
Abstract
A systematic review of the effectiveness of off-loading in the diabetic foot was done. Searches were conducted in October 2022 using the PubMed and Scielo databases. Randomized clinical trials or controlled clinical trials were included. Two authors performed the study selection and data extraction, and any discrepancies between the 2 reviewers were resolved through discussion with a third reviewer. Fourteen papers met the selection criteria with 822 patients included, but the sample sizes in all studies were small. Most of the published studies were done in European countries. Total contact cast was the most effective off-loading. The present review studies the effectiveness of off-loading systems in patients with diabetic foot ulcer, as well as different off-loading methods, with total contact cast proving to be the gold standard, despite its adverse effects.
Introduction
According to the World Health Organization, diabetes mellitus (DM) is a chronic disease that occurs when the pancreas does not secrete enough insulin or when the body does not effectively use the insulin it produces. 1
One of the complications of DM is Diabetic Foot Syndrome. Diabetic Foot Syndrome is defined as ulceration, infection, and deep tissue destruction associated with diabetic neuropathy and peripheral arterial disease (PAD) in the lower extremities. 2
Diabetic foot ulcer (DFU) is a complication with high incidence. These ulcers are associated with severe morbidity and a great reduction in patients’ quality of life. It is very common to find osteomyelitis in these lesions, an infection of the bone that requires early treatment to avoid its spread and negative consequences.3,4
The prevalence of foot ulcers in the DM population is 4% to 10%. The lifetime risk of developing this complication is estimated to be 15%. The risk of foot ulceration and lower limb amputation increases with the patient's age and duration of DM. 4 The many risk factors and interactions between other conditions such as obesity, psychosocial factors, activity, and treatment compliance make it very difficult to control and assess the situation, thus, making it hard to reproduce the different kinds of therapies and results shown in the literature. 5 The failure to decrease the number of amputations may be partially attributed to poor understanding of direct wound care, off-loading, and choice of the appropriate treatment modality. 6
The mainstays of current DFU management include local wound care through debridement, dressings, off-loading, vascular assessment, treatment of active infection, and glycemic control. 7
For good and rapid healing of DFU, the absence or relief of pressure is vital. For this reason, different types of off-loading systems depend on the case to be treated. Some off-loading devices are postsurgical shoes with rigid soles, boots, orthopedic walkers, and felts. The total contact cast (TCC) is considered the gold standard device, although it is not indicated in patients with PAD or infection.7,8 The authors consider that off-loading methods promote the healing of DFU. It should be emphasized that pharmacological treatment alone cannot lead to the successful treatment of DFUs without adequate off-loading. Inadequate off-loading is one of the most frequent reasons for delayed wound healing. 9 Therefore, the main aim of the review is to evaluate the effectiveness of off-loading in patients with active DFU.
Methods
Study Design
A systematic review of the effectiveness of off-loading in DFU was carried out using a checklist of The Preferred Reporting Items for Systematic Reviews and Meta-Analyses. 10
Literature Search
Searches were conducted in October 2022. For this systematic review, several bibliographic searches were carried out in the PubMed and Scielo databases. The following search terms were used in the PubMed database: “Diabetic foot ulcer” and “off-loading.” And another search is carried out in the Scielo database, using “Diabetic foot ulcer” and “off-loading” as search criteria. In both cases, AND was used as the Boolean operator. Vancouver style, citing in order of appearance in the bibliography section.
Article Selection Criteria
Inclusion criteria were as follows: published articles were selected that demonstrated research on diabetic foot off-loading systems regardless of the year of publication, but up to complete healing of the lesion and the effectiveness of different off-loading systems and their types. In addition, the focus was on inclusion in controlled clinical trials and randomized controlled clinical trials. All the studies that have been chosen are conducted in humans with DM. The languages selected for the articles are Spanish and English.
Exclusion criteria were as follows: case reports, meta-analyses, letters, editorials, and articles that did not show interest in off-loadings and their effectiveness were excluded. References from systematic reviews and meta-analyses were also examined to identify additional articles. In addition, articles dealing with off-loading through surgeries were excluded.
The search and selection of articles were performed by 2 independent raters (SV-R-R and AT-G). Any discrepancies between the raters were resolved through discussion with a third reviewer (JLL-M).
Results
Search Results
In the initial search, with the search descriptors and the Boolean operator AND, 658 articles were acquired, of which, after applying the inclusion and exclusion criteria, 564 articles were discarded, leaving 94 records to examine. After an assessment of the title and abstract, 76 articles were excluded, leaving 18 full-text articles assessed for eligibility. Four full-text articles were excluded due to protocol criteria or insufficient data. Ultimately, 14 articles were used to produce the results of this systematic review (Figure 1).
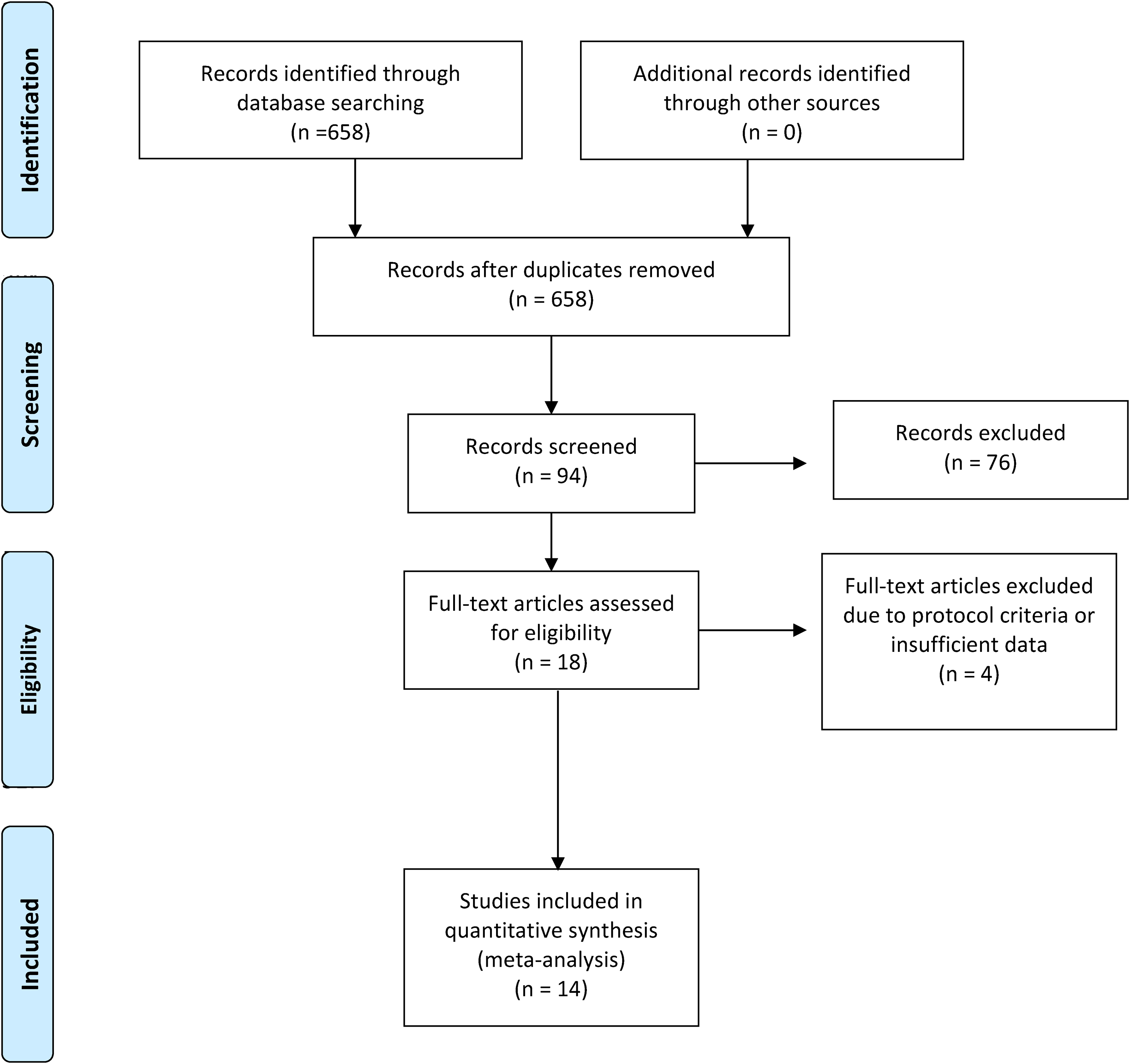
Flowchart of the identified studies.
Characteristics of the Included Studies
The data extracted from the 14 articles in the systematic review are summarized in Table 1. A total of 822 patients were included in the total number of articles.
Summary of Studies Included in the Systematic Review.
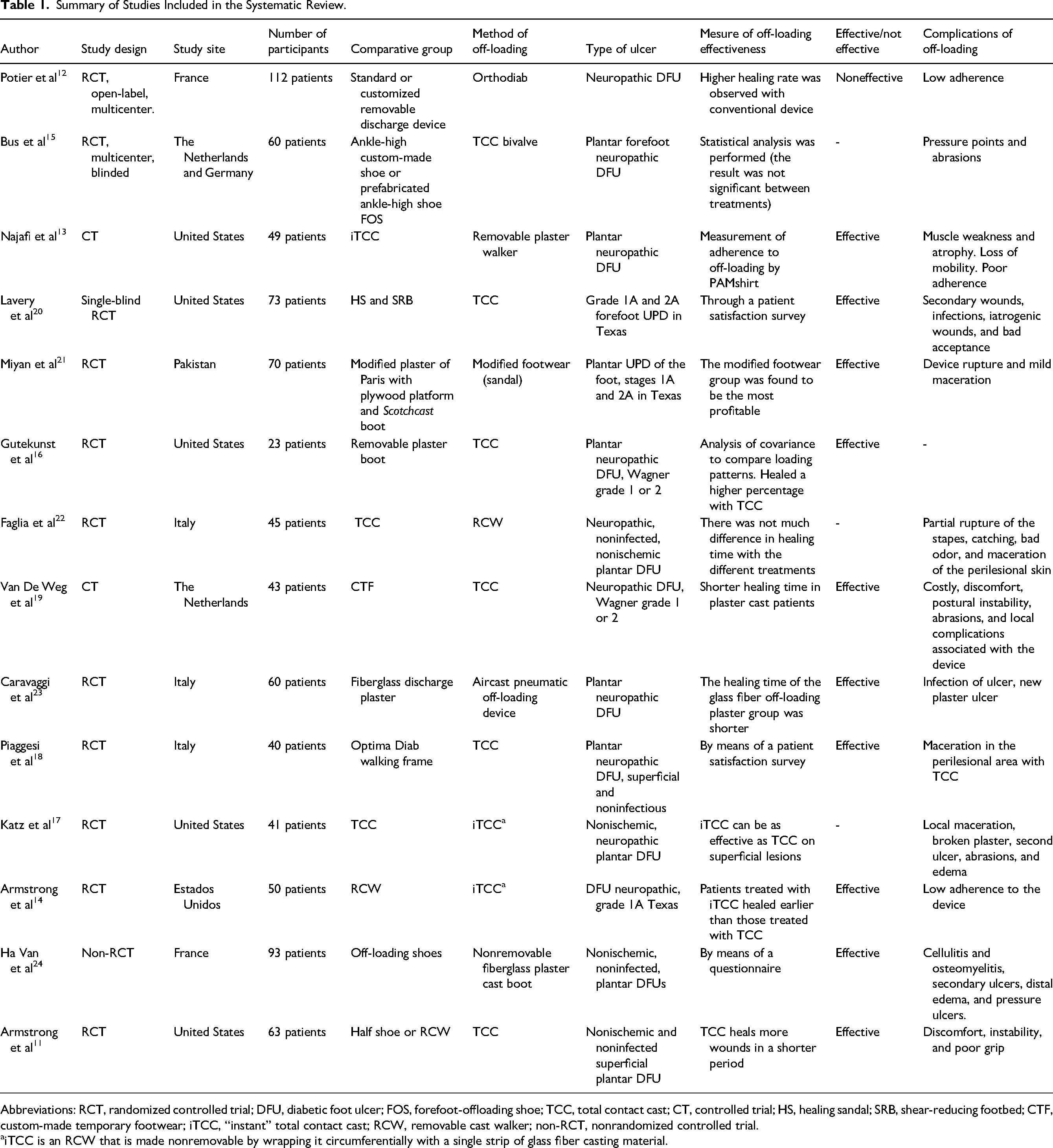
Abbreviations: RCT, randomized controlled trial; DFU, diabetic foot ulcer; FOS, forefoot-offloading shoe; TCC, total contact cast; CT, controlled trial; HS, healing sandal; SRB, shear-reducing footbed; CTF, custom-made temporary footwear; iTCC, “instant” total contact cast; RCW, removable cast walker; non-RCT, nonrandomized controlled trial.
iTCC is an RCW that is made nonremovable by wrapping it circumferentially with a single strip of glass fiber casting material.
Most of the publications have been developed in European countries, but several have been carried out in the United States, one of them in Pakistan. The sample sizes were generally not very large, with only one article exceeding 100 subjects.
The first clinical trial of off-loading devices for the management of UPD was published in 2001 by Armstrong et al. 11 The last published article is from 2 years ago (2020) by Potier et al, 12 which shows that, despite being a fundamental pillar for the management of UPD, it is not a topic of concern among scientific publications, with only 14 RCTs in the last 22 years.
Concerning the off-loading device used in the studies, TCC is the most used. In addition, the most common method used to assess treatment efficacy was healing time, where shorter times are more effective for off-loading. Most of the articles showed off-loading devices that were found to be effective.
Finally, among the complications, we can observe that the most frequent are muscle weakness and atrophy, secondary to immobilization. However, the patient's poor adherence to these devices also stands out.
Discussion
After reviewing 14 articles, we can state that off-loading efficacy is crucial for managing DFU, but the ideal off-loading must be chosen in each case. Najafi et al 13 and Armstrong et al 14 agree that patients are less active when treated with irremovable casts than with removable shoes or casts. Irremovable casts are considered the gold standard off-loading treatment for DFU. 13 Similarly, removable off-loading is the common standard of care for treating DFU. 12 The present study 15 suggests a higher prevalence of healing in patients treated with TCC. This irremovable cast does not indicate ulcers with soft tissue infection or osteomyelitis. 11
In addition, Gutekunst et al 16 also show that to improve healing, it is advisable to use immovable devices such as the TCC or a cast walker boot that has become immovable.
Likewise, Najafi et al 13 and Armstrong et al 14 seem to agree that there are significant differences in activity behavior between patients off-loaded with a removable cast walker (RCW) and those off-loaded with the same device but nonremovable (iTCC), concluding that patients treated with iTCC healed earlier than those treated with RCW.
However, Katz et al 17 suggest that iTCC may be as effective as standard TCC and may also be associated with fewer complications, less time to implement, and therefore, lower cost.
Potier et al 12 studied the Orthèse diabète, a removable off-loading that immobilizes the foot and ankle joints but did not show any superiority over the standard removable off-loading for the healing of neuropathic DFU. Therefore, this method does not seem very effective for this type of ulcer. In addition, more adverse events were detected with this method compared to the conventional approach. However, Piaggesi et al affirm the efficacy and safety of the Optima Diab immovable walker, which is more practical, less expensive, and more accepted by patients than the TCC. 18
Bus et al 15 conducted the first single-blind multicenter RCT to compare 3 removable off-loading devices for the healing of neuropathic DFU; no significant differences in healing efficacy were observed between these 3 devices. Likewise, Van De Weg et al 19 show the first RCT comparing off-loading using a standard TCC with a custom-made shoe.
Similarly, Lavery et al 20 evaluated the efficacy of 3 off-loading techniques for healing DFU: TCC, a healing sandal, and a removable boot with a shear-reducing insole (SRB). The authors concluded that patients treated with TCC had the highest proportion of healed wounds and the fastest healing time. However, the SRB had the lowest healing and the highest attrition rate during the study. A patient satisfaction survey is conducted.
On the other hand, in Pakistan, Miyan et al 21 evaluated the efficacy of locally applied pressure relief techniques on plantar foot ulceration in people with DM. The modified footwear group was the most cost-effective among the 3 techniques. Faglia et al described another type of off-loading called Stabil-D; this walker promotes healing due to its rigid capacity and good pressure distribution. Therefore, it is a good off-loading option for patients who do not tolerate TCC. 22
Caravaggi et al 23 compare an Air cast pneumatic off-loading device and a fiberglass off-loading plaster. It was concluded that the healing time with the fiberglass off-loading plaster is shorter. Ha Van et al also claim that the nonremovable fiberglass plaster boot effectively reduced the risk of osteomyelitis and healing DFU, as it enforced compliance with off-loading. 24
Nowadays, although the use of TCC is considered the gold standard of off-loading for DFUs, it should be noted that the recommendation is aimed at patients with neuropathic ulcers. In contrast, the use of TCC is limited in patients with neuroischemic ulcers and contraindicated in patients with infection and/or critical ischemia. In addition, the presence of ischemia complicates the management of DFUs with no direct benefit being obtained by off-loading, and revascularization being necessary for the correct management of the patient and to obtain ulcer healing. 22
Importance of the Study
In short, based on the scientific evidence found for this review, early treatment of DFU should be considered of great importance. Also, off-loading is vital to reduce the pressure and friction on the ulcer and thus help to heal more quickly. Also, whenever an off-loading is administered, it is advisable to explain to the patient the importance of compliance with the treatment, as well as not walking excessively to avoid complications. Poor adherence to the device, weakness, muscle atrophy, and postural instability is common adverse effects.
Weaknesses and Strengths of the Study
This is the only systematic review of controlled clinical trials addressing the different types of off-loading in DFU. The available evidence is insufficient to decide how to treat an ulcer in a patient with DM, as each patient and each ulcer is different and requires individualized treatment. Therefore, more studies comparing different types of off-loading are needed.
In addition, most studies are not blinded, as there is no possibility of blinding the discharge to the patient and the investigator, which may influence the analysis of efficacy, and there is a risk of bias.
One of the strengths of our study is to compare the different off-loading methods, analyzing their adverse effects, ulcer etiology, and off-loading effectiveness in each study, ultimately identifying the most effective method.
Unanswered Questions and Future Research
There are few studies comparing the methods of off-loading currently in use, and there is a lack of scientific evidence to recommend their use. Therefore, RCTs with a blinded evaluator comparing different off-loading devices for managing DFU are needed to help understand the advantages and disadvantages of different treatments.
Conclusion
Using off-loading devices generally promotes ulcer healing in patients with DM. Here, we compared off-loading methods for active diabetic foot ulceration (TCC, FOS, RCW, HS, and SRB). TCC was identified as the most effective off-loading method despite its adverse effects on ulcers in patients with diabetic foot.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.