
Abstract
This study was conducted in a methodological design with the aim of adapting the “Diabetic Foot Self-Care Questionnaire of the University of Malaga, Spain (DFSQ)” to Turkish, and examining its validity and reliability. The study population of the methodological research consisted of a total of 161 patients diagnosed with diabetes who presented to the Diabetes Clinic Unit. The translation-back translation technique was employed for the linguistic equivalence of the questionnaire. To test the validity of the scale, linguistic and content validity were examined, and exploratory factor analysis was conducted. Cronbach's alpha reliability coefficient, item-total score correlations test, and test–retest technique were used to assess the reliability of the scale. The scope validity index values of the Turkish version of DFSQ ranged between 0.85 and 1.00, and there was no difference in scores given by the consulted experts (Kendall's W = 0.720; p = .707). Exploratory factor analysis conducted to examine the factor structure of the scale revealed that the scale consisted of 16 items and three subscales, explaining a total variance of 84.09%. The factor loadings of the scale ranged from 0.90 to 0.97. The calculated Cronbach's alpha coefficient for the Turkish version of the scale was 0.66.: It was found that the Turkish version of DFSQ is valid and reliable for the Turkish population. The research identified that DFSQ is a valid and reliable tool for determining diabetic patients’ knowledge and attitudes toward foot self-care in cross-cultural studies.
Introduction
The increasing prevalence of diabetes mellitus (DM) and its associated complications, ranging from morbidity to mortality, pose a global health problem. 1 According to the International Diabetes Federation, there are currently 415 million diabetics worldwide, and it is projected to increase by 55% to reach 642 million by the year 2020.2,3
In Turkey, a similar increase in diabetes prevalence has been observed, with a nationwide comprehensive study reporting a prevalence rate of 13.7%.3,4 Diabetic foot, one of the most significant complications with high mortality and cost, is more prevalent in diabetes. Studies have reported that the likelihood of diabetic foot occurrence throughout a lifetime in individuals with diabetes is approximately 15% and the risk of amputation in diabetic individuals is reported to be 25 times higher compared to those without diabetes. Within two years following the first amputation, the incidence of a second amputation in the contralateral extremity is 50%.5,6 Compared to cancer statistics, the 5-year mortality rates of individuals who have undergone lower extremity amputation due to diabetic foot ulcers are concerning. 4 According to official published data, it has been determined that in Turkey, in the last few years, there are over one million people with diabetes, and half a million people have been diagnosed with diabetic foot infections. Diabetic foot ulcers resulting from neuropathy contribute to the loss of sensation in the feet, compromised tissue integrity, and susceptibility to minor trauma and ulcer development. This leads to a decline in quality of life, increased amputations, and higher treatment costs. 7 Cavanagh reported that the costs associated with diabetic foot vary between $3096 and $107,900 per patient in five different countries. The direct cost of diabetes treatment worldwide was $237 billion in 2017, with one-third of this cost being spent on lower extremity complications. 8
The American Diabetes Association (ADA) has stated that foot care education and daily foot care practices can prevent amputations caused by diabetes by 50%. 1 As with other complications, glycemic control is crucial for preventing diabetic foot ulcers. Tight glycemic control (HbA1c < 7%) can reduce amputations by 35%. 1 It is crucial to conduct regular diabetic foot examinations, provide appropriate footwear, and ensure proper treatment of nonulcerative pathological conditions in individuals with diabetes. Comprehensive diabetic foot risk assessment, patient and healthcare professional education, and a multidisciplinary team approach to foot care can reduce foot complications and amputations by 85%. 2 Self-care behaviors in diabetes are defined as the behaviors individuals with diabetes or at risk of diabetes engage in to stay alive. 9 The self-care behaviors identified by the American Association of Diabetes Educators as contributing to favorable outcomes in individuals with diabetes include exercise, self-monitoring, medication adherence, problem-solving, risk reduction behaviors (smoking cessation, regular eye examinations, foot care), and effective coping strategies.1,9,10
Currently, special guidelines published by the ADA and the International Working Group on the Diabetic Foot address the management of diabetic foot. 1 Patient education and adherence to therapeutic regimens are widely recommended in clinical guidelines for the management of diabetic foot complications. 2 In this context, the development of patient-reported outcomes (PRO) tools, where the outcomes are reported by patients themselves, has become popular in chronic disease care. PRO tools are personal recording instruments where patients document their overall health status, disease experiences, treatment effectiveness, and side effects. To enable effective diabetic foot self-care, an appropriate assessment tool is needed.11,12 Patient-reported outcome questionnaires are commonly used in this context. 13 However, aside from the mentioned evaluation tools, there is a lack of specific instruments that adequately assess self-care in diabetic foot due to insufficient criteria for evaluating self-foot care.14–20 Flores et al (2015) developed the Diabetic Foot Self-Care Questionnaire of the University of Malaga (DFSQUMA), which is a scale for assessing foot self-care without amputation as reported by patients. 20 Although the original version of the scale is in Spanish, limited cross-cultural adaptations have been made.11,21
In Turkey, there is a considerable number of approximately one million individuals with diabetic foot ulcers. 4 Therefore, there is a need for individual reporting tools that assess the quality of diabetic foot self-care and the factors limiting self-care in our country. Consequently, this study was conducted to adapt the DFSQ into Turkish and examine its validity and reliability properties.
Methods and Materials
Research Design and Aim
This study was conducted in a methodological descriptive design between June 2022 and January 2023 to test the validity and reliability of the “DFSQUMA” in the Turkish population.
Research Sample
The population of the study consisted of patients diagnosed with diabetes who presented to the Diabetes Clinic Unit of a university hospital in Turkey. The sample size for the study was determined based on a power analysis using a similar previous study as a reference, considering a margin of error of 5% (d = 0.05). A total of 162 patients were included in the sample. 11 The study included voluntary patients aged 18 years and older who had been diagnosed with Type I or Type II diabetes. Patients with toe or lower extremity amputations and illiterate individuals were excluded.
Measurement and Procedures Data Collection Tools
The “Patient Identification Form” and the “DFSQUMA” were used to collect research data.
Patient Identification Form
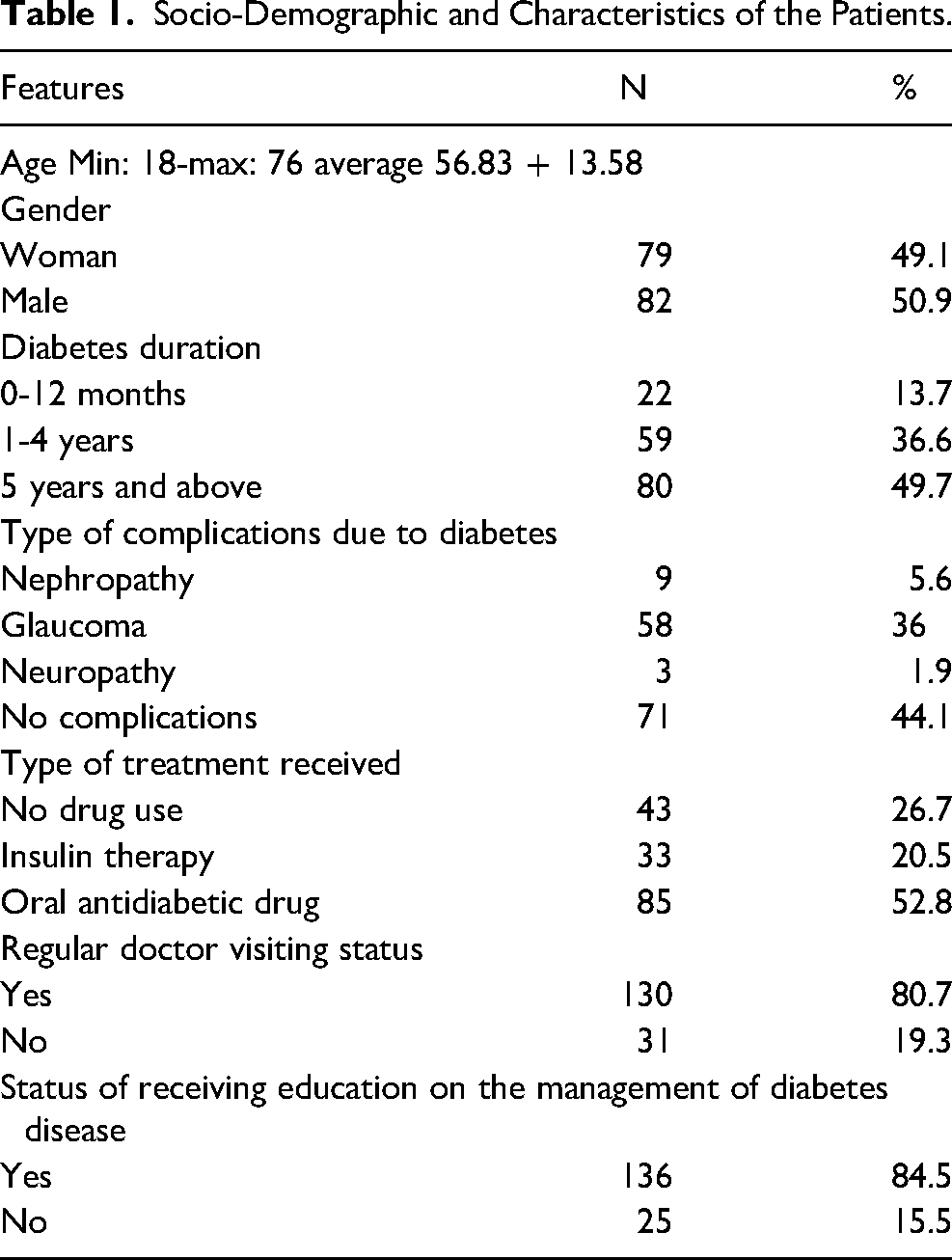
The Patient Identification Form included questions to determine the sociodemographic characteristics of the patients such as age, education level, and gender, as well as disease history and adherence related to diabetes, including the duration of diabetes diagnosis, treatment type, type of complications related to diabetes, diet, and exercise (Table 1). The form comprised a total of 15 questions.
Socio-Demographic and Characteristics of the Patients.
Diabetic Foot Self-Care Questionnaire
The “DFSQUMA” was developed by Flores et al (2015) in Spain. 22 The original version of the questionnaire is in Spanish. The questionnaire consists of a total of 16 questions, addressing self-care for preventing diabetic foot (first seven items), self-care management (items 8-11), and questions regarding the importance and selection of shoes and socks (items 12-16). The DFSQ includes three subscales: “self-care,” “self-care management,” and “shoes and socks” (Table 2). Each question has a 5-point Likert-type response scale, with option A scored as five points, option B as four points, option C as three points, option D as two points, and option E as one point. The scale was conducted between October 2012 and March 2013 at the Pediatric Clinics and Diabetic Foot Unit of the University of Malaga, Spain. After conducting psychometric tests on a sample of 209 diabetic patients, the questionnaire was finalized with 16 items, and found to be valid and reliable. Cronbach's alphas were 0.89 after excluding four items due to low reliability. The interitem correlations were on average 0.34 (range: 0.06-0.74). 22
Cross-Cultural Adaptation Linguistic Equivalence
For the linguistic equivalence of the DFSQ from Spanish to Turkish, the translation-back translation technique was used. Two language experts, fluent in Turkish and proficient in Spanish, translated the expressions in the scale into Turkish. Then, two different experts, who were fluent in both languages and unaware of the original scale, translated the Turkish version back into Spanish. The final translation was obtained by merging the translations made by both experts. A language expert, fluent in Spanish as their native language, verified whether the Spanish and Turkish versions corresponded to each other. The scale was finalized by the researchers, ensuring equivalence in both languages, and making necessary adjustments for content validity.
Content Validity
After achieving linguistic equivalence, the comprehensibility, appropriateness, and content validity of the expressions in the final Turkish version of the scale were evaluated by consulting seven experts, including six academic staff members and one diabetes education nurse. Using the Davis technique, the experts rated their opinions on the initial version of the scale, assigning scores as “A-Appropriate” (four points), “B-Needs minor revision” (three points), “C-Needs major revision” (two points), and “D-Inappropriate” (one point) for each expression. The “content validity index” (CVI) for each item was calculated by dividing the number of experts who marked options A (four points) and B (three points) for the item by the total number of experts. A CVI value above 0.80 is considered acceptable for items. 23 Since all items in the scale had a CVI value higher than 0.80, no item was removed from the scale in terms of content validity. The scale items were rephrased according to the experts’ opinions, resulting in the most suitable expressions.
Pilot Application
After linguistic adaptation and content validity, a pilot application was conducted with 10 patients who had the same characteristics as the target sample to evaluate the comprehensibility of the expressions in the scale. Since there were no incomprehensible items in the scale during the pilot application, no changes were made to the scale, and validity/reliability analyses were performed. The patients participating in the pilot study were not included in the research sample.
Data Collection Method
The data were collected by the researcher through face-to-face interviews. To test the test–retest reliability of the scale, the same sample (44 patients) was reevaluated at a 3-week interval. The average interview duration for each questionnaire was approximately 10-15 min.
Data Analysis
The data obtained in the study were analyzed using Statistical Package for Social Sciences for Windows 24.0 program. Kendall's W concordance coefficient and the Davis technique were used for evaluating linguistic validity. 23 Descriptive statistics were used to analyze the socio-demographic characteristics of the patients. For the validity study of the scale, content validity and construct validity analyses (exploratory factor analysis [EFA]) were performed. Kaiser–Meyer–Olkin (KMO) Sampling Adequacy and Bartlett's Sphericity tests were used to evaluate the suitability of the scale for factor analysis. Item-total correlation coefficients and Cronbach's alpha (α) reliability coefficients were calculated to determine the reliability level of the scale. Test–retest was also conducted to assess the stability of the scale over time. In statistical analysis, p < .05 was considered statistically significant.
Limitations of the Study
The fact that the study was conducted in a single center constitutes a limitation of the study.
Ethical Considerations
Prior to the data collection process, permission was obtained via email from Flores, one of the researchers who developed the original scale, to use the scale in the Turkish patient sample and to adapt it to Turkish. Ethical approval was obtained from the Ethics Committee of the relevant university for the subsequent stages of the study, and permission to conduct the study was obtained from the institution. Communication was established with the authors via email for the adaptation of the scale to Turkish, and permissions were obtained. In addition, the purpose of the study was explained to the patients included in the research sample, and their verbal consent was obtained. The study procedures were conducted in accordance with the Helsinki Declaration.
Results
Participants
The average age of the patients included in the study was 56.83 ± 13.58 years, and 49.1% of them were female. It was found that 49.5% of the patients had been diagnosed with diabetes for more than 5 years, 52.8% were receiving oral antidiabetic medication, 80.7% regularly attended check-ups, and 84.5% received education about the disease. When the type of complications developed due to diabetes was questioned, it was found that 44.1% of the patients had no complications, while 36% had diabetic retinopathy and 5.6% had nephropathy.
Content Validity
After ensuring linguistic validity, the content validity was evaluated by presenting the scale to seven experts. The majority of the expressions in the scale were rated as “Needs minor revision” (3 points) and “Appropriate” (4 points). According to the Davis technique, the CVI for each item was between 0.85 and 1, and the total CVI of the scale was 0.96.23,24 The expert opinions showed no significant discrepancies in the scoring, indicating a significant agreement (Kendall's W = 0.263; p = .024).
Construct Validity (Factor Analysis)
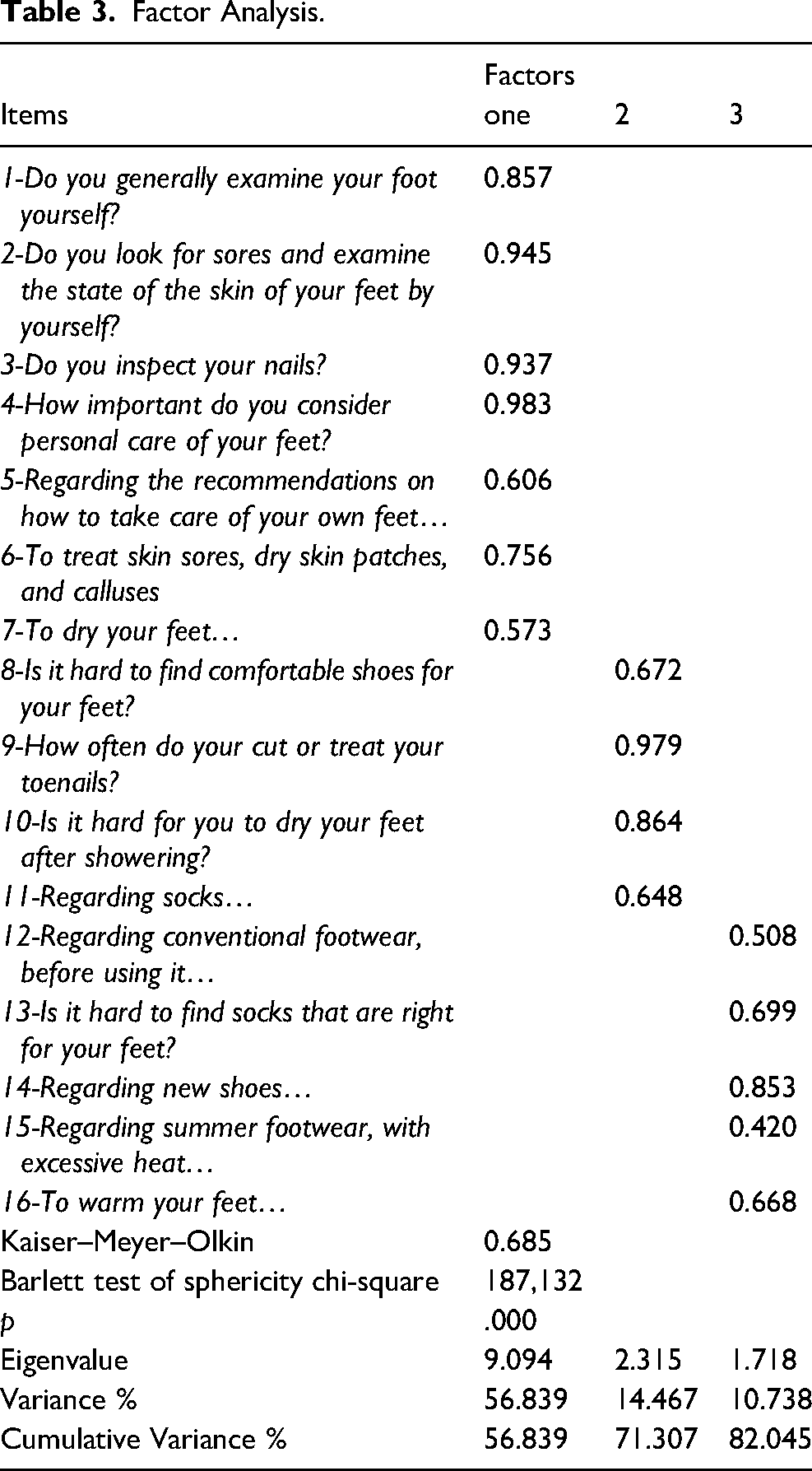
To determine the factorial structure validity of the scale, an EFA was conducted. In this study, the KMO value was calculated as 0.685, and Bartlett's Test of Sphericity yielded χ2 = 187.132; p < .001, indicating that the scale data were suitable for factor analysis. The rotated solution revealed a three-factor structure for the questionnaire, accounting for a total of 82.045% of the observed variance: personal self-care (items 1-7), podiatric care (items 8-11), and footwear and socks (items 12-16). According to the EFA, the factor loadings of the items in the first factor ranged from 0.573 to 0.983, in the second factor from 0.648 to 0.979, and in the third factor from 0.420 to 0.853 (Table 3).
Reliability Analysis Item-Total Correlation and Internal Consistency Analysis
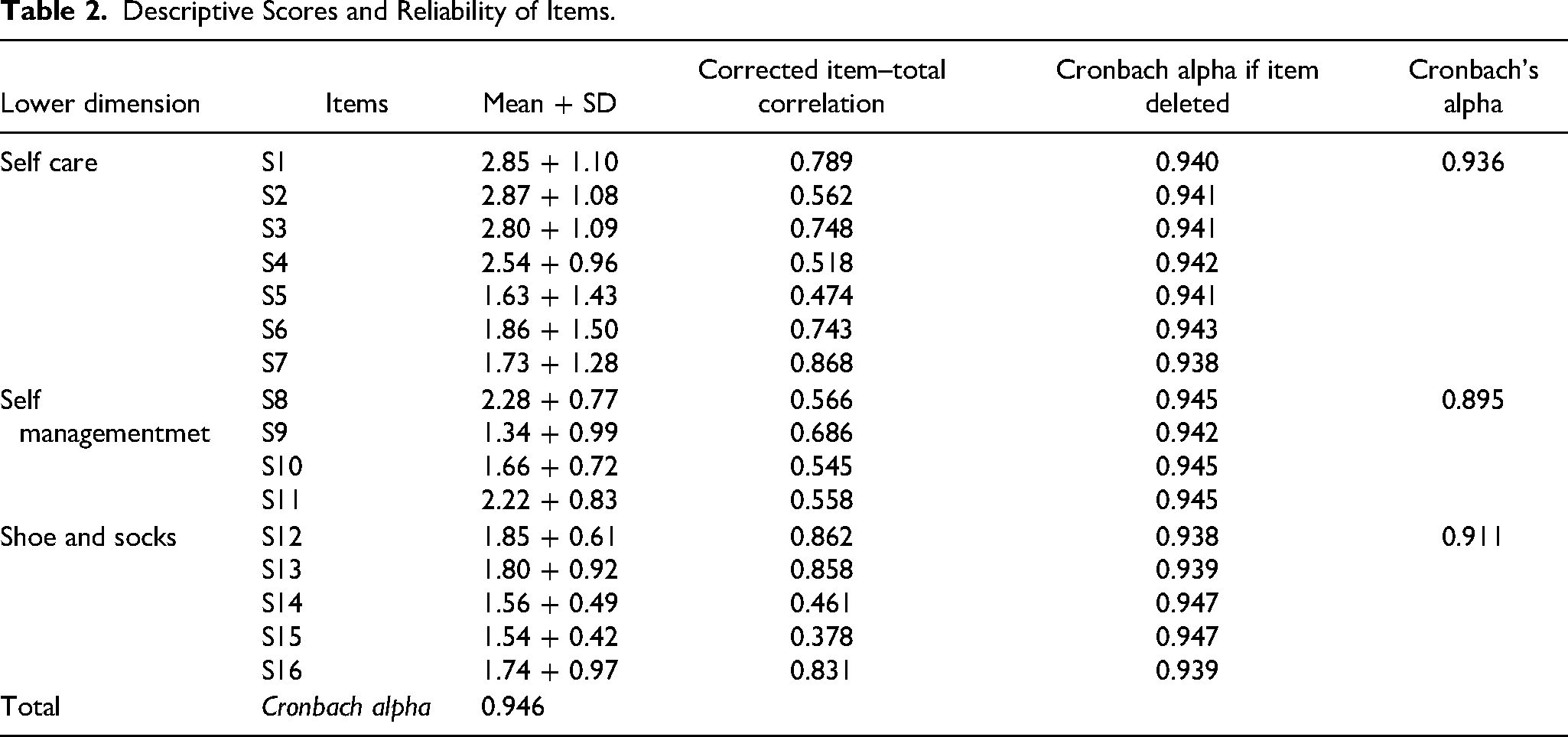
For the reliability analysis, Cronbach's alpha coefficient, item-total correlation, item analysis, and the stability of internal consistency over time were examined. The item-total correlation coefficients of the scale ranged from 0.47 to 0.86 for the “self-care” dimension, from 0.54 to 0.68 for the “self-care management” dimension, and from 0.37 to 0.86 for the “footwear and socks” dimension. Since there were no items with a total correlation score below 0.20, no item was removed from the scale. The item analysis did not identify any items that significantly affected Cronbach's alpha. The Cronbach's alpha reliability coefficient for the entire scale was found to be 0.94. The reliability coefficients for the subscales were calculated as α = 0.93 for self-care, α = 0.89 for self-care management, and α = 0.91 for footwear and socks (Table 2). In the Arabic version of the scale, the total Cronbach's alpha coefficient was 0.95, and the Cronbach's alpha coefficients for the self-care, self-care management, and footwear and socks subscales were 0.93, 0.88, and 0.98, respectively, which were also high as in our study.
Descriptive Scores and Reliability of Items.
Factor Analysis.
Test–Retest Reliability Analysis
In the final stage of the study, a test–retest measurement was conducted at a 3-week interval on 44 patients to test the stability of the scale over time. According to the test–retest analysis, there was no statistically significant difference (p > .05) in the mean scores of the scale factors and the total scale, and the correlation coefficient was 0.98, indicating a strong relationship between the two measurements (p < .001) (Table 4). These results indicate that the scale provides highly reliable measurements.
Test Re-test Statistical Analysis Results.
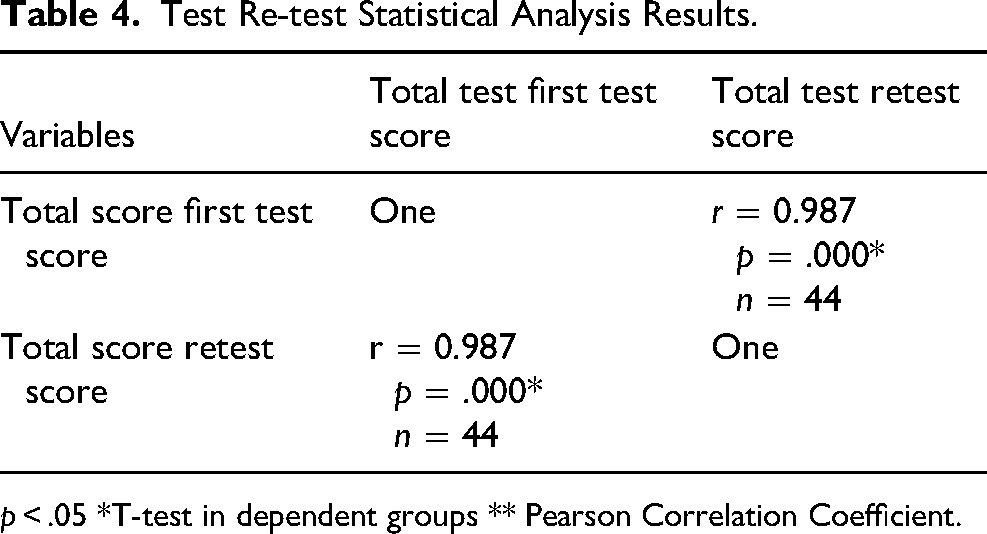
p < .05 *T-test in dependent groups ** Pearson Correlation Coefficient.
Dıscussion and Conclusion
Diabetic foot, one of the major complications of diabetes, is the leading cause of foot and leg amputations. 25 Diabetic foot is a significant health problem due to its impact on prolonged hospital stays, increased costs, morbidity, and mortality.19,24,25 A prevalence study conducted in our country reported that the number of patients with diabetes is over 7 million. 4 In order to improve the quality of life of patients with diabetic foot and reduce care costs, it is critically important for diabetic patients to understand the importance of foot care and ensure self-care. This study aimed to contribute to the literature in our country by examining the validity and reliability of the DFSQ Turkish form, which evaluates foot care in patients with diabetes and examines their knowledge, attitudes, and practices related to diabetic foot care.
Before using measurement tools developed for a specific culture in different cultures, it is necessary to establish linguistic equivalence. 26 In this study, the linguistic equivalence of the Turkish and Spanish versions of the scale was evaluated through the translation-back translation method, and it was determined that the items in both forms were similar, indicating linguistic equivalence.
In scale adaptation studies, content validity is assessed to determine whether the measurement tool adequately measures the desired concept both quantitatively and qualitatively.27,28 In this study, after ensuring content validity, the validity of the scale was evaluated through factor analysis. Therefore, in this study, the CVI of the scale items were calculated using the Davis technique. The obtained CVI values for the scale items ranged between 0.85 and 1, indicating that the items in the scale adequately represented the situations to be measured. According to Kendall's W concordance analysis, there was significant agreement and consistency in the independent expert opinions’ ratings of the scale items (Kendall W = 0.26; p = .02).
After the content and construct validity analyses, the most fundamental characteristic that measurement tools should possess, reliability, was evaluated. 29 In this study, the reliability of the adapted scale was evaluated through test–retest reliability analysis and item-total correlation analysis. According to the test–retest analysis, there was a strong relationship between the repeated measurements, with a correlation coefficient of 0.98. Furthermore, there was no significant difference in the mean scores of the scale factors and the total scale between the two measurements (p > .05). These findings indicate that the scale provides consistent and reliable results in repeated measurements. In the original study of the scale, the reliability was assessed using interitem correlation analysis, and it was found that the reliability of the scale was at an ideal level. 21 In this study, the Cronbach's alpha coefficient for the entire scale was found to be 0.946, and the coefficients for the subscales were α = 0.93, α = 0.89, and α = 0.91. These values indicate that the Turkish version of the scale has sufficient reliability to be used for evaluating patients’ knowledge, attitudes, and practices related to diabetic foot self-care.
In conclusion, based on the findings obtained from the analyses conducted for the adaptation of the DFSQ to the Turkish population, it was determined that the Turkish version of the scale, consisting of 16 items and three subscales, is reliable and valid in Turkish patient groups. It is believed that the scale will be helpful in determining the knowledge and attitudes of diabetic patients about diabetic foot care in our country. Thus, the results obtained from these forms in diabetes patient education programs can guide the organization of educational content, the implementation of appropriate strategies, and the identification of high-risk patient groups.
Footnotes
Acknowledgement
We would like to thank all the nurses who agreed to participate in the study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.