
Abstract
The aim of this nonsystematic mini review was to discuss serum levels of zinc in subjects with diabetic foot ulcers (DFUs). Most studies have reported low zinc levels in subjects with DFUs. Furthermore, there is some evidence that oral zinc supplementation may have a positive and beneficial impact on DFUs healing. Nonetheless, findings have so far not provided definitive answers. More studies are needed to clarify the role of zinc and its supplementation in this setting.
Diabetes mellitus (DM) is a major health problem due to its serious chronic complications, including foot ulcers (DFUs).1,2 The latter can lead to hospitalizations, amputation, increased morbidity and mortality.1,2
Zinc is a significant and quite essential nutrient which is imperative for growth, and development, along with the maintenance of immune function. 3 The deficiency of this nutrient is recorded to be associated with delayed wound healing and immune. 4
Taking under serious consideration the abovementioned claim, in this nonsystematic review article we tried to investigate the potential impact of zinc supplements and treatment on DFUs, along with the levels of this element in DM subjects with DFUs in general by examining the current literature.
Search Strategy
We conducted an electronic search in PubMed, Google Scholar, and EMBASE from January 1984 until June 2023 using combinations of the following keywords: “diabetic foot,” “diabetic foot ulcer,” and “zinc.” Only original articles written in English were included, while references to included studies were thoroughly examined. Animal studies were excluded.
Zinc: An Important Mineral
Zinc is a trace element, which is crucial for the human body’s homeostasis. 5 This micronutrient catalyzes more than 100 enzymes, facilitates protein folding, and is involved in gene expression regulation. 5 Subjects with alcoholism, malnutrition, and inflammatory bowel disease are at an augmented risk of zinc deficiency. 6 In addition, zinc deficiency may become manifest by nonspecific symptoms, such as diarrhea, alopecia, poor wound healing, immunocompromise, growth retardation, nail dystrophy, glossitis, and hypogonadism in males. 6 Zinc supplementation appears to have therapeutic potential in many different medical conditions. 6
Diabetic Foot Ulcers
DFUs are linked with increased morbidity and mortality. They may lead to hospitalization or lower-limb amputation.7,8 DFUs result from peripheral arterial disease, diabetic neuropathy, and infection, often precipitated by a minor trauma.7,8 At a molecular level, impaired angiogenesis, suboptimal chronic inflammatory response, barrier disruption, impaired growth factor function, as well as several aberrant pathways play a role.7,8
Zinc Levels in Subjects With DFUs
Some studies have studied zinc levels in patients with DFUs (Table 1).9-15
Levels of Zinc in DM Subjects With DFUs.
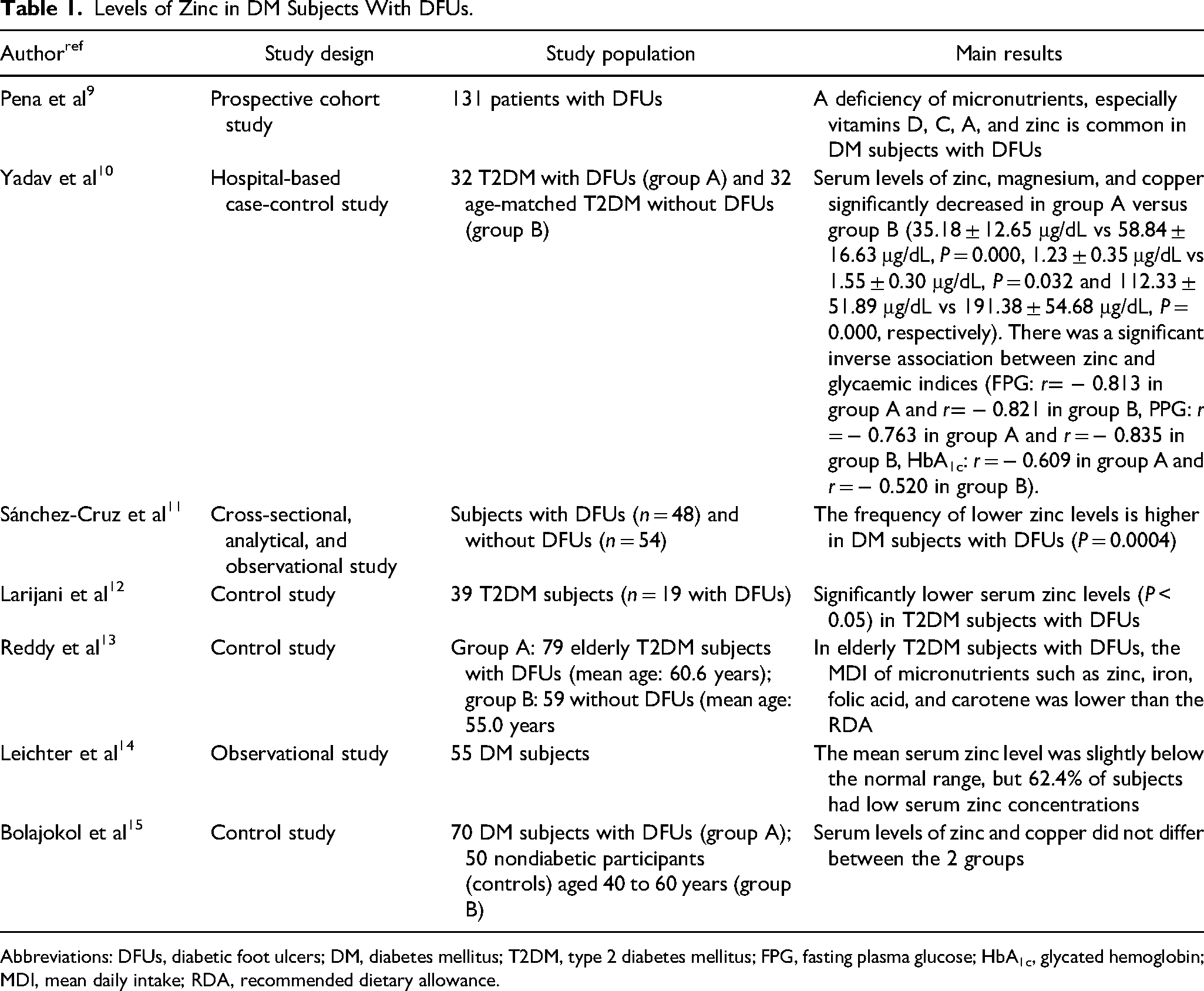
Abbreviations: DFUs, diabetic foot ulcers; DM, diabetes mellitus; T2DM, type 2 diabetes mellitus; FPG, fasting plasma glucose; HbA1c, glycated hemoglobin; MDI, mean daily intake; RDA, recommended dietary allowance.
In a prospective study, Pena et al 9 examined micronutrient status among subjects with DFUs. They found that deficiency of micronutrients, especially vitamin C, vitamin D, vitamin A, and zinc (present in 26.9% of subjects) was common in this series. 9
Yadav et al 10 investigated the status of minerals in T2DM subjects with DFUs. They included 64 subjects aged 40 to 60 years: group A (n = 32) with DFUs and group B (n = 32) without DFUs. 10 Serum levels of zinc, magnesium, and copper were significantly decreased in group A versus group B (35.18 ± 12.65 μg/dL vs 58.84 ± 16.63 μg/dL, P = 0.000, 1.23 ± 0.35 μg/dL vs 1.55 ± 0.30 μg/dL, P = 0.032, and 112.33 ± 51.89 μg/dL vs 191.38 ± 54.68 μg/dL, P = 0.000, respectively). 10 There was a significant inverse correlation of zinc, copper, and magnesium levels with fasting (FPG) and postprandial plasma glucose (PPG), as well as glycated hemoglobin (HbA1c). This association was strongest for zinc in both groups (FPG: r −0.813 in group A and r −0.821 in group B, PPG: r = −0.763 in group A, and r = −0.835 in group B, HbA1c: r = −0.609 in group A and r = −0.520 in group B). 10
In a cross-sectional, observational study, Sánchez-Cruz et al 11 examined the frequency of low zinc levels among subjects with DFUs. Low zinc levels were seen in 70% of subjects with DFUs and 25% of DM subjects without DFUs (odds ratio [OR]: 5.2, 95% confidence interval [CI]: 2.139-12.65, P = 0.0004). 11 Subjects with lower zinc levels had higher body-mass index (P = 0.011). 11
Similarly, Larijani et al 12 included 39 T2DM subjects (19 with DFUs). They have shown significantly lower (P < 0.05) zinc levels among T2DM subjects with versus without DFUs. 12
Another study looked at the differences in dietary intake of macro- and micronutrients in elderly T2DM subjects with and without DFUs. 13 Group A included 79 elderly T2DM subjects with DFUs (mean age: 60.6 years) and group B 59 without DFUs (mean age: 55.0 years). 13 In group A, the mean daily intake (MDI) of micronutrients such as zinc, iron, folic acid, and carotene was lower than the recommended dietary allowance (RDA). 13
Leichter et al 14 examined the clinical features of 55 DM subjects referred for treatment of serious pedal infections. The mean serum zinc level was slightly below the normal range, but 62.4% of the DM subjects had low serum zinc concentrations. 14
Finally, Bolajokol et al 15 investigated micronutrient levels in T2DM subjects with DFUs and examined their effects on glycemic indices. Group A included 70 T2DM subjects with DFUs and group B 50 non-DM participants (controls) aged 40 to 60 years. The levels of vitamin C (3.7610.43 vs 5.57 ± 0.43 ptmol/L; P = 0.003), selenium (0.48 ± 0.01 vs 0.81 ± 0.04 srmol/L; P = 0.000), and vitamin E (19.57 ± 1.01 vs 25.57 ± 0.27 pLimol/L; P = 0.000) were significantly lower in group A. 15 Nonetheless, zinc and copper levels did not differ between the 2 groups. 15
DFUs and Zinc Administration
There is some preliminary evidence that zinc supplementation may improve DFUS healing (Table 2).16,17
Zinc Supplementation and DFUs.
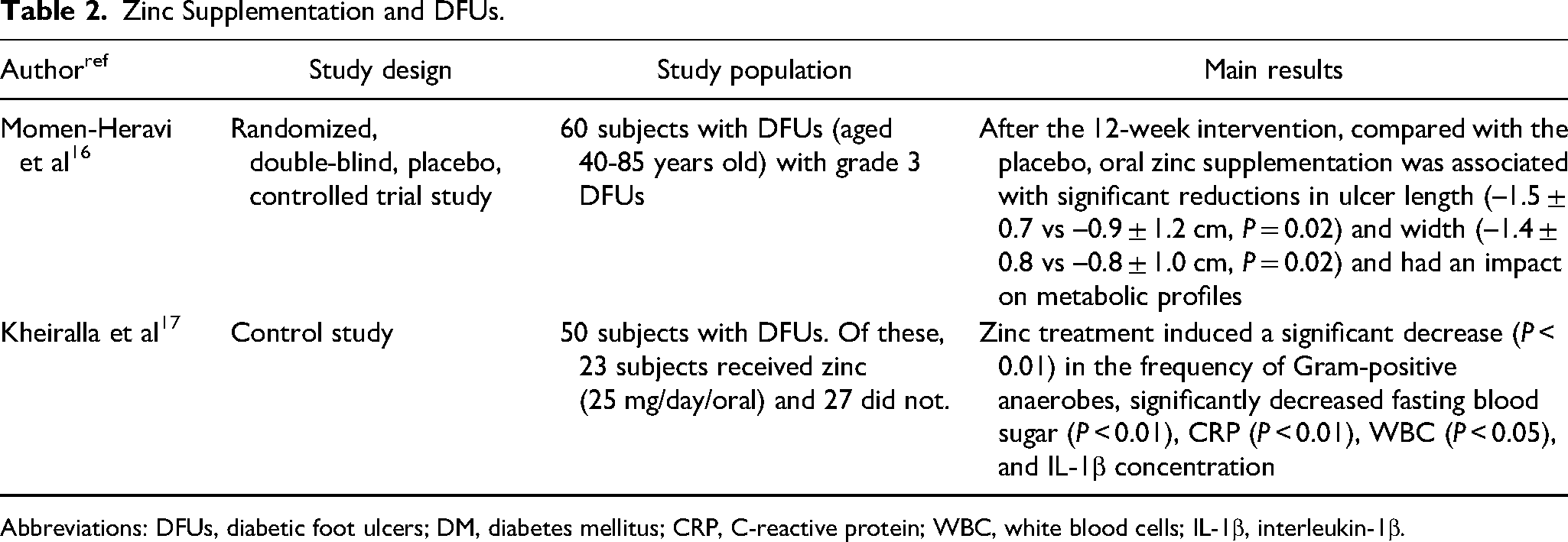
Abbreviations: DFUs, diabetic foot ulcers; DM, diabetes mellitus; CRP, C-reactive protein; WBC, white blood cells; IL-1β, interleukin-1β.
Momen-Heravi et al 16 investigated the effect of oral zinc supplementation on DFUs. They carried out a randomized, double-blind, placebo-controlled trial including 60 patients (aged 40-85 years) with grade 3 DFUs. These were randomized to 220 mg zinc sulfate supplements containing 50 mg elemental zinc (group A) or placebo (group B) daily for 12 weeks (30 participants in each group). 16 After 12-week oral administration, significant reductions in ulcer length (–1.5 ± 0.7 vs −0.9 ± 1.2 cm, P = 0.02) and width (–1.4 ± 0.8 vs −0.8 ± 1.0 cm, P = 0.02) were seen in group A versus B. Subjects in group A also exhibited improvements: increases in high-density lipoprotein-cholesterol (+ 4.1 ± 4.3 vs + 1.1 ± 5.1 mg/dL, P = 0.01), plasma total antioxidant capacity (+91.7 ± 213.9 vs −111.9 ± 188.7 mmol/L, P < 0.01), total glutathione (+68.1 ± 140.8 vs −35.0 ± 136.1 µmol/L, P = 0.006); decreases in high sensitivity C-reactive protein (–20.4 ± 24.6 vs −6.8 ± 21.3 µg/mL, P = 0.02) and plasma malondialdehyde concentrations (–0.6 ± 0.9 vs −0.2 ± 0.7 µmol/L, P = 0.03). 16 Other improvements in group A related fasting plasma glucose (–40.5 ± 71.0 vs −3.9 ± 48.5 mg/dL, P = 0.02), serum insulin concentration (–8.0 ± 15.4 vs + 1.1 ± 10.3 µIU/mL, P = 0.009), homeostasis model of assessment-estimated insulin resistance (–3.9 ± 7.1 vs + 0.8 ± 5.9, P = 0.007), quantitative insulin sensitivity check index (+ 0.01 ± 0.03 vs − 0.002 ± 0.02, P = 0.04) and HbA1c (– 0.5 ± 0.8 vs −0.1 ± 0.5%, P = 0.01). 16
Kheiralla et al 17 examined the bacteriological profile of DFUs and the effect of factors such as complement C3, interleukin-1β, and zinc treatment on them. They included 50 subjects with DFUs. 17 Of these, 23 subjects received zinc (25 mg/day/oral) and 27 did not. Zinc treatment induced a significant decrease (P < 0.01) only in the frequency of Gram-positive anaerobes, while it had no effect on Gram-positive and -negative aerobes and polymicrobial isolation rates. 17 In addition, it significantly decreased fasting blood sugar (P < 0.01), C-reactive protein (P < 0.01), white blood cell count (P < 0.05), and interleukin-1β concentration in the zinc-treated group as compared to the nontreated group, while it had no effects on complement C3 and other parameters. 17
Discussion
The main finding of this mini review is that low zinc levels are observed among patients with DFUs. Furthermore, there is preliminary evidence that zinc administration might yield beneficial results in terms of DFUs healing, as well as metabolic parameters.
However, there are some limitations. First, the number of patients was small. Moreover, most studies were single center and this could limit the generalizability of reported findings. Of note, the follow-up was not long. One final limitation may be inherent in the nature of this article as a mini review, but this is justified by the paucity of information.
Therefore, it is important that further studies concerning this issue will be conducted, with more participants, polycentric characteristics of the studies, and longer follow-up in order to evaluate the outcomes of its administration over a longer period of time. In addition, further studies to determine the optimal zinc dosage are imperative. Indeed, for the time being, it is impossible to provide even preliminary suggestions on dosage. Moreover, studies investigating the optimal synergistic combination of zinc, vitamins, and trace minerals, concerning amelioration of DFUs and DM complications should be conducted. It is therefore crucial for physicians to monitor their patients’ vitamin and trace mineral levels as they play an important role in the evolution of the health status of these people.
In conclusion, low zinc levels may be encountered among patients with DFUs. Additionally, oral administration of zinc supplements may contribute to the reduction of ulcer size and improved metabolic profile.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: N. Papanas has been an advisory board member of Astra-Zeneca, Boehringer Ingelheim, MSD, Novo Nordisk, Pfizer, Takeda, and TrigoCare International; has participated in sponsored studies by Astra-Zeneca, Eli-Lilly, GSK, MSD, Novo Nordisk, Novartis, and Sanofi-Aventis; has received honoraria as a speaker for Astra-Zeneca, Boehringer Ingelheim, Eli-Lilly, ELPEN, Galenica, MSD, Mylan, Novo Nordisk, Pfizer, Sanofi-Aventis, Takeda, and Vianex; and attended conferences sponsored by TrigoCare International, Eli-Lilly, Galenica, Novo Nordisk, Pfizer, and Sanofi-Aventis.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.