
Abstract
This study was designed to evaluate the efficiency of the combination of autologous platelet-rich plasma gel (APG) and Manuka honey gauze in the treatment of Stages 3–4 pressure injury of older adults. Patients were divided into four groups: Manuka honey gauze and APG (M + A), Manuka honey gauze (M), APG (A), and a control group (C). Different treatments were given, then wound bed coverage with granulation tissue, wound size reduction, and Pressure Ulcer Scale for Healing (PUSH) score were examined. Paraffin-embedded sections of wound tissues were analyzed and wound swab cultures were assessed. Kruskal–Wallis test and Mann–Whitney U test were performed in statistical analysis at a 5% significance level. A total of 42 patients were accepted. Significant increase of wound bed coverage with granulation tissue (51.24%, P = .004, Kruskal–Wallis test) and decrease of PUSH score (−5) were observed in the M + A group at the end of the observation (P = .032, Mann–Whitney U test). The hematoxylin–eosin staining of wound tissues showed that typical squamous epithelium was seen in wound bed of patient in M + A group. Manuka honey gauze and APG were proved to be superior treatments for pressure injury of old patient. Increase of granulation tissue coverage, reduction of PUSH score, and improved growth of epithelium were observed in M + A group. There was no side-effect, and the treatment would not cause infection.
Introduction
Pressure injury is a localized damage to the skin and underlying soft tissue, usually over a bony prominence or related to a medical or other device. 1 Annual treatment costs of pressure injury in the American are estimated at $9.1–$11.6 billion. 2 Prevalence of pressure injury among paralytic patients is 1.23% in 2016, China, which is even higher among old patients. 3 Stages 3–4 pressure injury is full-thickness skin and/or tissue loss. 1 Pressure injury healing is a dynamic process consisting of three sequential but overlapping stages: inflammation, proliferation and remodeling.4,5 The causes of delayed injury healing are relevant to the three stages. Blood artery insufficiency, biofilm formation and immunity dysfunction lead to poor conditions such as growth factor deficiency, lack of tissue scaffold for repairing, hampering the healing of wounds.6,7
Autologous platelet-rich plasma gel (APG) is derived from platelet-rich plasma (PRP). PRP is defined as a portion of the plasma fraction of autologous blood with a platelet concentration above baseline. 8 The components in APG include several growth factors like transforming growth factor-β to stabilize the tissue in wound, increase extracellular matrix synthesis, and stimulate new blood vessel formation, and ultimately lead to fibrous connective tissue and scar developments.9–13 PRP and APG are widely used in wound healing.12,14 The bioactivities of honey accelerate the healing process in wound.15–17 Acidity of honey increases the release of oxygen from hemoglobin, which goes against the activity of destructive proteases. High osmolarity of honey creates an outflow of lymph and makes a moisture environment to promote regeneration. 18 Honey has an antibacterial activity due to hydrogen peroxide, however, much of it is inactivated by the enzyme catalase existing in human bodies. Manuka honey, unlike others, contains the antimicrobial elements which can withstand the decomposition activity of wound exudate and still be active to inhibit the growth of bacteria. 17
The goal of this research is to evaluate the efficiency of the combination of APG and Manuka honey gauze in treatment of Stages 3–4 pressure injury of senile patients. We speculate that APG might build a scaffold for cell migration and fibrous tissue regeneration, and Manuka honey might provide a clean and moisture environment for wound repair. We combinate them together to evaluate the therapeutic effect, and through comparing with the existing conventional pressure injury treatment, we try to find a new treatment for pressure injury.
Patients and Methods
Patient and Public Involvement
A prospective, randomized controlled, open-labeled clinical trial was carried out in our Hospital from July 2018 to Jan 2019. The study was approved by the Ethics Committee of our Hospital.
The effectiveness of the treatment was assessed by wound bed coverage with granulation tissue, wound size reduction and Pressure Ulcer Scale for Healing (PUSH) score at the end of 8-week observation period. In addition, paraffin-embedded sections of wound tissue were observed under a microscope, and comparison was made between the treatments. Wound swab culture was assessed. Forty-two patients were registered in the trial in which their eligibility for inclusion was assessed before acceptance (Table 1). The diagnostic criteria of Stages 3–4 pressure injury is in accordance with the Pressure Injury Staging System. 1 Patients were divided into four groups with the random number table, namely Manuka honey gauze and APG (M + A), Manuka honey gauze (M), APG (A), and a control group (C) (Figure 1).
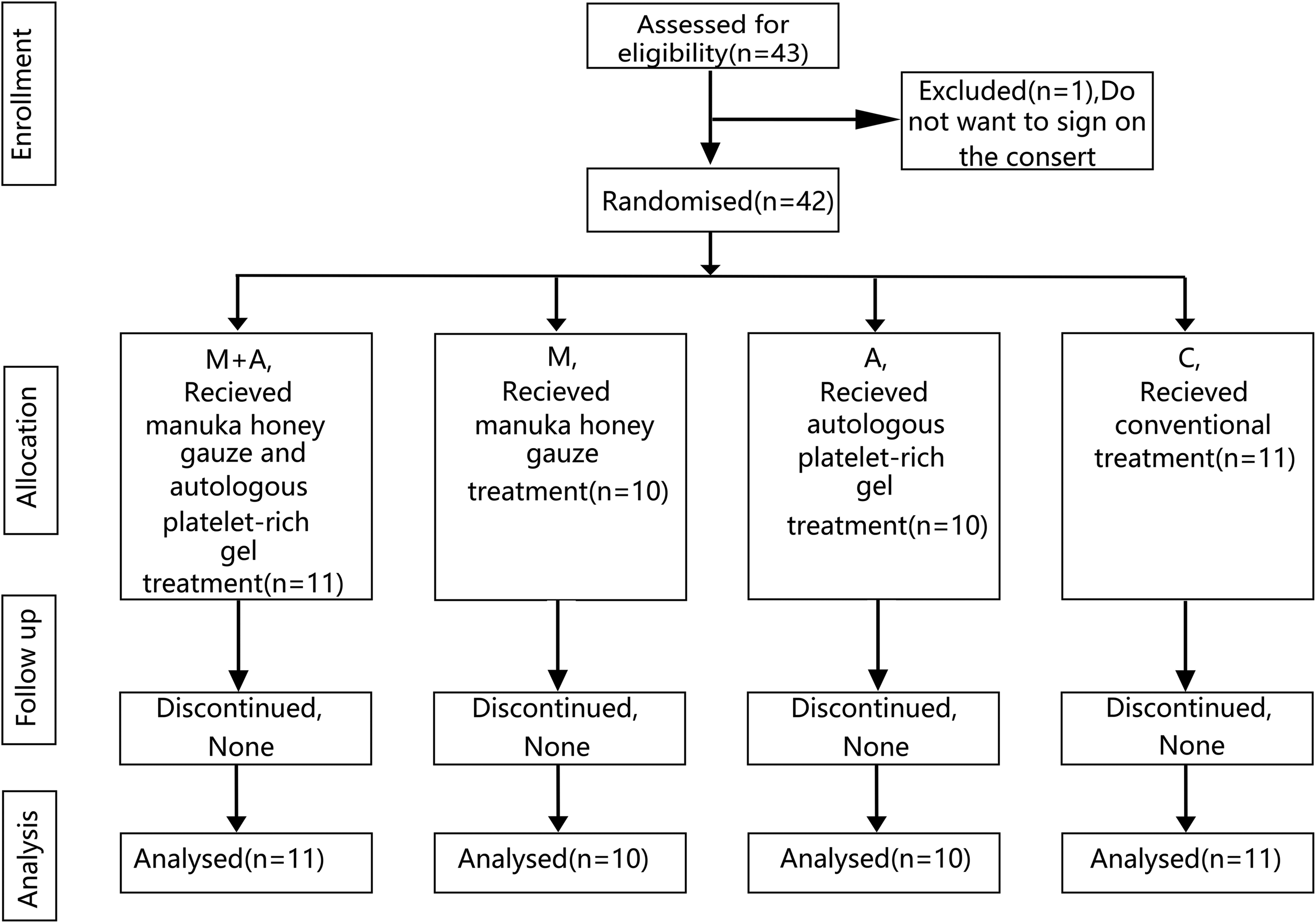
Consolidated Standards of Reporting Trials (CONSERT) flow diagram.
Inclusion and Exclusion Criteria.
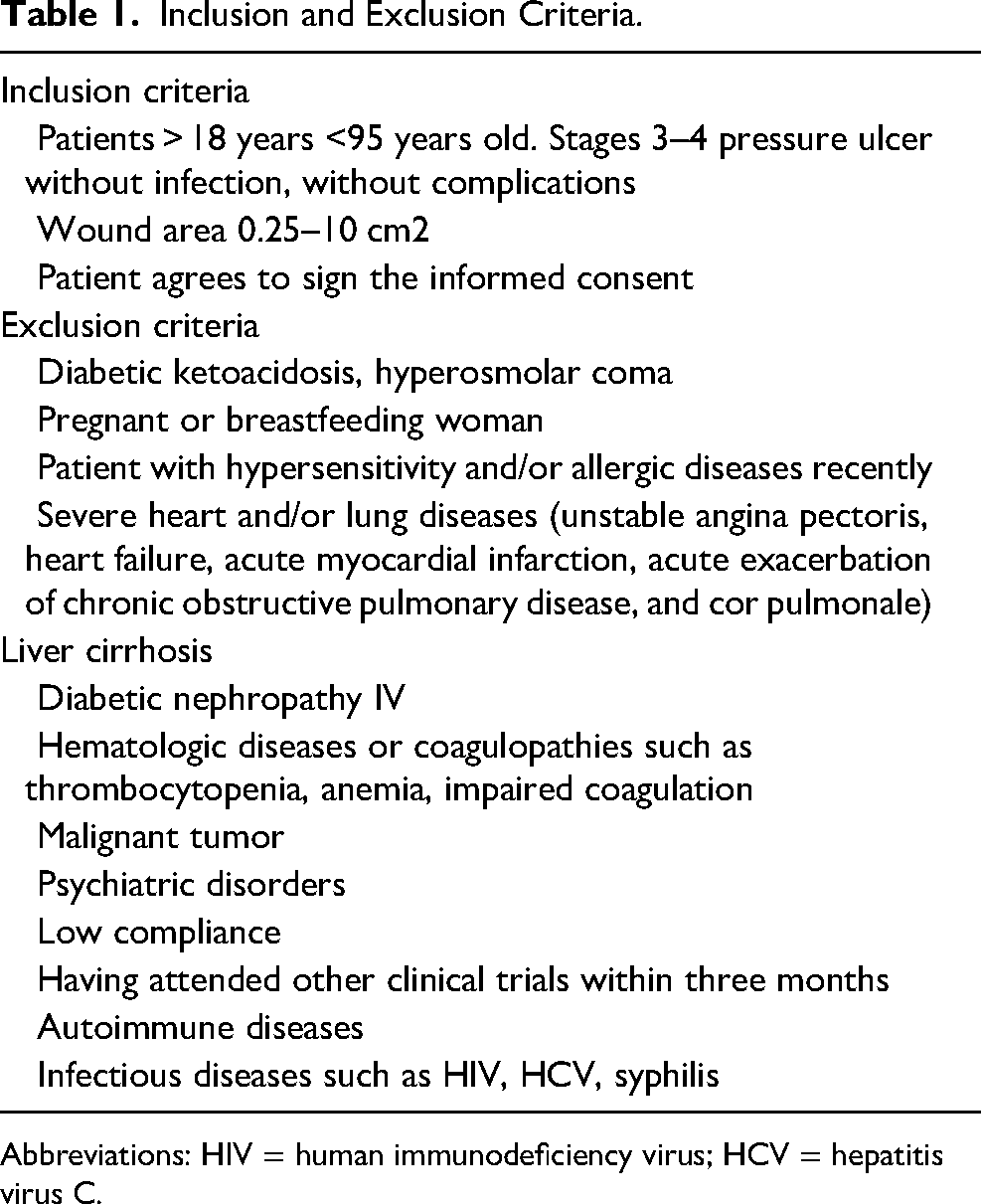
Abbreviations: HIV = human immunodeficiency virus; HCV = hepatitis virus C.
APG Preparation
Fifteen milliliter peripheral blood sample of patient or more was processed (the total volume depended on the area and depth of patients’ wound). PRP was prepared, using the previously described technique with modification. 19 Briefly, blood was centrifuged at 200×g, 4°C for 10 min. The blood was separated into three layers, the upper, the middle, and the lower layers. The upper and middle layers were moved to another tube, 2500×g, for 15 min. The upper plasma was discarded, lower 1/3 plasma and precipitation were mixed to be PRP. Platelets were counted under the platelet counter to make sure that the number of platelets was higher than 1000 × 106/ml, which was then activated with bovine thrombin (10:1, 1000 U/ml in 10% calcium chloride solution) to form a gel (Figure 2).
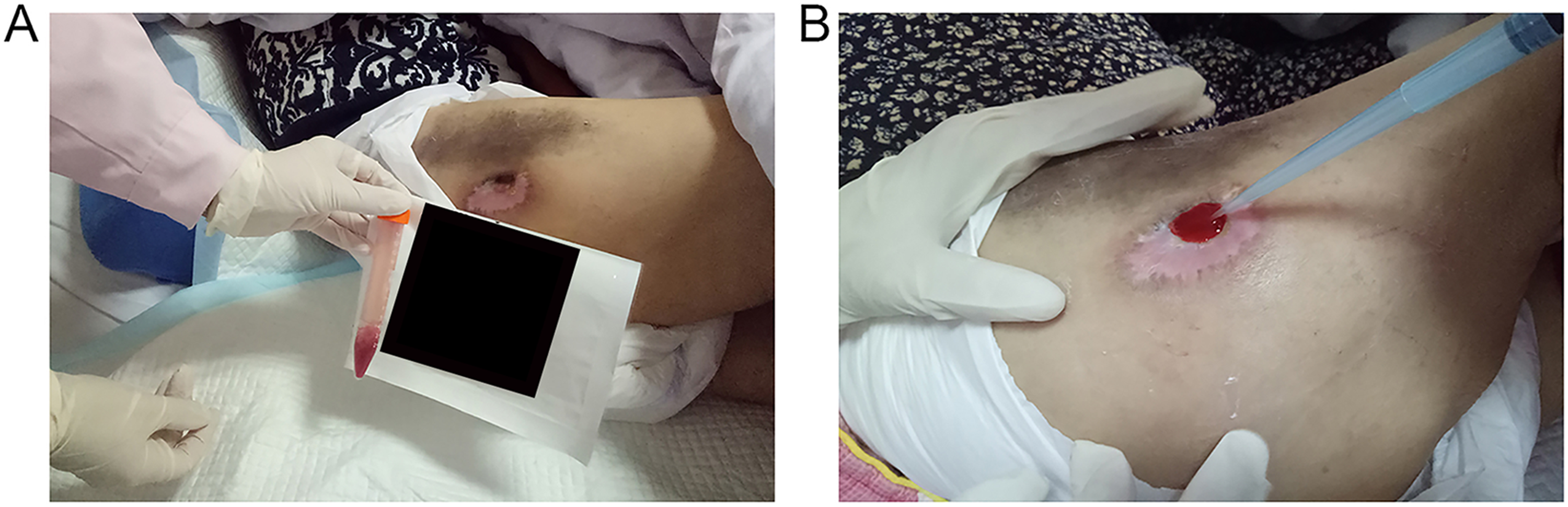
Pictures of the treatment.
Treatments of the Patients
For patients in M + A group, firstly, the inner space of wound was filled with PRP. Proper volume of bovine thrombin solution was then injected into PRP, then, the gel was formed. The surface of the gel was covered with Manuka honey gauze (Brightwake, Notts, UK) and a secondary dressing (Figure 2). In M group, wound was treated by Manuka honey gauze without APG. Patients were treated by APG in A group, contrarily. Treatment for patients in control group is conventional moist therapy. During the observation, the wounds were assessed and renewed every 3 days. A detailed study protocol is provided in Table 2. ImageJ (version 1.52v, NIH, USA) tool was used for the evaluation of the wound bed coverage with granulation tissue and wound size.
Study protocol.
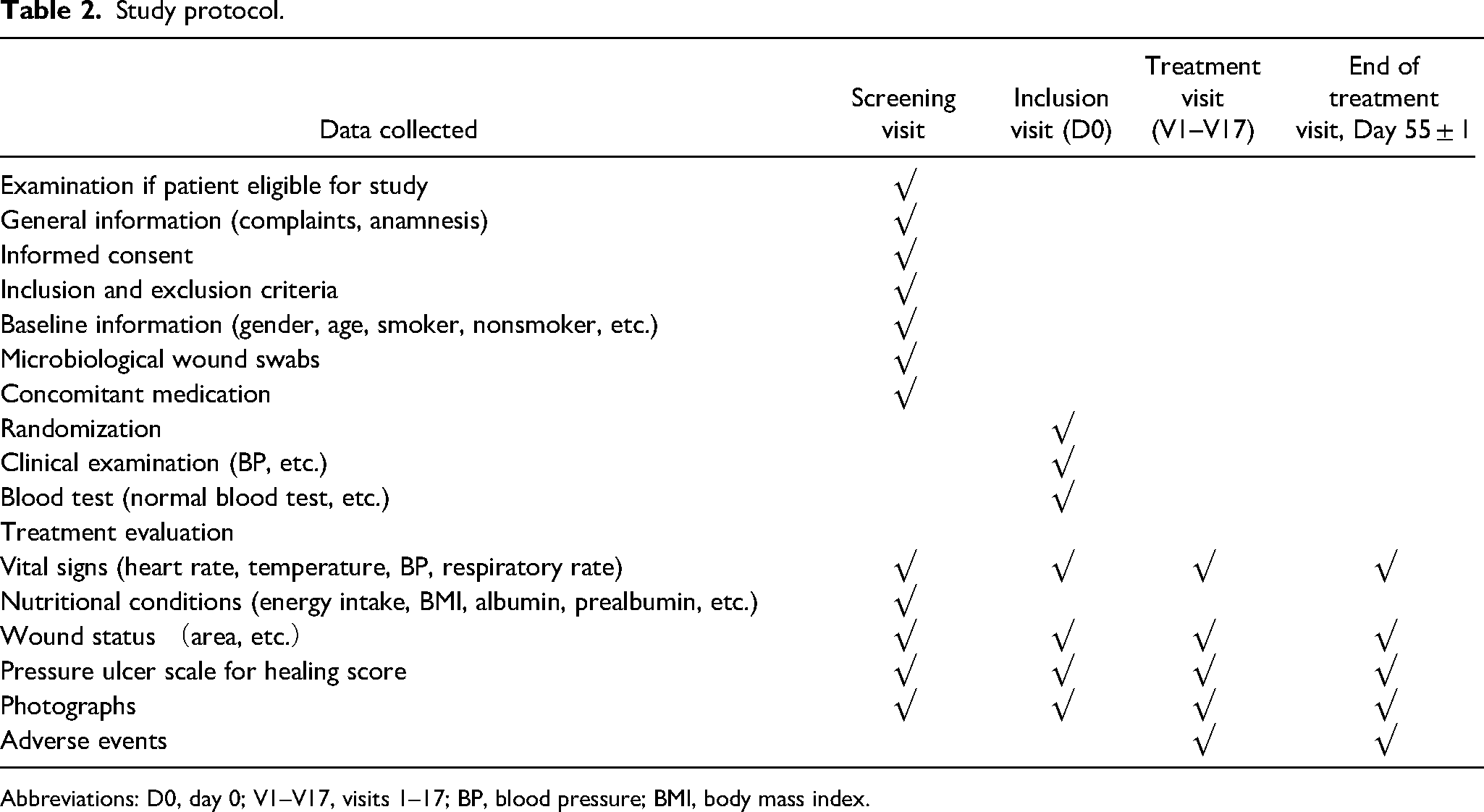
Abbreviations: D0, day 0; V1–V17, visits 1–17; BP, blood pressure; BMI, body mass index.
Statistical Analysis
All statistical analyses were performed at a 5% significance level (α = 0.05). Kruskal–Wallis test was used for analysis of wound bed coverage with granulation tissue. Mann–Whitney U test was processed for comparation of PUSH score reduction. IBM SPSS Statistics was used in analysis, version 22 (IBM Corp., NY, USA).
Results
A total of 42 patients were accepted in the study (11 in M + A, 10 in M, 10 in A, and 11 in C). Sociodemographic data and general health status were homogenous (Table 3). Evaluation of localization of the ulcer revealed that there was no statistically significant difference between different groups (Table 4).
General Information of the study patients.
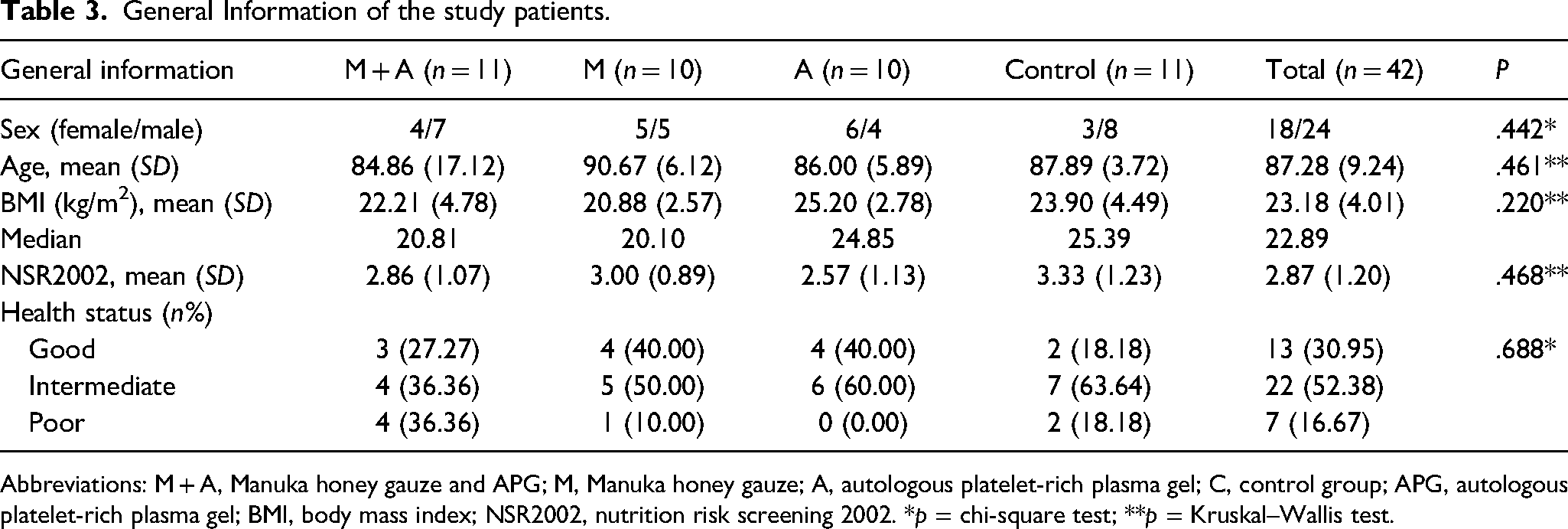
Abbreviations: M + A, Manuka honey gauze and APG; M, Manuka honey gauze; A, autologous platelet-rich plasma gel; C, control group; APG, autologous platelet-rich plasma gel; BMI, body mass index; NSR2002, nutrition risk screening 2002. *p = chi-square test; **p = Kruskal–Wallis test.
Localization of the wounds.
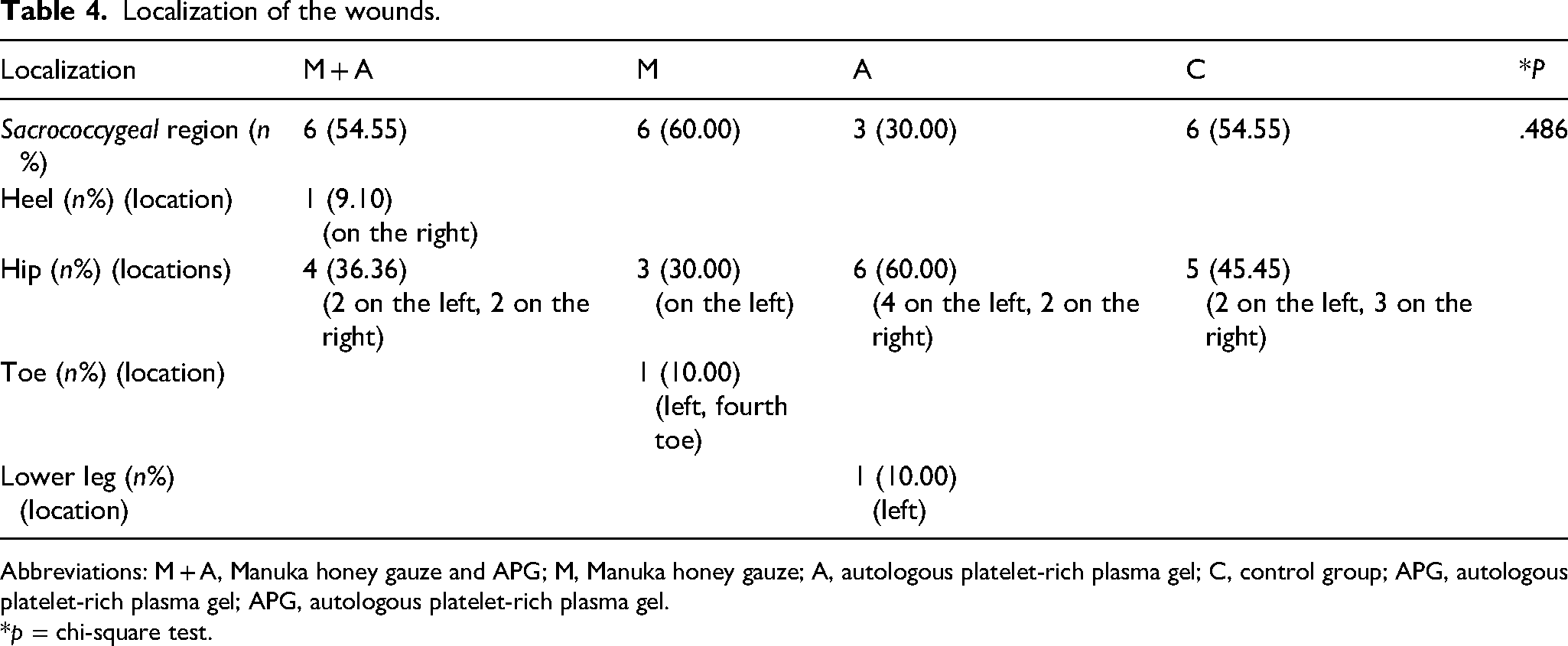
Abbreviations: M + A, Manuka honey gauze and APG; M, Manuka honey gauze; A, autologous platelet-rich plasma gel; C, control group; APG, autologous platelet-rich plasma gel; APG, autologous platelet-rich plasma gel.
*p = chi-square test.
Evaluations of Wound Bed Conditions by Granulation Tissue Coverage Rate, PUSH Score, and Wound Size Reduction
A significant difference of wound bed coverage with granulation tissue was observed between inclusion and end visits in M + A group (P = .004). A higher rate of granulation tissue in the M + A group was found (51.24%, Figure 3). There was a significant difference of the decrease of PUSH score (P = .032). The reduction of PUSH score was obvious in M + A group compared with other groups at the end (5 for M + A group, Figure 4). The mean wound size at the inclusion and end visit did not differ significantly. During the 8-week's observation, only one wound completely reepithelialized. The differences of wound size reduction were not statistically significant (Table 5). The treatment of Manuka honey gauze together with autologous platelet-rich gel was superior compared with the conventional or single method.
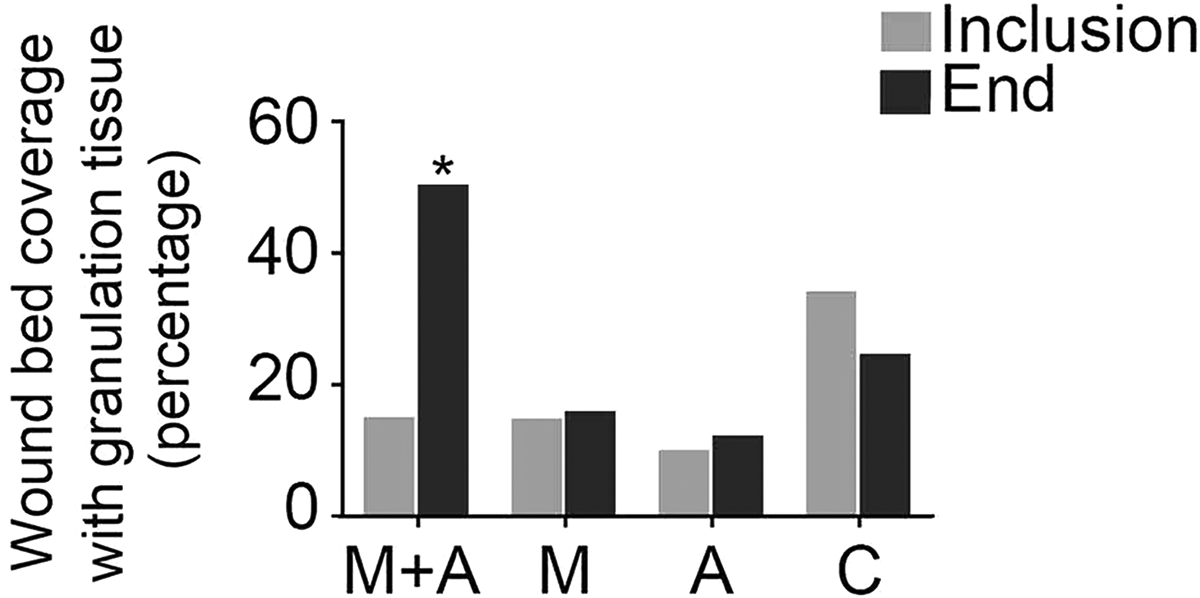
Wound bed coverage with granulation tissue wound bed coverage of granulation tissue was assessed. The rate increased notably in the M + A group at the end of the treatment compared with other groups (51.24%, *p = .004). Rate = area of granulation tissue/area of the wound × 100%.
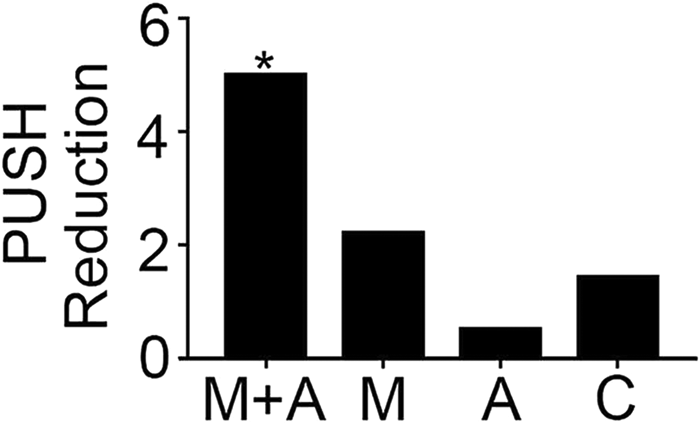
PUSH score reduction PUSH score reduction, significant difference was observed in M + A group (5, *p = .032).
Wound size reduction.
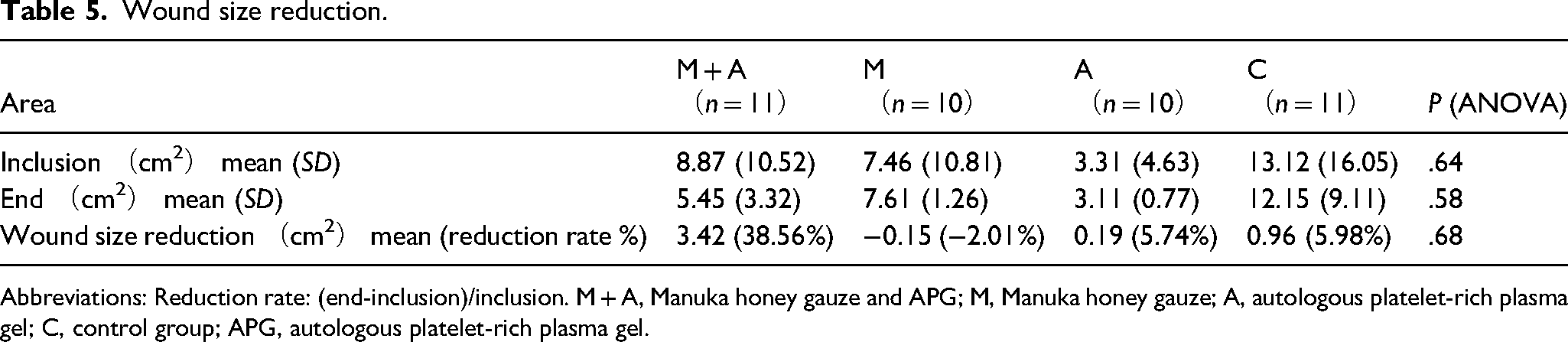
Abbreviations: Reduction rate: (end-inclusion)/inclusion. M + A, Manuka honey gauze and APG; M, Manuka honey gauze; A, autologous platelet-rich plasma gel; C, control group; APG, autologous platelet-rich plasma gel.
Pathological Assessment of the Wounds
The hematoxylin-eosin staining of wound bed tissues at the end showed that typical squamous epithelium was seen in wound bed of group M + A. Squamous epithelium was also seen in group M, however, a few neutrophils and lymphocytes were detected (Figure 5). The background of pathological section in group A contained dense and disorderly arranged collagen fibers. A few sporadic adipocytes, lymphocytes, and fibroblasts were observed on section of group A. A lot of lymphocytes and neutrophils were seen in C group, which was a sign of tissue necrosis. Pathological sections showed that typical squamous epithelium grew well on the wound bed of the M + A group.
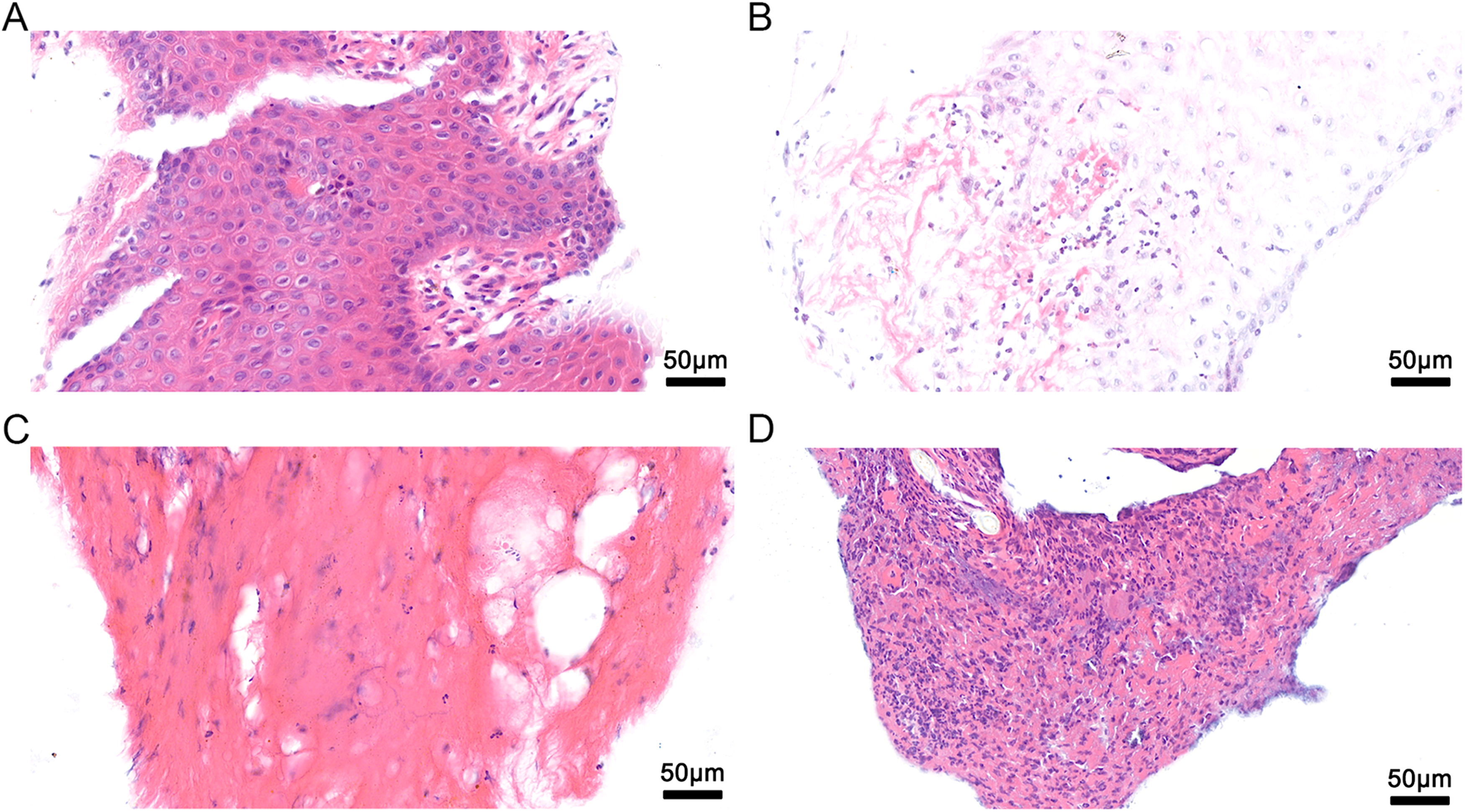
Pathological assessment of the wounds. (A) The hematoxylin–eosin staining of wound bed tissues at the end of observation showed that typical squamous epithelium was seen in wound bed of group M + A. (B) Squamous epithelium was also seen in group M, however, a few neutrophils and lymphocytes were detected locally. (C) The background of biological section in group A consisted of dense and disorderly arranged collagen fibers. There were a few sporadic adipocytes, lymphocytes and fibroblasts. (D) Tissue necrosis, with a large number of lymphocytes and neutrophils in section of D group.
Microbiological Wound Swab Cultures
Three kinds of bacteria were found in wounds before the treatment, Methicillin-resistant Staphylococcus epidermidis, Methicillin-resistant Staphylococcus aureus, and Proteus mirabilis. Antibiotics were used according to the antimicrobial susceptibility test before the treatment to make sure there was no infection in the wound. Only one case of positive result of wound exudate culture was seen during the observation in control group, in which Corynebacterium striatum was found (Table 6). However, there was no obvious sign of wound infection, and no adverse event, too. Treatments of Manuka honey gauze or APG or both were considered to be safe.
Microbiological evaluation of the wounds.
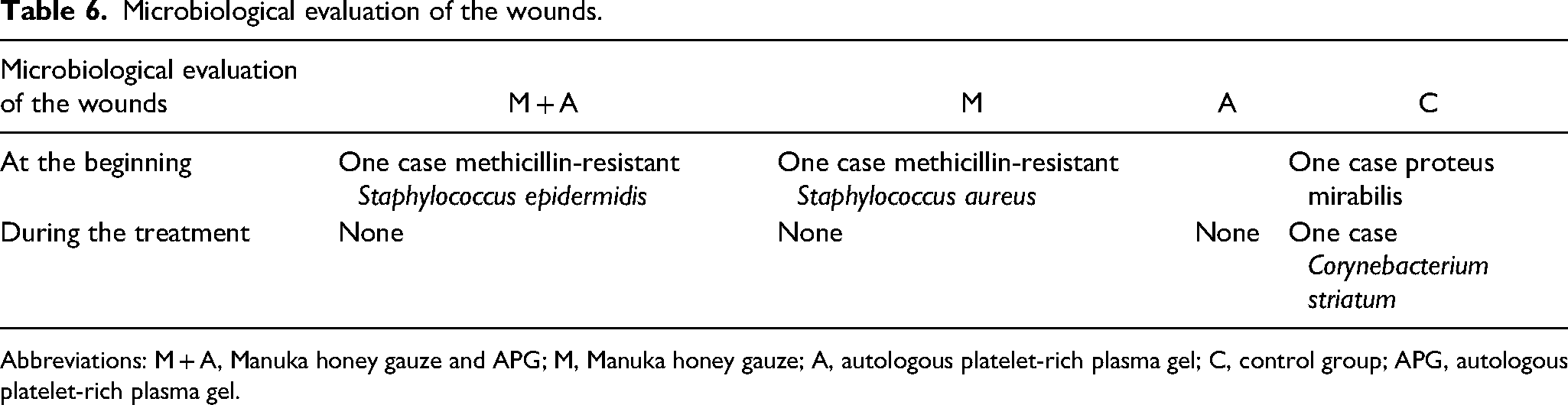
Abbreviations: M + A, Manuka honey gauze and APG; M, Manuka honey gauze; A, autologous platelet-rich plasma gel; C, control group; APG, autologous platelet-rich plasma gel.
Discussion
In this study, we combined APG and Manuka honey gauze together to treat Stages 3–4 pressure injury. Increase of granulation tissue coverage, reduction of PUSH score and improved growth of epithelium were observed, which shed light on a promising future of the use of the combination.
In Geriatric Ward, pressure injury is usually occurred on disabled old patients. Pressure injury is intractable since akinetic patients lying in bed are always suffering from diabetes mellitus, atherosclerosis, malnutrition, anemia, etc. These diseases are causes of a hostile environment contributing to poor wound healing which is influenced by four aspects, angiogenesis, relief of oxidative stress injury, inhibition of bacteria reproduction, and modulation of immune reaction.20,21 Both Manuka honey and APG could regulate partial of the four aspects.
There is a unique content named methyl glyoxal in Manuka honey of which the antimicrobial activity is not inhibited by catalase, whereas the peroxide activity is.22,23 Manuka honey is effective against organisms. The evidence showing Manuka honey can reduce bioburden is well established.24–27 It is reported that Manuka honey protects RAW 264.7 macrophages against Lipopolysaccharides (LPS)-induced oxidative stress through improving antioxidant enzyme expressions and activities. Pretreatment with Manuka honey decreases LPS-induced overactivation of Nuclear Factor kappa-B (NF-κB), inducible Nitric Oxide Synthase (iNOS), Tumor Necrosis Factor alfa (TNF-α), and Interleukin 1 beta (IL-1β), meanwhile, the damage stimulated by LPS is also alleviated by Manuka honey.15,16 An increase in angiogenesis is seen in wounds treated with Manuka honey gel, followed by enhanced fibrosis and collagen organization and improved epithelialization. 28 According to the research aforementioned, Manuka honey helps to develop a healthier bed of granulation tissue. Similar trends are observed in our study, too.
The components of APG include transforming growth factor-β, platelet-derived growth factor, insulin-like growth factor, vascular endothelial growth factor, epidermal growth factor, and fibroblast growth factor-2. Vascular endothelial growth factor and fibroblast growth factor-2 stimulate the formation of new blood vessels. Platelets are able to generate antimicrobial oxygen metabolites, including superoxide, hydrogen peroxide, and hydroxyl free radicals.9–11 Therefore, once PRP is activated, it develops a three-dimensional network containing lots of growth factors and active antimicrobial proteins, which is a favorable seeding matrix to construct tissues. 29 APG is proven to be effective in modulation of immune-reaction as it contains platelet-derived epidermal growth factor, which is known to be chemotactic for macrophages and fibroblasts. Macrophages positively influence wound angiogenesis by driving resolution of antiangiogenic wound neutrophils, orchestrates vessel sprouting and regression. 30
In our study, the observation lasted only eight weeks since the health condition of disabled elders was unstable. The old patients were usually suffered from respiratory infection, reflux-related recurrent aspiration pneumonia, fever, vertigo, lacunar infarction, et al A long-term observation increased the incidence of concomitant diseases, which hampered wound healing as an interference factor. Pneumonia or other concomitant diseases would affect general health status and local environment of wound bed, and thus the healing of pressure injury would be prolonged. As a result, the observation time was limited to eight weeks. According to studies in vitro, both Manuka honey and APG are effective treatments in wound healing. However, in our study, the significant improvement of the pressure injury was only observed in patients treated with the combination of these two methods. On one hand, in vitro observation may oversimplify the in vivo situation, on the other hand, patients in our study were senile with poor vessel condition, weak self-repair ability, immunological disorder, poor antiinfection ability, and immobility. These hampered the recovery of the pressure injury.
There was no significant difference in wound size in a short observation time. The explanation was that if the wound was large and deep, leaving comparatively large cavity, the growth of epithelium would be hampered. Generally, good trend of epithelium growth depends on remodeling and flattening of the wound bed. As a result, the wound size would not be reduced obviously if the cavity was still large.
Manuka honey and autologous platelet-rich gel were proved to be superior treatments for pressure injury of old patients while the combination of these methods had not been used or reported. There was no side-effect, and the treatment would not cause infection.
The economic burden of pressure injury is heavy now, so cheap and effective treatments are in urgent need. The combination of Manuka honey gauze and APG is not only effective in promoting wound recovery, but also cheap and available for the average price for each treatment in this trial is 7–15 bucks. In the future, a larger scale of clinical study will be necessary to further confirm the results of our study and explore the mechanisms involved.
Footnotes
Authors’ Contributions
Lulu Xu, Xinmeng Wang and Yongmei Wu designed the experiment and protocol, collected patients' data and dressed the wounds. Lulu Xu analysed the data and wrote the manuscript. Zhen Zhang performed cultures on wounds. Xiafei Li and Jie zhang gave the financial support during the entire trial and directed the trial.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This prospective, randomized controlled, open-labeled clinical trial was carried out in Chongqing General Hospital from July 2018 to Jan 2019 (registration number: ChiCTR1800018441). The study was approved by the Ethics Committee of Chongqing General Hospital (s2017-028).
Funding
This work was supported by the Medical Technology Innovation Fund Project of Chongqing General Hospital (grant number Y2017MSXM01). The Joint Medical Research Project of Science and Technology Committee and Health and Family Planning Commission of Chongqing (grant number 2020FYYX037). Chongqing Yu Zhong District Science and Technology Plan Project (grant number 20170416) and Chongqing Natural Science Foundation (grant number cstc2021jcyj-msxmX1129).