
Abstract
According to the World Health Organization (WHO), ∼180,000 casualties are recorded every year due to burns, majorly from low- and middle-income countries that require medical attention. For the last 5 decades, silver sulfadiazine (SSD) 1% cream has been the most widely used topical antimicrobial agent for managing burn wound infections. Although SSD is considered the gold standard therapy in burn wound management, however in the last 10 years, several studies have reported the negative impact of SSD on the wound healing process. The therapeutic potential of SSD is restricted by its poor solubility, and antimicrobial action appears only after the dissociation of SSD into silver ions (Ag+) and sulfadiazine (SD). Pharmaceutical researchers and industries are looking for alternative strategies to overcome the challenges and limitations of the available SSD formulation due to rising costs, extensive time commitment, and the high risk of failure associated with the de novo development of new antimicrobial drugs. Recent advances in drug delivery systems nanotechnology-based strategies have had a colossal impact on them, particularly in burn wound management. Nanoparticulate systems and nanotools could be considered as potential drug delivery approaches for burn management. This contemporary review provides an abridgment of the literature on advanced SSD nanotherapeutics and their importance in managing burns.
Highlights
According to the WHO, about 180,000 casualties have been recorded every year due to burns.
SSD is the gold standard for treating burn wound infections.
Solubility issues limit SSD's therapeutic potential, as antibacterial effect begins only after dissociation into silver ions and sulfadiazine.
The high risk of failure is associated with the process of de novo development of new antimicrobial drugs.
Novel nanoformulation strategies offer an easy perspective for improving the therapeutic efficiency of the existing drug molecules.
Introduction
A burn is an injury that may affect the skin or other organic tissues predominantly by heat or by radiation, friction, electricity, chemical contact, etc 1 Burn lesion is a potentially traumatic state that damages the skin's outer protective barrier, allowing pathogenic microorganisms such as Escherichia coli (E. coli), Staphylococcus aureus (S. aureus) and Pseudomonas aeruginosa (P. aeruginosa) to enter.1,2 A series of circumstances, including a hypovolemic state, immunological and inflammatory responses, and metabolic alterations, are associated with burn injuries and leads to sepsis. To prevent and treat sepsis and septic shock, precise diagnostic criteria and prognostic indicators are therefore crucial. For burns that cover more than 20% of the total body surface area, sepsis can occur in burn patients at a rate of between 3% and 30% (TBSA). In fact, sepsis can occur in burn patients with burns that cover >20% of their entire body surface area, with a range of 3%–30%. 3 According to the World Health Organization (WHO), ∼180,000 casualties are recorded every year so far due to injuries related to burns, majorly in countries with low and middle-income. 4 Infection/sepsis, however, is responsible for 42% to 65% of all fatalities in burn patients. 3
Yoshino et al 5 have developed a guideline that helps clinicians with proper diagnosis and preliminary treatment of patients with burn injuries. Depending on the type of burn wound, the management of burn wound infection/sepsis entails a combination of wound cleansing, debridement, early burn excision and grafting, topical or systemic antimicrobial medication, etc According to a review of the available literature, silver sulfadiazine (SSD) is the most widely used topical silver-based prophylactic agent in burn wound patients. It was discovered by Charles Fox in the 1960s. It is a United States Food and Drug Administration (US-FDA) approved drug and is included in the list of WHO-approved essential medicines. It has been considered a gold-standard therapy and has been shown to be effective in managing burn wound infections. 6 The data, however, is insufficient to establish its therapeutic importance in burn wound healing. The literature review uncovers conflicting data on whether SSD encourages or discourages wound healing. Despite this proof, SSD is still considered a standard cure for burn management. SSD is a crystalline metallic salt of sulfonamide SD and is soluble in liquid ammonia (30%). It shows polymer-like characteristics, in which the Ag+ ion is tetracoordinated and encircled by 3 dissimilar deprotonated SD molecules, albeit each SD molecule is embedded with 3 unalike Ag+ ions. The polymeric make-up of SSD is also accountable for its poor solubility, therefore, exerting minimal therapeutic potential against pathogenic microbes.7,8 For the last 5 decades, it has been in clinical practice for the management of wound infections. However, in the last 10 years, several studies have reported the negative potential of SSD, such as retarded wound healing, slow and unaccomplished epithelialization, formation of black scars, silver toxicity, bluish-gray skin discoloration (argyria), insubstantial penetration, hypersensitivity, neutropenia, thrombocytopenia, some microbes (e.g., P. aeruginosa) showing resistance, etc Probably due to such adverse effects, it downgrades the positive potential of SSD.9-13
Several literature reports have deduced that the healing of second-degree burn wounds is impeded by existing delivery strategies and formulation of SSD, thus suggesting the necessity for improvement in available marketed preparations. Some studies have also demonstrated that SSD has deleterious effects on fibroblasts and keratinocytes, which may delay the wound-healing process. Therefore, an alternate delivery strategy is necessary to regulate the release of SSD and improve the wound-healing process. Formulation researchers work to overcome the challenges associated with SSD delivery and improve its therapeutic potential by employing novel nanomedicine approaches. Recent advancement in drug delivery systems nanotechnology-based strategies have had an immense impact, particularly in burn wound management. Nanoparticulate system and nanotool could be efficient drug delivery approaches for burn management. This contemporary review provides an abridgment of the literature on advanced SSD nanotherapeutics and their importance in managing burns. 14
Antimicrobial spectrum and Mechanism of Action
SSD is available in the market as a 1%w/w cream/ointment/powder/gel (Silvadene®, Thermazene®, Flamazine®, and others) for the treatment of second or third degree burn wound infections. It exhibits excellent therapeutic potential against a variety of pathogens (gram negative and positive bacteria and yeasts), due to the numerous cellular target sites of silver illustrated in Figure 1. Of note, it has activity against P. aeruginosa, responsible for burn wound infection.3,15 Microbes that are at risk to topical SSD include S. aureus, Staphylococcus epidermidis (S. epidermidis), β-hemolytic streptococci (S. pyogenes or S. agalactiae), Klebsiella pneumoniae, E. coli, Enterobacter (including E. cloacae), Citrobacter, Proteus, Morganella morganii (M. morganii), P. aeruginosa, Providencia, Serratia, and Candida albicans (C. albicans). 16
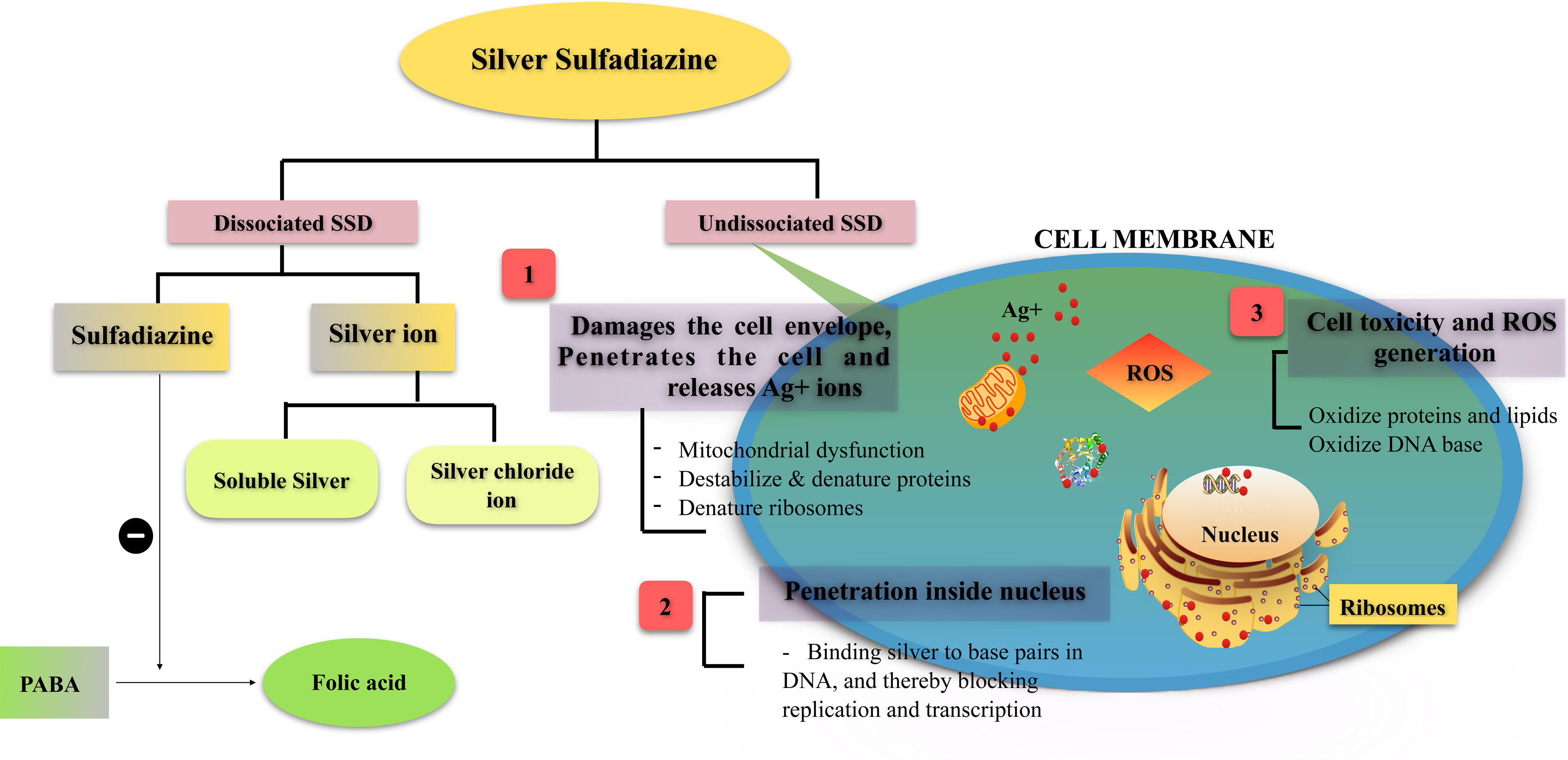
An illustration of probable silver sulfadiazine mechanism of action.
The accurate mechanism of action of SSD is uncertain and not clearly spelled out still to date, and whether the broad-spectrum antimicrobial potential is due to either the silver or the SD moieties, or both acts synergistically. However, in Figure 1, a probable mechanism of action has been illustrated. As the literature review suggested, the mechanism of action of SSD presume dual pharmacodynamic function by both SD and silver. The SD moiety hinders bacterial metabolic function while silver ions get in contact with the microbial DNA and contribute largely to the bactericidal action. Therefore, SSD accomplishes antibacterial action by binding to the base pairs in the DNA helix and thereby interrupting the transcription mechanism.14-22
In particular, after the application of SSD in second/third degree burns, it gets in contact with body fluids and changed into sulfhydryl groups and proteins to free SD, which can be systemically absorbed. Undissociated SSD disrupts the microbial cell envelope and infiltrates the cell, thus releasing Ag+ ions intracellularly. SD restricts the synthesis of folic acid from P-amino-benzoic acid (PABA) and hinders the growth of bacteria by analogs of crucial metabolites. Moreover, the Ag+ ion is a highly reactive moiety and avidly binds to negatively charged proteins, RNA, DNA, and chloride ions. This quality is considered the main attribute of its antibacterial potential, but it also affects its delivery to the wound bed due to its affinity for proteins in the complex wound environs. Besides that, SD did not exhibit antibacterial potential in low concentrations but showed specific synergism together with subinhibitory levels of SSD. In burn wound management, SSD likely performs its therapeutic action by the release of a low concentration of Ag+ (≈1-2 ppm) in a controlled manner into the wound region, and this interferes with, or modulates, several cellular processes. There are numerous deleterious effects on microbes rather than only specific inhibitory mechanisms.16,18,21-26
Moreover, it is interesting to ponder how the wound exudates’ anionic content (Cl−) affects silver solubility, and obtainable ions might exert a bactericidal action. Serum and wound exudate contain chloride (Cl−) ions that influence the accessibility of silver ions in the solution. As in the wound exudates, a low concentration of Cl−(∼100 mM) present, soluble Ag+ will bind to the bacterial cell membrane, interrupting the respiration mechanism.27,28
The potential of highly diluted heavy metals like silver to restrict microbial contamination was referred to as “oligodynamic” coined by von Nägeli in the year 1893. The oligodynamic effect is a biocidal effect of heavy metals and has often been applied to silver. In 1968, Charles Fox reported that sustained release of SSD in the wound fluids containing Cl− and thiol groups leads to the solubilization of SD, thus improving the biocidal effect of Ag+ with the additional antibacterial action of the released SD. Silver-based formulations are considered to interact with a microbial sulfhydryl group, RCOO−, PO3−, amines, hydroxyls, imidazoles, and indoles, either alone or in a different combination.16,29 Trevors discussed the probable mechanism of silver at the cellular level in the microbes, including the following.
30
The binding of Ag+ to base pairs in DNA and thereby interrupt or terminate the transcription mechanism. Binding to microbial cell membrane components interferes with the respiration mechanism and interrupts ATP (adenosine triphosphate) synthesis, and. Preventing phosphate uptake and triggering the release of components like glutamine, proline, succinate, and phosphate from E. coli.
In addition, 2 studies have been conducted on staphylococci and appraised the actions of sublethal concentrations of SSD, and found that sublethal concentrations of SSD were adept to trigger the release of proteases, coagulase, and enterotoxin A and C. These investigations endowed with further evidence that inapt concentrations of SSD may increase the virulence of wound pathogens.31,32
Cytotoxicity and Limitation of Silver Sulfadiazine in Clinical Practice
Generally, in the burn patient, toxicities such as allergy, hemolysis in glucose-6-phosphate dehydrogenase deficiency, development of immune complexes, and methemoglobinemia have been reported upon SSD therapy due to the sulfonamide moiety (sulfadiazine). 11 The systemic toxicity of sulfonamide is determined based on individual chemistry and metabolism. Hematologic problems are the most common concern, such as granulocytopenia, aplastic anemia, hemolytic anemia, and leukopenia. Cutaneous drug reactions, including erythema multiforme, pruritus, skin rash and discoloration, Stevens-Johnson syndrome, and photosensitivity, have all been observed.3,33 Undoubtedly, neutropenia has been reported with SSD treatment in burn patients, but this cannot be completely ascribed to the SD. It would seem to be the case that systemic or local toxicity from SD, as released from emulsion-based topical formulation applied according to the manufacturer's directions, is most unlikely. However, in a clinical study on patients with severe burns who were treated with an emulsion-based topical formulation, the formulation excipients propylene glycol and palmityl alcohol showed quantifiable toxicity, such as allergic contact reactions. Similar reactions to the SD have been documented, while Degreef and Dooms-Goossens (1985) state that there is no clinical testimony that SSD is contraindicated in a patient who previously allergic to sulfonamide. Although most such reactions are to pharmaceutical excipients with SSD, allergic contact dermatitis to silver as SSD and as the nitrate has been documented.34-38 Besides that, cytotoxicity in vitro has been explained and hypothesized as a basis for delayed wound healing as revealed anecdotally. 39 Silver levels in the blood have been found to upsurge after topical SSD therapy. 40 Upon dissociation, the SD is eliminated from the body in shorter order than silver. 41 When using SSD cream (1%) for leg ulcers and acute burns for a long time, a high silver level in the blood (above 20 mg/L) has been linked to renal impairment, hepatic and nerve toxicity, and neonatal granulocytopenia.40-43
Furthermore, the silver in SSD topical cream may cause argyria if used for an extended period of time.44,45 Stumbling blocks of currently available SSD formulations include the necessity for recurrent dressing changes because of short-acting, pain in the course of dressing, local maceration, keratinocyte as well as fibroblast toxicity, and microbial resistance.46-51 Moreover, impaired wound healing is considered a clinical manifestation of mild toxicity, as substantiated by in vitro studies on various skin cell lines.40,52
In a study, Rosen et al 53 have reported a mechanism by which SSD retards the wound healing process and suggest that SSD changes the expression of interleukin-1 (IL-1) family genes, which in turn impairs downstream cytokine production and delays wound healing. SSD applied topically to the burn-inflicted area shows a significant delay in wound closure compared to controls (Figure 2a). By day 10, the SSD-treated group exhibited 16.3% wound closure compared with 42.1% closure in controls (P < 0.005; Figure 2b). By day 15, wounds treated with SSD had developed a persistent crust atop an incompletely re-epithelialized epidermis (Figure 2c). According to immunohistochemistry, increased and persistent inflammatory granulation tissue was seen in the wounds of SSD-treated patients contrast to controls throughout time, with a more significant number of neutrophils and fewer macrophages infiltration as determined by myeloperoxidase (MPO) and ionized calcium-binding adapter molecule-1 (IBA-1) staining, respectively (Figure 3a). On day 3, cytokine investigation revealed the lack of various pro-inflammatory factors previously seen in untreated tissue, including macrophage inflammatory protein (MIP)-1a, monocyte chemotactic protein, and interleukin-1 receptor antagonist (IL-1ra) (Figure 3b). SSD-treated wounds had considerably lower IL-1a and macrophage inflammatory protein (MIP)-2 expression levels than controls. Such evidence supports a causal link between SSD and impaired wound healing, but more investigation is necessary.

SSD impairs wound closure. (a) Wounds of BALB/c mice untreated (upper panel) or treated with SSD (SSD; lower panel) on days 0, 7, and 13. Bar¼5 mm. These experiments were performed in triplicate. (b) Wound size analysis of BALB/c mice skin lesions. Time points represent the mean of the findings for 56 and 46 treatment measures for untreated controls and SSD, respectively, and error bars indicate SEMs. *P < .05 in comparing the SSD-treated with SSD-untreated groups. (c) Histological examination of SSD-untreated and SSD-treated BALB/c mice at days 7 and 15. Hematoxylin and eosin staining. Scale bars left to right: 1000, 100 mm. Blue staining showed collagen utilizing Trichome. Scale bar¼100 mm. 53 Abbreviations: SSD, silver sulfadiazine; SEM: scanning electron microscopy.
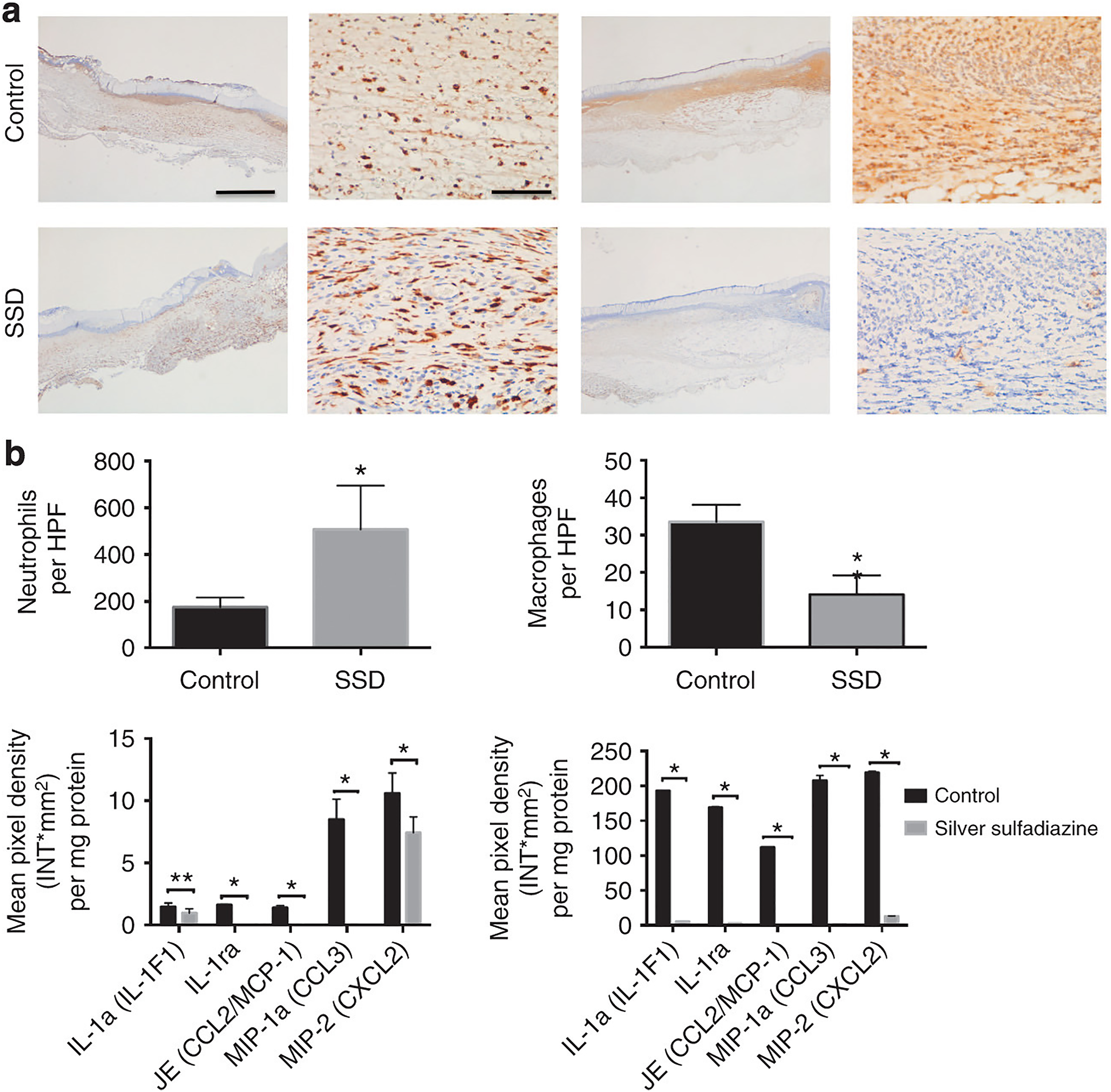
The immune milieu in burn wounds is altered by silver sulfadiazine (SSD). (a) Histological examination of untreated and SSD-treated wounded BALB/c mice at day 7. Representative MPO (left) and IBA-1 (right) immunostained slices of the burn lesions are shown. The brown staining suggests cellular infiltration into the wound bed. Scale bars¼1000 and 100 mm(left to right). (b) First row: Number of neutrophils and macrophages per field in wounded skin tissue of untreated and SSD mice. The data are presented as the mean number of neutrophils and macrophages in 15 distinct fields for 20 separate wounds, and error bars denote SEMs. *P < .0001 in comparing the SSD-treated group with the untreated groups. Second row: Quantification of signals from wounds (n¼10 per group) on days 3 and 7. The blots were scanned and signal intensity was measured. IL-1a, IL-1ra, MIP-1a, and MIP-2. (Notably, as antibodies specific for each individual cytokine are used in this cytokine array, absolute levels for different cytokines cannot be compared.) Error bars represent SEMs. *P < .0001 in comparing the SSD-treated group with the untreated groups. 53 . Abbreviations: SSD, silver sulfadiazine; MPO, myeloperoxidase; SEM, scanning electron microscopy; MIP, macrophage inflammatory protein; IBA-1, ionized calcium-binding adapter molecule-1; IL-1, interleukin 1; IL-1ra, interleukin-1 receptor antagonist.
The onset of microbial resistance, confirmed delayed wound healing, and the development of systemic problems are all undesirable characteristics linked to the therapeutic use of SSD, necessitating the use of advanced burn therapy and dressings.54-57 The cytotoxicity associated with the prolonged use of SSD can be kept down by optimizing its formulation technique and delivery strategy. 58 Despite the lack of convincing evidence for SSD cytotoxicity in other in vivo studies, 59 and even though the data on SSD cytotoxicity is unclear after decades of usage in clinical practice, SSD remains the conventional topical therapy for burns.57,58
Silver Sulfadiazine Loaded Nanoparticulate Fabrication for Burn Wound
The pharmaceutical industry is looking for alternative strategies to overcome the challenges and limitations associated with the available drugs/therapy due to rising costs, extensive time commitment, and the high risk of failure related to the process of de novo development of novel antimicrobial drugs. Enhancing the safety and efficiency of existing drug molecules is relatively easy and less time-consuming than developing new therapeutic molecules. Novel nanoformulation strategies offer an easy perspective for improving the therapeutic efficiency of the existing drug molecules.
SSD, in particular, has gained widespread recognition and is widely regarded as the gold standard treatment for burn wound infections. Following the FDA's approval, various pharmaceutical companies across the world began marketing SSD-based topical formulations like SilvadeneTM and FlamazineTM. An animal study provided the first proof that SilvadeneTM (1% micronized SSD) had a positive effect on wound healing in addition to its antibacterial action. The administration of SSD topically to clean wounds in pigs boosted epithelialization rates by 28%. 60 SSD, also known as FlamazineTM 1% cream (Smith & Nephew), has been a mainstay of topical burn wound therapy 61 and has been used successfully to manage microbial infection in acute 62 and chronic 63 wounds. Numerous novel silver-based topical formulations have been tested in clinical trials on chronic wounds,64,65 with generally positive results. Clinical evidence on SSD preparation is largely in the area of burns wound management,55,66-68 although there are studies on clinical application in chronic leg ulcers,63,69 and acute wounds. 62
Despite the proven record of currently available SSD-marketed preparations in clinical practice, it is now in a dilemmatic state. Because such preparations were developed empirically with insufficient knowledge of the role of carrier systems in delivering the drug molecule at the desired rate, concentration, and site of action. Since then, the medication has been associated with a slew of pharmaceutical and clinical issues. The quick release of medication at the wound site, which necessitates multiple applications per day, leads to poor patient compliance. Besides that, SSD itself faces solubility challenges, because it is only soluble in 30% ammonia.7,8 Several recent literature reports have concluded that the obstacles associated with existing SSD formulation have a negative impact on therapeutic outcomes and patient health. Scientists are attempting to employ a novel formulation strategy and repackage an old drug (SSD) in a new bottle. Table 1 summarizes the impact of the nanoformulation approach on SSD pharmaceutical and clinical outcomes.
SSD Loaded Nanoparticulate Fabrication for Burn Wound Management.
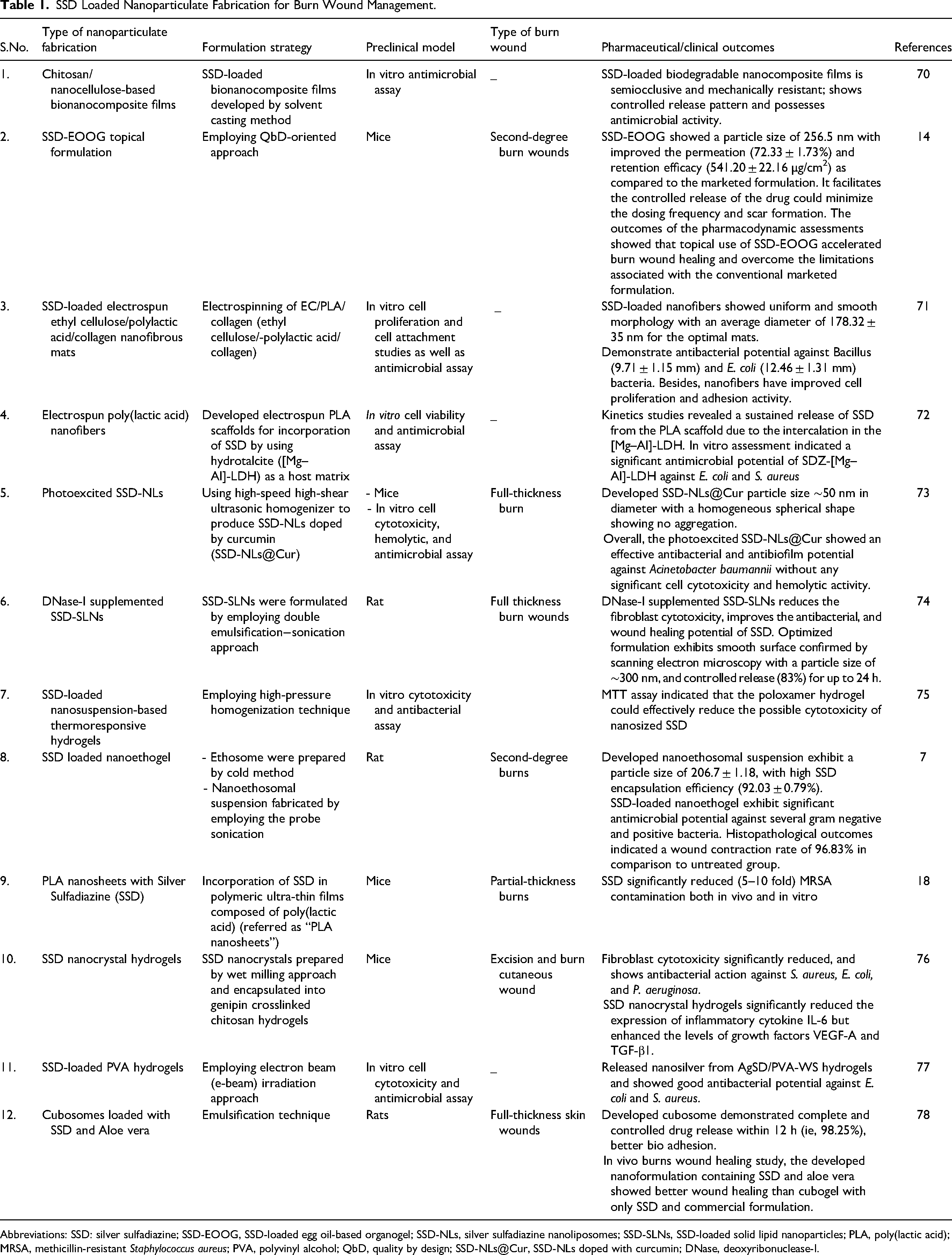
Abbreviations: SSD: silver sulfadiazine; SSD-EOOG, SSD-loaded egg oil-based organogel; SSD-NLs, silver sulfadiazine nanoliposomes; SSD-SLNs, SSD-loaded solid lipid nanoparticles; PLA, poly(lactic acid); MRSA, methicillin-resistant Staphylococcus aureus; PVA, polyvinyl alcohol; QbD, quality by design; SSD-NLs@Cur, SSD-NLs doped with curcumin; DNase, deoxyribonuclease-I.
Several studies have been undertaken by several researchers to investigate the SSD-loaded nanoformulation and nano-assembly potential in the management of burns and burn wound infections, which is briefly explained below.
Singh et al 79 have developed polycaprolactone (PCL)-PEO(shell)/PEO-SSD(core) nanofibers by employing a novel co-axial airbrushing approach. The outcomes of the study indicate that the SSD-loaded core-shell nanofibers deposited directly on to the burn wound and releases the drug in a controlled manner and showed concentration-dependent antibacterial potential against E. coli. Developed SSD nanofiber mats show excellent cellular compatibility and favor the growth of stem cells as well as fibroblast cells. In addition, the gene expression assessment reveals their skin regeneration potential by upregulating extracellular matrix proteins (Col I, Col III, and elastin).
Fatima et al 80 have designed and formulated SSD-loaded nanoemulsion-based cosmetotherapeutic lotion by using ultrasonication method. The optimized nanoformulation shows particle in nano size range (213 nm) with good encapsulation efficiency (≈80%). In this formulation, argan oil was used as a cosmetotherapeutic agent to enhance the permeation of drug. The SSD loaded nanolotion exhibited better antimicrobial potentials against variety of bacterial (E. coli, K. pneumoniae, and S. aureus) and fungal (C. albicans) strains due to the particularly large surface area of the nanocarriers in contrast to marketed formulations.
In a study, Nejaddehbashi et al 81 fabricated an electrospun membrane of PCL nanofibrous mat containing 0.3% weight SSD with a thickness of 500 µm. The release profile shows an almost immediate release of the drug (up to 60%) in 4 days, followed by a 20-day steady release of 80% of the drug. PCL can control the release profile of SSDs. The PCL/SSD nanofibrous membrane with a thickness of 500 µm and a concentration of 0.3% (w/v) SSD performed well as a wound dressing and accelerated wound healing in vivo.
Thakur et al 14 have formulated SSD-loaded egg oil-based organogel (SSD-EOOG) preparation using a quality by design oriented approach and have further evaluated it for in vivo efficacy in a rat model and stability. They have reported enhanced permeation (72.33 ± 1.73%), retention efficacy (541.20 ± 22.16 µg/cm2), wound contraction rate (78.23 ± 5.65%) and faster re-epithelialization in the SSD-EOOG-treated group. The study's findings concluded that egg oil-based organogels can revive the therapeutic value of SSD for burn wound treatment.
In a separate investigation, Pourhajibagher et al 73 investigated the antibacterial activities of photoexcited SSD nanoliposomes (SSD-NLs) doped with curcumin (SSD-NLs@Cur) on Acinetobacter baumannii (A. baumannii). The results of the investigation demonstrate that no substantial cytotoxic or hemolytic effects were noticed. The A. baumannii count in planktonic and biofilm forms, as well as gene expression levels, decreased (P < 0.05) when SSD-NLs@Cur-aPDT was used. After antimicrobial photodynamic therapy, the epidermis regenerated considerably, and the bacterial load dropped significantly, according to histopathological analyses.
In a study, Patel et al 74 formulated a deoxyribonuclease-I (DNase-I) supplemented SSD-loaded solid lipid nanoparticles (SSD-SLNs) to minimize fibroblast cytotoxicity and overcome biofilm-induced resistance. In comparison to SSD with DNase-I (82.9%), the newly developed SSD-SLNs SLNs in combination with DNase-I suppressed ∼96.8% of P. aeruginosa biofilm. SSD-SLNs were shown to be less toxic (cell viability 90.3 ± 3.8% at 100 g/mL) than SSD (cell viability 76.9 ± 4.2%) against a human dermal fibroblast cell line. Finally, after 21 days of therapy with SSD-SLNs and DNase-I, the in vivo wound healing investigation revealed complete wound healing, whereas marketed SSD formulations exhibited incomplete wound healing after 21 days. According to the findings, combining SSD-SLNs with DNase-I is an effective therapeutic strategy for biofilm-associated wound infections that also speeds wound healing. Furthermore, Taglietti et al 82 have developed an innovative nano-assembly by using a “layer-by-layer” approach to fabricate a high microbicidal self-assembled nano-monolayer of SSD on hydroxylated material surfaces, utilizing the reaction between a monolayer of thiolic functions on glass/quartz surfaces and a newly synthesized derivative of the well-known topical antimicrobial agent SSD. In vitro, the surface-functionalized materials were effective against both S. aureus and E. coli.
Venkataraman and Nagarsenker used a microprecipitation–high-pressure homogenization process to develop SSD nanosuspension-based nanogel for the treatment of burn wounds. In vivo investigations showed that 0.5% SSD nanogel was more effective than 1% commercial cream in wound healing. Furthermore, in 2017, Barkat et al, 8 formulated and characterized the nanosuspension-based SSD nanogel containing aloe gel for the management of second-degree burns and burn wound healing using an animal model (Albino Wistar rats). They have adopted a novel formulation strategy, controlled nanoprecipitation, to produce SSD nanosuspension to overcome the solubility challenges associated with the SSD. The SSD nanogel treated group showed better healing in comparison to the group treated with SSD-marketed formulation. In a similar study, Liu et al 75 have formulated stable SSD nanosuspensions (SSD-NSs) with improved SSD solubility, as well as a suitable carrier (thermoresponsive hydrogel) for SSD-NS delivery. The use of SSD nanosuspensions in combination with a thermoresponsive hydrogel increased SSD antibacterial activity while lowering cytotoxicity.
In a study, Razavi et al, 7 developed a nano-ethosomal formulation containing SSD that was used to minimize bacterial burden and healing time in burn injuries. Antimicrobial tests revealed that the SSD-loaded ethosome formulation reduced colony numbers significantly. The SSD ethosomal gel-treated animal had a wound contraction rate of 96.83%, while the untreated animal had a rate of 59.41%, according to histopathological examination. The study's findings suggested that SSD ethogels could improve SSD's healing ability when used to treat burn wounds.
In addition, SSD-loaded chitosan nanoparticles embedded in wound dress padded with glutaraldehyde were designed and evaluated by El-Feky et al 83 . They claim that the newly developed dressing facilitates the SSD release in a controlled fashion in the burn wound environment to manage wound sepsis and infection. Efficient management was achieved due to the prolonged, uninterrupted contact time between the drug and the burn wound.
Gao et al 76 developed and tested genipin-crosslinked chitosan hydrogels as a possible delivery carrier for SSD nanocrystals. In the hydrogel network, SSD nanocrystals were distributed uniformly and had excellent physical stability. SSD nanocrystals from hydrogels exhibited a swelling-dependent release pattern, which was well fit by the Peppas equation. The fibroblast cytotoxicity of SSD nanocrystals encapsulated in hydrogels was significantly reduced, but their antibacterial activities against S. aureus, E. coli, and P. aeruginosa were still equivalent to unencapsulated SSD nanocrystals. SSD nanocrystal hydrogels substantially reduced the expression of the inflammatory cytokine IL-6 while significantly increasing the levels of the growth factors VEGF-A and TGF-1 in excision and burn cutaneous wound models in mice. In comparison to the marketed SSD cream formulation, hydrogels containing SSD bulk powders, and blank hydrogels, wounds treated with SSD nanocrystals demonstrated the best healing state histopathologically. In another investigation, bacterial cellulose (BC) dressing for burn wound healing that contained homogenous SSD nanoparticles was fabricated and assessed by Wen et al 84 . BC-SSD demonstrated high antibacterial efficacy against S. aureus, P. aeruginosa, and E. coli in vitro. The burn wounds of rats treated with BC-SSD demonstrated better wound contraction than the control group. Epithelialization proceeded faster in wounds treated with BC-SSD, according to histological examination.
Moreover, Sandri et al 85 developed SSD nanocomposites based on montmorillonite-chitosan (MT/CS) for topical therapy of chronic skin lesions. By lowering the cytotoxicity of SSD while keeping its antibacterial capabilities, the loading of SSD in MT/CS nanocomposites aimed to overcome the wound healing delayed action. SSD loaded in the 100 MT/CS nanocomposite has good in vitro biocompatibility, gap closure properties (fibroblasts), and antibacterial properties, particularly against P. aeruginosa, which frequently complicates skin diseases. Sandri et al 86 have also developed an enhanced wound dressing for tissue restoration based on SSD solid lipid nanoparticles (SLN), which they used in conjunction with platelet lysate (PL) to treat skin diseases. SSD was encapsulated in SLN, which inhibited the drug's cytotoxic action on normal human dermal fibroblasts in vitro, as well as its association with PL. Dressings based on chitosan glutamate show antibacterial activity both with and without PL, suggesting that they are an appropriate prototype for treating skin lesions.
Dharashivkar et al 87 used a thin-film hydration approach to formulate an improved niosomally encapsulated SSD gel for the management of burns. Even when administered at half the concentration (0.5%) of the marketed formulation, the in vitro antibacterial potential of niosomally encapsulated SSD gel was as good as that of marketed cream (1%) against S. aureus. Even when applied once a day, an in-vivo investigation revealed that developed niosomal gel containing 0.5% w/w SSD was more effective in burn wound healing than a 1% w/w commercial formulation.
In a study, Morsi et al 88 have developed SSD-loaded cubosomes based gel, a novel nanoparticulate system for burn wound management. Silver toxicity is minimized by facilitating the controlled release of SSD and by reducing the dose of SSD, which leads to better patient compliance and avoids repeated application. The outcomes of the in vivo histopathological assessment showed the prepared cubogel formulation is successful in the management of deep partial-thickness burns with excellent healing potential and the least side effects in comparison with the commercially available product (Dermazin®).
Based on the aforementioned literature, the formulation researchers designed and fabricated several SSD containing nanoformulation, however, their clinical usefulness is still uncertain and needs further optimized work.
Silver Sulfadiazine Market Outlook
As per the WHO, around 180,000 fatalities occur due to burns every year, most of them being in developing countries. Globally increasing burn injury incidences, as well as increased adoption in developing countries, are expected to drive the global SSD market reach. For the most part, Asia Pacific is yet to be explored. However, new competitors in the wound care industry such as China, India, Australia, and Japan are projected to emerge in the near future and provide new income streams. Because of its documented adverse effects, SSD is losing its position as the industry's most important product. As a result, the worldwide SSD market is stalling. Moreover, rising prices of silver, which are among the main raw materials used in SSD production, are expected to impede the growth of the global SSD market. Major players functioning in the global SSD market are 3M Company, Monarch Pharmaceuticals, Baxter International, Inc., Johnson & Johnson Limited, and Teva Pharmaceutical Industries Ld
Conclusion
Despite varied market opinions, SSD remains one of the most popular drugs for managing burns and burn wounds. Since its first launch as a cream formulation for topical application some forty years ago, SSD has been considered the gold standard treatment for burns and burn wound infection. Its widespread clinical application has been proven to be considered safe with relatively low resistance potential. Despite the proven record of currently available SSD-marketed preparations in clinical practice, they are now in a dilemmatic state. Because such preparations have been formulated empirically with little understanding of the relevance of carrier systems in delivering the drug molecule. Besides that, the drug itself has been associated with several clinical and pharmaceutical challenges, such as poor solubility and permeation through the skin, silver toxicity, wound healing retardant action, etc The advent of new-generation formulation development technology such as novel nanostructured drug carrier systems and nanofabrication could revive its importance and clinical utility as standard burn wound therapy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed no financial support for the research, authorship, and/or publication of this article.