
Abstract
We reviewed donor site wound healing among morbid ≥65-year-old patients after split-thickness skin graft (STSG) harvesting. Patients were treated for a pretibial laceration or hematoma in Kymenlaakso Central Hospital, Finland, between 2015 and 2019. Twelve morbid patients with a mean Charlson Comorbidity Index of 7.1 (range 4-12) and a mean age of 80.6 years (range 69-91) were studied. Nine patients were female. Eight had a chronic cutaneous fragility syndrome, eg, dermatoporosis. All donor site areas were located on the thigh and were less than 2% TBSA. One donor site infection occurred. STSG integration on the pretibial wound bed was successful with all patients, and none of the patients needed further operative treatment. Graft thickness varied between 0.010 to 0.014 inches. STSG donor sites healed within the normal range of 21 days in 50% of patients. Among two patients, healing took 25 days, and among four, 37 to 97 days. All donor sites healed via local wound care without the need for regrafting. 4Our study indicates that harvesting STSG from elderly and morbid patients with poor skin condition is safe and does not result in significant complications. Prolonged donor site healing can occur, which can be managed with regular local wound care.
Introduction
Managing the donor site wound after split-thickness skin graft (STSG) harvesting is important since delayed healing in the donor site may cause pain, discomfort, and a poor cosmetic outcome.1,2 Local treatment of the donor site aims to create an environment that facilitates re-epithelization, minimizes pain, decreases the risk for local infection, and reduces hospital stay. 3
STSGs are considered one of the most indispensable methods for reconstruction of cutaneous and subcutaneous defects.2,4,5 STSGs are the third step in the reconstructive ladder, right after healing by secondary intention and primary wound closure. 4 STSGs serve a fundamental role in various clinical situations such as treating burns, traumatic wounds, chronic wounds, and particular defects after oncologic resections.2,5,6 Harvesting an STSG leads to a sheet of the skin consisting of the epidermis and a varying thickness of dermis, leaving sufficient dermis on the donor site for secondary healing to occur via re-epithelization.2,7
In general, healthy patients heal their STSG donor site without problems.2,8 However, especially elderly patients may have comorbidities and dermatoporosis that can affect wound healing. 9 Dermatoporosis is a distinct medical entity that leads to chronic skin fragility.10,11 The clinical features include senile purpura, stellate pseudoscars, and atrophy of the dermis and epidermis.10–13 The use of systemic and topical corticosteroids, genetic factors, and environmental factors such as UV-radiation all contribute to the development of dermatoporosis.10–13 However, dermatoporosis is not restricted to these factors and its prevalence is estimated to be around 30% in individuals aged over 60 years. 14 Other comorbidities that can complicate healing are diabetes, chronic venous impairment, peripheral vascular disease, malnutrition and immunocompromised states. 15
With elderly patients, previous literature suggests immediate regrafting of the STSG donor site with remaining excess skin to facilitate healing.1,8,16 Routine donor site healing generally happens between 7 to 21 days.2,15 Infections of donor sites are generally rare, though they have been described in several patient cohorts with an incidence of 0 to 56% in a systematic literature review. 2
This study aimed to review the outcome and healing of STSG donor sites in morbid elderly patients with dermatoporotic skin.
Patients and Methods
The Institutional Review Board of the hospital approved this retrospective chart review study and its protocol.
We performed an electronic search using the LifeCare® patient database of Kymenlaakso Central Hospital for all patients diagnosed with a pretibial injury from first January 2015 to 31st December 2019 in the central hospital or its surrounding smaller health care centers.
This study included patients aged ≥65 years who underwent STSG on their pretibial laceration or hematoma after surgical debridement. Computerized medical records of all included patients were reviewed by one author (TS). Factors reviewed included age, gender, Charlson Comorbidity Index (CCI), dermatoporosis, Clavien-Dindo classification for postoperative complications, graft integration on the wound bed, donor site location, donor size area (% TBSA), donor site dressings, donor site infections, graft thickness (in), mesh ratio, donor site follow up visits and healing.
Prolonged healing of the STSG donor site was defined as being >21 days based on the previous literature.2,15 Donor site healing was reviewed from nurse or physician recordings, and complete healing was accepted when no further dressing changes were needed. Dermatoporosis was confirmed based on patient photographs and medical history files descriptive text including “parchment-skin, paper-thin skin, cortisone-skin, and very fragile skin”.
Results
The specific inclusion criteria resulted in 15 patients. Nine (60%) were treated for a pretibial hematoma and six (40%) for a pretibial laceration. One patient died shortly after surgery due to unrelated aortic valve stenosis and heart failure. Two patients were treated postoperatively in nursing homes, so further information on healing was not available.
Thus, 12 patient donor sites and wound beds were reviewed for healing. A majority, nine, of the patients were female. The mean age was 80.6 years (range 69-91). Eight patients had advanced dermatoporosis. Mean CCI was 7.1 (range 4-12). All donor site areas were less than 2% TBSA. One minor donor site infection classified as a Clavien Dindo 1 complication occurred. The patient's infectious donor site discharge cultivated sensitive staphylococcus aureus bacteria recurrently and was treated with frequent dressing changes and per oral cephalosporins. No other postoperative complications were noted. Graft intake on the wound bed was successful in all cases. See Table 1 for detailed demographic data of all 12 patients and Figure 1 for the donor site infection.

Minor donor site infection with staphylococcus aureus cultivated from discharge. Image of this dermatoporotic patient was taken after wound care 30 days post STSG. The infection healed with per oral antibiotics and frequent dressing changes.
Demographic Data of 12 Patients Treated with a STSG in Order of Healing Time.
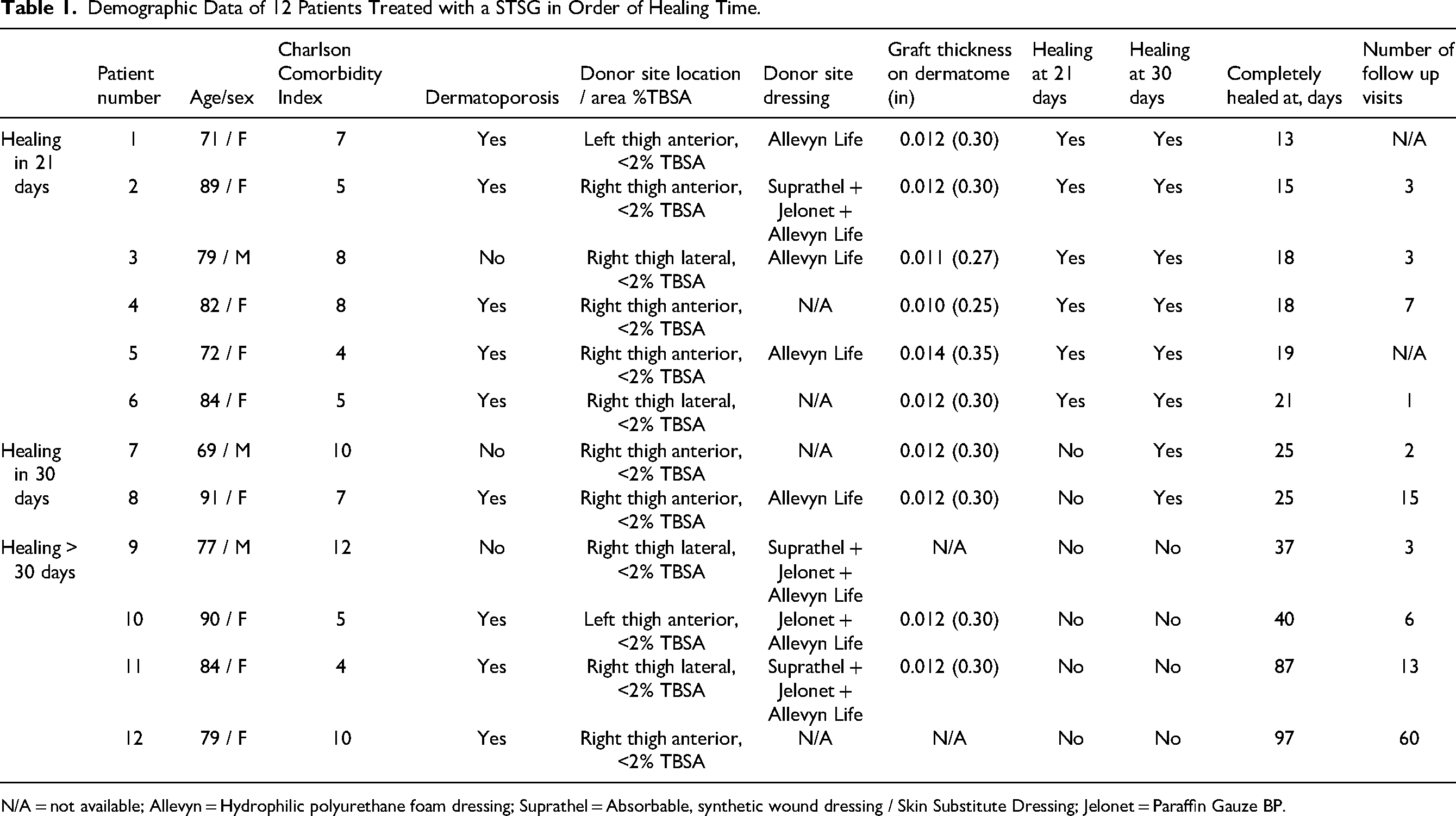
N/A = not available; Allevyn = Hydrophilic polyurethane foam dressing; Suprathel = Absorbable, synthetic wound dressing / Skin Substitute Dressing; Jelonet = Paraffin Gauze BP.
Grafting and Donor Site Dressings
All STSGs were taken with a Zimmer™ dermatome from the ipsilateral thigh and meshed 1:1.5. Specific anatomic location was the anterior thigh in 8 patients and lateral thigh in 4 patients. Graft thickness was 0.010 inches in 1, 0.011 in 1, 0.012 in 7 and 0.014 in 1. In two patients, graft thickness was not reported.
Detailed use of donor site dressings was reported in nine patients. A hydrophilic polyurethane foam dressing (Allevyn™) was used in all patients, which was advised to be removed between 14 to 21 days postoperatively. In addition, a skin substitute dressing (Suprathel™) was used in three patients, and a paraffin gauze was placed on the donor site before applying Allevyn™.
Donor Site Healing and Follow-up Visits
None of the donor sites were regrafted immediately or later. The first dressing removal took place between 6 to 25 days postoperatively (mean 15.3). The mean overall healing time was 34.7 days (range 13-97). The mean amount of follow-up visits, including donor site dressing changes, was 11.3 (range 1-60).
Six patients’ donor site healing was prolonged for over 21 days (range 25-97). With two patients, healing took 25 days, and with four, 37 to 97 days. All donor sites healed via local wound care without the need for regrafting.
Discussion
We analyzed donor site healing of ≥65- year-old patients with pretibial injuries treated with an STSG. Our cohort consisted of 12 patients with a mean age of >80 years and unambiguous dermatoporosis in eight patients. Half of the patients healed within the expected time range of 7 to 21 days. The other half experienced prolonged donor site healing, but only four patients healing took over a month. All donor sites healed with local wound care. One donor site infection occurred, contributing to prolonged healing.
Graft thickness in this study was relatively high considering the frailty of patients and the high incidence of dermatoporosis. Immediate regrafting was not used despite literature recommendation.1,8,16 Donor site healing time among frail patients could be shorter if a thinner graft (eg, 0.008in) was used and excess skin grafted back immediately. Moist wound-healing dressings should be used routinely on donor sites. 7
Pretibial skin defects among elderly patients often become chronic, requiring tens, even hundreds of wound care appointments. 9 STSGs are typically used only when long conservative treatment is uneventful, even though previous studies have shown that patients with chronic wounds benefit from STSGs to improve health-related quality of life. 17
Our cohort patients’ graft intake on wound bed was 100%. Even though donor site healing was prolonged with half of the patients, chronic wound formation from traumatic pretibial injury defects can be considered a more unfavorable outcome. Primary operative treatment can be refrained gratuitously in fear of complications regarding operative treatment with a frail patient group.
This study implicates that skin grafting is safe and can be mini-invasive as small STSGs can be harvested under local anesthesia.
The limitations of this study arise from its small cohort size and retrospective study design. Thus, data on donor site healing compared to younger patients, postoperative pain and health-related quality of life could not be gathered. A previous study indicated that younger patients of <65 years describe significantly higher postoperative pain on donor sites than elderly patients. 17
To conclude, donor site healing can be prolonged with elderly patients. However, no significant complications were recorded despite poor skin conditions and high patient morbidity. Using an STSG to prevent pretibial skin defects from becoming chronic wounds seem reasonable. Access for dermatomes should be alleviated in an outpatient setting to encourage early and mini-invasive treatment of pretibial skin defects. Prospective randomized controlled studies on donor site healing among dermatoporotic patients and conservative versus operative management of pretibial injuries are needed since the incidence of chronic wounds and pretibial injuries are estimated to increase as the population ages.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.