
Abstract
Cholesterol embolization syndrome is an increasing but underestimated problem after endovascular intervention or after the start of thrombolytic therapies. Embolies from the aortic wall involves abdominal organs and the skin of the lower extremities or buttocks. In our case a progressive ulceration and necroses occurs spontaneously. Endovascular treatment of the lower extremities was successful for a short period. Due to the progression of necrosis, both legs were amputated. Biopsies were taken from the skin were initially no directions to the diagnosis of Cholesterol embolization syndrome. After a second elliptical excision biopsy the diagnosis of cholesterol embolization syndrome was confirmed. Because the rapid progression of skin necroses despite the treatment of prednisone, patient died due to sepsis and renal failure. This case shows when arterial revascularization is performed and progression in skin necrosis occurs despite optimal arterial vascular status the diagnosis CES should be considered and treated in an early state of disease.
Introduction
Cutaneous Cholesterol Embolization Syndrome (CES) is an increasing but often unrecognized diagnosis due to its poor clinical recognition. 1 Cholesterol embolism may occur after the start of anticoagulant or thrombolytic therapy or after endovascular procedures or may occur spontaneously.2–5 Atherosclerotic plaques are lined along the great and intermediate great vessels. 6 The effect of the embolism depends on the position of the plaque in the aorta. 7 Plaques along the descending aorta mostly affecting the lower extremities, kidneys, intestine, or skin. Skin involvement results in blue toes syndrome or livedo reticularis in the upper legs and buttocks, in 88% of cases. From these patients, around 40% develop ulcers or necrosis. 8 In patients with CES, with only cutaneous involvement, a mortality of 33% is reported.2,8 In this case report, we present a severe and fatal course of CES.
Case Description
A 62 years old male with a medical history of ischemic cerebrovascular accident, dyslipidemia, hypertension, adiposity, and peripheral arterial vascular disease, consulted the outpatient clinic because he had progressive ulcers of both feet (chronic limb ischemia grade 5). The ulcers had developed two months before the consultation. An ankle/arm index showed 28% on the left and 38% on the right leg. The diagnosis of arterial ulcers was made. Magnetic Resonance Angiography (MRI) showed an atherosclerotic wall plaque lining along the aortic wall and multiple occlusions in the iliac and crural arteries
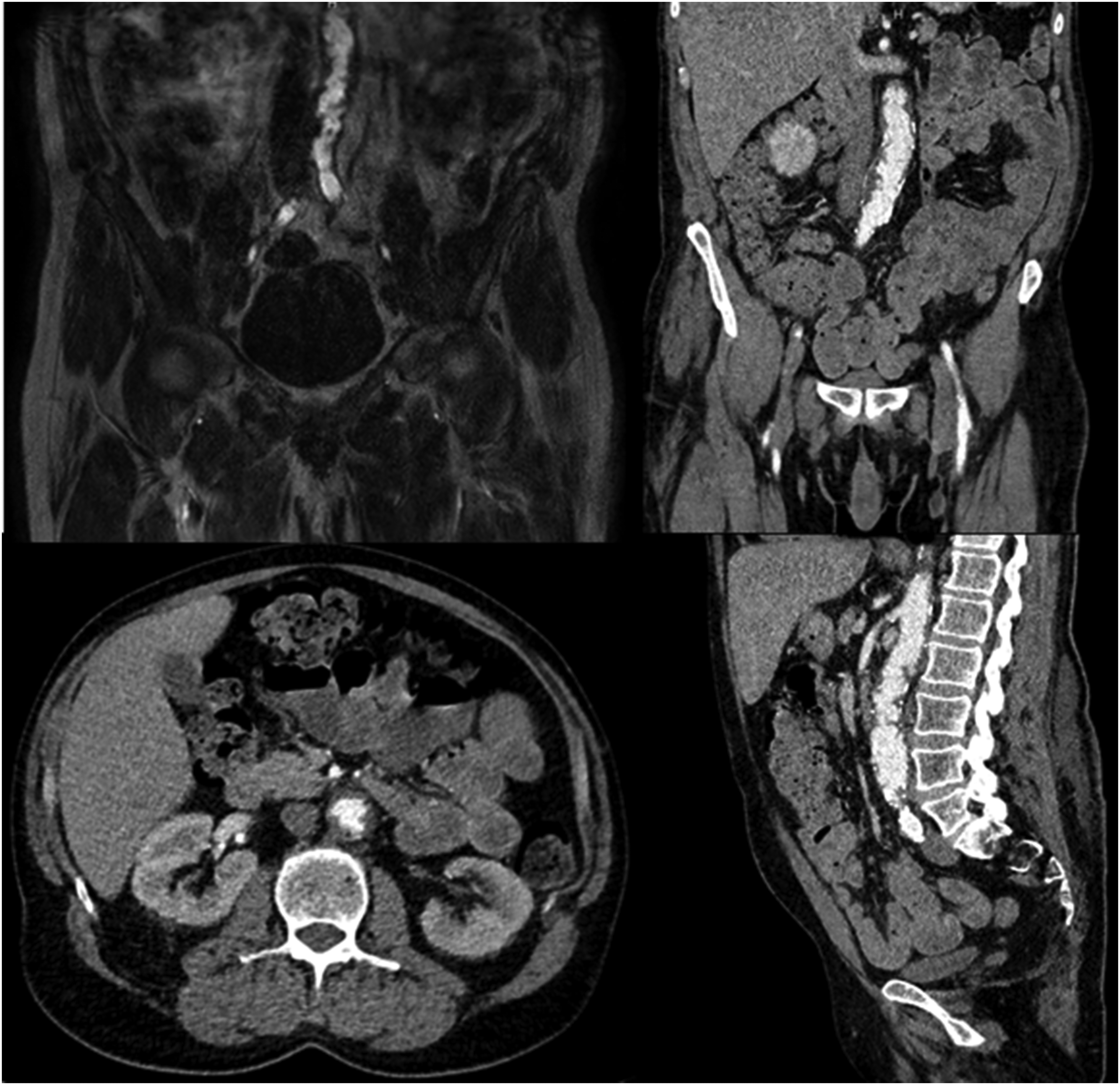
Radiographs from the aortic plaque.
Ten days after discharge, the patient presented with progressive and infected wounds on the left leg, following which the left lower leg was amputated. After seven days, a forefoot amputation of the right foot was carried out because of progressive worsening of necrosis and infection. Five days later, multiple necrotic plaques surrounded by livedo reticularis and retiform purpura developed over the trunk and upper legs

Pictures from different time periods in the progression of skin necrosis.
Discussion
Cholesterol embolism syndrome is an increasingly common disease. Since the start of endovascular treatments and the possibilities for thrombolytic therapies, the incidence of CES has increased. It is more common in men than women, with the classic age being 60 years and older. Risk factors are smoking, hypertension, peripheral- and central vascular disease. Laboratory findings such as acute renal insufficiency, eosinophilia and, increased erythrocyte sedimentation rate can be found in CES.2,9 Skin involvement mostly results in blue toes syndrome (74%) and 50% of patients with visceral manifestation have skin lesions. Early recognition of skin necrosis is essential in the management and prevention of the high morbidity and mortality of this disease. Cutaneous necrosis is often a symptom of broad sequelae of pathologies, one of which is CES.
10
Histology confirms the diagnosis of CE with a sensitivity of 86% to 92%.6,8 In our case, the first histological biopsies were negative for cholesterol crystals, possibly due to the small biopsy size of 3 mm and 4 mm with a higher risk of sampling error. Therefore, a larger elliptical incision biopsy should be taken to prevent misdiagnosis
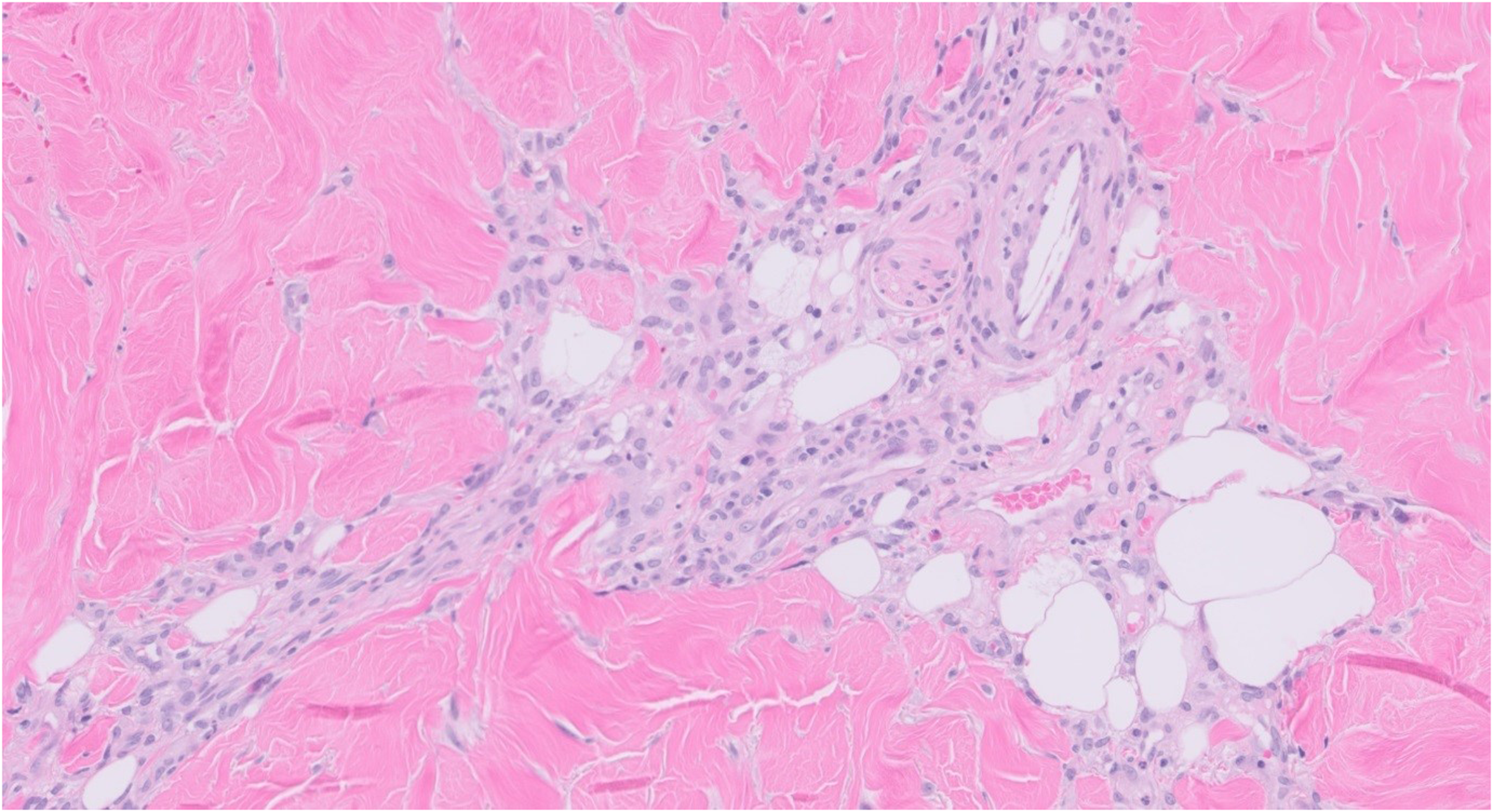
Pathology: second biopsy shows cholesterol crystal embolisms.
Differential diagnostically, heparin-induced skin necrosis was considered (HISN). Necrotic skin lesions occur in 0.2%-7.5% of patients receiving heparin, however the most common lesions are minor lesions on the injection side, a minority of cases with extended lesions are caused by unfractionated heparin and anecdotal described in distant lesions from low molecular weight heparin. There are no reports describing the incidence of such extend necrotic lesions under heparin therapy as described in this case report.11–13 Heparin-induced skin necrosis usually develops with erythematous painful subcutaneous nodules that rapidly increase in size. After this, blisters and ulcerations form. Skin biopsies of these lesions show necrosis, infarcts, or vasculitis. 14 Heparin-induced skin necrosis usually occurs after 5 to 10 days and occurs mainly in women. 10 Unlike CES, there are laboratory tests for HISN. Although HISN is associated with HIT, however, a reduced platelet count is not always found. Diagnosis of HISN is confirmed by the presence of IgG antibodies against Heparin Platelet Factor-4. These antibodies were not found and there was no evidence of vasculitis.15,16
Heparin-induced skin necrosis or HIT normally improves upon withdrawal of the heparin. 15 In our case, there was no improvement in skin lesions despite discontinuation of heparin and switching to fondaparinux and a course of high-dose prednisone. During admission in our hospital patient received nadroparin prophylaxes and was discontinued during one month without any improvement in skin lesions. The blood tests were negative for HISN or HIT. A second larger histological biopsy was taken to confirm the CES diagnoses. Our case was treated in a multidisciplinary manner with the dermatologist and internal medicine.
The treatment of CES is based on three characteristics of this disease. First, establishing the aortic plaque with cardiovascular risk management using statins, blood pressure regulation, and lifestyle changes. Statins are beneficial in improving cutaneous manifestations and renal outcomes.17,18 Further, reducing the inflammatory response of cholesterol crystals was high-dose prednisone, and colchicine is effective in reducing symptoms and extend of necroses in cutaneous manifestation.19,20 Despite the high dose of prednisone in our case, no improvement was seen in his cutaneous lesions. New perspectives for the treatment of CES is targeting the inflammatory response by inhibition of interleukin 1 and 5 which are mediators in the inflammation in CES. Pharmaceutical treatments should started in an early stage of disease in targeting these inflammatory responses are colchicine, canakinumab, cyclophosphamide, and corticosteroids, in our case there was no positive effect on high dose of corticosteroids. 21 Surgical intervention can be considered to remove or bypass the embolization source. In one study endarterectomies and bypass surgeries for CES documented survival of 89% of patients after one year of follow-up. 22 Nowadays, new techniques with endovascular stents are promising in covering the aortic plaques to prevent further embolization.23,24 After the diagnosis of CES was confirmed in our case, stent placement covering the aortic wall plaque was considered. Due to the rapid progression of necrosis in the groin, buttocks, and legs, it was no longer possible to access the groin for endovascular treatment. The lesson learned from this case is when arterial revascularization is performed and progression in skin necrosis occurs despite optimal arterial vascular status the diagnosis CES should be considered.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.