
Abstract
It is necessary to know the resistance profile of Staphylococcus aureus to better control diabetic foot ulcer infections, to establish rational antibiotic therapy, and to avoid the development of resistant strains. This cross-sectional study evaluated the clinical parameters, virulence, and antimicrobial resistance profiles of S aureus in patients with diabetic foot disease admitted to a public hospital. S aureus strains were identified in patients with diabetes with amputation indication. Infected tissue samples were collected, microbes were isolated and identified. The microbial resistance profile was determined. Samples were also analyzed for biofilm formation and other virulence markers. The 34 individuals examined were mostly men, black, aged 60 years on average, and generally had a low income and education level. Most individuals had type 2 diabetes, and the mean time since diagnosis was 13.9 years. On an SF-36 (the Medical Outcomes Study 36-item short-form health survey) quality-of-life questionnaire, 75% of individuals obtained a score equal to 0 for physical impairment. S aureus specimens from 17 patients were isolated, corresponding to 50% of samples. Five isolates were classified as methicillin-resistant S aureus (MRSA). Molecular typing revealed that 20% of MRSA strains were SCCmec type V and 80% were type I. All isolates were sensitive to doxycycline; 61.5% were resistant to erythromycin, 38.5% to cefoxitin, 30.7% to clindamycin and ciprofloxacin, 23% to meropenem, 15.3% to gentamicin, 38.5% to oxacillin, and 7.7% (one strain) to vancomycin. Regarding biofilm production, 53% of samples were able to produce biofilms, and 84.6% had icaA and/or icaD genes. Additionally, the following enterotoxin genes were identified in the isolates: seb, sec, seg, and sei (5.9%, 5.9%, 11.8%, and 23.9%, respectively) and agr types 1 (5.9%) and 2 (11.8%). Genotypic evaluation made it possible to understand the pathogenicity of S aureus strains isolated from the diabetic foot; laboratory tests can assist in the monitoring of patients with systemic involvement.
Introduction
Diabetes mellitus (DM) is a chronic disease that presents with a persistent increase in blood glucose levels, pancreatic insufficiency, and dysfunction of receptors in metabolic pathways, or a combination of these. The incidence of DM is increasing worldwide; it is estimated that 415 million individuals are affected by the disease. This is strongly correlated with genetic variations and environmental factors, especially with lifestyle; diabetes is considered an epidemic of the 21st century. 1 Diabetes gives rise to other diseases, by way of successive attacks on the epithelium of organs and tissues. 1 The continual increase in glycemia results in a saturation of the glucose-uptake receptors, and in addition to the direct aggression of excess glucose, the glycosylation of proteins causes numerous complications, such as renal failure. 2 DM takes a chronic progressive course; to maintain patient care, laboratory tests provide monitoring of affected patients.
According to the World Health Organization, hyperglycemia is the third determining factor of premature mortality, as it favors the development of chronic micro- and macrovascular DM complications, including diabetic foot, retinopathies, renal failure, neuropathies, coronary disease, cerebrovascular disease, and peripheral arterial disease. 1 Diabetic foot syndrome is characterized by reduced sensitivity to pain in the lower limbs. This remarkable characteristic may be attributable to the presence of neuropathies due to peripheral arterial disease, which in more severe cases can culminate in the removal of the affected limb. 3 In the United States, infected foot ulcers in patients with diabetes are the leading cause of non-traumatic amputations. In line with this, in 2014, the prevalence of 29.1 million people with DM in the USA was verified, representing about 9.1% of the total population. 4 In studies in Brazil, the prevalence of DM varied from 7.6% to 20%, with a higher prevalence in females and in individuals with no education or with incomplete elementary education 5 . The cost of treating the number of people affected by diabetic foot ulcers (DFUs) surpasses that of cancer, depression, and lung diseases, highlighting the importance of optimizing treatment. 6 The main etiological agents of the chronic profile of infections in DFU are Escherichia coli, Pseudomonas aeruginosa, and Staphylococcus aureus. The latter is considered the main cause, as it is present in the skin microbiota of most healthy individuals and may opportunistically manifest as a disease.4,6
S. aureus is a Gram-positive bacterium that produces several virulence factors, including exfoliatins (ETA and ETB), enterotoxins (eg, SEA, SEB, and SEC is Staphylococcal enterotoxin A, B and C), toxic shock syndrome toxin, and Panton–Valentine leucocidin (PVL), which may contribute to diseases such as septicemia, endocarditis, impetigo, boils, folliculitis, and osteomyelitis.6,7 Molecular biology techniques help in identifying genes to determine antimicrobial-resistant strains, such as mecA, which confers low sensitivity of microorganisms to the antimicrobials used in clinical practice.8,9 At the beginning of S aureus infection in DFUs, surface proteins are produced that facilitate bacterial adhesion to the host's skin tissue. Once adhered to the tissue, the microorganism may produce polysaccharides that coat the bacterium, representing an essential component for the development of what is called biofilm.10,11 Bacteria that make up the biofilm have a higher tolerance to antibiotics, which plays an important role in antimicrobial resistance. Several genes are involved in the initiation and maintenance of staphylococcal biofilms. Among these, the most widely studied are icaA and icaD, which are associated with polysaccharide intercellular adhesin, which contains N-acetylglucosamine, one of the main components of the exopolysaccharide matrix that involves bacterial cells in biofilms. 12
Knowing the prevalence of S aureus biofilm colonization in DFUs is of great importance, since the mode of biofilm growth in infectious organisms compromises the host's immune system; the biofilm growth of S aureus is thus becoming an important contributor to the chronicity of ulcers 13 in addition to S aureus being highly resistant to antimicrobial therapy. Empirical antibiotic therapy is the primary treatment regimen for infection of DFUs. In practice, for patients who do not present with risk factors for infection by pathogens that are unusual or resistant to empirical treatment, beta-lactam antibiotics such as penicillin and first-generation cephalosporins are administered. For those at risk of infection by resistant pathogens, treatment may involve broad-spectrum beta-lactams, beta-lactamase inhibitors, carbapenems, or cephalosporins of the latest generation. 14
The prevalence of methicillin-resistant S aureus (MRSA) in diabetic foot ulcer infections varies between countries and is higher in patients receiving prolonged antibiotic therapy for a chronic evolution of diabetic foot infection, or hospitalized patients who have had an anterior amputation. 14 Eleftheriadou et al (2010) stated that the prevalence of MRSA among patients with diabetic foot ulcer infections varies between 15% and 30%. 15 MRSA infection is a worrying factor, since the time for ulcer healing is longer in MRSA patients than in patients infected by other microorganisms. 15 Garcia et al (2015) observed that patients with MRSA-infected ulcers took 1 to 3 months to heal, while ulcers infected with methicillin-sensitive S aureus (MSSA) took 15 days to 1 month to heal. 16 From this perspective, it is necessary to know the local microbiota and the resistance profile of S aureus to better control diabetic foot ulcer infections, to establish rational antibiotic therapy, and to avoid the development of resistant strains. 4
In view of the above, this study aimed to assess the clinical parameters, virulence genes, antimicrobial resistance profiles and associated genes, phenotypic forms, and biofilm formation capacities of strains of S aureus in patients with diabetic foot disease admitted to a regional public hospital.
Methodology
Study Design
This was an observational, cross-sectional study, carried out with 34 patients selected according to their medical history at the hospital in question, in 2017 and 2018. The study was approved by the Human Research Ethics Committee (08731912.5.0000.5556). All participants agreed to participate in the study by providing their written informed consent.
Sociodemographic Data and Assessment of Style and Quality of Life
Socio-demographic, epidemiological, and lifestyle data were collected using a systematic questionnaire. This comprised the medical history regarding the patient's history of diabetes, follow-up, and treatment; aspects related to diabetic foot complications were specifically included. In assessing the quality of life (QOL), we used the SF-36 (the Medical Outcomes Study 36-item short-form health survey), which was translated and validated for the Brazilian context by Ciconelli et al. 17 SF-36 is a questionnaire that assesses eight aspects of an individual's life (functional capacity, physical, social, and emotional aspects; pain, general health, mental health, and vitality) using scores ranging from 0 to 100, where 100 represents the highest index, reflecting the optimal state for that aspect. 17
Vascular and Physical Examination
For ankle brachial index (ABI) analysis, systolic blood pressure (SBP) was measured. For this, we used a portable vascular Doppler device (DV 610, Med Mega) and an aneroid sphygmomanometer. The pressures were obtained for the brachial arteries, as well as for the dorsalis pedis and posterior tibial arteries, both left and right. The highest systolic pressure measurement was used to calculate ABI. The value was obtained by dividing the highest SBP obtained in each artery of the lower limbs by the highest SBP obtained in the upper limbs, according to the formula: ABI = SBP ankle/SBP brachial. ABI values between 0.91 and 1.29 were considered normal, while those <0.9 or >1.3 were considered abnormal. 18
Lesions were evaluated for depth, systemic repercussion, and the presence of local inflammatory signs, thus allowing them to be classified according to the Wagner, the University of Texas, and the PEDIS scales.19,20 The Semmes–Weinstein test with a 10-g monofilament was used to assess tactile sensitivity, as recommended in the Diabetic Foot Manual of the Ministry of Health, Brazil. 21
Microbiological Analysis
Collection and Transport
Samples from open and closed ulcers were collected by the Vascular Surgery Service team at the regional public hospital of Vitória da Conquista. Local antisepsis was performed prior to the collection. Alcoholic chlorhexidine (0.5%) was used for disinfection. Open ulcers were debrided and cleaned with sterile saline. After debridement, the samples were collected by wiping a swab over the wound surface approximately five times, focusing on the areas where there was evidence of infection (pus and inflamed tissue). The swab was transferred to a tube containing 10 mL of brain heart infusion broth (Kasvi). The samples were then transported under refrigeration (4 °C) for processing, <24 h after collection, at the Microbiology Laboratory.
Bacterial Isolation and Identification
The tubes containing the samples were shaken in a vortex tube shaker to obtain a microbial suspension. For the isolation of S aureus, the samples were seeded in plates containing mannitol salt agar and incubated under aerobic conditions at 37 °C for 18 to 48 h. The isolates were identified based on the morphological characteristics of the colonies and the morphological staining. From each subculture, the isolates were subjected to catalase and coagulase assay and polymerase chain reaction (PCR) analysis for the nuc gene. Strains in the Gram, coagulase, catalase, and gene tests that tested positive for nuc were characterized as S aureus and were stored in a freezer at − 80 °C for further analysis.
Phenotypic and Genotypic Characterization of Antimicrobial Resistance
The susceptibility of the isolates was evaluated by the broth microdilution method in Mueller–Hinton broth (HiMedia Laboratories) for oxacillin/methicillin and vancomycin, according to the methodology recommended by the National Committee for Clinical Laboratory Standards (NCCLS) M7-A6. 22 Additionally, susceptibility to erythromycin (15 µg), doxicillin (30 µg), clindamycin (2 µg), gentamicin (10 µg), ciprofloxacin (5 µg), cefoxitin (30 µg), and meropenem (30 µg) were assessed by the disk-diffusion method according to the guidelines of NCCLS M100-S26. 23
The strains resistant to oxacillin/methicillin were subjected to PCR to detect the mecA gene and to characterize the staphylococcal cassette chromosome mec (SCCmec) gene. DNA extraction was performed according to the boiling method described by Fan et al. 24 The DNA obtained was subjected to PCR to detect the gene mecA as described by Vannuffel et al. 25 , 26 For the characterization of SCCmec, the samples were submitted to a multiplex PCR to detect genes for chromosomal cassettes from I to V using primers described by Boye et al. 27
Evaluation of Biofilm Production
Biofilm detection was performed according to the adapted methodologies described by Karaolis et al and Oliveira et al.28,29 Biofilm production was compared with that of Streptococcus pyogenes American Type Culture Collection (ATCC) 75194 (A492nm = 0.07). Additionally, the presence of biofilm was also evaluated by icaA and icaD gene detection using the methodology described by Korem et al. 30
Genotypic Characterization of Virulence
The samples were subjected to multiplex PCR to detect accessory gene regulator (agr) groups using primers described by Gillot. 31 Other toxigenic genes were identified by multiplex PCR in searching for the eta, etb, and tsst genes, based on sequences published by Becker, Roth, and Peters. 32 The strains were also tested for the presence of the genes encoding PVL (pvl), using the primers previously described by Lina et al. 33 Enterotoxin genes (sea–sei) were also identified by conventional PCR techniques based on multiplex and uniplex reactions, using synthesized primers based on the sequences published by Becker et al, Rosec and Gigaud, and Omoe et al.32,34,35
Statistical Analysis
Statistical analysis was performed using the Statistical Package for the Social Sciences version 23.0 (SPSS Inc.). In the descriptive statistical analysis, continuous variables were expressed as measures of central tendency and dispersion (mean, median, and standard deviation) and categorical variables as frequencies and percentages. For analyses of possible correlations between microorganisms and clinical variables, Spearman's correlation test was used and results were considered to be statistically significant when P < .05.
Results
Clinical and Epidemiological Data
Table 1 summarizes the clinical and epidemiological data of patients with diabetic foot disease. A total of 34 individuals with “diabetic foot” complications were treated at the Vascular Surgery Service of the regional hospital of Vitória da Conquista. Among the 34 patients studied, 24 (70.6%) were men and 10 (29.4%) were women. Their ages ranged between 34 and 85 years (mean: 60.03 ± 13.90 years), with the mean age of the female patients being 62.10 ± 14.74 years and that of the males, 59.12 ± 13.72 years. The ages corresponding to the 25th, 50th, and 75th percentiles were 51.09, 59.66, and 70.81 years, respectively. The individuals were mostly black (64.7%), married or in a stable relationship (44.1%), had low levels of education, had not attended elementary school (55.9%), or were illiterate (14.7%). A monthly income below the minimum wage was reported by 82.30% of the individuals, which at the time of the interview was R$954.00 or US$250.00.
Clinical and Epidemiological Variables of Patients with Diabetic Foot Disease Admitted to a Regional Public Hospital in Vitória da Conquista, Bahia, Brazil.
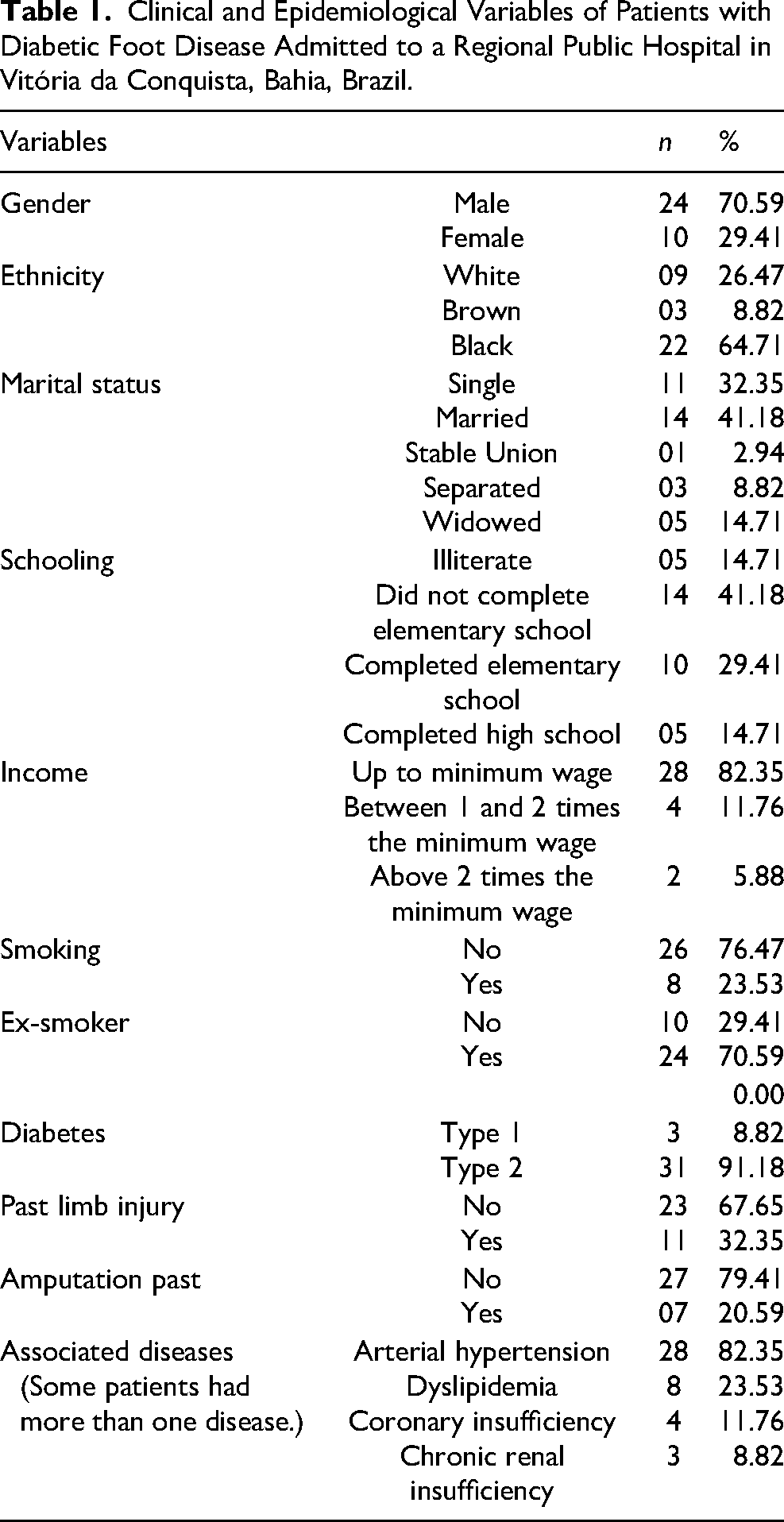
Most individuals had type 2 diabetes (91.2%). The mean time since the diagnosis was 13.9 years (±7.9). A previous history of foot ulcers was reported in 32.4% of patients, and 20.6% of patients reported previous amputation. The prevalence of smoking was 23.5%. Other participants (29.4%) reported that they previously had a habit of smoking, having stopped this habit on average 5.09 years (±11.71) before participating in the study. The prevalence of systemic arterial hypertension was 82.4% (n = 28). The prevalence of dyslipidemia, coronary insufficiency, and renal failure was 23.5%, 11.8%, and 8.8%, respectively.
The results of the subjects’ QOL assessments using the SF-36 survey are shown in Table 2. The data were evaluated from the transformation of responses into scores on a scale from 0 to 100, where 0 is the worst and 100 the best condition for the evaluated characteristic; their physical and emotional impairment stand out, since 75% of the individuals obtained a score equal to 0 for their physical impairment. The individuals were evaluated, and their injuries were stratified according to the criteria of the Wagner and University of Texas classification systems, and the results are shown in Tables 3 and 4.
Classification of Individuals with Diabetic Foot Disease Admitted to a Regional Public Hospital in Vitória da Conquista, Bahia, Brazil, According to Individual Domains Obtained Through the Medical Outcomes Study 36-item short-form health survey (SF-36) Questionnaire.
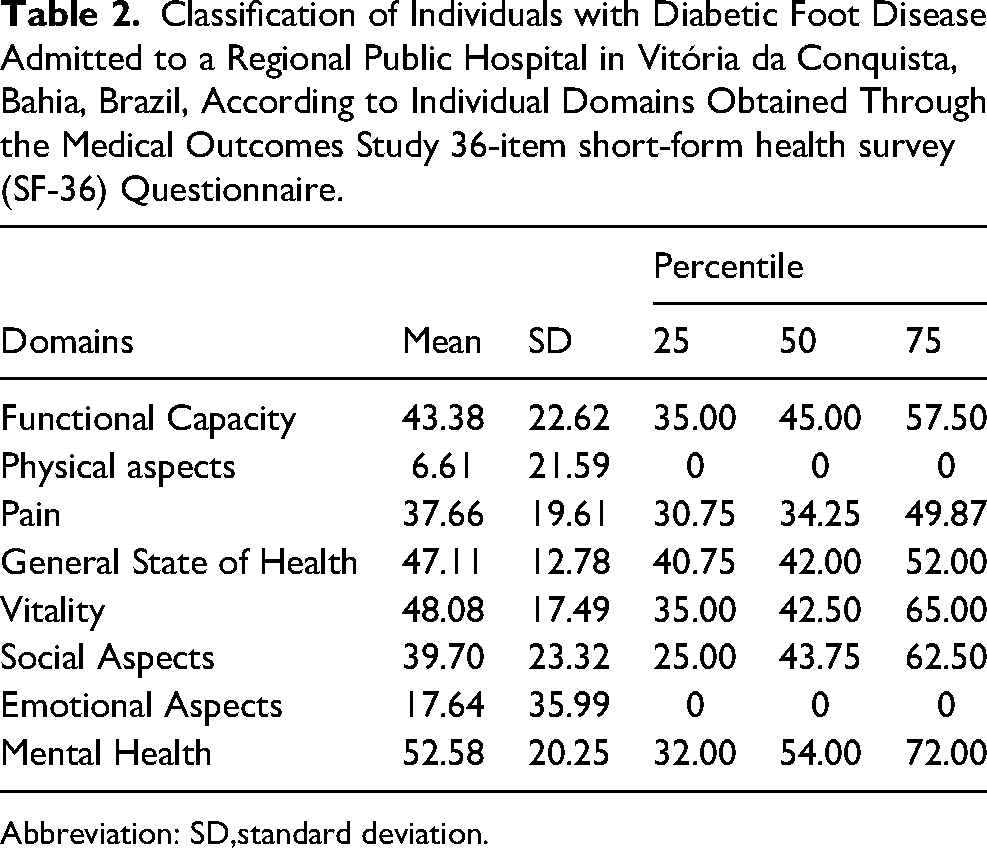
Abbreviation: SD,standard deviation.
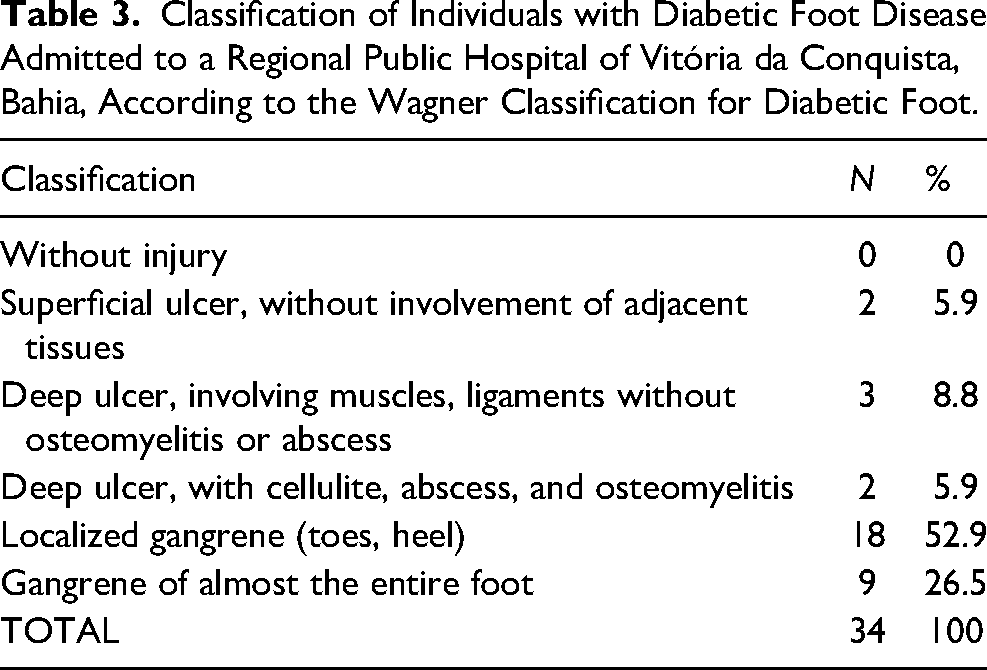
Classification of Individuals with Diabetic Foot Disease Admitted to a Regional Public Hospital of Vitória da Conquista, Bahia, According to the Wagner Classification for Diabetic Foot.
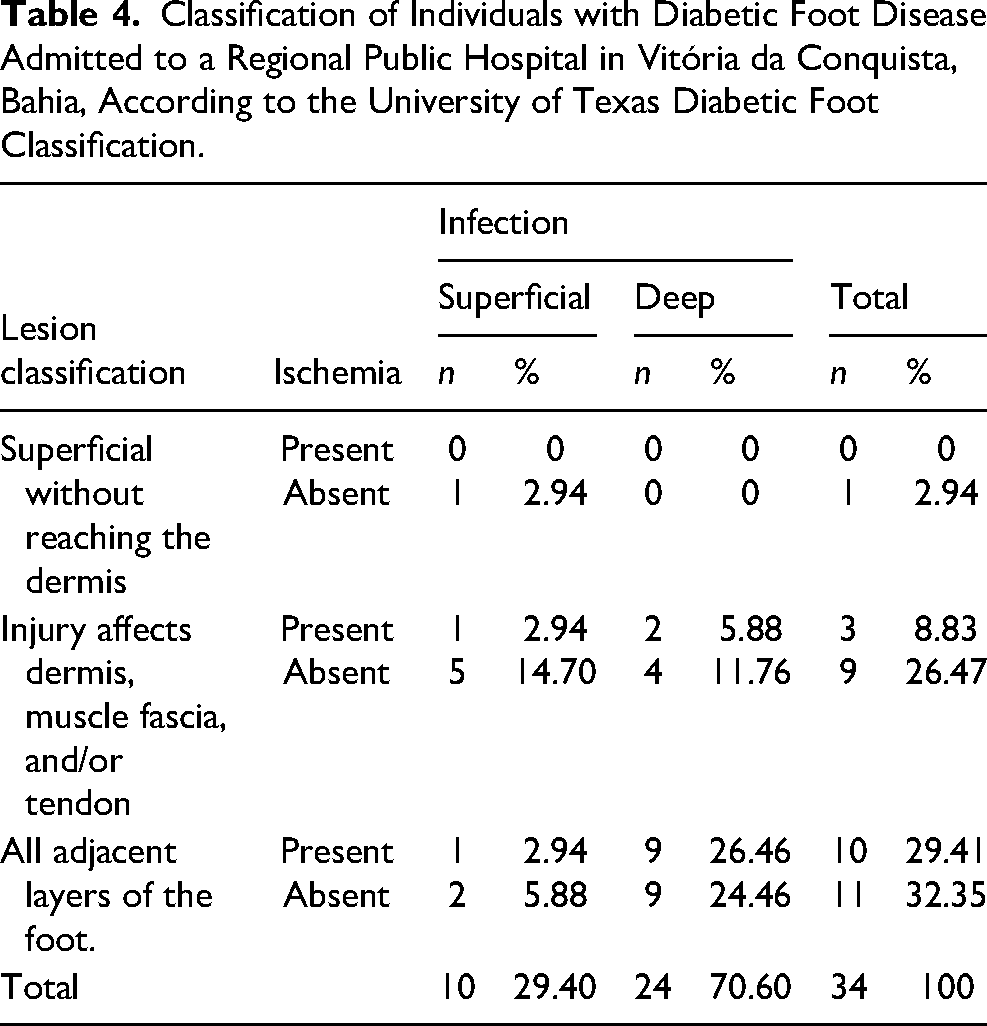
Classification of Individuals with Diabetic Foot Disease Admitted to a Regional Public Hospital in Vitória da Conquista, Bahia, According to the University of Texas Diabetic Foot Classification.
Bacterial Isolation and Susceptibility
Of the 34 samples analyzed, 17 (50%) yielded S aureus strains. No correlation was observed between the presence of the microorganism and age, type of diabetes, classification of individuals with diabetic foot disease, and lesion classification (P > .05). Among the 13 isolates analyzed by the antibiotic sensitivity test (four isolates did not grow in the reactivation stage), eight strains (61.5%) were resistant to erythromycin, five strains were resistant to cefoxitin (38.4%), four strains (30.7%) were resistant to clindamycin, four strains (30.7%) were resistant to ciprofloxacin, three strains (23.0%) were resistant to meropenem, and two strains (15.3%) were resistant to gentamicin. No strain showed resistance to doxycycline.
In determining the minimum inhibitory concentration (MIC), 38.5% (5 of 13) were resistant to oxacillin/methicillin. As for vancomycin, 92.3% (12 of 13) of the isolates were sensitive, and one strain (7.7%) was resistant. This isolate was also resistant to oxacillin/methicillin. No correlation was observed between the presence of antibiotic-resistant microorganisms and age, type of diabetes, classification of individuals with diabetic foot disease, and lesion classification (P > .05).
Genotypic Characterization of Antimicrobial Resistance
All strains resistant to oxacillin/methicillin presented the mecA gene and were characterized as MRSA (Figure 1A). SCCmec detection was performed for the five MRSA strains (Figure 1B). Among the strains evaluated, one (20%) presented SCCmec type V, and four (80%) presented SCCmec type I. SCCmec types II, III, and IV were not identified in this study. MRSA isolates of SCCmec types I and V demonstrated resistance profiles similar to those of cefoxitin and erythromycin (Table 5).
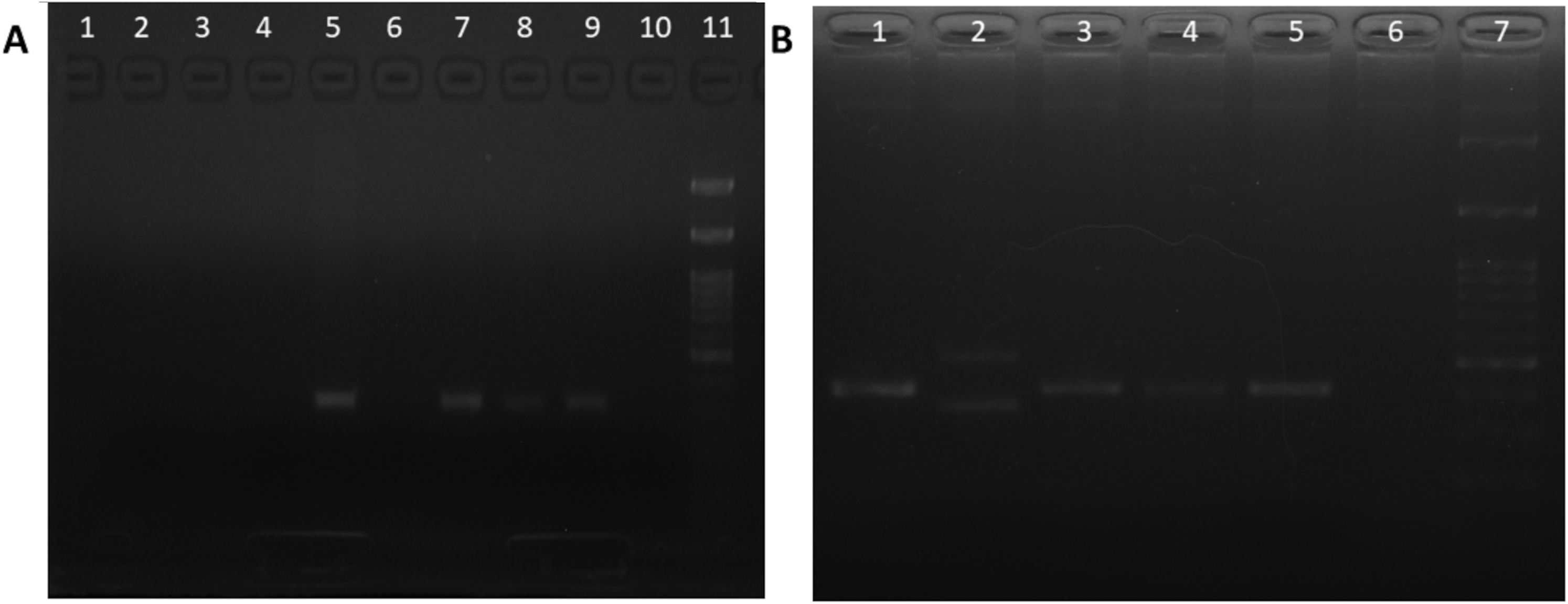
(A) Electrophoresis of PCR products with primers to detect mecA gene in staphylococcus aureus resistant to oxacillin/methicillin strains. Lanes 1 to 8: Strains tested; lane 9: positive control (S aureus ATCC 43300); lane 10: negative control with water; lane 11: molecular size markers of 100 bp. Lanes 5, 7, and 8 show positive results. (B) Electrophoresis of PCR products for staphylococcal cassette chromosome mec (SCCmec) gene characterization in MRSA strains. Lanes 1 to 5: Strains tested; lane 6: Negative control with water; lane 7: Molecular size markers of 100 bp. Lanes 1, 3, 4 and 5 show positive results for SCCmec type I. Lane 2 show positive result for SCCmec type IV.
Antimicrobial Resistance According to Types of Staphylococcal Cassette Chromosome mec in Methicillin-Resistant Staphylococcus aureus Isolated From Patients with Diabetic Foot Disease Admitted to a Regional Public Hospital in Vitória da Conquista.
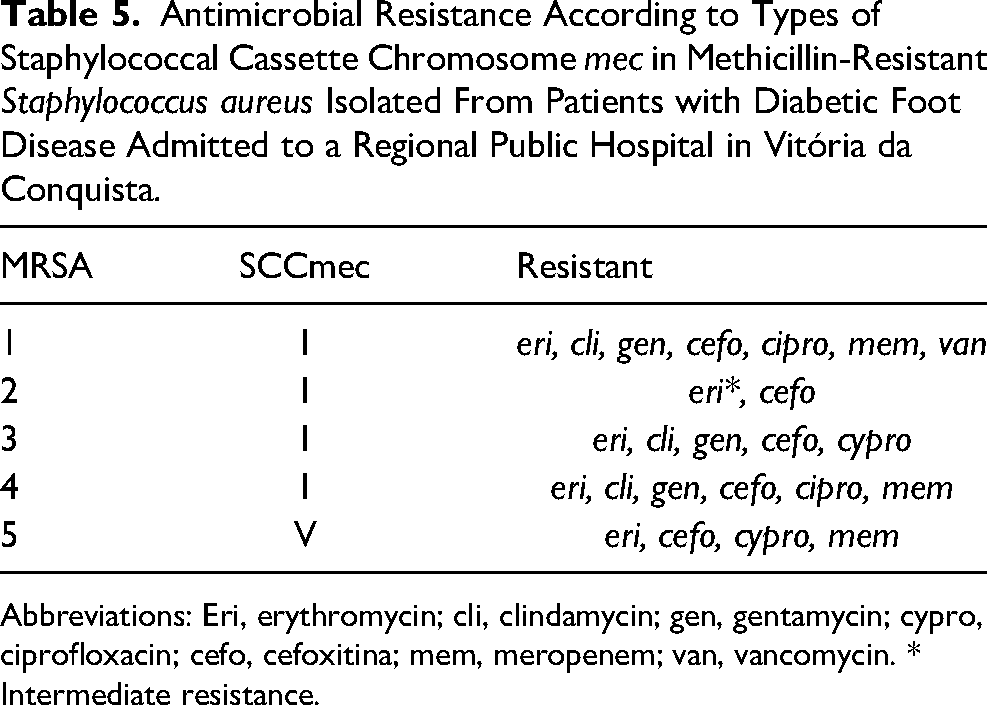
Abbreviations: Eri, erythromycin; cli, clindamycin; gen, gentamycin; cypro, ciprofloxacin; cefo, cefoxitina; mem, meropenem; van, vancomycin. * Intermediate resistance.
Isolation, Phenotypic, and Genotypic Evaluation of Biofilm Production
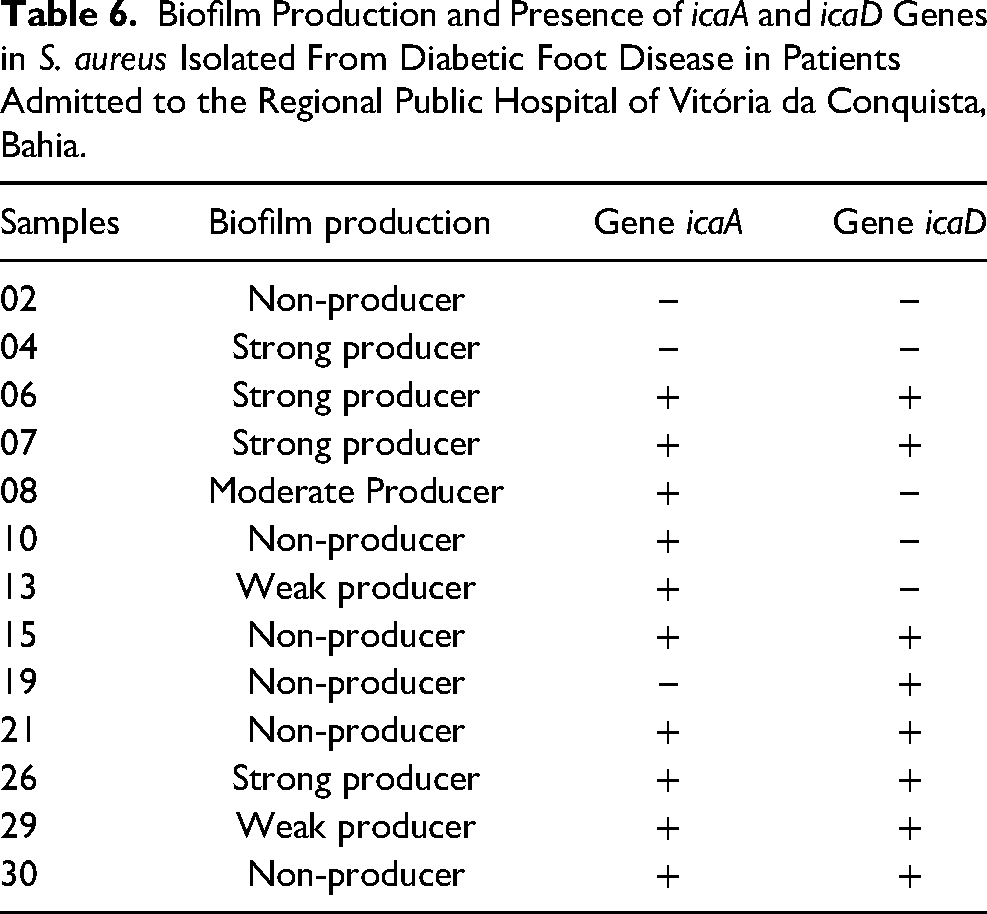
Among the 13 samples evaluated, 7 (53.8%) were able to produce biofilms at different levels. Regarding genotypic analysis, 11 (84.6%) isolates were positive for icaA and/or icaD, and 7 (53.8%) had both genes simultaneously (Table 6).
Biofilm Production and Presence of icaA and icaD Genes in S. aureus Isolated From Diabetic Foot Disease in Patients Admitted to the Regional Public Hospital of Vitória da Conquista, Bahia.
Genotypic Characterization of Virulence of Isolates
The enterotoxin genes seb, sec, seg, and sei (5.9%, 5.9%, 11.8%, and 23.5%, respectively) were present in the 17 specimens isolated, and the accessory regulatory genes, types 1 (5.9%) and 2 (11.8%), were identified. Genes for exfoliatins (eta and etb), enterotoxins (sea, sed, see, sej, and seh), pvl, and tsst were not detected in the samples analyzed. Regarding the distribution of genes, 11 (64.7%) isolates were positive for at least one of the evaluated genes, and four (23.5%) isolates had two or more concomitant genes (Figure 2).
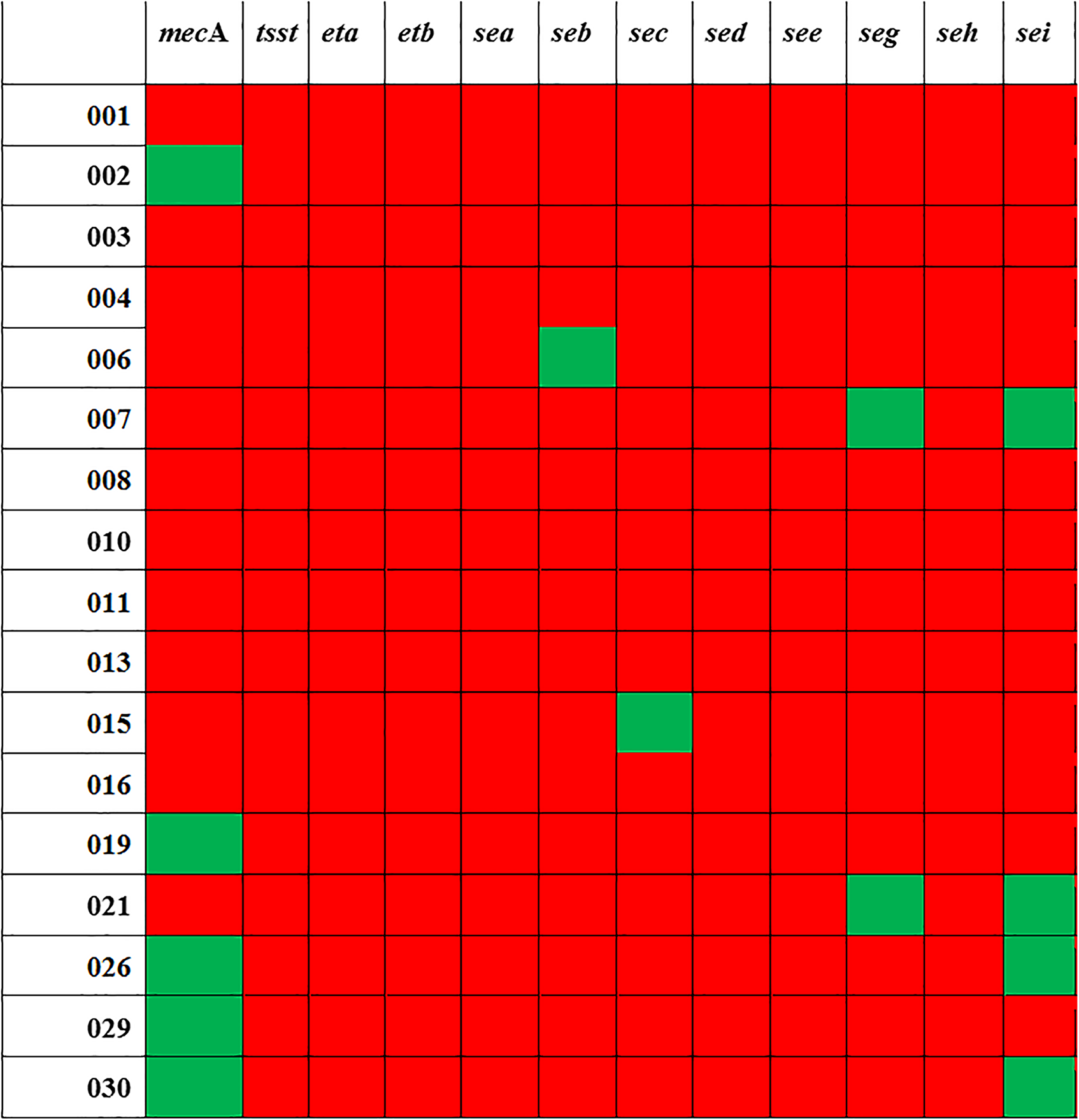
Virulence genes distributed among 17 strains of Staphylococcus aureus isolated from patients with diabetic foot disease, illustrating the presence (green) or absence (red) of the genes.
Discussion
The profile of the study population indicated a mean age of 60 years, ranging from 34 to 85 years. They were predominantly male, black, married (44%), with incomplete elementary education and an income below the minimum wage. Of the study population, 23.5% were smokers and 29.4%, ex-smokers. They presented with type 2 DM and a third had a history of one or more limb injuries and 20.6% past amputation. The most prevalent comorbidity was arterial hypertension. Parisi et al, in a multicenter study, also described a greater proportion of men with a previous history of ulcer (35.7% vs. 18%; P < .001) and a greater proportion of men than women with a report of amputation (23.5% vs. 6.5%; P < .001), as well as the same profile for age (57.7 years) and prevalence of type 2 diabetes (90.7%). 36 However, Chen-Ku et al., when studying complications related to type 2 diabetes, reported that the gender distribution was not disproportionate. 37
In the 34 individuals in our study, we found a high prevalence of localized gangrene (52.9%); the next most common was gangrene of almost the entire foot (26.5%); three subjects (8.8%) had deep ulcers involving muscles and ligaments, without osteomyelitis or abscess; two subjects (5.9%) had deep ulcers with cellulite, abscess, and osteomyelitis, and two subjects (5.9%) had superficial ulcers without involvement of adjacent tissues (Table 3). It is worth noting that 79.4% of the studied patients had a history of previous amputation and that the average disease time since diagnosis in this study was 13.91 years (±7.97 years). Parisi et al. reported a very similar average time of 14.2 years (±9.8 years). 36 The development of diabetes complications is related to the duration of the disease; this relationship was well demonstrated in a cohort study in which more than 70 000 individuals in their sixth decade of life were observed, and both age and duration of diabetes proved to be predictors of diabetic complications regardless of the clinical course. 38 Cortez et al observed an increase in the percentage of amputation, diabetic foot, nephropathies, diabetic retinopathies, acute myocardial infarction, and stroke, depending on the years since diagnosis. In individuals who had been diagnosed with diabetes for >10 years, the percentage of complications was 32.2%, and for those who had been diagnosed <5 years previously and between 5 and 10 years prior to this study, it was 12.1% and 14.2%, respectively. 39
In this study, a higher prevalence was noted in individuals with a low educational level (illiterate or with incomplete elementary education) and with a monthly income below the minimum wage. In a systematic review summarizing and quantifying the published evidence and associations between type 2 diabetes and socioeconomic status, Agardh et al reported an overall increase in the risk of type 2 diabetes in lower socioeconomic groups, whether measured by educational levels, occupation, or income. 40 The association between increased prevalence of diabetes and low socioeconomic status was also described by Wu et al . 41 In Brazil, the risk factors for DFUs identified by Zavala and Braver were low levels of education (58.3% with incomplete elementary education), arterial hypertension (65.5%), physical inactivity (61%), and microvascular diseases (29.8%); the mean duration of diabetes was 12.9 years, and the fasting glycemic average was 189.7 mg/dL. 42
The evaluation of QOL seeks to objectively evaluate aspects often intangible in the process of illness; this analysis has been increasingly included in studies because it allows an assessment of an individual's physical, emotional, and social status. Aguiar et al concluded that the SF-36 is a reliable tool for assessing the QOL of patients with diabetes in Brazil. 43 The eight domains of the SF-36 are scored on a scale from 0 to 100, with 100 being the best possible health status. In an evaluation of diabetic individuals, Santos et al reported that physical aspects, more than mental health aspects, affected the QOL of these individuals. 44 These findings are consistent with the findings of the present study, in which the physical component had the lowest score (mean score was 0), while the related aspects in the mental health domain had the highest score (mean score of 52.58) (Table 2). The marked influence of physical aspects on the QOL in our population may be because we evaluated patients with active injuries, who presented with substantial functional impairment of the foot, by either the Wagner classification or the University of Texas classification.
In the present study, 17 samples (50.0%) were positive for S aureus among the 34 samples analyzed, with five isolates being characterized as MRSA strains. Gram-positive aerobic microorganisms, especially S aureus, are predominant in the acute colonization of skin wounds. 45 A multicenter study by Lipsky et al observed that 77% of DFUs were colonized by Gram-positive aerobes, with S aureus the dominant pathogen. 46 Likewise, Mendes et al found 51% prevalence of S aureus in Lisbon DFU patients, of which 24.5% were MRSA. 47 However, Hatipoglu et al found a lower prevalence (19.1%) of S aureus infection in studies carried out between 2007 and 2011 in Turkey, of which 5.7% were characterized as MRSA 48 . In Brazil, few studies have described the prevalence of S aureus isolates in DFUs. Fernandes et al, studying the colonization and susceptibility of DFU and varicose ulcers in the state of Goiás, found that S aureus was the dominant pathogen in DFUs, with a prevalence of 32% (16 of 50); among all the isolates of S aureus, including those from varicose ulcers, MRSA had a 69% prevalence. 49 In the state of Minas Gerais, Jorge et al found an S aureus prevalence of 14.8% in 136 cultures from 70 patients with DFUs, the dominant pathogen being Gram-negative Proteus mirabilis with a prevalence of 23.5%. 50 In the past 10 years, MRSA infections have attracted worldwide attention, 51 as the treatment of these infections has become increasingly demanding. 52 MRSA refers to strains resistant to practically all antibiotics in the β-lactam group; this resistance is conferred by obtaining a mobile genetic element, known as SCCmec, in which the gene is located. The mecA gene encodes an altered penicillin-binding protein (PBP2a/PBP2). Thus, MRSA strains continue to biosynthesize the cell wall, even in the presence of inhibitory levels of β-lactam antibiotics. Among the positive mecA strains, one isolate had SCCmec type V, and four isolates had SCCmec type I. Feng et al studied 57 MRSA isolates from the diabetic foot, and found that 49.1% carried SCCmec type III and 50.8%, SCCmec type IV. 51
Among the 13 isolates obtained in the present study, 61.5% were resistant to erythromycin, 38.4% were resistant to cefoxitin, 30.7% were resistant to clindamycin, 30.7% were resistant to ciprofloxacin, 23% were resistant to meropenem, and 15.3% were resistant to gentamicin; none of the isolates showed doxycycline resistance. Sekhar et al 53 , analyzing isolates obtained from patients with diabetic foot disease, found a 28.6% prevalence of resistance to erythromycin, 38.5% to oxacillin, and 17% to gentamicin; 100% of the S aureus isolates were sensitive to doxycycline. 53 Anvarinejad et al found a 70% resistance to clindamycin and ciprofloxacin, and suggested that the high resistance was due to almost all patients using clindamycin and ciprofloxacin as empirical therapy. 52 In the present study, one strain was resistant to vancomycin. Several studies have reported 100% sensitivity to vancomycin,51,54–57 although other studies have reported a sensitivity of <100%. Chaudhry et al reported a vancomycin-resistant S aureus (VRSA) percentage of 80%, of which 90% were also resistant to oxacillin 58 . In Brazil, Fernandes et al found no VRSA strain among 27 staphylococcal strains isolated from patients admitted with DFU. 49 According to Charles et al, risk factors for VRSA infections include the presence of an underlying disease such as diabetes, recent major surgery, and previous treatment with vancomycin. 59
When analyzing the pathogenicity of the isolates, for the accessory gene regulator (agr), types 1 (5.9%) and 2 (11.8%) were identified. Azmi et al reported the prevalence of four agr groups in 248 Palestinian strains: 39.5% agr 1, 33.0% agr 3, 9.3% agr 2, 3.6% agr 4, and 14.5% were negative for agr by PCR. 60 The establishment of an infection is caused by the mechanisms of adhesion, insertion, and maintenance of the pathogen in the host. The correlation of genes that protect the life of bacteria is called a quorum, and includes the role of the accessory regulatory gene (agr), 61 which acts by coordinating virulence genes, and is thus related to the capacity to harm the host.62,63 According to Rossato, agr 1 is found in noninvasive infections; in contrast, agr 2 is present in infections with a more serious character. 63 The agr gene exerts activity dependent on the agr enterotoxin (SEB, SEC, SED, etc); however, agr-independent enterotoxins exist (SEA, SEJ). 61 In the present study, the genes related to enterotoxins were identified as seb, sec, seg, and sei (5.9%, 5.9%, 11.8%, and 23.9%, respectively). When evaluating the genotype, it was observed that two strains had more than one gene. Enterotoxins are grouped into classic enterotoxins (SEA–SEE) and new enterotoxins (SEG, SHE, SEI, and SEJ). These toxins can contribute jointly or individually to the pathogenesis of complications and to the severity of human diseases, and can lead to sepsis. 64 Genes for exfoliatins (eta and etb), enterotoxins (sea, sed, see, sej, and seh), pvl and tsst were not detected in the samples analyzed. The small number of patients included in the study may explain the non-identification of pvl, tsst, eta, and etb genes in any of the 17 samples of S aureus analyzed in this study, as these genes have a low prevalence in samples from patients with diabetes affected by ulcers.6,7
Biofilms are defined as microbial communities of sessile cells that are connected by microbial intercellular adhesion molecules and are often incorporated into a protective extracellular polymer matrix.65–68 The prevalence of S aureus biofilms is critical, since infections associated with biofilms are mostly recurrent and can act as a barrier, physically reducing the penetration of the antimicrobial agent. In the present study, seven isolates (53.8%) were able to produce biofilms. Similar results were found by Belbase et al with strains of S aureus, in which 46.1% of the isolates were considered biofilm producers. 69 In another clinical study on the evaluation of S aureus virulence determinants in DFU infections, an even greater proportion (100%) of positive strains for this microorganism produced biofilms. 70 Among the biofilm producers in the present study, 28.6% (2 of 13) were weak producers, 14.3% (1 of 13) moderate producers, and 57.1% (4 of 13) strong producers. In a study carried out in India, with samples of DFU infections, approximately 54.0% of the strains of Staphylococcus were strong biofilm producers. 71 Azmi et al found 32.7% of strains were weak producers, 46.4% moderate producers, and 21% strong producers. 60 Regarding intercellular adhesion factors in the present study, 84.6% (11 of 13) of the isolates were found to be positive for icaA and/or icaD, with 53.8% (7 of 13) having both genes simultaneously. In some samples, there was no correlation between the presence of icaA and/or icaD genes and the ability to form biofilms. These data reveal that although bacterial strains have the genetic capacity to produce biofilms, this does not necessarily mean that biofilms will be formed, because the detection of genes does not imply their functionality. Petrelli et al, evaluating the biofilm-formation capacity of 37 strains of S aureus isolated from catheter infections, also observed strains that simultaneously presented the icaA and icaD genes, but were unable to produce biofilm. 72 Hou et al also found no correlation between the presence of genes and the formation of biofilms for some samples. 73 In the present study, we also observed a possible ica-independent strain, phenotypically presenting biofilm production yet lacking an apparent genotypical explanation. According to Figueiredo et al, the mechanisms involved in ica-independent biofilms are multifactorial and not yet fully understood. 74 Studies on ica-independent biofilms are widely performed with strains of S aureus from different origins, and the major structural components of biofilms produced by one strain may not be the same for all strains of S aureus depending on environmental signals. 75
The present study has some limitations. First, the smaller number of participants was due to number of patients admitted to the hospital during the study period. Moreover, the numerous refusals of patients (condition of pain and discomfort) was due to the fact that the collection of information was performed during patient admission. Thus, this sample also tended to have more individuals with type II diabetes than individuals with type I diabetes.
Conclusion
The data from this study are of fundamental importance for establishing the profile of virulence and microbial resistance, as well as the clinical and socioeconomic profile of patients with DFUs infected by S aureus in the southwest region of Bahia, Brazil. Such data may be used by multidisciplinary teams to diagnose, empirically treat, and monitor patients affected by the disease, improve the quality of care, and reduce costs. With a growing number of studies on the topic in the northeast of Brazil, the results may be used to inform investigations into DFUs in this region and in other locations.
Footnotes
Author Contributions
ACPL, LDN, MMT, JMAS, and LOS contributed equally to this paper.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (Grant no. Code 001).