
Abstract
An increased extracellular water/intracellular water (ECW/ICW) ratio determined by bioimpedance has been related to mortality in patients undergoing hemodialysis. We aimed to evaluate the impact of body water distribution in patients with diabetes-related foot ulcers. Seventy-six patients were evaluated with bioimpedance, handgrip strength, and laboratory examinations. The ECW/ICW ratio is a prognostic factor for early mortality.
Introduction
Bioimpedance analysis (BIA) is a precise technique to evaluate muscle quantity and body water distribution. Extracellular water is related to fluid overload in both the intravascular and the interstitial spaces, which can be a sign of renal impairment and heart failure. Intracellular water is related to muscle and body cell mass, 1 which is impaired in malnutrition. Recent data have linked the extracellular water to intracellular water (ECW/ICW) ratio to the malnutrition-inflammation-atherosclerosis (MIA) syndrome. 2 An increase in the value of the ECW/ICW ratio has been related to mortality in patients undergoing dialysis.1,3 However, the association of the ECW/ICW ratio with mortality has not been evaluated in other populations. Since inflammation, malnutrition, and vascular complications are present in patients with diabetes and foot ulcers (DFU),4,5 we aimed to investigate the prognostic value of the ECW/ICW ratio in patients with diabetes admitted for DFU.
Material and Methods
Seventy-six patients were prospectively recruited at the Vascular Surgery Department (Juan Ramón Jiménez Hospital, Huelva, Spain) from March 2021 to July 2022. The inclusion criteria were patients with DFU as the main diagnosis at admission. The exclusion criteria were patients younger than 18 years, patients with neurological and/or cognitive disorders that could interfere with the evaluation, patients with active cancer or immunosuppressive treatments, and patients who did not consent to be included in this study. Diabetes-related complications were obtained from clinical records. The peripheral arterial disease was diagnosed by the vascular team treating the patients. An evaluation was performed 24 to 48 h after admission and included tools for controlling nutritional status (CONUT), 6 anthropometric measures, and laboratory tests for inflammatory and nutritional markers. The prognostic nutritional index (PNI) was calculated as follows: (10 × albumin) + (0.05 × lymphocytes count). The glomerular filtration rate (GFR) was calculated with the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) formula. 7 Nephropathy was considered present when the GFR was <60 mL/min/m2, albuminuria was present in 2 urinary samples or the patient was in dialysis. Handgrip strength was determined with the Jamar®Hydraulic hand dynamometer (Sammons Preston; Rolyon). To evaluate body composition, BIA was performed with the validated measuring device BIA-101 Akern Systems®. In order to estimate muscle mass from BIA, we obtained the parameter fat-free mass index (fat-free mass/height2). Early mortality was defined as any death regardless of the cause occurring in the 6 months after admission.
Statistical Analysis
The generalization of the Shapiro–Wilk test for the multivariate variables test was used to study the normal distribution of the samples. Categorical variables are reported as the number and percentage of the sample. Nonparametric Spearman's rho was used to study the linear correlation between the ECW/ICW ratio and other inflammatory and nutritional values. Interpretation of the correlation coefficient was established according to the previously reported conventional approach. 8 Univariate analysis between patients who died and those who survived was conducted. Variables with a p-value <.05 in the univariate analysis were then introduced in a multivariate backward Cox’s regression model. Data were censored to December 15, 2022. Hazard ratios (HRs) with confidence intervals (CIs) were estimated. A p-value <.05 (2-tailed) was set as the threshold of statistical significance. Statistical analysis was performed using jamovi software [The jamovi project (2021). jamovi (Version 1.6) Computer Software. Retrieved from https://www.jamovi.org] for macOS. Cox’s regression model was performed using SPSS version 20 for macOS (SPSS Inc.).
Results
The mean age of the cohort was 70.5 years, and most patients were male (81.6%) with type 2 diabetes (93.4%). Patients mainly had the peripheral arterial disease (92%), and 34.7% had diabetic neuropathy. The most frequent macrovascular complication before admission was myocardial infarction (21.1%), and the most frequent microvascular complication was retinopathy (61.6%); 55.3% of patients had nephropathy and 3.9% were in dialysis. According to the CONUT score, 36.8% were at risk of moderate or severe malnutrition, and 73.7% had altered dynamometry values. During hospitalization, 38.2% of patients suffered a minor amputation, 17.1% a major amputation, and 10.8% reamputation. The mean follow-up was 291 days, in which 25 patients (32.9%) had any readmission for DFU. The mortality rate at 6 months was 21.1% (16 patients). The main etiology of death was cardiac (8 patients), followed by infectious (5 patients) and other causes (3 patients).
Linear correlation analysis of the ECW/ICW ratio is shown in Table 1.
Linear correlation analysis of the ECW/ICW ratio.
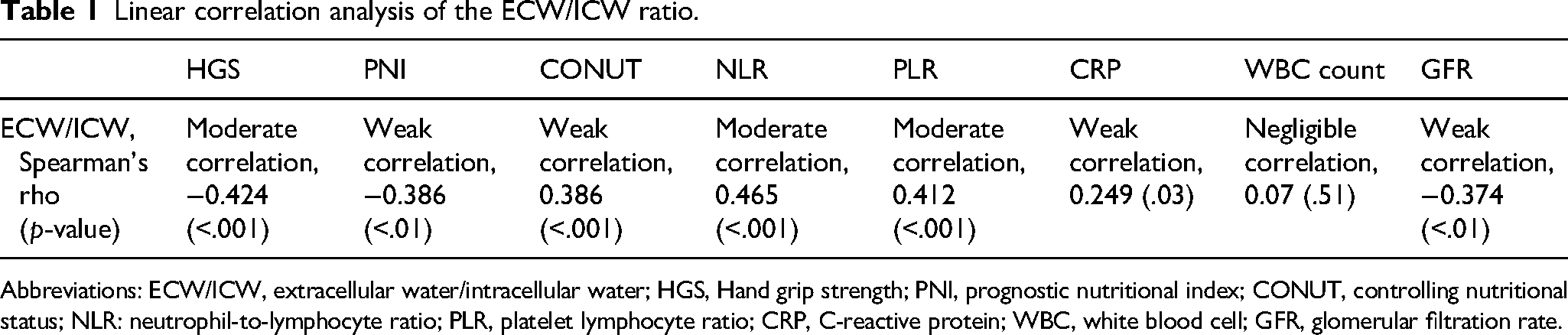
Abbreviations: ECW/ICW, extracellular water/intracellular water; HGS, Hand grip strength; PNI, prognostic nutritional index; CONUT, controlling nutritional status; NLR: neutrophil-to-lymphocyte ratio; PLR, platelet lymphocyte ratio; CRP, C-reactive protein; WBC, white blood cell; GFR, glomerular filtration rate.
Cox's multivariate regression analysis showed that the ECW/ICW ratio (HR: 2.73, 95% CI: 1.13–6.57, p = .02) and neutrophil-to-lymphocyte ratio (NLR; HR: 1.30, 95% CI: 1.11–1.52, p < .01) were risk factors associated with early mortality.
Conclusions
The ECW/ICW ratio has been proven to be associated with short-term mortality in patients admitted with DFU. The same finding has just been reported in patients undergoing hemodialysis.1,3 Furthermore, we have found a significant correlation between ECW/ICW and renal impairment, malnutrition, muscle strength, and inflammation. Other studies also reported that an increasing ECW/ICW was associated with malnutrition, 9 inflammation, and decreased muscle quality. 10 Fluid leakage into the interstitial space is characteristic of inflammation, and we have found a correlation between ECW/ICW and inflammation, as determined by the NLR, platelet-to-lymphocyte ratio, and C-reactive protein, but not with the white blood cell count. The NLR had previously been related to infection severity 11 and morbimortality 12 in patients with DFUs. Furthermore, the ECW/ICW was also significantly correlated with the 2 nutritional scores evaluated in the present study. Malnutrition is multifactorial in these patients. Intestinal edema is associated with endotoxin translocation 13 and malabsorption. Cytokines released during inflammation could also increase protein catabolism and produce anorexia. Therefore, inflammation in patients with DFU 4 might lead to malnutrition and muscle loss. Since the 2 scores used in the present study, CONUT and PNI, include albumin and the lymphocyte count, it is not unusual that both nutritional screenings correlate with ECW/ICW in our study. Based on our findings, the ECW/ICW ratio could be a reliable marker of MIA syndrome. However, further research is needed.
Our study has limitations. The sample size was small and from a single center with a short follow-up. Furthermore, most patients were male, which could generate bias. We understand that ECW/ICW is influenced by the comorbidities present in these complicated patients and it could be a confounding factor. Finally, the presence of infection was not recorded in the database, and it would be interesting to study the impact of infection in ECW/ICW.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Every patient provided written informed consent to enter this study, approved by the Ethics Committee of Juan Ramón Jiménez Hospital (Huelva, Spain) with the number PI 010/20.