
Abstract
The recurrence of venous ulcers is the wound reopening after a period of completed epithelisation of a previous ulcer due to exposure to causal factors and lack of prevention. Venous ulcers have a high recurrence rate that may increase through the years. Epidemiological evidence on its incidence and risk factors is scarce due to the lack of patient follow-up in outpatient clinics and adherence to treatment after healing. The objective was to analyze the incidence of venous ulcers recurrency in outpatients and the risk factors for its occurrence. It is an observational historical cohort with retrospective data collection, performed through electronic medical records. Setting: private health insurance outpatient clinic. The participants were adult patients with healed venous ulcers. Incidence of venous ulcer recurrence was calculated within individuals with healed ulcers from 2014 and 2018 with a follow-up of at least one year. Bivariate analysis and logistic regression were used to explore risk factors considering demographic, clinical, and wound-related variables. As a result, sixty-five (65) of the 134 patients with healed venous ulcers had a recurrence, leading to an incidence of 48.5%, with a mean onset time of 230.1 (SD 267) days. Patients with recurrent venous ulcers were primarily women (39/48.1%), with a mean age of 64 (SD 15.5) years, 57 (50.8%) had some comorbidity, with systemic arterial hypertension as the most frequent (47/51%). Obesity (15/88.2%) increased the risk of venous ulcers recurrence by 8.7 (OR 95% CI 2.1-60.8; P = .009) times. In conclusion, venous ulcers recurrence incidence was 48.5%, with obesity as a risk factor. This study demonstrates that the clinical approach of people with venous ulcers should not finish when the wound is healed. For ulcer recurrence prevention interventions addressing systemic factors, besides topical management of the wound, are essential.
Keywords
What is Already Known
Approximately 50% to 76% of venous ulcers open again after healing, tending to increase with following years
There is a lack of epidemiological data about venous ulcer recurrence compared with the extensive literature regarding venous ulcer management
What This Paper Adds
Recurrent venous leg ulcers were identified primarily in women > 60 years, obese, hypertensive, and diabetic.
An incidence of venous leg ulcers recurrence of 48.5% was identified in an outpatient clinic.
Obesity increased by 8.7 times the chances for patients with healed ulcers to have an ulcer recurrence.
Introduction
Noncommunicable diseases (non-infectious chronic diseases) count for up to 71% of deaths worldwide; cardiovascular diseases (ischemic heart disease and stroke) lead the list. Additionally, Diabetes Mellitus is in the ninth position; both conditions share pathological features, with Chronic Venous Disease as one of the resultant complications.1,2
Chronic Venous Disease presents the following highlighted risk factors: age, female sex, family history, obesity, pregnancy, static standing, sedentary lifestyle, and smoking.3,4 Studies show a higher venous ulcer prevalence in women than men, with a ratio of 3:1. The most affected age group is people over 60 years.5-7 Venous ulcer is the most severe Chronic Venous Disease late complication, and it is the primary etiology of lower limb ulcers representing 55% to 75%.4,8 Possible venous ulcer causes include inflammatory processes, resulting in leukocyte activation, endothelial damage, platelet aggregation, intracellular edema, and oxidative stress with tissue destruction. 9
Recurrent active venous ulcer is in the uttermost clinical manifestation of the Chronic Venous Disease, according to the CEAP standardized clinical classification system, which stands for Clinical (C), Etiological (E), Anatomical (A), and Pathophysiological (P) characteristics of the disease. The classes C5 and C6 indicate the presence of an ulcer, healed in the case of C5, active in C6, and recurrent in C6r; the inclusion of the recurrent status of the venous ulcers was one of the additions in the 2020 classification update, acknowledging the recurrency as a possible and common status for people with advanced Chronic Venous Disease. 10
Meta-analysis of observational studies on the prevalence of chronic wounds estimated a pooled prevalence of 1.51 leg ulcers per 1000 individuals from 9 studies developed in different countries. 11 About 1% of adults in developed countries are affected by some leg ulceration at any time in their life. Population from the USA has involved a prevalence of venous leg ulcers of 0.5% to 0.8% in the general population and an incidence of between 2 and 5 new cases per 1.000 individuals per year. 7
Epidemiological records of the disease in non-developed countries are few, and no official estimates are established at the national or regional levels. However, four studies conducted in different cities in Brazil, applying different methods, and including different samples, obtained respectively a prevalence from 1.5% to 83,3% of active or healed venous ulcer cases in an outpatient population.12-15
The cost of venous ulcer management is high. A secondary study developed in the United Kingdom reported costs representing 1.2% of the annual budget. The main costs were driven by the nurse visits followed by the dressings and compression therapy. 16 Indirect costs for the patient and family should also be considered since venous ulcers could become a family burden, negatively impacting their economic dynamic and quality of life. 17 The patient's lifestyle is also impacted due to the recurrent outpatient clinic visits for dressing changes and an unpleasant odor due to wound exudate.14,18,19
One of the main characteristics of venous ulcers is the high rate of recurrence. Approximately 50% to 76% of ulcers open again after healing, tending to increase over the years.20,21
Patients with venous ulcers are increasingly seen in ambulatory care facilities, through multi-professional or Stomatherapy Nursing clinics, both in the public and private sectors, avoiding hospitalizations for wound treatment.6,22 Some specialized services have high-tech products, offering their patients holistic and individualized treatment. 23 In the absence of specialized outpatient clinics, patients are “lost” among disconnected health professionals, with different approaches and follow-up. Reducing the patient's journey through a specialized center is fundamental in several aspects, mainly in the economic, clinical, and psychosocial scope.
Venous ulcer epidemiological exploration is essential in public health as it constitutes a global problem with frequent recurrences, affecting people of different age groups and causing biopsychosocial and economic difficulties. 24 Scientific evidence on the incidence of venous ulcer recurrence and risk factors is still scarce in different clinical contexts and countries. Thus, more studies are needed to understand the problem better and enable reorganizing and redesigning comprehensive and resolute care.
Given the above, this study aimed to analyze the incidence of recurrent venous ulcers in patients treated at an outpatient clinic and the risk factors for its development. The secondary aim was to describe the characteristics of the patient with a recurrent venous ulcer.
Methods
This study is an observational historical cohort with retrospective data collection, conducted at a Stomatherapy Outpatient Clinic of “a Healthcare Operator located in the city of São Paulo, Brazil.” This nursing practice attends to people with acute and chronic wounds, referred by physicians from different specialities, emergency room healthcare teams, or free demand. The present study was extracted from a Master's dissertation. 25
The studied population consisted of all medical records of patients treated at the clinic from April 2014 to April 2018. The convenience sample consisted of adult patients aged 18 years and older with a venous ulcer that completed epithelisation. Having complete record data was also considered for the inclusion of patients in the final sample. The diagnosis of lower limb wounds as venous ulcers is routinely made in the research setting, following a protocol considering clinical findings on the skin during the comprehensive assessment: lipodermatosclerosis, hyperpigmentation, eczema, edema, varicose veins, ulcer characteristics, anatomic location, presence of pain, and Ankle Brachial Index (ABI) 0.9 to 1.4 mmHg.26-28
The data collection was performed using the patients’ electronic medical records to fill out the collection form. For patients with a healed venous ulcer in 2018, the medical record was analyzed until April 2019 to verify if their venous ulcers recurred. Therefore, there were different follow-up times for analyzing medical records within included patients; patients registered in 2014 were followed up for five years, and patients registered until April 2018 were followed up just for one year, until April 2019.
Data collection was implemented after the Healthcare Provider Research Ethics Committee's approval (Number 3137875), which exempted the project from applying informed consent.
The researchers developed the instrument for data collection based on previous published venous ulcer epidemiological studies and the variables available in the electronic medical records for the entire sample. The following variables were collected: demographic (sex and age in years) and clinical (presence of comorbidities, smoking, diagnosis of Diabetes Mellitus, Systemic Arterial Hypertension, and heart disease. Presence of obesity diagnosed by Body Mass Index in Kg/m2), as well as variables related to venous ulcers (recurrence time in days and recurrent venous ulcer location). The patient's current situation in the healthcare provider (currently in treatment, abandoned treatment, inactive, discharged) was collected to control loss of follow-up during the data collection period.
Firstly, the collected data were inserted in the Research Electronic Data Capture (REDCap), a web-based workflow research data collection and electronic management tool. 29 The data were subsequently exported to a Microsoft EXCEL® spreadsheet application and analyzed using the free statistical software R 3.6.1. 30 Descriptive statistics were performed, with absolute (n) and relative (%) frequencies calculated for categorical variables; and central tendency measures for numerical variables such as mean, standard deviation, minimum and maximum values. Individuals with unclear ulcer etiology, an unhealed venous ulcer, or more than 10% missing data were excluded from the sample.
For the probability statistics, associations between the dependent variable (presence of venous ulcer recurrence) and the independent variables (demographic and clinical) were analyzed using the Chi-squared test. The non-parametric Wilcoxon-Mann-Whitney U test was used for numerical variables, comparing whether there was a significant difference in age between patients with or without venous ulcer recurrence. A binary logistic regression model was also performed, using all variables to verify possible recurrence predictors.
The Receiver Operating Characteristic Curve (ROC) was calculated to assess the predictive quality of the regression, which represents the accuracy or overall performance of the test, as it considers all sensitivity and specificity values for each variable value. 31 The relationship between the area under the ROC accuracy classifies logistic regression as excellent (0.80 to 0.90), very good (0.70 to 0.79), good (0.60 to 0.69), and poor (0.50 to 0.59). 32 The logistic regression model showed good accuracy (0.60 to 0.69) in the present study, obtaining a ROC of 0.612 (95% CI 0.525-0.698).
Tests that obtained a statistical significance level of 5% for the entire study were considered significant. Only the first recurrence was considered to calculate the incidence of recurrent venous ulcer, using the following formula: venous ulcer recurrence incidence = Number of patients with recurrent venous ulcer / Total number of patients with healed venous ulcer × 100.
Results
For the study purposes, 874 patients treated at the Outpatient Clinic from 2014 to 2018 were screened. After the inclusion criteria analysis, 659 patients were excluded for having wounds from other etiologies, 18 for having vascular ulcers with mixed or unclear etiology, and 63 for having an active venous ulcer during the data collection. Consequently, 197 patients with venous ulcers were selected as a target population with a final sample composed of 134 patients with healed venous ulcers as described in Figure 1. There were no excluded individuals due to missing data.
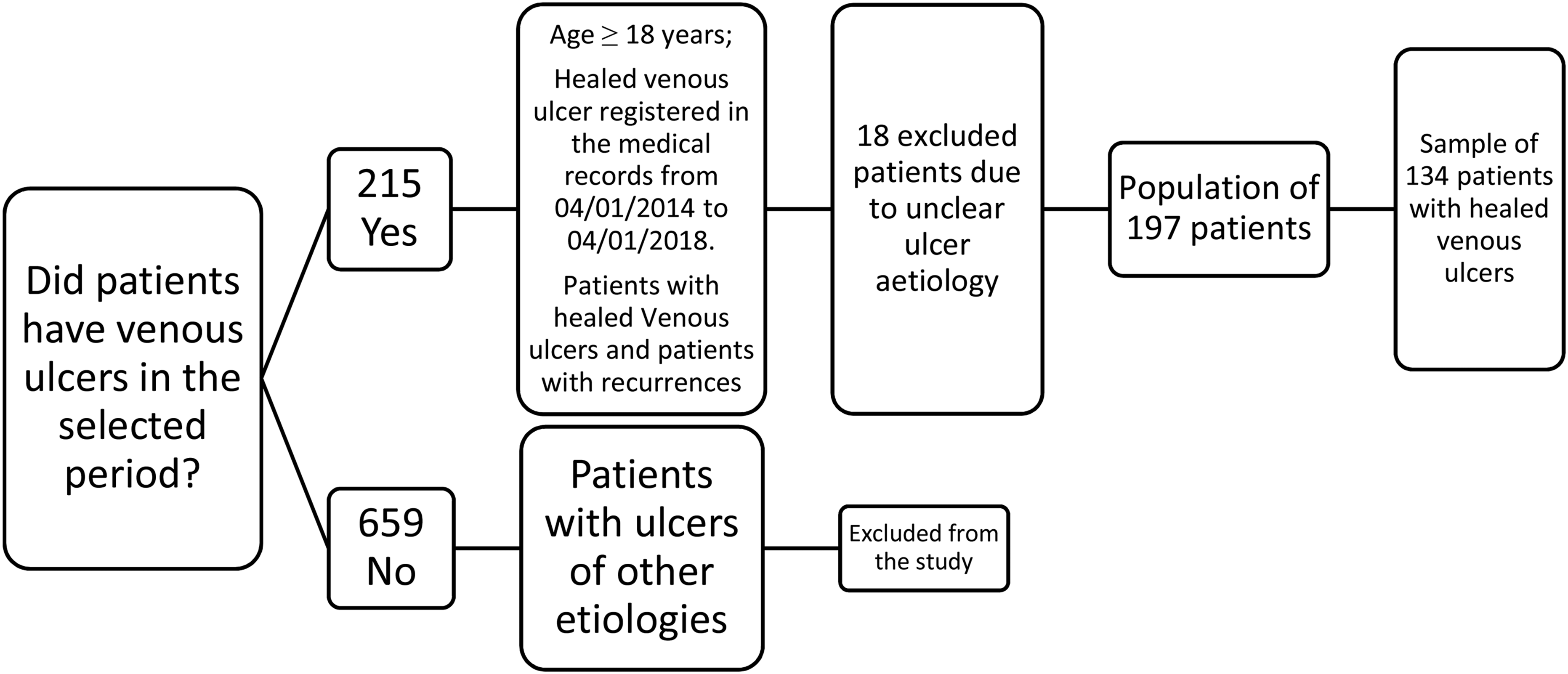
Flow diagram of patients’ inclusion in the final sample size.
The average age of 134 patients was 63.5 (SD = 15) years, ranging from 27 to 88 years, with a predominance of females (81/60.4%). Comorbidities were present in 112 (84.8%) patients, and hypertension was the most frequent among them (92/69.7%).
Sixty-five (65) of the 134 healed venous ulcer patients had a recurrence, so the incidence was 48.5%, all of which had only one recurrence during the follow-up. Recurring time ranged from 27 to 1078 days (from 1 to 36 months), with an average of 230.1 days (8 months) and a standard deviation of 267.0 days after discharge from the service with total ulcer healing.
Patients with recurrent venous ulcer (n = 65) were mainly women (39/60%), with a mean age of 64 years (SD 15.4), minimum age of 27 years, and a maximum of 88 years.
The predominant location of recurrent ulcers was in the medial malleolus, represented by 27 (41.5%), followed by the lateral malleolus 16 (24.6%), and in other regions, including the middle and distal third of the leg, composing a total of 22 (33.8%) cases.
Regarding the clinical characteristics of the patients with recurrent venous ulcer, 57 (50.8%) had some comorbidity, the most frequent being hypertension (47/51%) followed by Diabetes Mellitus (25/53.1%), obesity (15/88.2%), and heart disease (14/60.8%). Only one patient was registered as a smoker.
Table 1 shows the associations between groups with and without venous ulcer recurrence according to the demographic variables (gender and age), in which there were no statistically significant differences between groups with and without venous ulcer recurrence. Table 2 shows the associations between groups with and without venous ulcer recurrence according to the clinical variables.
Associations between Groups With and Without Venous Ulcer Recurrence According to the Demographic Variables in an Outpatient Clinic.
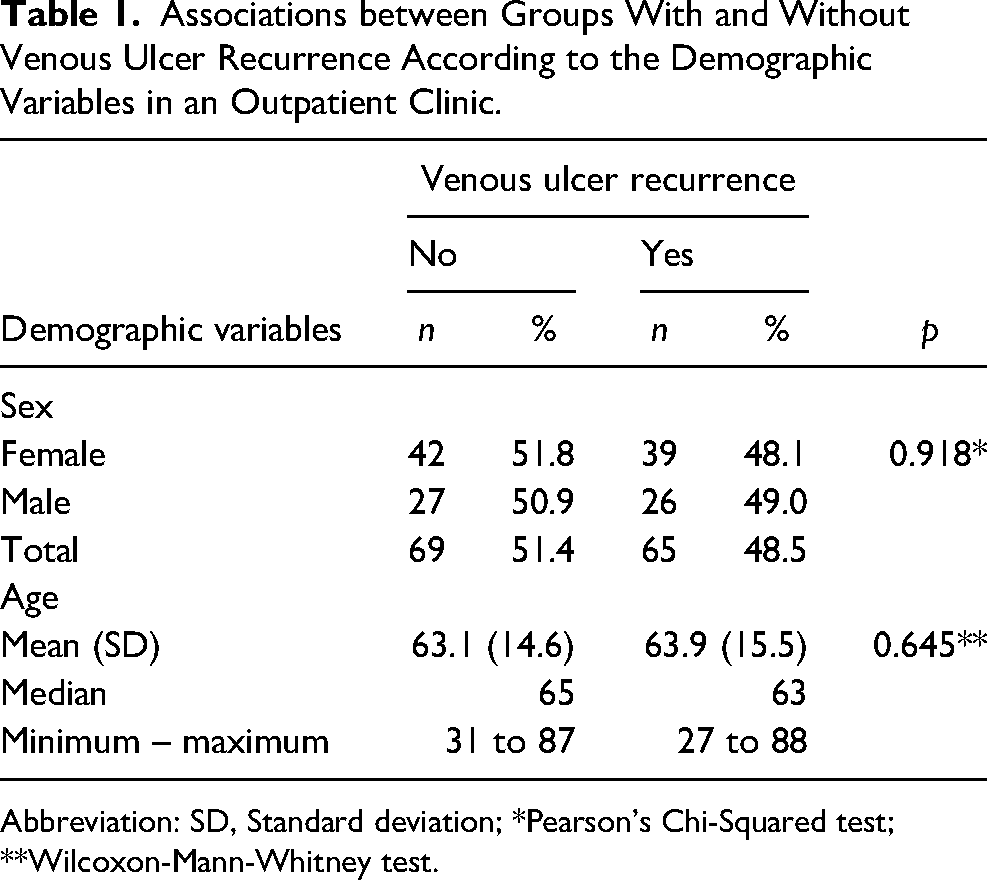
Abbreviation: SD, Standard deviation; *Pearson's Chi-Squared test; **Wilcoxon-Mann-Whitney test.
Associations Between Groups with and Without Venous Ulcer Recurrence According to the Clinical Variables in a Cohort of Adults Treated in an Outpatient Clinic.
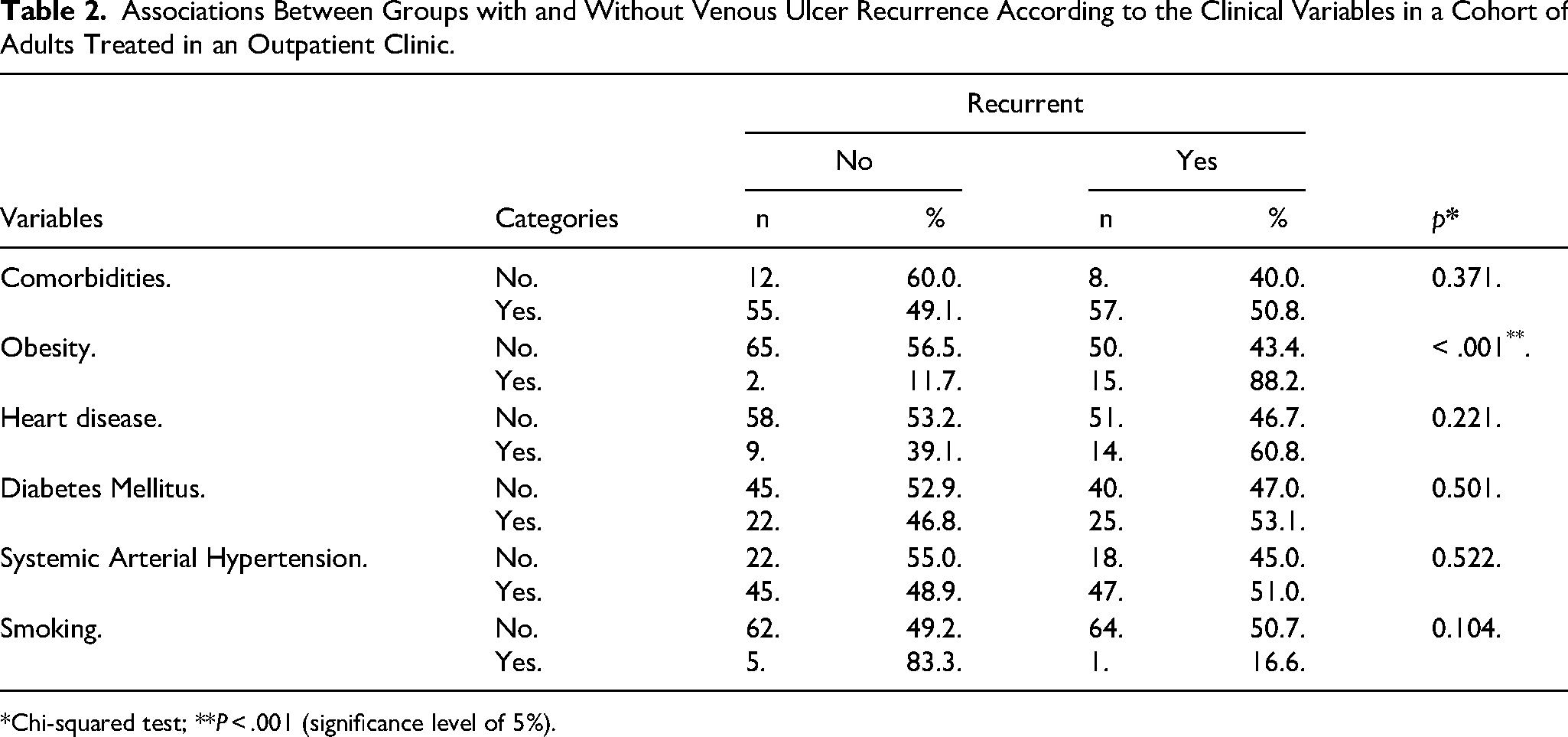
*Chi-squared test; **P < .001 (significance level of 5%).
Obesity was the only clinical variable associated with venous ulcer recurrence (p = .001). Table 2 shows that 88% of obese patients had a recurrence, while the rate for the other variables was around 50%.
Table 3 shows the logistic regression of the study variables for venous ulcer recurrence. Venous ulcer recurrence in patients treated at an outpatient clinic.
Logistic Regression Prediction of Recurrent Venous Ulcer Risk Factors in Adults Treated at an Outpatient Clinic.
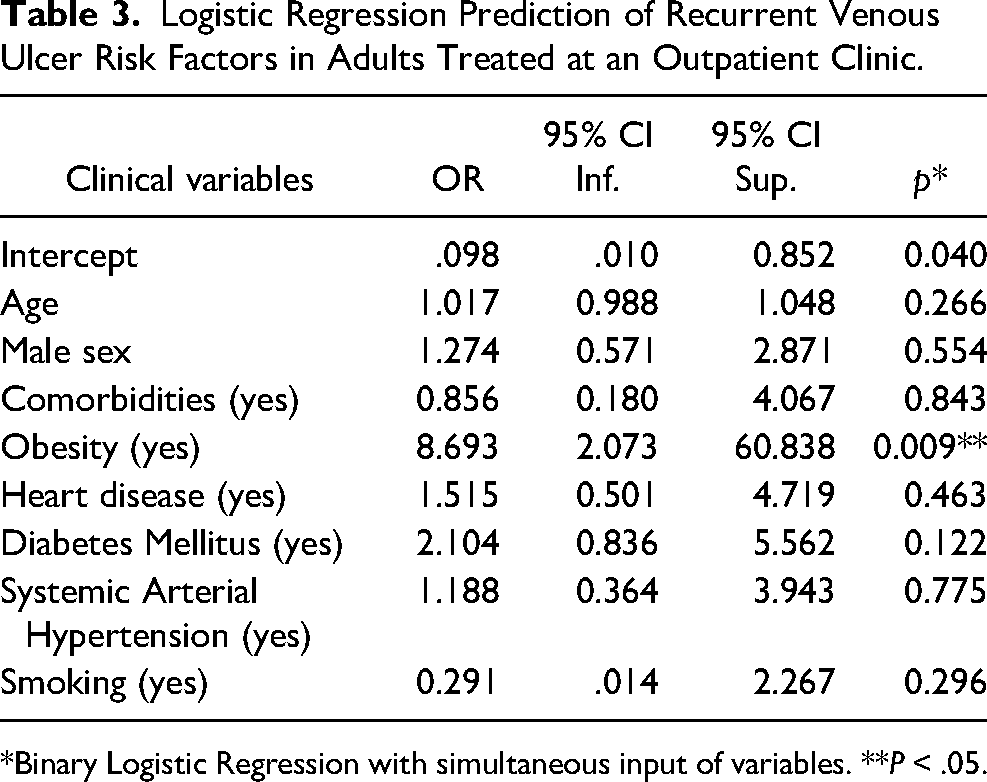
*Binary Logistic Regression with simultaneous input of variables. **P < .05.
Obesity was the logistic regression model's only predictor of venous ulcer recurrence (P = .009). Obese patients were 8.7 times more likely to have venous ulcer recurrence than non-obese patients (95% CI 2.073-60.838).
Discussion
The risk, or the venous ulcer recurrence, is part of the burden experienced by people with advanced Chronic Venous Disease, possibly increasing the negative impact on their quality of life33,34 due to the possibility of entering to a repeated suffering cycle in addition to the high personal and social cost of the disease. 5
The lack of epidemiological data about venous ulcer recurrence compared with the extensive literature regarding venous ulcer management justified this study which obtained an incidence rate of 48.5% among outpatients who attended a Stomatherapy Clinic at a healthcare provider for private health insurance.
In the available literature, venous ulcer recurrency rates are usually identified as a secondary outcome, leaving just a few studies aiming at the epidemiological exploration of the recurrent ulcers. A systematic review which aimed the description of the global profile of individuals with venous ulcers included 20 epidemiological studies from different countries, three of which reported venous ulcer recurrence, allowing the calculation of 56% as a pooled recurrence rate (n = 156) for the European Union region and 76% (n = 42) for South America. 24 These findings indicate the need for new prevention strategies after healing.
Longitudinal studies from Australia reported 50.5% to 78% in hospitals and community outpatient facilities, and domiciliary care.20,35,36 The identified rate in the present study is similar to those publications, especially close to the prospective cohort performed in ten outpatient clinics, reporting a rate of 50.5% recurrence. 20 A multisite study conducted with individuals recruited from five wound clinics in the same country found a recurrence rate of 52%; 36 however, the same authors’ group published a higher venous ulcer recurrence incidence (68%), analyzing patients’ records from two hospitals and three clinics, six years before the other studies 35 indicating the decrease in the recurrence rates.
Similar high recurrence indicators were found in Brazilian studies reporting rates from 62.2% to 67.9%. A retrospective cohort of 50 adults followed during ten years after their ulcers were healed in the Brazilian southeastern, reported a recurrence incidence of 62.2%, 21 and a cross-sectional study of 154 patients with active ulcers in the Brazilian northeastern, identified a prevalence of 67.9% of recurrences with higher prevalence in patients with ulcers due to secondary etiology (P < .001). 37
Some studies have shown lower recurrence rates. A Swiss historical cohort reported an incidence of 33.1% within 145 patients from three different outpatient clinics. 38 A prospective cohort study in Spain with a sample of patients with 180 ulcers submitted to sclerotherapy identified an incidence of 8.1%, 14.9%, and 20.8% in the first, second, and third years of follow-up. 39
Patients with venous ulcer recurrence in the present study were primarily women over 60 years of age. This information corroborates results from one of the previously mentioned studies, which described a predominantly female population (76%), aged between 26 and 85 years old, with a mean age of 69 years, 54% being more than 60 years of age. 21 A systematic review that explored the global perspective of the venous ulcer patients’ profile also corroborated the predominant age between 47 to 69 years by analyzing 12 studies with 2657 patients in total. 24
Regarding the clinical characteristics of patients with recurrent venous ulcers, the most frequent were hypertension (47/51.0%) followed by Diabetes Mellitus (25/53.1%), obesity (15/88.2%), and heart disease (14/60.8%). These data are corroborated by an Australian secondary study, which combined the results of three previous prospective longitudinal studies totaling 250 adults attending wound clinics and reporting hypertension (43%) and heart disease (29%) as frequent comorbidities. 36
Those chronic diseases are in many cases associated with overweight or obesity. Obesity was the only identified predictive factor for venous ulcer recurrence in this study, increasing the risk 8.7 times compared to non-obese patients. A retrospective cohort study involving 325 patients with 345 venous ulcers that analyzed data through artificial neural network technique demonstrated that poor healing was significantly related to obesity, among other factors such as a history of previous ulceration, high amount of exudate, and age. The study also highlighted that obesity influences venous disease, although insufficient evidence supports a direct association between ulcer development and obesity. 21
Obesity is recognized as a risk factor for chronic venous insufficiency in men and women, mainly over 60 years old,5,40 due to the intra-abdominal pressure increase causing resistance to venous return, leading to venous outflow disorder. Additionally, overweight and obesity are related to low physical activity due to the reduced calf muscle pump function secondary to the disturbing range of ankle motion. Obesity-associated clinical conditions also difficult mobility by cause of cardiovascular, respiratory, and osteomuscular issues, characterizing the person's sedentary lifestyle. Obesity-related physiological changes as the increase in adipokine secretion, venous outflow disorder, possible venous outflow obstruction, and reduced mobility can lead to systemic inflammation, causing microcirculatory dysfunction, which altogether can lead to leg ulceration. 40
Obesity also acts as a disease with insufficient immune system response, which may negatively influence wound healing. 41 A prospective study on quality of life conducted with 27 patients with chronic wounds in two specialized outpatient services showed that obesity was statistically associated with an inferior quality of life. 42
The location of venous ulcer in the medial and lateral malleolus anatomic region was predominant as other venous ulcer recurrence characteristics. Considering that obese patients have difficult mobility, the foot's visualization and manipulation can be a problem in many cases, justifying why those areas could be more compromised. This result corroborates a retrospective cohort study with 94 patients and 137 venous ulcers whose authors commented that the most affected anatomical region was the gait area (2.5 cm below the malleolus to the point where the calf muscles detach posteriorly). 43
In the present study, the mean venous ulcer recurrence time was eight months, similar to results from a study about recurrence prevention, which identified an average of 7.9 months for venous ulcer recurrence. 15 A systematic review on the subject showed an absence of studies reporting this outcome, thus highlighting its importance because this data would facilitate the performance of survival analyzes. 44
Literature including systematic reviews on preventive measures to avoid the recurrence of venous ulcers recommend chronic venous ulcer complementary therapies when necessary, including surgery and regular medications, comorbidities control, and educational actions, highlighting: the placement of compression stockings before getting out of bed; regular socks change (from 3 to 6 months); the use of socks that correspond to the diameter and length of the leg, measured by a professional or trained person; quit smoking; adopting healthy nutrition and controlling body weight; avoid mechanical trauma to the injured leg; raising the legs above heart level several times a day, and regular physical activity.45-47
The present study results should be analyzed considering its limitations: retrospective methodology, lack of information about the disease, prevention interventions, and limited follow-up. The retrospective methodology does not assure the registered information's reliability. Collecting data from clinical records without desirable variables such as varicose veins, post-thrombotic syndrome, wound etiology differential diagnosis as septic thrombophlebitis (due to drug abuse or intravenous drug disorders that can evolve to skin necrosis), and compression therapy made impossible the exploration of further associated factors. Another limitation was the discontinuity of post-discharge follow-up due to the withdrawal of some patients from the outpatient clinic or the health insurance, limiting the characterization of preventive measures outcomes, such as elastic stockings adherence and the evolution of the chronic venous disease.
In addition, clinical records did not have formal registration of educational interventions applied to patients during venous leg ulcers management, including the guidance of skincare and compression therapy, even though specialized nurses had as practice recommending those practices verbally to patients. Moreover, the present study population did not have covered the stockings by the healthcare insurance, compromising peoples’ adherence to the preventive measures.
It is hypothesized that some of the present study patients may have adhered to the compression therapy, regardless of the lack of documentation, which explains the identified incidence lower than other published records. Better implementation of educational interventions on prevention could have decreased the recurrence rate, as confirmed in a similar cohort where stockings, rest, and moisturizer in lower limbs skin was associated with recurrence prevention (p = .043), 21 as well as mentioned by other published studies.48,49
Studies with further analysis, including vascular disease characteristics, venous ulcer characteristics, and venous ulcer topical treatment and educational interventions, are necessary to understand better the risk factors for venous ulcer recurrence, contributing to the establishment of more effective venous ulcer prevention and management in outpatient settings.
The present study positively impacted the local nursing clinical records system by updating the registered variables during the stomatherapy nursing consult. The result was the implementation of a robust electronic medical record specific to the stomatherapy outpatient clinic, which includes all parts of the Nursing Care Systematization; moreover, through the complexity of the information, which is required, these records can also direct the findings to the necessary interventions aiming at quality of care, management, prevention, and follow-up of the patients with a venous ulcer.
Implications for Clinical Practice
Based on the present results, it is recommended that local multi-professional teams work together for the improvement of the venous ulcer recurrence prevention guidelines, beginning in recognition of the problem through calculation of the local prevalence and incidence as well as associated local variables; to know better the population and identifying those conditions that need special attention, as in this study was the presence of “obesity.”
Despite this study, there are still few publications on the subject, leading to an absence of epidemiological records, which hinders decision-making and the implementation of improvement projects at the managerial level, especially in outpatient clinics.
After that, it is recommended to create venous ulcer prevention programs based on the specific characteristics of the local attended population. 46 This process could be performed through educational programs for patients and clinicians, protocols, and outcomes monitoring using electronic medical records.
Conclusions
This study identified a venous ulcer recurrence incidence of 48.5%. Obesity was the leading risk factor that increased the chances of recurrence by 8.7 times. The epidemiological exploration of venous ulcer recurrences allowed the characterization of target interventions and the recognition of prevention bundle need after wound healing, including comorbidities control optimization, compression therapy, skincare, and weight control. Comprehensive clinical records with specific variables related to chronic venous disease, treatment, and prevention are essential for retrospective epidemiological exploration of risk factors.
Footnotes
Acknowledgments
To the health insurance provider Amil's managers and leaders for the permissions to implement this project in the Stomaltherapy Nursing Service. To Catia Araujo for contributing to the data collection. To Bernardo Santos for statistical analysis and consulting. To Prof. Dr. Kevin Woo by the scientific advice during the preparation of this paper.
Declaration of Competing Interests
Michele N.B. Rocha declares being an employe at ConvaTec® Medical Care Brazil since 2020. Carol V. S. González declares having received a doctorate scholarship from Coordination for the Improvement of Higher Education Personnel CAPES and personal fees for consulting for 3M-KCI® by not related to the present study. Eline L. Borges declares having received funding from the Research Support Foundation of the State of Minas Gerais – FAPEMIG. Process no CDS - APQ-00904-15 for research development by not related to the present study. Vera L.C.G. Santos declares having received a faculty scholarship from the National Council of Scientific and Technological Development – CNPq. She also reports the licensed patent No. BR 10 2013 032620-8 by not related to the present study. Soraia A.N. Rabeh does not declare any competing interest. Paula C. Nogueira declares having received a faculty scholarship from the National Council of Scientific and Technological Development – CNPq, Process No BR 421154/2018-7 by not related to the present study.
Funding
This study was partially financed by the Coordination for the Improvement of Higher Education Personnel (Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - CAPES) - Finance Code 001. Funding role: the funding agency did not interfere with the study design, data collection analysis or interpretation, writing of the report, nor the decision to submit the article for publication.
Author Contributions
Michele N.B. Rocha: conception and project administration, design of the study, data curation, data interpretation, manuscript writing, and final approval. Carol V.S.González, Eline L. Borges; Vera L.C.G. Santos; design of the study, data interpretation, manuscript review, editing, and final approval. Soraia A.N. Rabeh: design of the study, manuscript review, and final approval. Paula C. Nogueira: conception and project administration, design of the study, validation and supervision, data interpretation, manuscript review, editing, and final approval.
Data Sharing
Research data (database, informed consent, and statistical analysis plan) will be available with as few restrictions as possible. Requests should be sent to the corresponding author.
Ethics Approval
This article's study was approved by the Hospital Pró-Cardiaco ESHO Empresa de Serviços Hospitalares in Brazil, No. No. 3137875.