
Abstract
Low macrophage viability in chronic diabetic foot ulcers (DFUs) may lead to inadequate interleukin (IL) expression and the persistence of infection. This study evaluates the association between macrophage function, IL-2 expression, and wound microflora in chronic DFUs. Diabetic patients with DFUs (group 1, n = 40) and without DFUs (group 2, n = 40) were compared for macrophage function in serum by viability testing. Immunological response was measured by serum IL-1β, IL-2β, and IL-10 levels. The aerobic and anaerobic microflora of the DFUs were assessed by culture and molecular methods. Demographic, clinical, and biochemical factors were statistically analyzed by χ2 test and Student t test. Multiple correspondence analysis (MCA) was used to detect the pattern of association between glycosylated hemoglobin (hemoglobin A1c), serum IL-2 levels, and macrophage viability. Of the total DFU cases, 22 (55%) showed the presence of polymicrobial microflora. Low macrophage viability with predominant Gram-negative flora was seen in 10 (25%) cases in group 1. Serum IL-2 levels were significantly lower (P = .004) in patients in group 1 along with elevated levels of hemoglobin A1c (P = .038). MCA showed an association between low viability of macrophages and lower IL-2 levels and elevated hemoglobin A1c levels with lower serum IL-2 levels. As compared to group 2, the low viability of macrophages was significantly associated (P = .007) with lower IL-2 levels in group 1. Elevated hemoglobin A1c levels are strongly associated with lower IL-2 levels and low macrophage viability. This might be a contributing factor to the persistence of infections in chronic DFUs.
Diabetes mellitus (type 2) is one of the fastest-growing noncommunicable diseases, especially in developing countries. 1 Diabetic foot ulcer (DFU) is a very common and often severe complication. Uncontrolled diabetes further increases the prevalence of such ulcers from 4% to 10%. 2 Estimates indicate that nearly 15% of patients with diabetes mellitus present with DFUs. 3 The pathogenesis of these ulcers sequentially follows the processes of peripheral neuropathy, poor immune response, bony deformity, peripheral vascular disease, and injuries or traumatic wounds. 4
Wound healing is a complex interplay of several events, including inflammation and angiogenesis, mediated by several macrophage-induced cytokines and growth factors. 5 The role of macrophages in wound healing cannot be overemphasized. In addition to their prominent scavenger actions in removing bacteria and nonviable wound tissue, macrophages also play a major role in the overall immune modulation locally in the healing wound. The activation of these macrophages is in turn dependent on key interleukins (ILs) such as IL-1, IL-2, and IL-10. IL-2 has an essential role in the modulation of the immune system in terms of tolerance, T-cell activation, bacterial cell killing, and in discriminating between “self” and “foreign” stimuli. In diabetic patients, IL-2 levels have been reported to be decreased, which leads to poor antibacterial defense and in turn, further complicates wound healing. 6 Hence, macrophage dysfunction in the presence of uncontrolled DM, bacterial colonization, and inadequate cytokine expression in the DFU can play a significant role in nonhealing. 6 With this background, the present study was carried out to assess macrophage function in association with the bacterial profile and cytokine levels in patients with DFU.
Methods
Study site: A case–control study was carried out in the Department of General Surgery and Microbiology of our University tertiary care hospital. The study was of 2 years duration and was approved by the Institutional Ethical Committee, and informed consent was obtained from the participants.
Study population: It consisted of diabetic patients with and without DFUs attending the wound clinic of the 2000-bedded tertiary care hospital. Considering the prevalence rate of DFU of 10% in population-based studies, sample size was calculated to be 35, using the formula n = (Zα/2) p (1 – p)/d2, where n = required sample size, Z = value for the level of confidence at α confidence level, p = expected prevalence, d = precision at 10% error rate. However, considering the loss to follow-up and to increase the power of the study, 40 patients were included in each group. The study population was divided into 2 groups: Group 1 with 40 type 2 diabetic patients with DFUs, and Group 2 with 40 type 2 diabetic patients without DFU, all in the age group of 18 to 60 years. Infection in DFU was defined by the presence of one or more of the factors including redness, exudate, discolored ulcer edges, foul odor, local edema, and pain. 7 Inclusion criteria for group 1 were DFUs of more than 6 weeks duration and not undergoing any systemic antibiotic treatment for their wounds in the last 30 days. Patients with sepsis, osteomyelitis, pregnancy, malignancy, and immune suppressive disorders were excluded from the study in both groups. Subjects were randomly assigned to the groups. Relevant data on patients’ demographic details, duration of DFU, body mass index, and the size and depth of DFUs were collected. Laboratory values of complete blood count, fasting and postprandial blood sugar, and glycosylated hemoglobin (HbA1c) were recorded.
Sample Collection
Samples from DFUs were collected by using Levine's technique. 8 Prior to sample collection, the wound surface was cleansed using sterile saline-moistened gauze. Using Levine's technique, a sterile cotton swab was rotated over a 1 cm2 area with sufficient pressure to express tissue fluid. The swab's tip was placed in sterile transport media and taken immediately to the microbiology laboratory. Tissue fluid, if available, was also collected by sterile syringes in sterile vials for the culture. The samples were divided into 2 parts, one for quantitative aerobic culture and the other for detection of common anaerobes using molecular methods. All the samples were subjected to Gram staining for direct observation. Whole blood and serum samples were also collected for macrophage function and serological estimations of ILs, respectively, and stored at −80 °C until further estimation.
Aerobic Culture
All the samples were inoculated on Blood agar and Mac Conkey agar (HiMedia Laboratories Pvt. Ltd) and incubated at 37 °C overnight. Colony forming units (CFUs) were calculated to determine the total bacterial count on each plate using the following formula:
CFU/mL = (number of colonies × dilution factor)/volume of the culture plate.8,9 Further growth on the culture plates was identified by colony morphology, Gram staining, and standard biochemical tests.
Detection of Anaerobic Organisms
Due to the unavailability of an anaerobic culture facility, molecular detection of targeted common anaerobes was performed. The genomic DNA extraction was carried out using QIAmp DNA mini kit (Qiagen) as per the manufacturer's instructions from tissue/wound fluid samples. The quality of the DNA was measured by NanoDrop analysis (Thermo Fisher Scientific). The extracted DNA was stored at −20 °C for further processing. Four genera of anaerobes (Bacteroides, Peptococcus, Clostridium, and Prevotella) were screened through conventional polymerase chain reaction (PCR) using genus-specific primers. 10 PCR products were run on 1.5% agarose gel along with a molecular marker of 100 bp ladder (GeNei Laboratories Pvt. Ltd).
Macrophage Function Test
Trypan blue dye exclusion test was performed to determine the viability of macrophages. Trypan blue test stains dead cells blue which takes up the color due to defects in cell membranes as against intact cell membranes in living cells which do not take the color. For this, blood components were separated by density gradient centrifugation using the Ficoll solution (Sigma Aldrich Chemicals Pvt. Ltd). Equal parts of the interphase layer of mononuclear cells and 0.4% trypan blue solution (Sigma Aldrich Chemicals Pvt. Ltd) were added. Following incubation at room temperature for 2 min, the cells were visualized in a hemocytometer. Cells-stained blue was identified as low viability and unstained ones were considered as viable. 11 Additionally, macrophage viability was also investigated through 3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide (MTT) assay (Elabscience Biotechnology Co. Ltd) as per the manufacturer's instructions. The assay was carried out in a 96-well microplate, and the optical density was measured at 570 nm using a microplate reader (LisaScan® EM Elisa plate reader, Transasia Bio-Medicals Ltd).
Estimation of Immunological Responses in Patient's sera
The estimation of the IL-2 beta response in the patient's sera was done by Human IL-2 ELISA Kit PicoKine™ (Boster Biological Technology) as per the manufacturer's instructions. For the estimation of IL-1β and IL-10 response, GenLISATM Human ELISA kit (KRISHGEN Biosystems) was used as per the manufacturer's instructions.
Statistical Analysis
The 2 groups were compared on various factors. The χ2 test was used for categorical variables, and the Student t test was used to compare the numerical variables. Multiple correspondence analysis (MCA) was used to detect the pattern of association between the hemoglobin A1c levels, IL-2 levels, and macrophage nonviability. The association between the variables was inferred in terms of the degree of closeness and clustering of points on the map along with the angle from the origin and points’ position in the quadrant. 12 Statistical tool SPSS, version 23 (IBM Corporation) and 2021 Medcalc software (version: bvba) were used for the analyses. Values of P less than .05 were considered significant.
Results
The study population in group 1 showed a mean age of 50.0 ± 5.9 years with male to female ratio of 13:27. In group 2, mean age was 49.5 ± 6.43 years with male to female ratio of 26:14. The mean ulcer size in group 1 was 20.8 ± 16.46 cm2, ranging from 1.3 cm2 to 78 cm2. In both groups, a majority of the subjects (90%-95%) were within normal BMI. Blood levels of fasting (P = .302), postprandial (P = .23) glucose, and hemoglobin A1c (P = .001) were raised in group 1 as compared to group 2 (Table 1).
Comparison of the Clinical Characteristics and Biochemical Parameters Between Group 1 and Group 2.
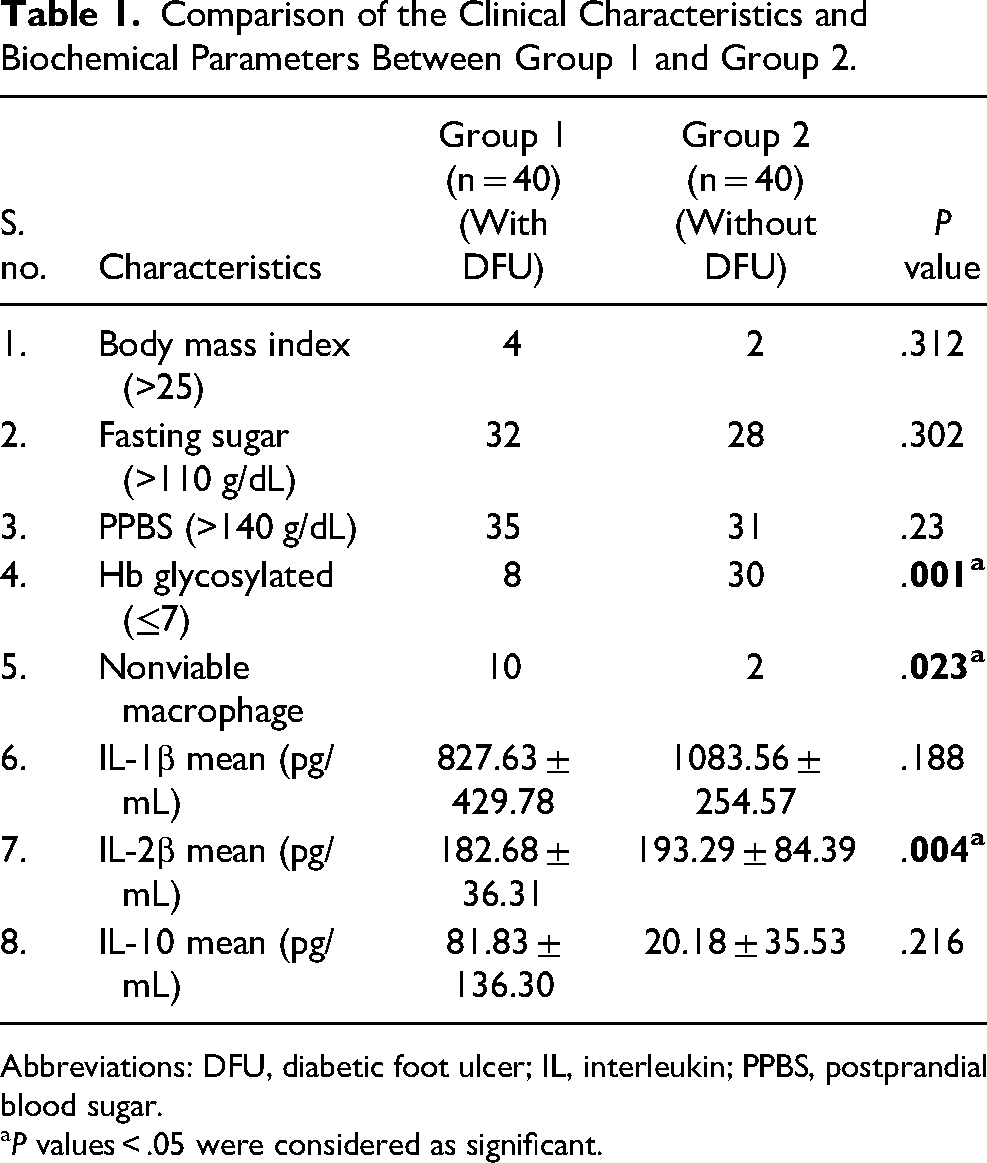
Abbreviations: DFU, diabetic foot ulcer; IL, interleukin; PPBS, postprandial blood sugar.
P values < .05 were considered as significant.
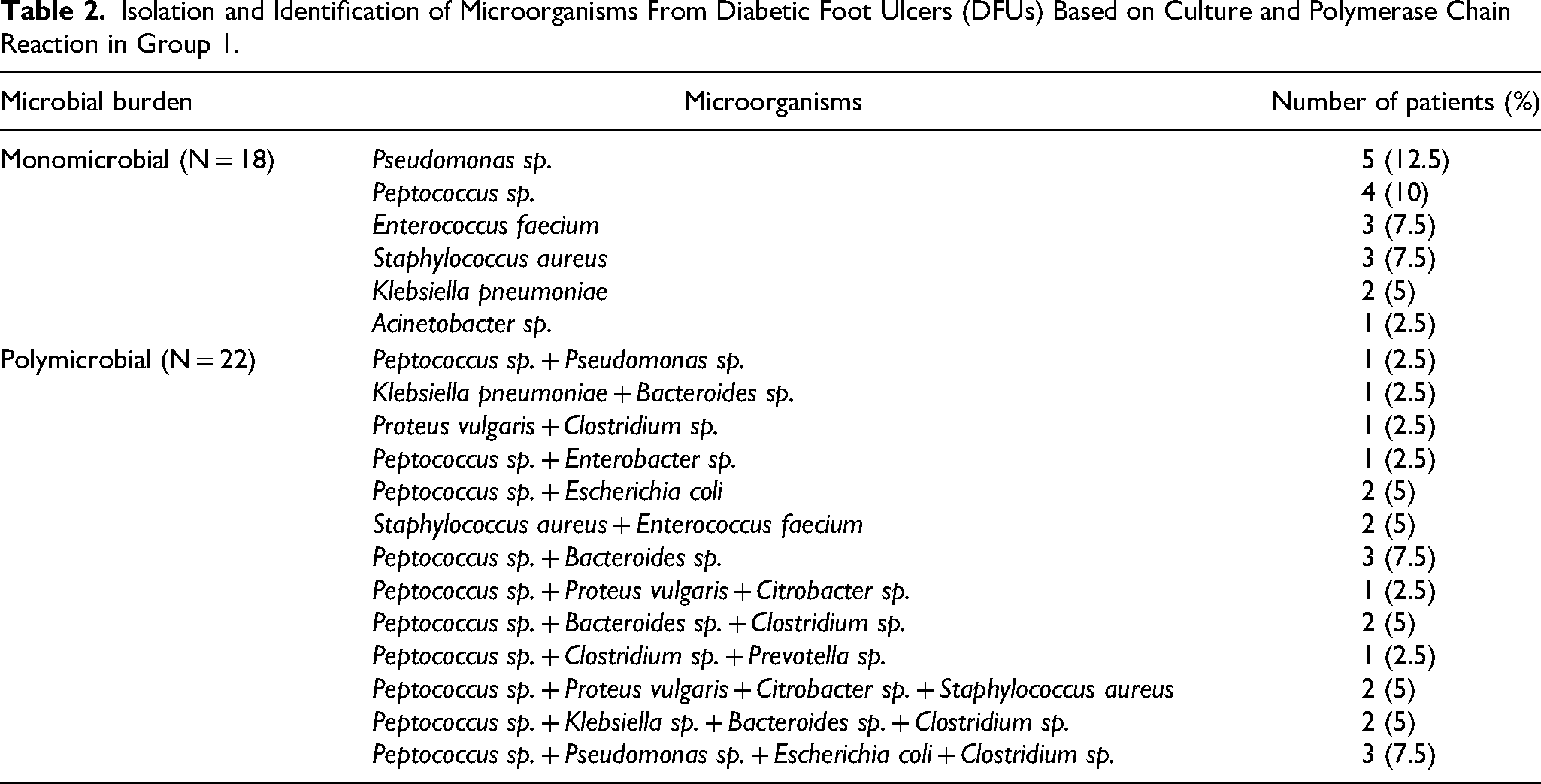
Among the DFU cases, 18 cases (45%) had monomicrobial wound flora, whereas 22 (55%) had polymicrobial flora. In culture reports, Gram-negative organisms were detected in 20 (50%) cases, Gram-positive organisms in 8 (20%) cases, and mixed organisms in 2 (5%) cases. All the aerobic growth showed CFU count > 106 CFU/mL by quantitative culture. Pseudomonas aeruginosa, followed by Staphylococcus aureus, was the most common organism in culture, whereas Peptococcus was the most common anaerobe isolated. The complete microbial profile is shown in Table 2.
Isolation and Identification of Microorganisms From Diabetic Foot Ulcers (DFUs) Based on Culture and Polymerase Chain Reaction in Group 1.
On screening for the viability of mononuclear cells, viable cells were seen in the majority of the cases in group 2 (38/40; 95%). However, in group 1, low viability among the mononuclear cells was seen in 10 cases (25%). On comparison with the microbial profile, all these cases with lower macrophage viability had DFUs that screened positive for Gram-negative organisms only. Additionally, all cases with low macrophage viability had larger sizes (mean = 37.48 ± 12.46 cm2) and longer duration of DFUs (mean = 278 ± 3 days).
The mean values of estimated cytokines are shown in Table 1. There was a significant difference between serum IL-2 levels (P = .004) in group 1 and 2 cases. No significant differences could be observed in the other IL levels. The DFU size in group 1 was not significantly associated with the serum IL-2 levels (P = .93). The serum levels of IL-2 were found to be significantly associated with hemoglobin A1c (P = .038). All cases of low macrophage viability had elevated levels of hemoglobin A1c and lower levels of IL-2 as shown in Table 3. MCA showed a strong association between nonviable macrophages and lower IL-2 levels and viable macrophages with higher IL-2 levels. Also, elevated levels of hemoglobin A1c were found to be associated with lower IL-2 levels as shown in the MCA scatter plot in Figure 1. The comparison of the viability of the macrophages with the IL-2 levels within group 1 and those of group 2 is shown in Table 4. Low macrophage viability was found to be significantly associated with lower IL-2 levels in patients with DFUs. No such association was seen in group 2.
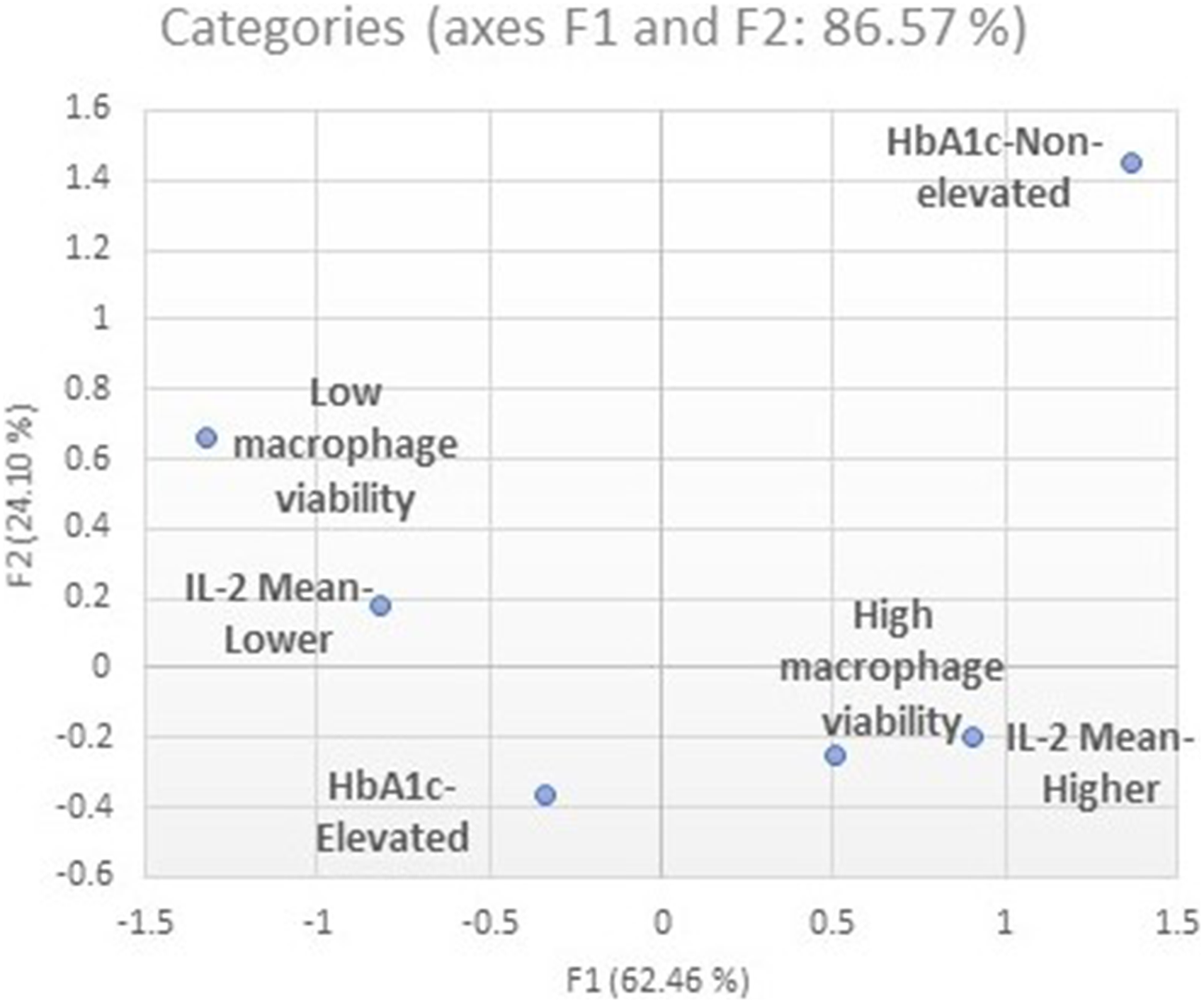
Association between hemoglobin A1c level, interleukin (IL)-2 level, and low macrophage viability obtained by multiple correspondence analysis.
Comparison of Hemoglobin A1c With IL-2 Level and Macrophage Nonviability.
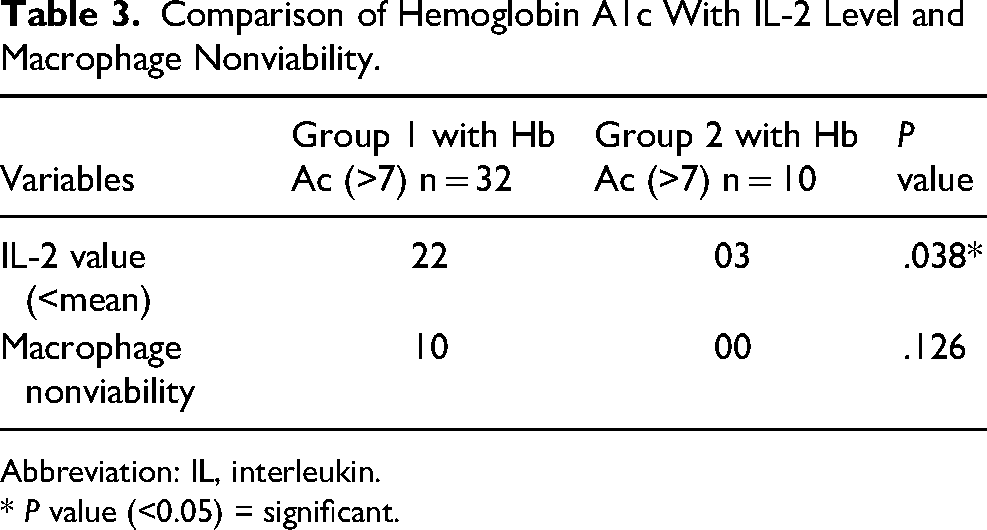
Abbreviation: IL, interleukin. * P value (<0.05) = significant.
Comparison of the IL-2 Levels With Macrophage Viability in Group 1 and Group 2.
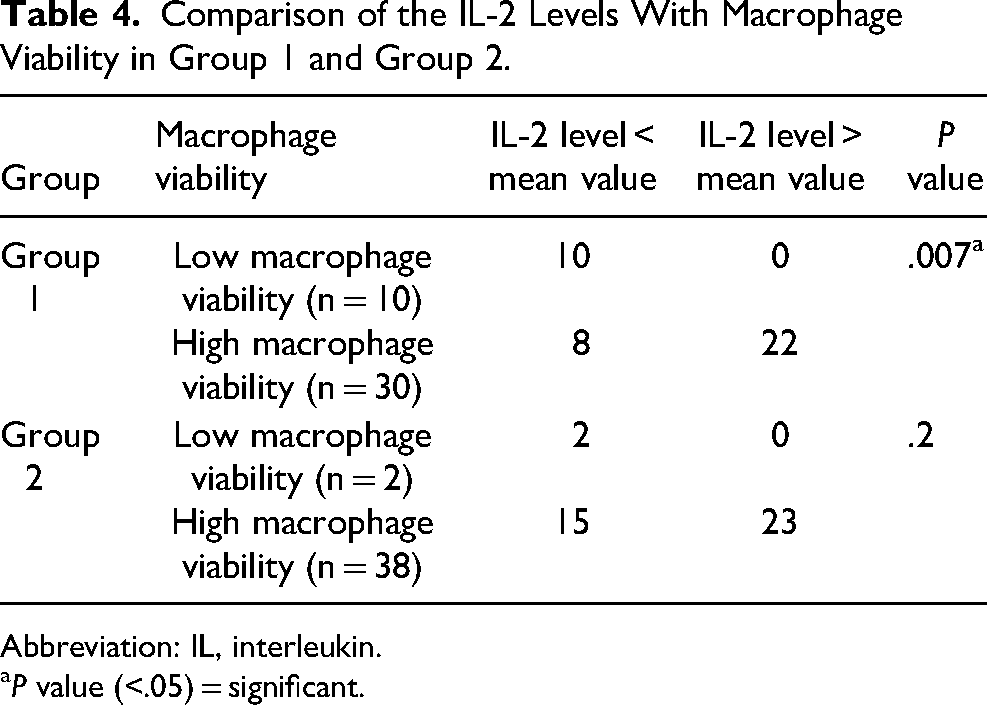
Abbreviation: IL, interleukin.
P value (<.05) = significant.
Discussion
The sharp rise in the incidence of diabetes mellitus has been in parallel with the concurrent increase in DFUs as a major complication. 13 Wound healing in DFUs is a complex process and is closely related to poor vascularity, neuropathy, and altered immune function. The macrophage function, cytokine levels, and interaction with microflora in the wound bed are significant determinants of healing. Recent studies on the effect of wound microflora and the outcome of treatment have shown a changing epidemiology of predominance of Gram-negative bacteria against Gram-positive bacteria.7,14 This study also revealed the increased isolation of Gram-negative bacteria from chronic DFUs. Although not within the scope of this study, excessive systematic and topical antibiotic use have often been held responsible for this change in DFU flora. 15
Macrophages form the key cells in the process of wound healing. The activation of these macrophages is stimulated by pro-inflammatory cytokines. 16 The recent interest in the role of macrophages in wound healing has revealed that they are the single most effective means of removal of activated neutrophils from the wound bed through the M1 phenotype. 16 Neutrophils and their release reaction kill bacteria and also cause much tissue damage as well as breaking down of wounded matrix. Therefore, these cells need to be removed systematically by apoptosis to promote wound healing. Otherwise, their persistence or necrosis in the wound bed causes a prolonged inflammatory phase (hyperinflammation), which in turn stalls the onset of the proliferative phase. Macrophages are responsible for removing these neutrophils systematically through phagocytosis. However, due to the poor viability of these macrophages in the wound bed of DFU, especially in the presence of pathogenic microflora, this function cannot be executed adequately.5,16 These macrophages become locked in the pro-inflammatory phase, thus delaying healing and facilitating wound infection. One of the simplest and cost-effective methods to check the viability of macrophages is the trypan blue staining which has been employed in this study. Interestingly, DFUs with nonviable macrophages in this study were associated with Gram-negative microflora. It has been seen that lipopolysaccharides in the outer membrane of Gram-negative bacteria are an important factor known to activate the pro-inflammatory phases of macrophages. 17 In addition, the common Gram-negative organisms such as Pseudomonas spp, Klebsiella, and other Enterobacteriaceae members are also strong biofilm producers. There has been substantial evidence that bacterial biofilms negatively affect the healing process in chronic wounds. 18 Macrophage nonviability, therefore, might be one of the causes responsible for the persistence of these organisms in chronic DFUs.
The immunological response involving the T lymphocytes is significant in the pathophysiology of diabetes mellitus and DFU.
12
Exposure of granulocytes to long-term uncontrolled hyperglycemia often compromises their functions. One study showed
12
the upregulation of IL-2, IFN-γ, and TNF
Previous studies have observed that IL-2 or IL-2 receptor deficiency occurs in type 2 diabetes mellitus, although its cause has not been largely elucidated.20–22 In the present study, we found elevated levels of hemoglobin A1c to be significantly associated with lower levels of IL-2 and indirectly with low macrophage viability. The association between elevated hemoglobin A1c and decreased phagocytic activity of the neutrophils has been suggested in previous studies,23,24 predisposing diabetics with poor glycemic control to infections, which is in concurrence with the results of the present study. Consequently, the importance of glycemic control in diabetic patients cannot be overemphasized in order to prevent complications resulting from infections in chronic DFUs. Based on the study findings, we propose immunological and microbiological assessment of chronic DFU cases for better prediction and management of wound healing.
The present study is not without limitations. While a small sample size was involved, better diagnostic assays such as the macrophage culture, could not be performed due to the limitation of available resources. Besides, few confounding factors like other vascular parameters which could have affected the findings were not studied. However, the study provided an initial suggestion toward a meaningful association between elevated hemoglobin A1c levels, lower serum IL-2 levels, and low macrophage viability. The predominance of Gram-negative bacterial microflora in these DFU cases and its association with low viability of macrophages and poor IL-2 expression has not been examined before. This study, therefore, establishes a foundation for research on macrophage viability/dysfunction and the role of biofilm formation in DFU cases which could help predict the risk factors for chronicity and thereby assist in early intervention. Additionally, levels of hemoglobin A1c, serum IL-2, and tests for macrophage viability could be used as predictive markers of healing in chronic DFU. Such cases would require antibiotic therapy directed against Gram-negative microflora as revealed in this study.
Conclusion
The present study revealed strong associations between elevated levels of hemoglobin A1c, low serum IL-2 levels, low macrophage viability, and the presence of Gram-negative bacteria microflora in patients with chronic DFU, which could be potential factors responsible for delayed wound healing. These could be clinically used as predictive markers for healing in chronic DFU.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.