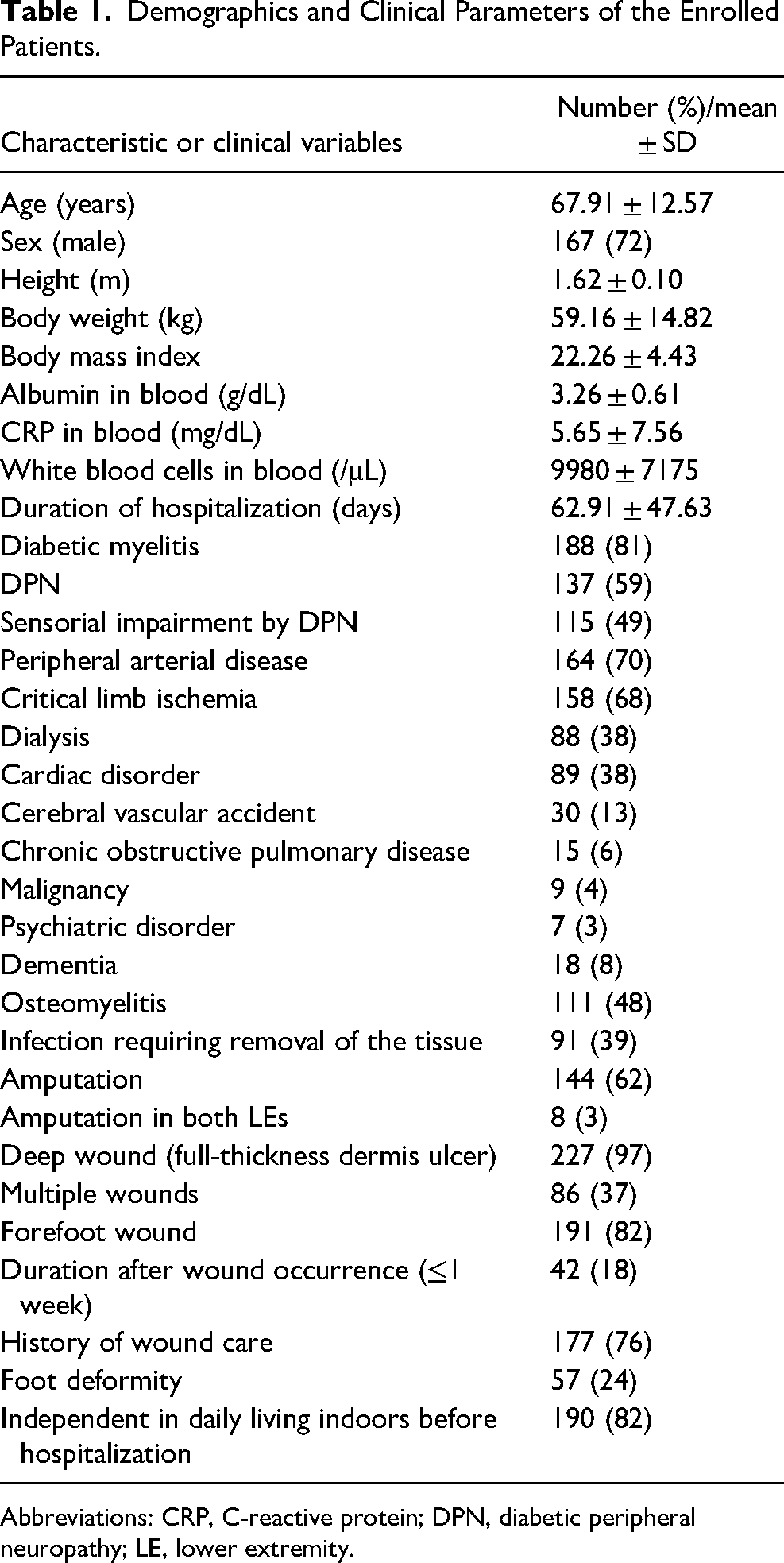
Abbreviations: CRP, C-reactive protein; DPN, diabetic peripheral neuropathy; LE, lower extremity.
Gait Restoration (Investigation I)
In order to examine the influence of early rehabilitation on gait restoration among eligible patients, we set additional minor exclusion criteria of patients who (1) underwent bed exercises only during hospitalization, (2) could walk before the rehabilitation intervention, and (3) could not confirm the exact numerical values of blood test data, resulting in the inclusion of 204 subjects (Figure 1A). Of the eligible patients for this analysis, 127 patients achieved walking during hospitalization. In the Cox proportional-hazards regression analysis with gait restoration as a dependent factor, 7 independent factors including early rehabilitation (hazard ratio [HR] 1.82, P < .01) were extracted by the stepwise method (Table 2).
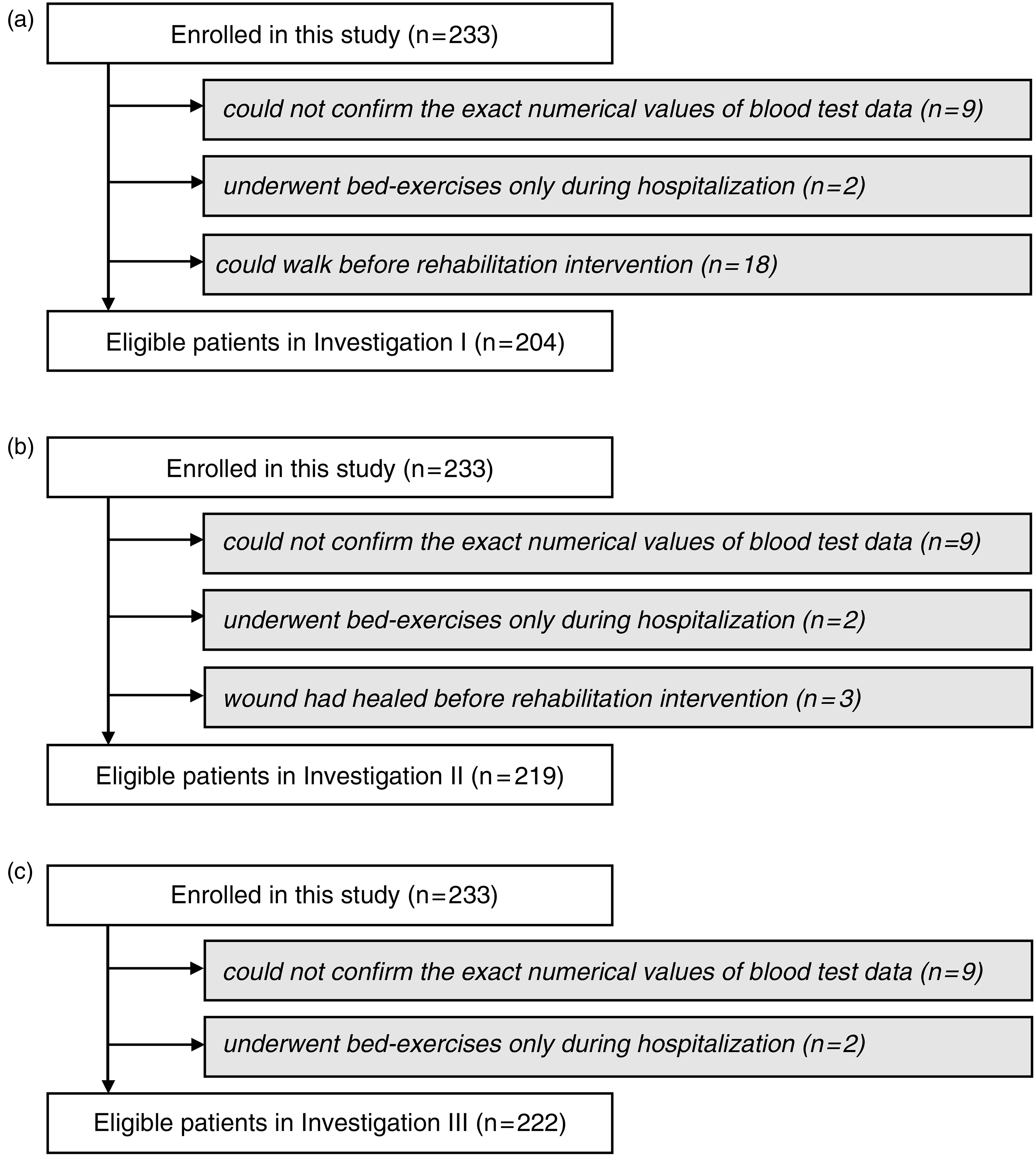
Flowcharts of patient selection. The flowcharts display the patient flow during (A) Investigation I, (B) Investigation II, and (C) Investigation III.
Extracted Independent Factors for Gait Restoration by the Stepwise Method in the Cox Proportional-Hazards Regression Analysis.
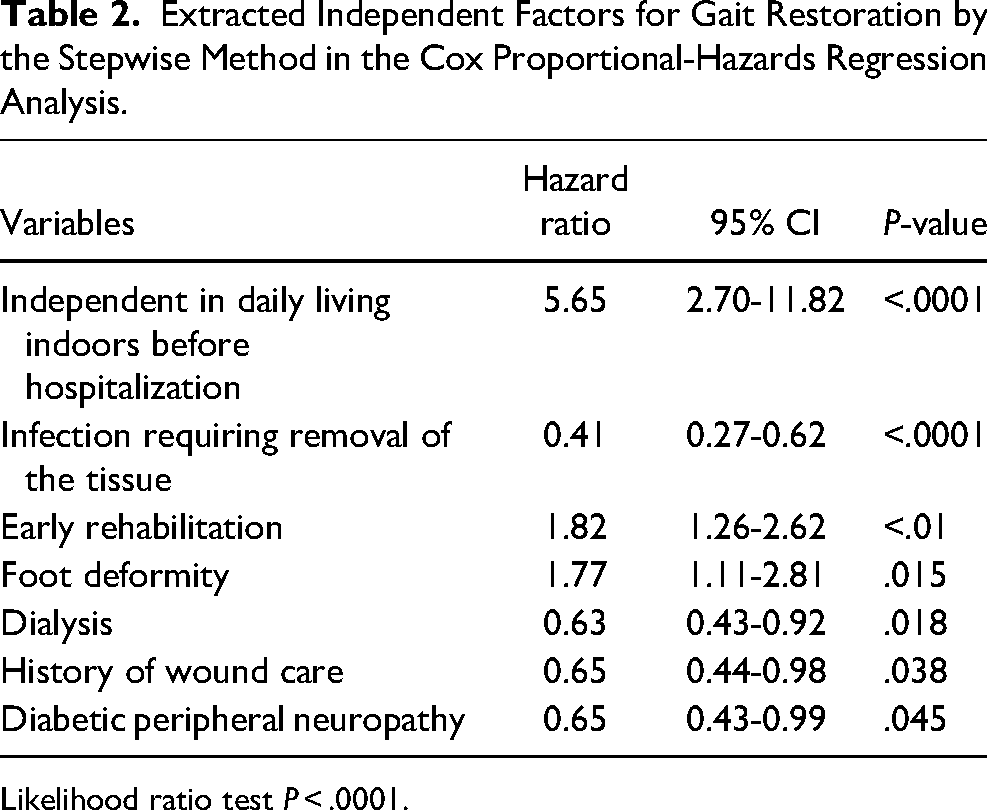
Likelihood ratio test P < .0001.
Wound Closure (Investigation II)
Patients (1) who underwent bed exercises only during hospitalization, (2) whose wounds had healed before the beginning of the rehabilitation intervention, and (3) whose exact numerical values of blood test data could not be confirmed were excluded to investigate the effect of early rehabilitation on wound closure (Figure 1B). In total, 219 patients were included, and the wounds of 98 patients healed during hospitalization. Based on the results from the Cox proportional-hazards regression analysis using wound closure as a dependent factor, 10 independent factors were extracted, in which early rehabilitation was not included (Table 3). To clarify the involvement of early rehabilitation with wound healing, we conducted this analysis by the forced entry method using 10 extracted factors and early rehabilitation, which showed early rehabilitation is not an independent factor for wound closure (Table 3, P = .44).
Extracted Independent Factors for Wound Healing by the Stepwise Method (Left) and the Forced Entry Method (Right) in the Cox Proportional-Hazards Regression Analysis.
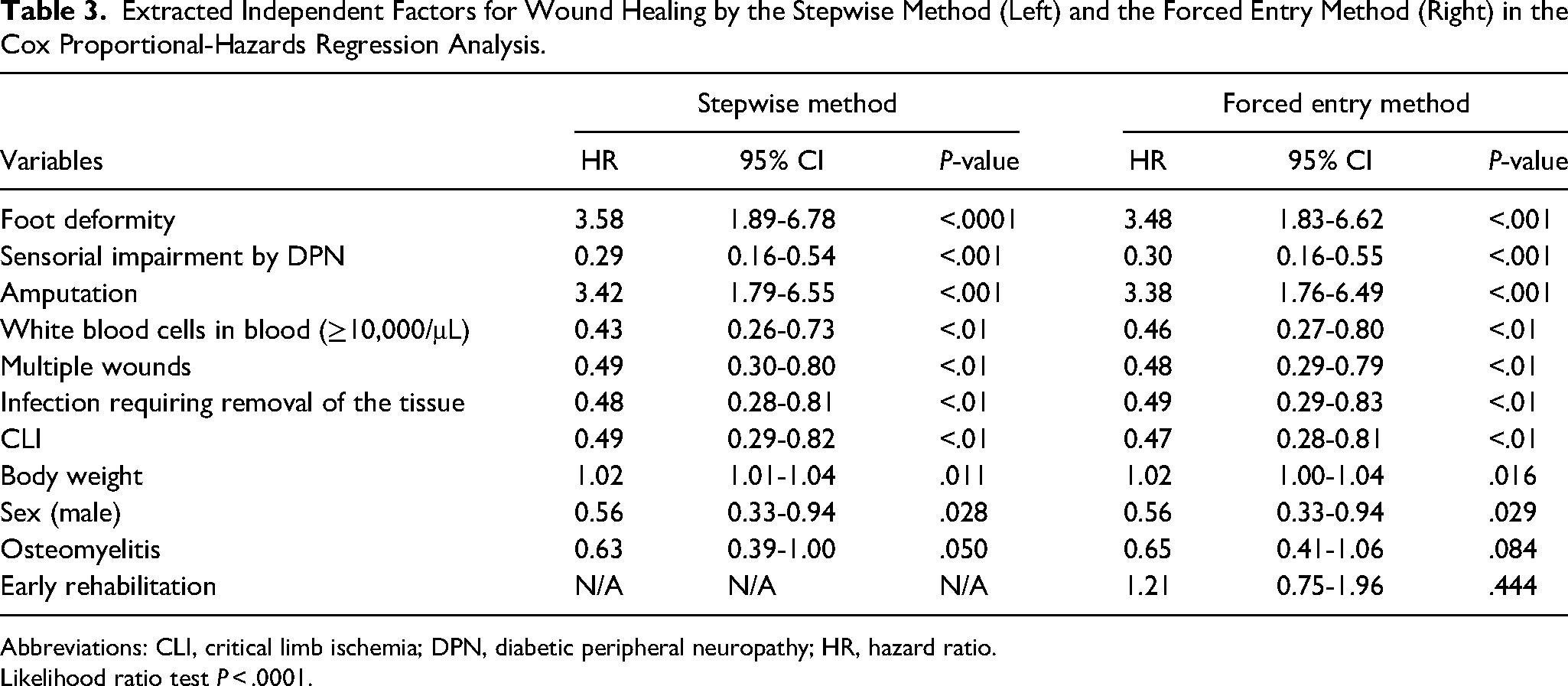
Abbreviations: CLI, critical limb ischemia; DPN, diabetic peripheral neuropathy; HR, hazard ratio.
Likelihood ratio test P < .0001.
Home Discharge (Investigation III)
Patients (1) who underwent bed exercises only during hospitalization and (2) whose exact numerical values of blood test data could not be confirmed were excluded to investigate the effect of early rehabilitation on home discharge (Figure 1C). A total of 222 patients were included, and 185 patients were discharged home. Based on the result from the Cox proportional-hazards regression analysis with home discharge as a dependent factor, 10 independent factors including early rehabilitation (HR 1.77, P < .001) were extracted using the stepwise method (Table 4).
Extracted Independent Factors for Home Discharge by the Stepwise Method in the Cox Proportional-Hazards Regression Analysis.
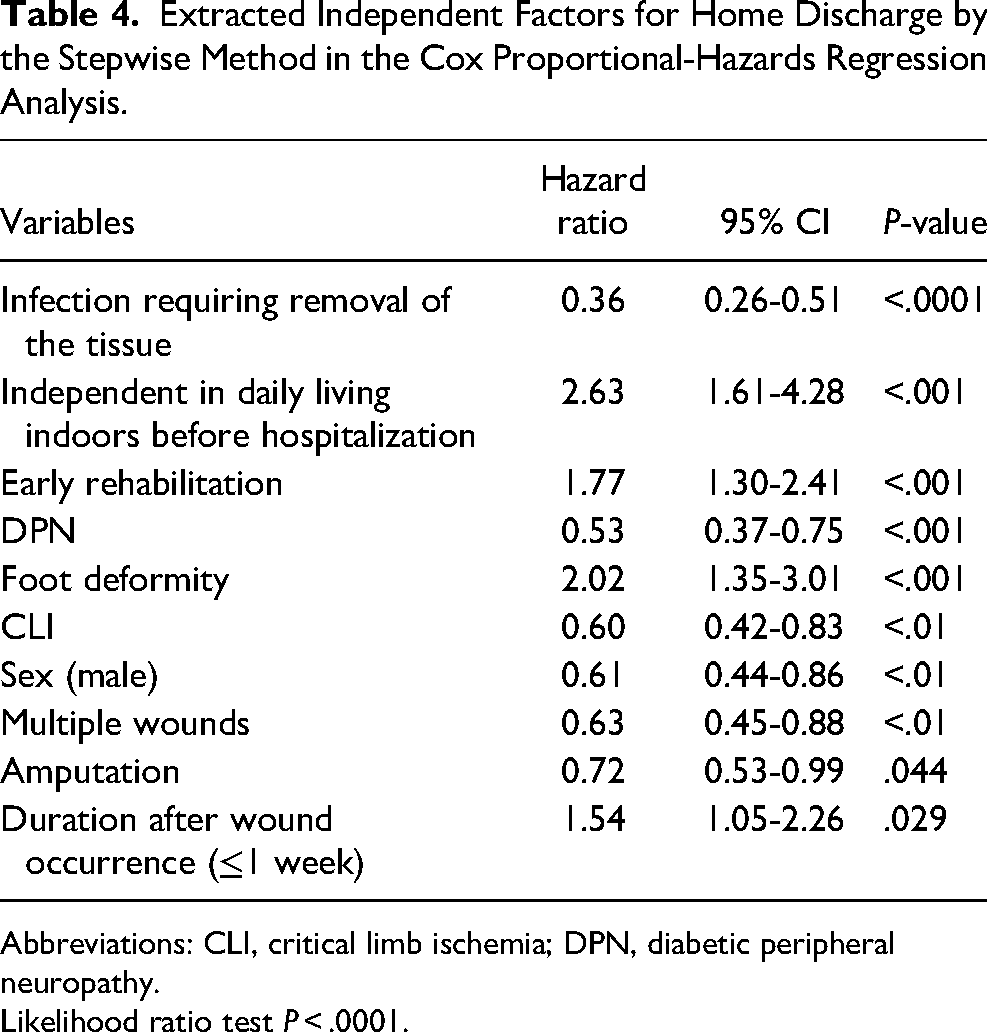
Abbreviations: CLI, critical limb ischemia; DPN, diabetic peripheral neuropathy.
Likelihood ratio test P < .0001.
Relationship Between Gait Restoration and Home Discharge
Early rehabilitation was found as an independent factor for gait restoration and home discharge. To clarify the relationship between these outcomes, we investigated the event occurrence of gait restoration and home discharge in all 233 eligible patients and the duration from admission to gait restoration and home discharge in 131 patients who achieved gait restoration and home discharge. Of the patients who achieved gait restoration during hospitalization, 90.3% were discharged home, while among those who did not achieve gait restoration, 69.6% were discharged home, resulting in a significant relationship between home discharge and gait restoration in the chi-square test (P < .001). Duration from admission to gait restoration significantly correlated to duration from admission to home discharge (Figure 2; Pearson’s product-moment correlation coefficient; r = .89, P < .0001).
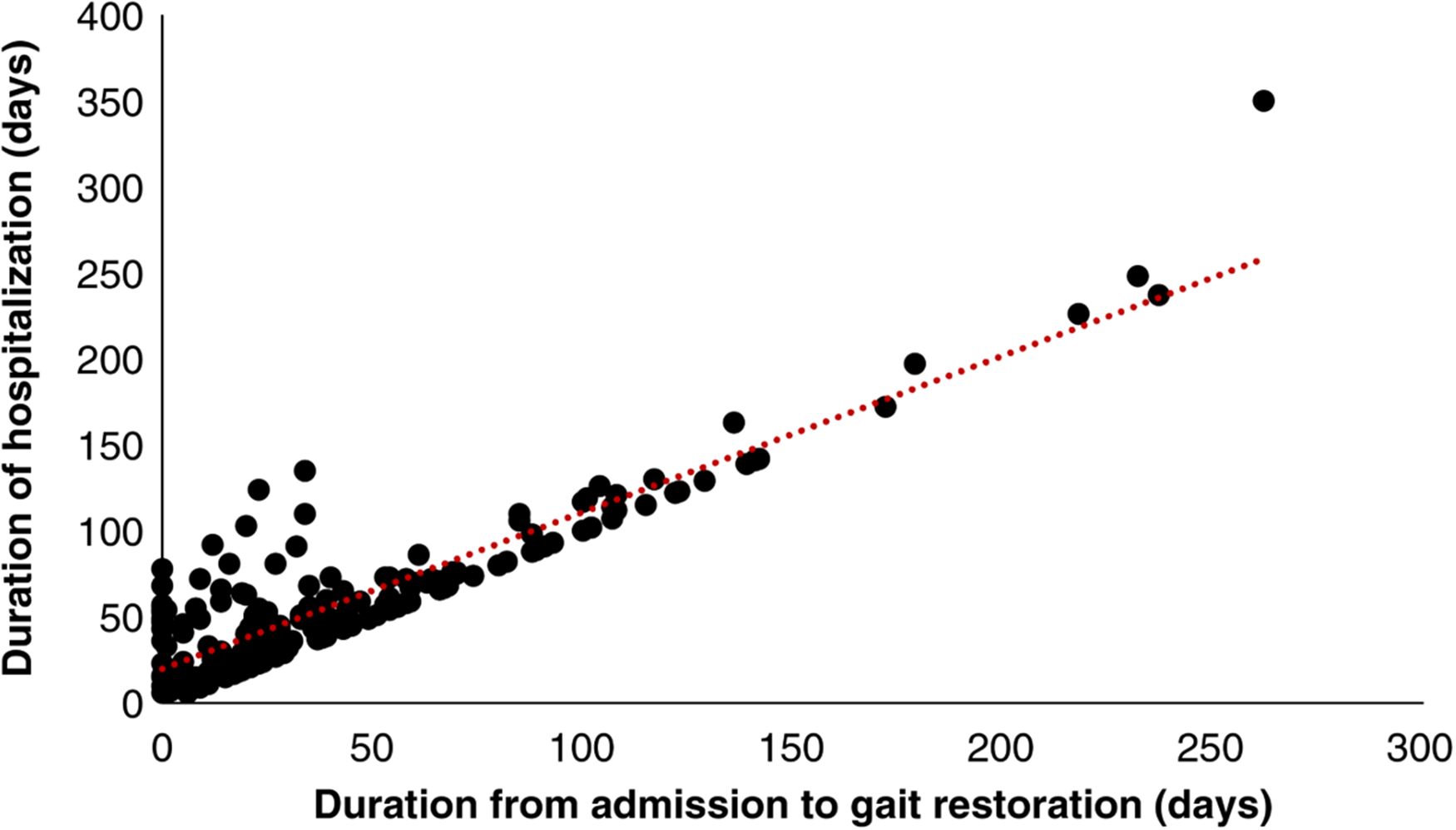
Correlation graph of the duration of hospitalization versus duration from admission to gait restoration.
Discussion
We investigated the relationship between the rehabilitation process with gait ability, wound closure, and home discharge and demonstrated the positive involvement of early rehabilitation for the prevention of lost gait and home discharge. This is the first report showing the clinical significance of early rehabilitation on LE chronic wound patients.
We found early rehabilitation is an independent factor to regain gait ability in daily life of LE chronic wound patients. Early rehabilitation is recommended to prevent the progression of disuse syndrome in several kinds of diseases 20 and is generally conducted with the expectation of a preventive effect on muscular dysfunction.21–24 As for diabetes patients, decreased neuromuscular function has been reported in both type 1 and type 2 diabetes. 25 Furthermore, loss of LE muscle strength in DPN patients has been reported in Japan. 26 For peripheral arterial disease (PAD) patients, a negative relationship between ischemia and the cross-sectional area in the calf muscle 27 and an association between ankle-brachial pressure index and muscle weakness were reported. 28
In the present study, we recruited patients with LE chronic wounds derived from diabetes and/or PAD, predominant diseases of CLI. Of the recruited patients, 81% had diabetes, and 72% of diabetes patients presented with DPN. In addition, 68% of all subjects were CLI patients. Furthermore, the average age of all the subjects was above 65 years, which is reported to be a factor for muscle atrophy by sarcopenia. 29 Therefore, most subjects were at risk for muscle atrophy upon admission. Gordon et al 30 reported resistance and aerobic training improve muscle strength as well as glycemic control and blood pressure in diabetes patients; Allet et al 31 reported the effect of balance and strength training on muscle strength and gait speed in the same. In addition, exercise training can improve the body function in PAD patients. It is known that exercise not only increases physiologic parameters and walking distance but also improves the cardiovascular risk profile in patients with PAD. 32 These reports support the usefulness of rehabilitation interventions for the recovery from physical deconditioning, including muscle weakness, in diabetes and PAD patients. In the present study, we found early rehabilitation to be a promoting factor for gait restoration, consistent with results for other diseases. This rehabilitation was defined by the intervention with standing exercises wherein patients used their LE skeletal muscles. Although we could not measure the muscle strength of the patients in the present study, early rehabilitation was successful as an exercise program for the LE skeletal muscles; moreover, this intervention promoted gait restoration by minimizing disuse syndrome in diabetes and CLI patients. Interestingly, early rehabilitation was also one of the promoting factors for home discharge in LE chronic wound patients. In addition, gait restoration during hospitalization was positively related to home discharge, and the duration before gait restoration and that before home discharge could be correlated. Therefore, rehabilitation aimed at early gait restoration can be considered a supportive intervention for the patient’s future social life.
In the present study, we found that early rehabilitation did not relate to wound healing. Based on guidelines for early rehabilitation in CVA patients, appropriate management of blood pressure is considered crucial. 33 This means that management affecting patient pathology must be performed in rehabilitation. In LE chronic wound patients, the major factors which affected wound healing were blood flow into the wounds, unwanted external force to wounds, and infection. 8 In Investigation II in the present study, 72.8% of CLI patients underwent revascularization, and 80.5% of the remaining CLI patients underwent amputation and/or debridement. This means that most patients who did not have enough blood flow to the wound site were appropriately treated by medical care.
With regard to the effect of external force management on wound healing, the use of foot offloading devices is known to be an important strategy for successful rehabilitation without wound damage. In the present study, 60% of patients had foot offloading devices applied, suggesting the application was based on patient background. Additional multivariable logistic regression analysis was performed, applying the usage of a foot offloading device as a dependent factor and extracting 6 factors, which included CLI, sensory impairment by DPN, foot deformity, and blood WBC count (≥10,000/μL) as positive independent factors (Supplemental Table S1). Although the present study does not clarify the best point of view to determine the relationship of offloading devices to LE chronic wound patients, the application of these devices to patients is important to represent the effect of early rehabilitation on gait restoration without unfavorable effects on wound healing.
In the analysis of gait restoration and wound healing, foot deformity was extracted as an independent factor with an HR higher than 1.0. Since a foot deformity is widely known as a risk factor for foot ulcer development, the presence of a foot deformity is supposed to interfere with wound healing. In the present study, hammer/claw toes accounted for approximately half of foot deformities (Supplemental Table S2). It is known that patients with this deformity easily develop toe ulcers, and toe ulcers heal earlier than midfoot and heel ulcers. 11 In addition, ulcer development on the toes was not distinguished from those on other forefoot areas in the present study. Thus, the positive involvement of foot deformity could be controlled by a confounding factor like the location of the ulcers. The present study also found that amputation was extracted as an independent factor with an HR higher than 1.0 on wound healing. In Baumfeld’s report, the healing duration in patients with amputation was shorter than patients without amputation, while that in patients with debridement was longer than patients without debridement in hospitalized patients due to complications of the diabetic foot. 34 Therefore, the amputation might shorten the healing time of LE patients through the process of primary treatment. As for the effect on gait restoration, amputation was not extracted as an independent factor. Meanwhile, the HR of amputation was 0.73 (P = .1) in the force entry method with 7 factors extracted in the stepwise method, and that in univariable analysis was 0.68 (P = .039). These data from additional analysis suggest the feasibility of minor amputation as the inhibitory factor on the patient's physical performance. Further detailed investigations are needed to know the effect of foot deformities and amputation on physical performance and wound healing. In addition, the present study detected the high HR of independence in activity of daily living indoors before hospitalization on gait restoration. We selected this item for analysis on the outcomes referring to the reports related to activity level, wound healing, amputation, and life prognosis.12,14,35,36 Therefore, the present study supported the previous reports, and determined the independence in activity of daily living indoors was a strong factor to predict the successful rehabilitation. Meanwhile, early rehabilitation was extracted as a positive factor on gait restoration as well as independence in activity of daily living indoors, supporting the importance of early rehabilitation on gait restoration for the patients who were dependent or independent in their daily life before hospitalization.
The present study has limited evidence of early rehabilitation on these patients because it was a retrospective study. The effect of earlier rehabilitation immediately or a week after administration could not be assessed because we adopted a period of 2 weeks to initiate rehabilitation by referring to the median in the present study. In addition, we could not analyze the dependency of the type of exercise and the volume on each outcome. To clarify the effectiveness of early rehabilitation intervention, the ideal timing to begin rehabilitation, and the effective contents of exercise in chronic LE patients, prospective studies need to be conducted in future.
In conclusion, we clarified the positive relationships of early rehabilitation with gait restoration and home discharge in chronic LE wound patients. This is an important finding to support patient's lives after ulceration. The findings need to be further investigated by randomized controlled trials in the future.
Supplemental Material
sj-docx-1-ijl-10.1177_15347346211039588 - Supplemental material for Effect of Early Rehabilitation on Gait, Wound and Home Discharge in Lower Extremity Chronic Wound Patients: A Japanese Multicenter Retrospective Study
Supplemental material, sj-docx-1-ijl-10.1177_15347346211039588 for Effect of Early Rehabilitation on Gait, Wound and Home Discharge in Lower Extremity Chronic Wound Patients: A Japanese Multicenter Retrospective Study by Noriaki Maeshige, Ph, Hisae Hayashi, PhD, Hiroto Terashi, PhD, MD, Miki Fujii, PhD, MD, Tetsuya Iwamoto, PhD, Yu Watanabe, MSc, Shinsuke Imaoka, MSc, Junichi Matsumoto, MSc, Mayo Nishikawa, BSc, Naoto Takeda, BSc, Ryuzo Mikawa, BSc, Yoriko Tsuji, PhD, MD, Ryuji Higashita, PhD, MD, Shinobu Ayabe, MD, Yuta Terabe, MD, Masahide Furukawa, MD, Junko Tanaka, PhD, MD, Takehiko Ohura, PhD, MD, Nobuhide Kawabe and PhD in The International Journal of Lower Extremity Wounds
Footnotes
Acknowledgments
The authors thank the staff members of Kasukabe Central General Hospital, Oita Oka Hospital, Kita-Harima Medical Center, Shin-Suma Hospital, Yao Tokushukai General Hospital, and Yokohama General Hospital who collaborated in this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the MHLW Research Program for Intractable Disease (grant no. 201611007A). The results of this study were presented at the annual congress of the Japanese Society of Limb Salvage & Podiatric Medicine 2017.
Ethical Approval
This research was approved by the ethics committee of the Kobe University Graduate School of Health Sciences, and informed consent was obtained by the opt-out method on each hospital website.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.