
Abstract
Diabetic peripheral neuropathy (DPN) is one of the risk factors for foot-related complications among people with type 2 diabetes mellitus (T2DM). Hence, we aimed to validate the Michigan Neuropathy Screening Instrument (MNSI) tool against biothesiometer with a cut-off value of ≥25 V and also to determine the cut-off point of MNSI score for the diagnosis of diabetic neuropathy among people with T2DM in India. A cross-sectional study was conducted among 357 people with T2DM in a tertiary care centre for diabetes in Chennai, South India. The eligible study participants underwent testing with a biothesiometer and the MNSI tool was administered. The patient version tool of MNSI was translated to the local language, Tamil. The MNSI scores (1, 1.5, 2, and 2.5) were compared with biothesiometer value. For the MNSI scores of less than 1, 1.5, 2, and 2.5, sensitivities were 97.6%, 97.6%, 96.8%, and 77.8% and specificities were 76.6%, 77.9%, 85.7%, and 88.3% respectively. The cut-off value of MNSI score was derived as two with AUC of 0.934. The sensitivity was 96.8% and the specificity was 85.7% with 89.6% accuracy. The high sensitivity indicates the positive cases are diagnosed correctly. There is no validated tool available for detection of DPN in Indian population. The Indian version of MNSI tool was found to be effective for screening diabetic neuropathy among people with T2DM. The MNSI tool was found to be reliable, convenient, and non-invasive for diagnosis of DPN and can be used in routine clinical settings.
Introduction
In India, 74.2 million people are currently living with diabetes which is predicted to rise to 124.9 million by the year 2045, according to the recently released International Diabetes Federation Atlas. 1 Diabetic peripheral neuropathy (DPN) is the most common complication of diabetes, almost 50% or more people with diabetes develop DPN. The prevalence of DPN varied between 9.6% to 78% in different populations in India.2–5 DPN causes foot complications which lead to severe morbidity and mortality. 6 The foot complications also contribute to the individual's financial burden. 7 Hence, prevention, timely detection, and treatment of DPN play a vital role in reducing the disease burden.
The nerve conduction study (NCS) is considered as a gold standard test for the diagnosis of DPN which evaluates the occurrence and development of neuropathy by detecting the ability of the peripheral nerve to transmit electrical signals in individuals. The test is time-consuming, expensive, and requires professional training to conduct the test. 8 Vibration perception thresholds (VPT) using biothesiometer is used to detect peripheral neuropathy. 9 Based on clinical signs and symptoms, quantitative sensory testing, sudomotor function, neurophysiology, skin punch biopsy, and corneal confocal microscopy can be used. Each method has its own advantages and disadvantages. 10 Biothesiometer utilises an electronic device that accurately records the vibration and this test has a high sensitivity of 82% and specificity of about 70%, with good reproducibility.11,12
To overcome the difficulties in performing gold-standard diagnostic tests, some early screening methods are used to diagnose DPN. Several clinical scoring systems have been developed using tools to assess the presence and severity of DPN. 13 One easy-to-use, inexpensive and non-invasive tool which can be used by both patient and physician is the Michigan Neuropathy Screening Instrument(MNSI). The MNSI is used to assess DPN based on patient's self-reports and physician clinical examination. 14 There is no validated tool available in India for easy assessment of DPN in a routine clinical setting. There is a need for validation of a simple non-invasive tool to assess signs and symptoms of DPN. Hence, this study may throw light on whether a reliable and convenient tool can be used for detection of DPN in routine practice. MNSI utility has been validated and discussed in several populations but not in people with diabetes in India. Hence, this study aimed to validate the MNSI tool and to determine the cut-off point of MNSI scoring for the diagnosis of diabetic neuropathy among people with type 2 diabetes from India.
Methods
This cross-sectional study was done among 357 study participants with type 2 diabetes in a tertiary care centre for diabetes, Chennai. South India between January 2021 and April 2021. Both gender aged above 18 years were included to compare the scores of MNSI and the Vibration perception threshold testing using a biothesiometer for the diagnosis of DPN. The study participants who were diagnosed with peripheral neuropathy caused by reasons other than diabetes were excluded from participating in this study (e.g., Vitamin B12 deficiency, alcoholism, and exposure to toxins) based on the clinical history, physical examination, and laboratory findings. Participants who speak other languages were excluded from this analysis. Biothesiometer test (BT) was conducted among all the study participants and the results were recorded. The biothesiometer values of 25 and above were considered neuropathy. 12 MNSI tool was administered to the study participants (both the patient version and the physical assessment), and the results were recorded. 14 BT and MNSI tool was administered to all the participants who voluntarily consented to participate in the study. The person who performed the biothesiometry was blinded to the MNSI Score. Other information like age, gender, duration of diabetes, treatment of diabetes, blood glucose levels, body mass index (BMI), personal habits like smoking and alcohol status, systolic and diastolic blood pressure were recorded. The study was approved by the Institutional Ethics Committee (IEC/N-007/02/2020).
MNSI Tool
Description
MNSI was designed to screen in the outpatient settings (basically in primary care settings) for the presence of DPN. This instrument is provided in two parts: The patient's version and the physical assessment. The patient version (patient symptoms score) has 15 questions related to the DPN symptoms (‘Yes’ or ‘No’ questions), which the study participants answered. The physical assessment was conducted by a trained health professional. This part consists of five segments (clinical score): the appearance of feet, ulceration, ankle reflexes, vibration perception, and monofilament test. The patient’s version was translated to Tamil (Regional language) by a professional translator at the centre. The translated version was sent to the Expert Team for a back translation and checked for the original quality and accuracy. The final MNSI tool with details on assessment is provided in Figures S1 and S2.
MNSI tool assesses neuropathic symptoms (pain, numbness, and temperature sensitivity), circulation impairment, and measure of general asthenia based on questionnaire. This is followed by clinical or physical assessment which includes appearance of feet (deformities, dry skin, callus, infection, fissure), ulceration (present/absent), grading of ankle reflexes, vibration perception threshold (on dorsum of great toe over distal interphalangeal [DIP] joint) along with monofilament testing (on the dorsum of the great toe midway between the nail fold and the DIP joint). Abnormality was determined by the number of positive responses or abnormal clinical findings in both questionnaire and physical assessment. The greater the score of MNSI, greater the risk of diabetic neuropathy.
Training
For proper implementation of the tool, the Expert Team had given training to our trainer who administered the MNSI (Patient version and Physical assessment) to the study participants. This training was held for a period of 3 days (1 day online training and 2 days of in-person training). The training included a theoretical part and practical administration of questionnaire and assessments among the outpatients. The trainer piloted the assessment on a few participants and was cross-checked by the Expert Team.
Statistical Analysis
Descriptive statistics were used to describe the demographic characteristics of the study participants. The distribution of data was not normal (Shapiro–Wilk Test). Hence, Mann–Whitney U Test and Chi-square test were conducted to identify the significance of the differences between groups for continuous and categorical variables, respectively.
Sensitivity, Specificity, positive predictive value (PPV), negative predictive value (NPV), accuracy, likelihood-positive test, and likelihood-negative test were calculated. The area under the receiver-operating characteristic (ROC) curve was estimated for the physical assessment to obtain the cut-off value. All statistical analysis was performed in SPSS Version 27 for Windows.
Results
The mean age of the study participants was 52.3 years (Standard deviation (SD): ± 8 years), the individuals with neuropathy were older as compared to those without neuropathy (P < 0.001). The majority of the study participants were male (Male: n = 244, 68.3% and Female: n = 113, 31.7%). Among 357 study participants, 258 participants were on oral hypoglycaemic agents (OHA: 72.3%), 13 were on insulin (3.6%), and 86 were on a combination of OHA and insulin (24.1%).The mean BMI was 27.6 ± 6 kg/m2. The participants with neuropathy had higher BMI (P = 0.067). The mean duration of diabetes in total participants was 10.1 ± 7.4 years. The participants diagnosed with neuropathy had a higher duration of diabetes than those without neuropathy (P < 0.001). The mean systolic and diastolic blood pressures were 129 ± 17.2 and 76.9 ± 10.2, respectively. The systolic blood pressure was significantly higher among those with neuropathy than without neuropathy with no difference in diastolic blood pressure. Fasting and postprandial glucose levels and HbA1c % was also higher in participants who had presence of neuropathy. There is no difference in lipid parameters among those with and without neuropathy (Table 1).
Socio Demographic and Biochemical Details of the Study Participants.
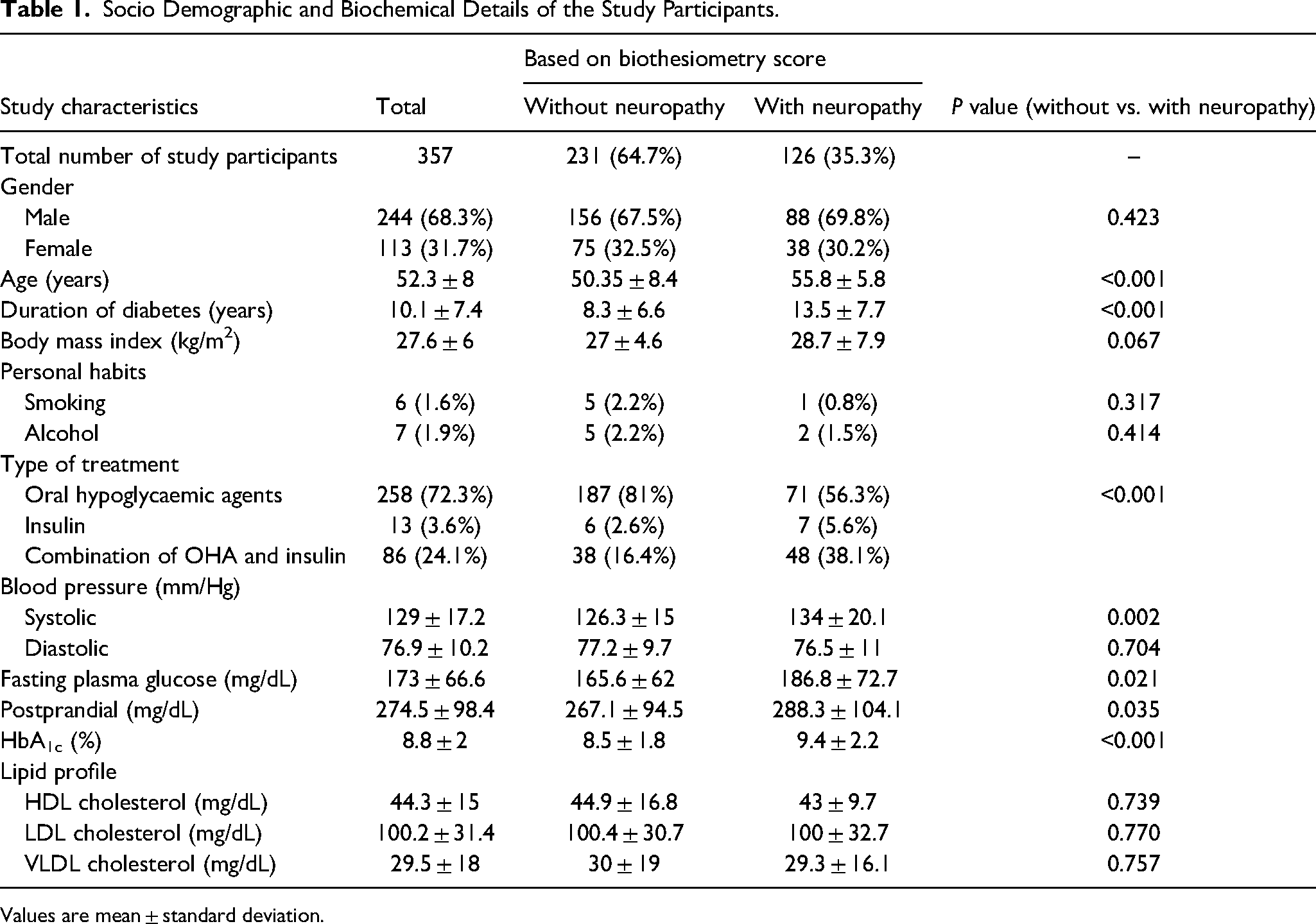
Values are mean ± standard deviation.
Based on the BT (Biothesiometer) values, 126 (35.3%) of the study participants had significant neuropathy, whereas 231 (64.7%) were normal. Table 2 shows the comparison of neuropathy among people with different MNSI scores and biothesiometer.
Comparison of Neuropathy Among Participants with Different MNSI Scores.
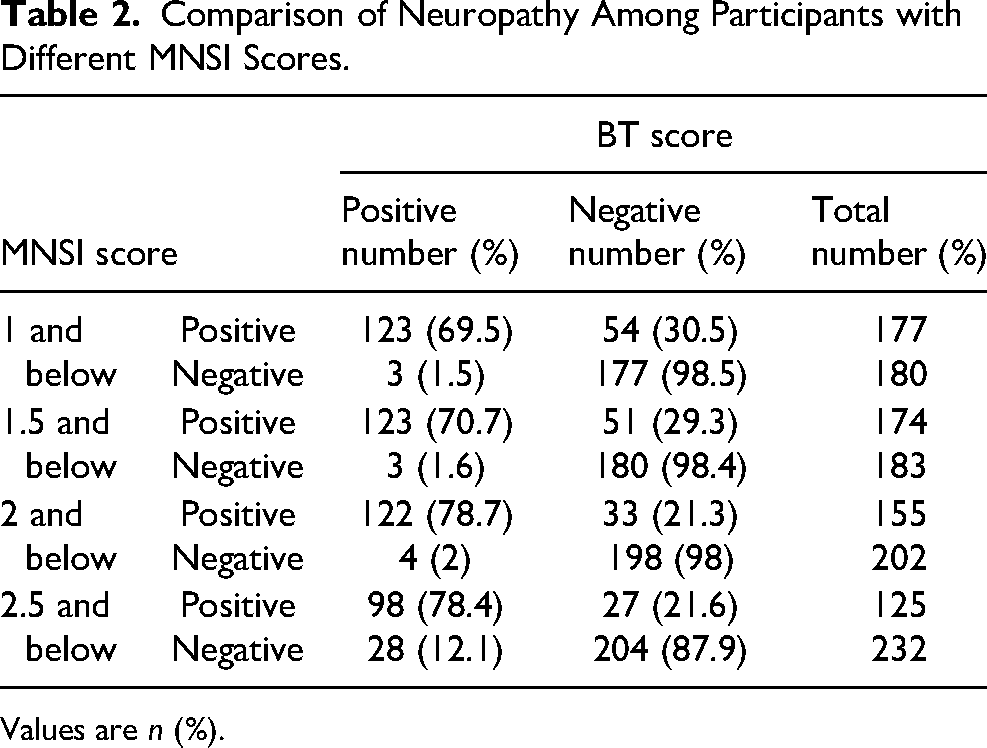
Values are n (%).
Table 3 shows the number of participants with and without neuropathy at different MNSI scores. Peripheral neuropathy was detected among 126 study participants by biothesiometer.
Number of Participants with and Without Neuropathy at Different MNSI Scores.

The agreement between MNSI scores and DPN diagnosis was estimated as shown in Figure 1.
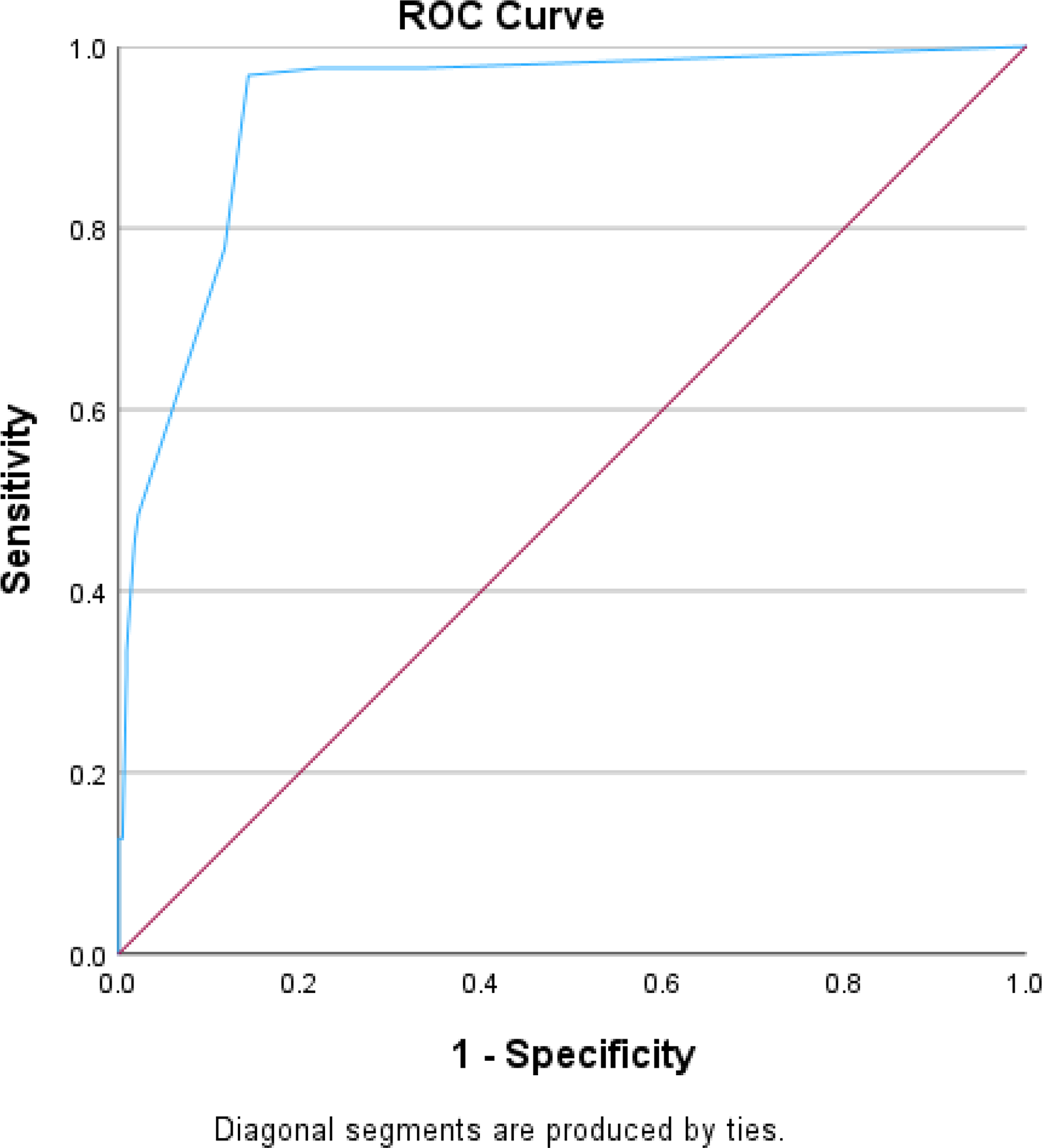
Receiver operating characteristic curve for BT and MNSI physical assessment. Area under the Curve (AUC) = 0.934.
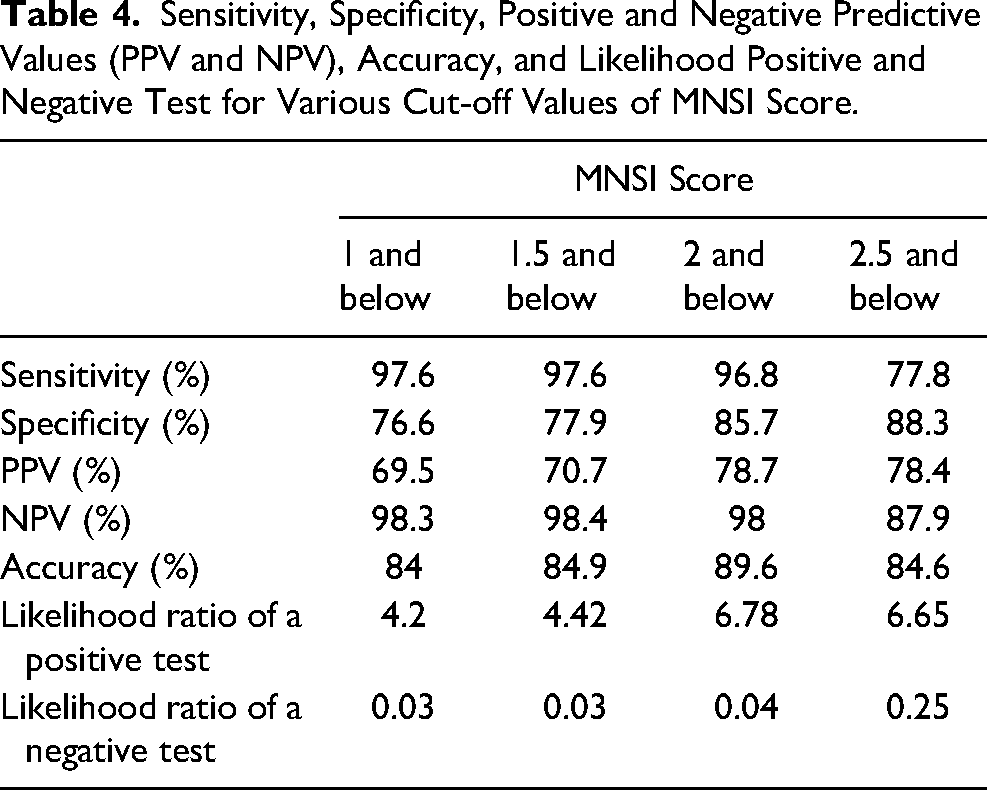
The area under the curve in the ROC analysis was 0.934 for the MNSI score cut-off value of 2 and below. Sensitivity, specificity, positive predictive values (PPV), negative predictive values (NPV), accuracy, likelihood-positive test, and likelihood-negative test for various MNSI scores were calculated and shown in Table 4. For the MNSI scores of less than 1, 1.5, 2, and 2.5, sensitivities were 97.6%, 97.6%, 96.8%, and 77.8% and specificities were 76.6%, 77.9%, 85.7%, and 88.3% respectively. The sensitivity for the cut-off value of 2 was 96.8%, and the specificity for the same was 85.7%. Accuracy at 1, 1.5, 2, and 2.5 cut-off values were 84%, 84.9%, 89.6%, and 84.6% respectively. The positive predictive value, negative predictive value, accuracy, likelihood positive test, and likelihood negative test for the cut-off value were 78.7, 98, 89.6, 6.78, and 0.04, respectively. The PPV increases from 69.5% to 78.4%, and NPV decreases from 98.3% to 87.9% at different cut points. The highest accuracy (89.6%) is at the cut-off value of 2. The likelihood ratio of a positive test was higher for MNSI scores ≤ 2 and ≤ 2.5.
Sensitivity, Specificity, Positive and Negative Predictive Values (PPV and NPV), Accuracy, and Likelihood Positive and Negative Test for Various Cut-off Values of MNSI Score.
Discussion
To our knowledge, this is the first study to validate the MNSI tool in people with type 2 diabetes from India and to translate the tool to the regional language (Tamil). In this study, we compared the MNSI scores with biothesiometer and noted that the Indian version of the MNSI tool was considered to be effective for screening DPN. Various tool validation studies had been published previously.10,15–18 The Arabic version of the MNSI tool showed 95.9% sensitivity, 62.5% specificity, and 0.93 area under curve value. The study compared the MNSI scores with nerve conduction studies. The cut-off value for this tool was ≥2.5. 18 Another study conducted in Iran derived ≥2 as the cut-off value. The sensitivity, specificity, and accuracy values for this study were 65%, 83%, and 76%, respectively. The area under the curve was 0.815. 19 The Turkish study derived the cut-off value for MNSI as ≥2 and obtained 100% sensitivity, 97.6% specificity, 97.6% positive predictive value, and 100% negative predictive value. The area under the curve was 1.00.15 (Our study replicated good results similar to other studies. The cut-off value derived from our study was 2.0. The sensitivity, specificity, and accuracy were 96.8%, 85.7%, and 89.6%, respectively. The area under the curve was 0.934. The cut-off value of 2 was found to be appropriate which gave the highest sensitivity and specificity. The AUC was also excellent.
We compared MNSI tool with biothesiometer in this study. The biothesiometer measures the vibration perception threshold (VPT) in people with diabetes. The VPT is measured in volts, which is gradually increased until the threshold of vibratory sensation is appreciated by the patient. The measurement of VPT using a biothesiometer is a long-established method for screening patients with diabetic neuropathy. 20 The biothesiometer was found to have 80% sensitivity and 98% specificity for detection of neuropathy. 21 An increased VPT has been found in patients with diabetic foot ulceration [DFU]. A VPT of ≥ 25 V was strongly associated with the risk of DFU. A raised VPT has been found in patients with DFU compared with normoglycemic and people with diabetes without diabetic foot ulcer. 22 MNSI tool in this study can be considered as a reliable tool based on the sensitivity, specificity, accuracy, PPV, NPV, and AUC values. Large fibre neuropathy can be assessed by using this diagnostic cut-off value derived from MNSI in this study. MNSI tool can be used in remote places where access to medical team is limited and also in large-scale epidemiological studies.
MNSI patient version has been demonstrated to be less sensitive than MNSI physical assessment. 17 In our study, MNSI physical assessment has shown good sensitivity and specificity. The cut-off value was determined only for the MNSI physical assessment in our study. The area under the curve (AUC) in our study was 0.934, whereas, in other studies, the AUCs were 1.00, 15 0.677, 16 0.798, 17 and 0.815, 19 respectively. The AUC was used to measure the performance of this tool in predicting the outcome. The AUC value of 0.9 and above was considered as excellent performance, and as the value increases, the performance will improve. 16 We assessed the diagnostic performance by ROC area under the curve for validity. The AUC was 0.934 in our study, which showed that the quantitative measurement of the MNSI test is high. This tool does not screen for autonomic nervous system involvement. 23 The tool was also used in Diabetes Control and Complications Trial (DCCT) study which was a multi-center, randomised controlled trial and clinical study which aimed to determine the intense therapy on the control of diabetes and its complications. 24
Strengths and Limitations
The Diabetes Control and Complications Trial (DCCT) also used MNSI tool for the diagnosis of neuropathy. 24 The training and back-translation was also done by the Expert Team. Another important strength of this study was its large sample size. There are limitations to this study as well. The MNSI tool was not compared with the gold standard method and other widely used tests like monofilament and tip-therm.
Conclusion
In conclusion, the Indian version of the MNSI tool was considered to be effective for screening diabetic neuropathy among people with type 2 diabetes. The cut-off value derived was 2 for MNSI physical examination. Hence, this tool was found to be reliable, convenient, and non-invasive for diagnosis of DPN and can be used in routine clinical settings.
Supplemental Material
sj-jpg-2-ijl-10.1177_15347346231163209 - Supplemental material for Precision of Michigan Neuropathy Screening Instrument (MNSI) Tool for the Diagnosis of Diabetic Peripheral Neuropathy Among People with Type 2 Diabetes—A Study from South India
Supplemental material, sj-jpg-2-ijl-10.1177_15347346231163209 for Precision of Michigan Neuropathy Screening Instrument (MNSI) Tool for the Diagnosis of Diabetic Peripheral Neuropathy Among People with Type 2 Diabetes—A Study from South India by Vijay Viswanathan, Balkhiwala Ahmed Khan, Sukanya Nachimuthu and Satyavani Kumpatla in The International Journal of Lower Extremity Wounds
Supplemental Material
sj-jpg-3-ijl-10.1177_15347346231163209 - Supplemental material for Precision of Michigan Neuropathy Screening Instrument (MNSI) Tool for the Diagnosis of Diabetic Peripheral Neuropathy Among People with Type 2 Diabetes—A Study from South India
Supplemental material, sj-jpg-3-ijl-10.1177_15347346231163209 for Precision of Michigan Neuropathy Screening Instrument (MNSI) Tool for the Diagnosis of Diabetic Peripheral Neuropathy Among People with Type 2 Diabetes—A Study from South India by Vijay Viswanathan, Balkhiwala Ahmed Khan, Sukanya Nachimuthu and Satyavani Kumpatla in The International Journal of Lower Extremity Wounds
Footnotes
Acknowledgements
We acknowledge Dr Eva Feldman, Dr Brian Callaghan, and Dr Evan Reynolds of University of Michigan who provided the required training to administer the MNSI tool for our study participants. We also thank our study participants who extended their support and co-operation for smooth conduct of study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.