
Abstract
Plasminogen (Pg) is currently considered a master regulator of wound healing, but the molecular mechanisms of its efficacy in improving impaired closure of chronic skin ulcers in type 2 diabetes patients remain unclear. Here, we investigated wound healing effects of autologous plasma-derived Pg in diabetes patients with chronic foot ulcers and evaluated Pg-induced changes in levels of key protein markers related to wound repair. Type 2 diabetes patients with chronic wounds of lower extremities were included in the study and received topical applications of Pg in a dose of 1.0 mg/mL every 2 days during 20 days, in addition to the standard wound management treatment. Patients treated only according to conventional protocol served as a control. Wound closure rates were monitored by digital planimetry of wound areas. Plasminogen supplementary treatment significantly accelerated relative wound closure as compared with diabetes patients from the control group (24 ± 4 days vs 120 ± 17 days, respectively, P < .01). As shown by Western blot, Pg application reduced expression of protein regulators of hypoxia events, angiogenesis, and autophagy such as hypoxia-inducible factor-1α (by 6.3-folds, P < .01), angiostatins (by 2.5-folds, P < .05), and autophagy marker LC3-II/LC3-I (by 8.6-folds, P < .05), while increasing vascular endothelial growth factor level by 1.9-folds (P < .05). Gelatin zymography showed that Pg-supplemented therapy decreased activity of matrix metalloproteinase-9 (MMP-9) by 3.5-folds at the end of treatment period (P < .01). We report here for the first time that topically applied plasma-derived Pg has a pronounced beneficial effect in promoting foot ulcer healing in patients with type 2 diabetes through preventing hypoxia-induced signaling, reducing autophagy flux, diminishing excessive MMP activity, and enhancing angiogenesis.
Introduction
Diabetic skin ulcers represent a real “silent epidemic” inside the world population, for which current remedies are limited or nonexistent. The majority of cutaneous wounds related to diabetes evolves toward chronicity, particularly in the lower limbs. Syndrome of diabetic foot is considered as one of the most adverse complications of diabetes mellitus, which leads to 84% of foot amputations. 1 Problems in diabetic foot treatment are linked with complexity of underlying pathological processes, which remain poorly understood. In the past years, there has been renewed interest in the understanding of impaired healing in chronic wounds and their treatment. There is a progress in testing and applying novel molecular and cellular treatments of chronic wounds based on the application of tissue engineering, stem cells, growth factors, enzymes, or their inhibitors. 2 However, the most effective treatment of diabetic chronic wounds remains undecided in spite of some advances.
Wound healing is a very complex biological process, involving highly organized sequence of 4 overlapping phases (hemostasis, inflammation, cell proliferation/migration, and tissue remodeling), which are spatially and temporally synchronized. As oppose to acute wounds, healing of chronic cutaneous lesions stops at one of these steps, usually at the inflammatory phase. 3 Proteases are essential for each phase of wound healing, playing special roles in degradation of extracellular matrix (ECM), tissue remodeling, cell migration, and inflammation. Any disturbances of proteolytic system functioning in injured cutaneous tissue may result in impaired dermal wound healing. 4 The current evidence has identified plasminogen (Pg) as one of the key participants of wound healing process. Plasminogen, a 92-kDa glycoprotein, is produced in the liver and circulated in plasma in the concentration of 1.8 to 2.2 µM (160-200 mg/L) as a catalytically nonactive zymogen of plasmin, a central protease of fibrinolytic system. 5 In addition to providing fibrin clearance, Pg has recently been indicated to regulate both initiation and resolution of inflammatory phase and to be involved in tissue remodeling during physiological wound healing process. 6 Plasminogen has been shown to act as a pleiotropic signaling molecule by regulating and coordinating activity of monocytes/macrophages, keratinocytes, platelets, and other cells, which are involved in wound repair. Current literature indicates that deficit or functional insufficient of Pg or its physiological activators may cause delay of healing.7–9 To emphasize the special role of Pg in reparative processes, this protein has been referred to as a “master regulator” of wound healing. 10
Although solid evidence for Pg necessity for successful wound healing has been extensively accumulated during various animal studies, an information about Pg as a suitable drug candidate for the treatment of wounds in patients with poor healing, especially in persons who suffer from diabetic foot ulcers, is still lacking. Therefore, for successful translation of preclinical data, the clinical relevance of abovementioned promising results is essential. In order to fill this gap, we organized the study, which was aimed at investigating for the first time to whether topical application of autologous plasma-derived Pg may improve healing of chronic foot ulcers in patients with type 2 diabetes mellitus. To elucidate putative molecular mechanisms of Pg-based intervention on wound healing, we evaluated effects of Pg application on tissue expression on the key protein markers of hypoxia, tissue remodeling, angiogenesis, and autophagy.
Materials and Methods
Plasminogen Isolation
Native Glu-Pg was isolated and purified from fresh citrated patient's plasma obtained once before onset of the treatment (total volume of plasma 50-60 mL from each patient). Plasma was divided to several aliquots of 20 to 25 mL each, which were loaded on 40 cm3 lysine-sepharose column (GE Healthcare, Amersham Biosciences) for affine chromatography, described earlier. 11
Individually prepared Pg had 95% to 99% purity as judged by SDS-PAGE (Figure 1). Isolated Pg did not display spontaneous proteolytic activity as assessed spectrophotometrically with the use of specific chromogenic substrate S-2251. Plasminogen preparations were dialyzed several times against phosphate-buffered saline, concentrated, additionally sterilized by ultrafiltration through the pressure-driven membrane, pooled, adjusted to 1.0 mg/mL by sterile buffered saline, aliquoted into plastic microtubes, and stored at −20 °C before use.
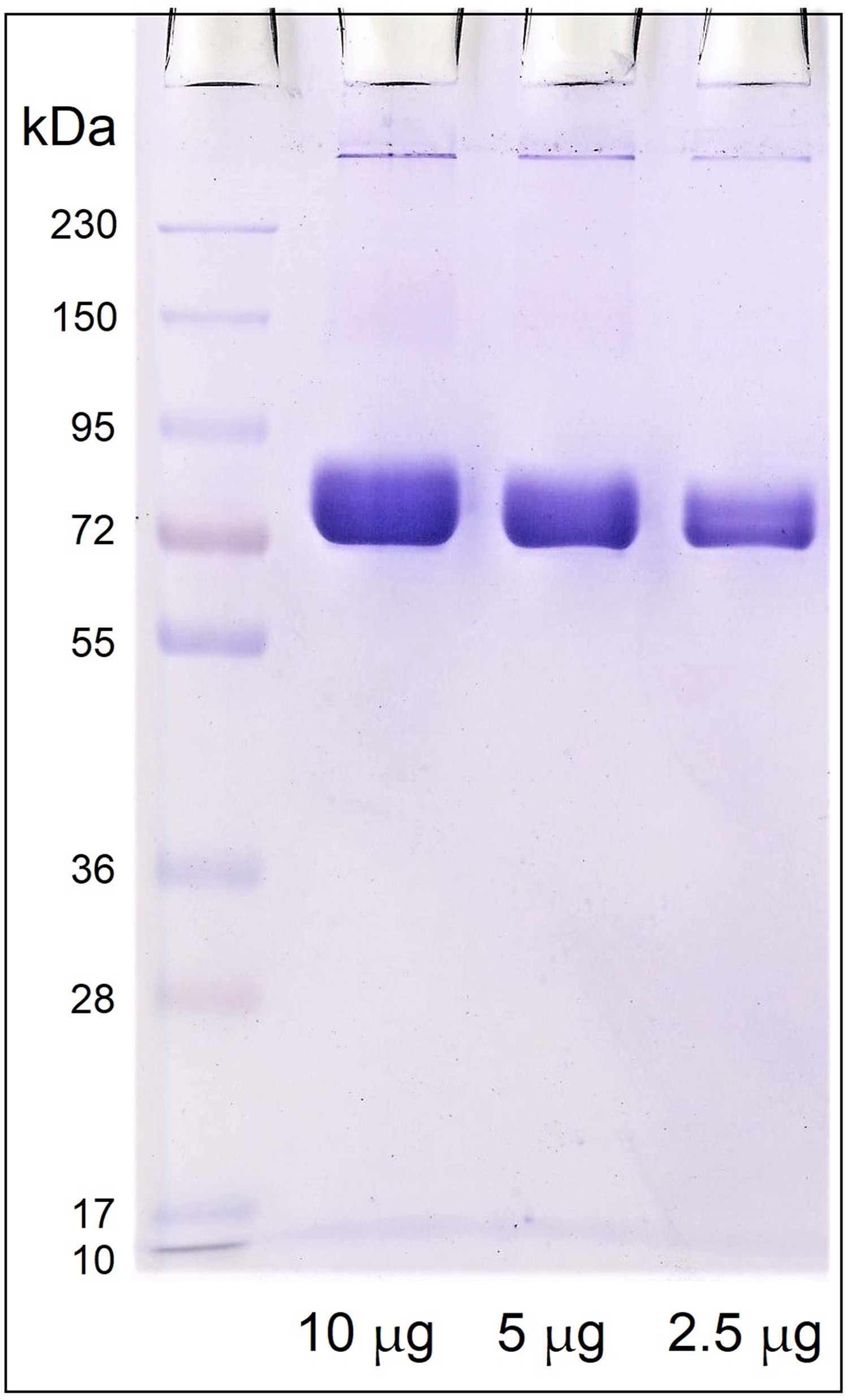
SDS-PAGE electrophoregram of plasminogen isolated from patient's plasma by affine chromatography on Lysine-Sepharose.
Patients
Forty-five patients with type 2 diabetes between the ages of 48 to 81 years with chronic wounds of lower extremities, which obtained stationary treatment, were included in the study. All wounds had failed to heal at least 6 weeks before the treatment initiation. PEDIS (
The patients willing to participate in the study and complying with the criteria signed an informed consent form. The enrolled patients were divided into 2 groups by simple randomization, there were no significant differences in the general demographic or clinical variables between participants (Table 1). We used a simple approach to randomize the groups because patients, treatment providers, or data collectors were not blinded due to the obvious nature of the intervention. No changes were made with respect to study methods or eligibility criteria after commencement of the treatment.
Demographic and Clinical Characteristics of the Patients.
Abbreviation: Pg, plasminogen.
Slightly higher percentage of recruited men into the Group I was due to a difference between male and female participants in willing to consent to alternative treatment. Study was started on November 1, 2022, and finished on October 30, 2023.
Local treatment of cutaneous wounds in patients from both groups was prescribed in accordance with standard protocols, which included the use of antiseptic option (chlorhexidine 0.05%, povidone-iodine, betadine 10%), water-soluble ointments, and regeneration stimulators such as methyluracil, hydrocolloid, and absorbent dressings (Hartmann, Mepilex). During the whole treatment period, all hospitalized patients obtained glucose-lowering preparations. In the studied group (Group I, n = 20), autologous Pg was locally applied on the wounded area as a solution in a dose of 1.0 mg/mL in sterile buffered saline every 2 days during 20 days (10 applications in total), in addition to the standard wound management procedures and the use of prescribed medications. Patients from control group (Group II, n = 25) were treated in accordance with the standard treatment protocol.
Tissue specimens from acute wounds (n = 5) were taken in individuals with normoglycemia after plastic surgery, and then were used in the measurements of matrix metalloproteinase (MMP) activity by zymography assay as a negative control.
Wound Planimetry
Digital planimetry was used in wound area measurement and therapy assessment. Computerized planimetry is a currently available method for calculating wound surface area, which is more precise and trustworthy for approximating the wound size and fairly simple to use in comparison with a traditional ruler method.
13
The wound is photographed with a ruler or a marker of known dimensions placed at the skin near the wound edge, and the image is transferred to a smartphone and open in planimetry software Imito Wound 2.0.0.17 (ImitoAG, https://imito.io/en/imitowound) (Figure 2). The ruler or marker is used for calibration of linear dimensions at the image. Wound size was expressed in cm2. The wound closure rate as changes in relative wound sizes was calculated using the formula
14
:
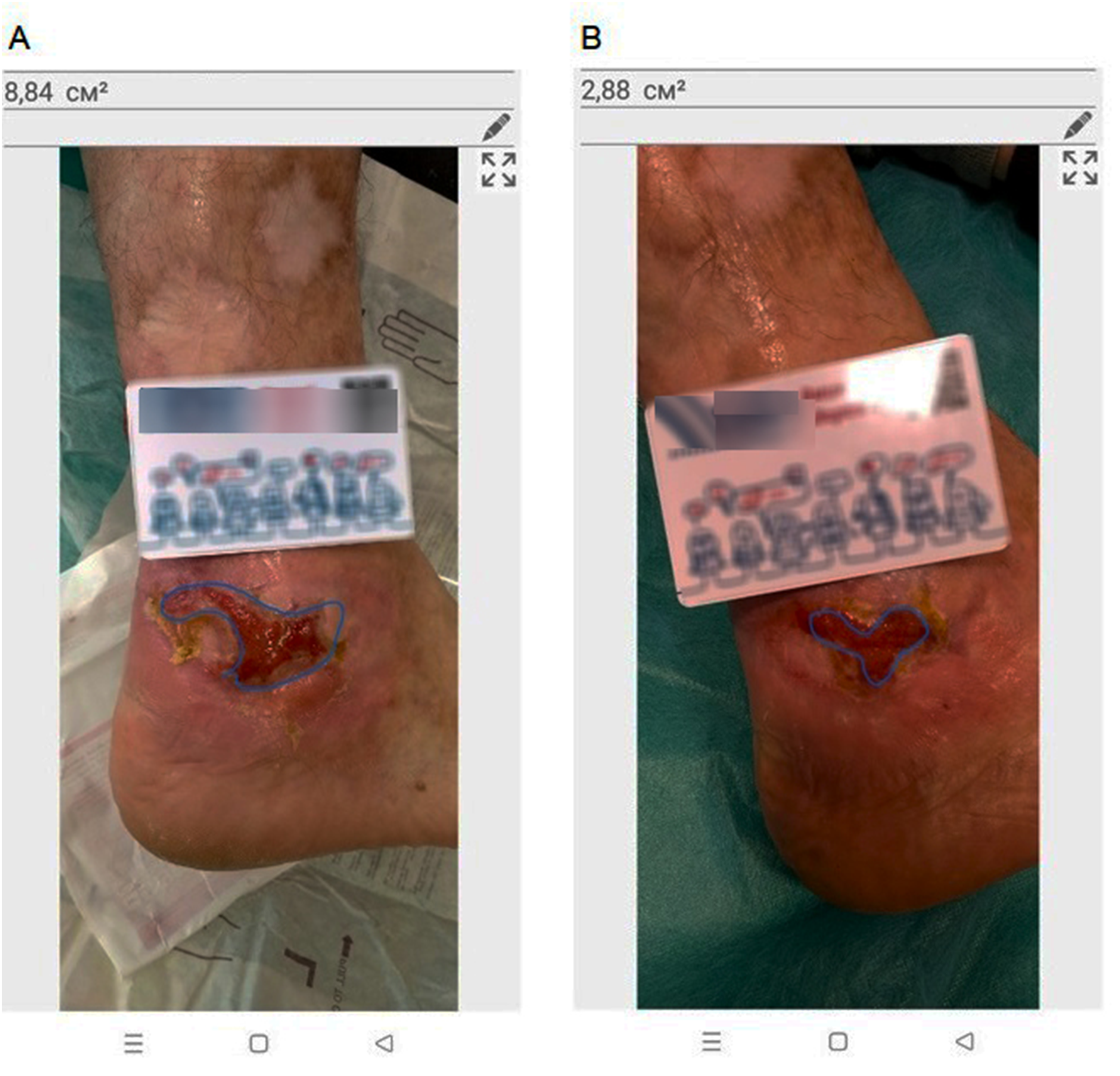
Photos of chronic skin lesion with the area measurement using the Imito AG application (smartphone print screens, an example). The wound margins are traced by The Examiner to determine the surface area. The software calculates the area by counting the pixels of the picture after it has been scaled with a marker placed in the same plane as the lesion (A—a photo made on February 6, 2022; B - A—a photo made on February 23 2022).
Tissue Sample Preparation
Dermal bioptates from the wound bed were collected from the patients before the first Pg application (0 day) and on the 18th day of the ongoing treatment period. Each tissue specimen consisted of the skin layers cutis and subcutis. Immediately after collection, all bioptates were stored at −80 °C until analyzed.
Protein samples of tissue specimens for western blots were prepared by grinding in liquid nitrogen and homogenization in ice-cold 50 mM Tris-HCl buffer (pH 7.4), additionally containing 150 mM NaCl, 0.1% SDS, 1.0% Triton X-100, and supplemented with proteases/phosphatases inhibitor cocktail (PierceTM Protease and Phosphatase Inhibitor, ThermoScientific). Protein extracts for MMP assay were prepared with the use of the same lysed buffer, which did not contain enzyme inhibitors. Tissue/buffer ratio was taken equal 1:5 (m/v). After homogenization steps, samples were sonicated for 60 s by ultrasonic disintegrator Sartorius (Labsonic® M) and centrifuged at 16 000 g for 45 min at 4 °C. The total protein concentration in each supernatant was determined spectrophotometrically by Stoscheck method. 15 The samples were diluted 1:1 in Laemmli Sample Buffer, frozen and stored at −80 °C before analysis.
Western Blot Analysis
The levels of regulatory proteins related to reparative processes and wound healing such as hypoxia-inducible factor-1α (HIF-1α), vascular endothelial growth factor (VEGF), angiostatins, and autophagy marker LC3 were measured by western blot. Samples were separated electrophoretically in 10% SDS-PAGE (100 µg protein per lane). Proteins were transferred from gel onto 0.45 ± 0.2 µm pore-size nitrocellulose membranes (Amersham Biosciences) by electroblot. The membranes were blocked in 5% nonfat skim milk solution (ApexTM Bioresearch Products) for 90 min at 37 °C. After blocking, the blots were probed with the primary antibodies against β-actin as a loading control (Invitrogen, no. MA5-15739), HIF-1α (Sigma Aldrich, no. HPA001275), VEGF (Invitrogen, no. MA5-12184), LC3 (Sigma Aldrich, no. L8918), or angiostatins (produced as described elsewhere 16 ) at 4 °C overnight. The membranes were washed in phosphate-buffered saline (pH 7.4), containing 0.05% Triton X-100 (PBST), and incubated with the appropriate antispecies secondary horseradish peroxidase (HRP)-conjugated antibodies (goat antirabbit or antimouse IgG, Invitrogen, cat. nos. G-21234 and 31430, respectively) for 90 min at 37 °C. After washing in PBST, the membranes were incubated with HRP substrate and exposed on x-ray film (Konica Minolta) by enhanced chemiluminescence technique. Signals were visualized, digitized, and analyzed using TL120 software (TotalLab Ltd). Molecular weights were determined using standard prestained transblot molecular weight markers (PageRuler, cat. no. 26616, Fermentas). Protein levels were expressed in arbitrary units after correction for β-actin.
Gelatin Zymography
Matrix metalloproteinase-9 activity was evaluated by gelatin zymography in bioptates from the cutaneous lesions to estimate effects of Pg treatment of diabetic wounds and compared that with MMP-9 activity in bioptates from acute wounds. The gelatinolytic activities were analyzed by separating proteins (50 µg/lane) in 8% polyacrylamide copolymerized with gelatin (5 mg/mL), as described earlier. 17 Briefly, after denaturing electrophoresis, the gels were washed twice for 30 min in cold 2.5% (v/v) Triton X-100 to remove SDS, and then 5 times for 5 min in cold bidistilled water. After washing, gels were incubated overnight at 37 °C in developing buffer (50 mM tris-HCl, pH 7.6, containing 0.15 M NaCl, 5 mM CaCl2, 1 mM ZnCl2, and 0.02% Tween-20). Zymograms were stained with 0.15% Coomassie Brilliant Blue R-250 (Merck Millipore) solution in 30% methanol and 10% acetic acid and destained in the same solution without Coomassie Blue. The final gel had a uniform blue background except in those regions to which MMPs had migrated and cleaved the substrate. The gelatinolytic activities were identified as transparent bands against the background of Coomassie Blue-stained gelatin. Resulting MMP bands were visualized and quantified densitometrically.
Statistical Analysis
Kaplan-Meier curves were constructed for all patients receiving Pg-based treatment and for those receiving standard treatment, using Wilcoxon statistics to test significant difference between groups. To analyze data of western blots and zymography, Mann-Whitney U test was used to evaluate differences between mean parameters. All variables were expressed as mean ± standard error of mean. For all tests, P < .05 was considered statistically significant. “OriginPro” software (major version 9.0 SR2 Pro English) was used to perform all statistical calculations.
Results
Plasminogen Topical Application Accelerates Diabetic Chronic Wound Closure
Continuous monitoring of a wound size by digital planimetry revealed that Pg local treatment improved healing and significantly accelerated wound healing rate as compared with those of patients treated according to standardized protocols (Figure 3). In average, complete closure of Pg-untreated wounds (control group) was achieved during 120 ± 17 days, while wound closure after Pg topical application was seen at 24 ± 4 days (P < .01). Photo collage depicted in Figure 4 exemplifies wound healing dynamics during local Pg treatment.
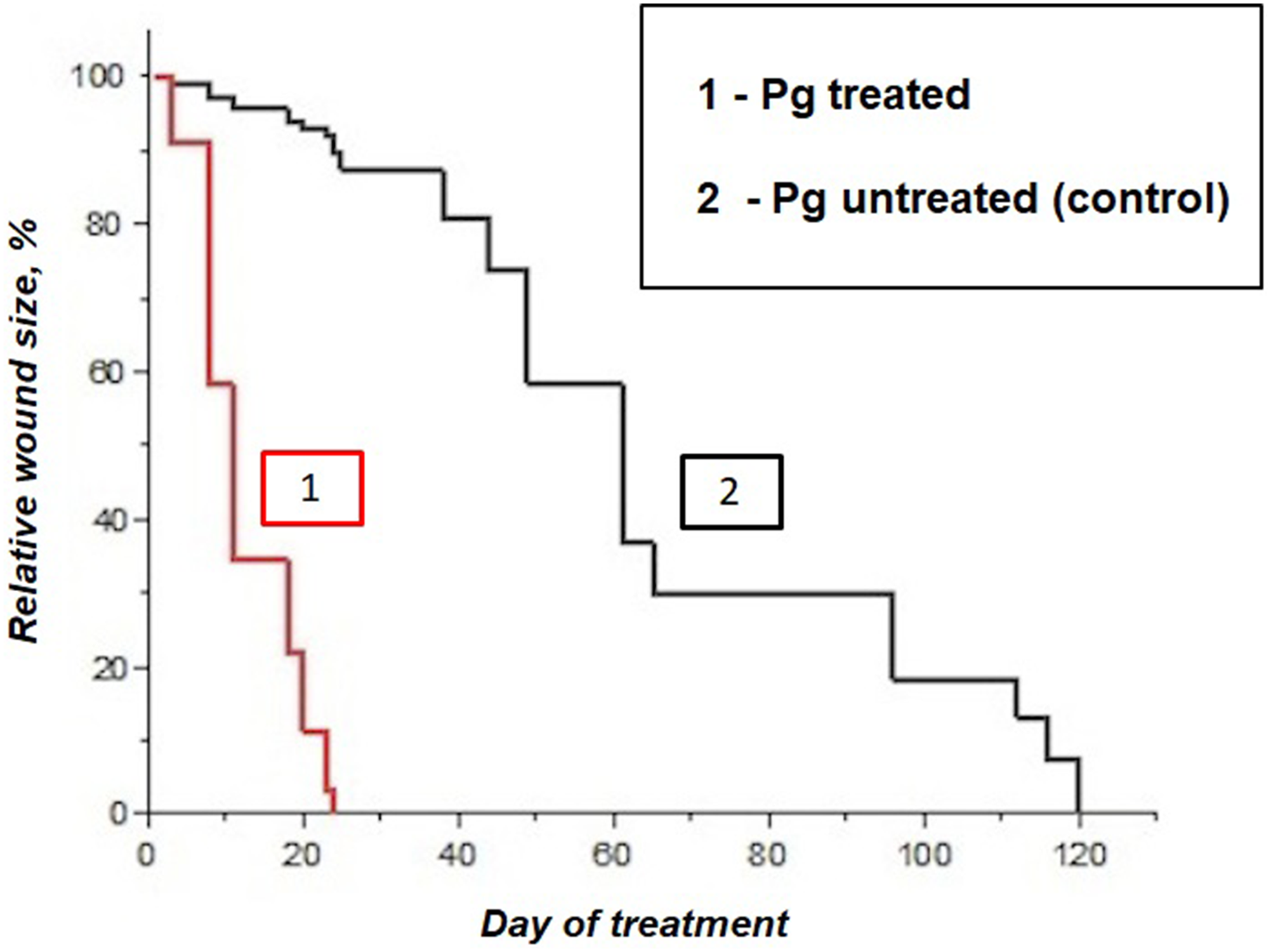
Kaplan-Meier healing curves depicting average wound closure rates. Significant difference are observed between plasminogen-treated and control groups (Wilcoxon, P = .0046).

Dynamics of clinical changes and healing of diabetic chronic foot ulcer treated with applications of autologous plasma-derived plasminogen.
Panels showing representative photographs of wound closure demonstrate enhanced healing of foot ulcers following the Pg-based treatment (Supplemental Materials).
All observed clinical symptoms are indicatives of locally applied Pg to induce the stage of acute inflammation through overcoming chronic inflammation phase, thus pushing wound to heal. After the sixth day of treatment, swelling and hyperemia decreased with reducing extent of exudation; wounds were also cleared of fibrin deposits. Between the 12th and 14th days of treatment with the use of local Pg applications, the wounds were completely cleaned from fibrin deposits, and the appearance of fine-grained granulation tissue were noted. The formation of granulation tissue in the wound cavity means a prerequisite for reepithelialization because it enables epithelial cell migration and wound closure. On the 16th day, the appearance of marginal epithelization and retraction of the wound area were documented. During 21 to 24th days, wounds were completely closed without notable signs of pathological scarring.
Plasminogen Treatment Improved Levels of the Key Protein Markers
In order to investigate plausible molecular mechanisms of Pg-induced benefits in wound healing, the key markers of hypoxia, angiogenesis, and autophagy were quantified in dermal lesion bioptates before and on the 18th day of the experimental treatment. Typical blotograms showing changes in HIF-1α, VEGF, angiostatins, and LC3 levels are depicted in Figure 5A, and the results of densitometric analysis are presented in Figure 5B. It was demonstrated that Pg application reduced expression of the central regulator of hypoxia-associated processes, HIF-1α, by 6.3-folds as compared with the initial value (P < .01). Obtained data may indicate that Pg application prevents progressive dermal ischemia.
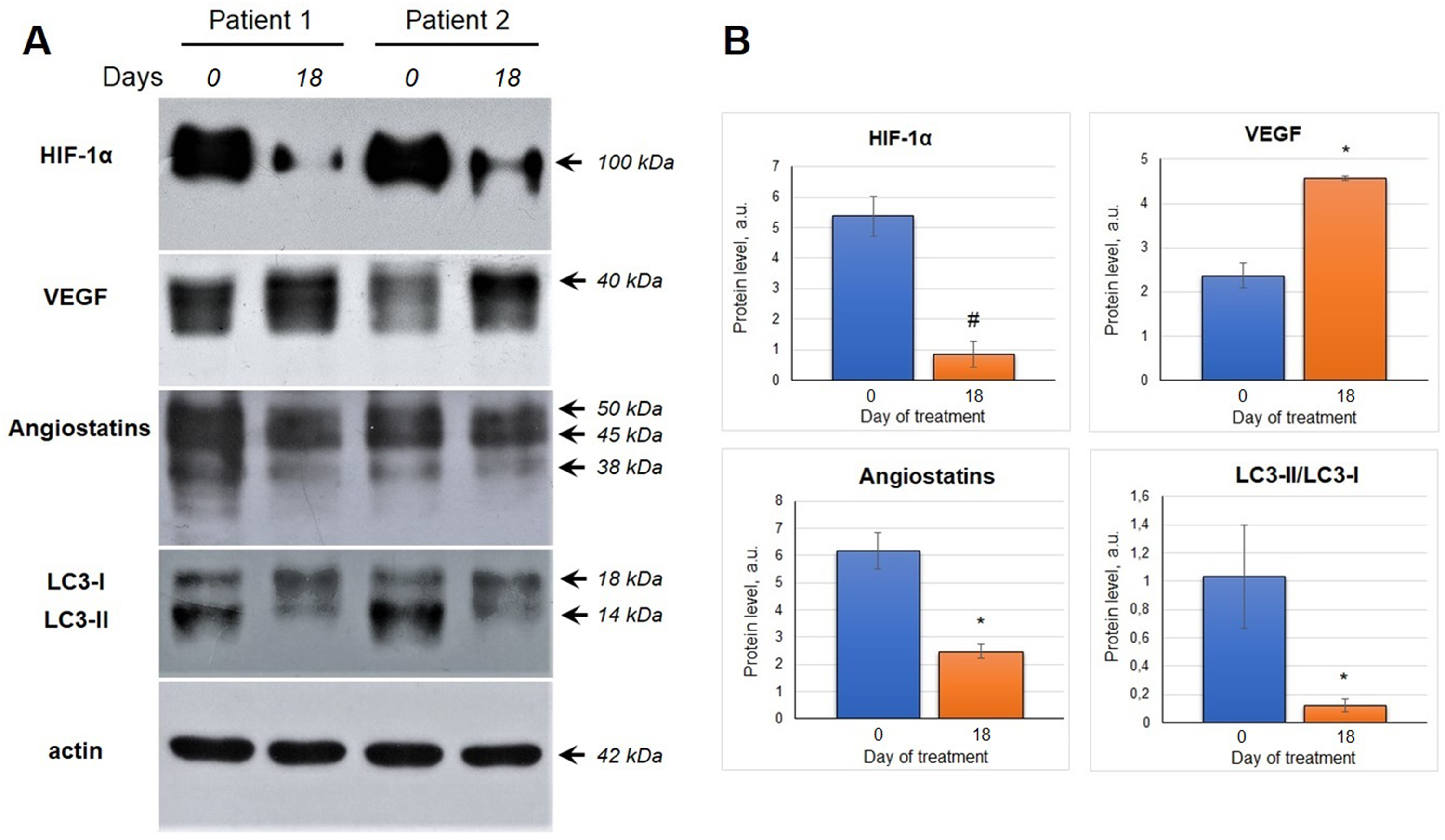
Changes in levels of the regulatory proteins in the wound dermal bioptates during plasminogen local application: A—representative blotograms, B—the results of immunoblot densitometric analysis (*P < .05; #P < .01, Mann-Whitney U test).
Plasminogen-based treatment affected expression of angiogenesis counteracting regulators, angiostatin and VEGF, thus shifting angiogenic balance toward activation state. It was shown that angiostatin polypeptides were presented as a set of 50-, 45-, and 38-kDa bands, which correspond to K1-4.5, K1-4, and K1-3 isoforms. Plasminogen treatment reduced total angiostatin content at the 18th day by 2.5-folds as compared with the initial level (P < .05), while increasing VEGF expression in wound bioptates by 1.9-folds (P < .05). These results mean that Pg promotes an angiogenic response through downregulating angiostatin formation and upregulating tissue expression of VEGF.
The results of quantitative analysis of autophagy-related protein LC3 in dermal bioptates demonstrate that Pg supplementation resulted in decreasing LC3-II/LC3-I ratio at the 18th day of treatment (by 8.6-folds, P < .05). This result suggests that the use of Pg as an option for treatment of diabetic chronic ulcers diminished autophagy flux, thus protecting tissue from autophagic cell death.
Plasminogen Treatment Reduces MMP-9 Overactivation in Diabetic Skin Ulcers
In chronic, hard-healing wounds, MMP overexpression has been long time known to contribute to the pathophysiology of healing disorders. 18 Earlier, we and other authors have shown that MMP collagenolytic activity remains permanently high in bioptates and fluids from nonhealing wounds, including diabetic ulcers and Martorell's syndrome. 19 In the present study, we compared MMP activities in persons with acute (surgery) wounds and trophic foot ulcers in diabetes patients treated with Pg application. Gelatin zymography revealed that acute wounds contain trace amounts of active MMP-9 isoform, whereas abundancy of MMP-9 activity was determined in diabetic ulcers (Figure 6). It could be assumed that excessive MMP-9 activity may contribute to wound healing abnormalities and chronicity of healing process. We showed that wound management with the use of Pg reduced MMP-9 activity by 3.5-folds at the 18th day of treatment as compared with the initial value (P < .01). It means that tissue remodeling is nearly to be completed, and high MMP activity is no longer needed.
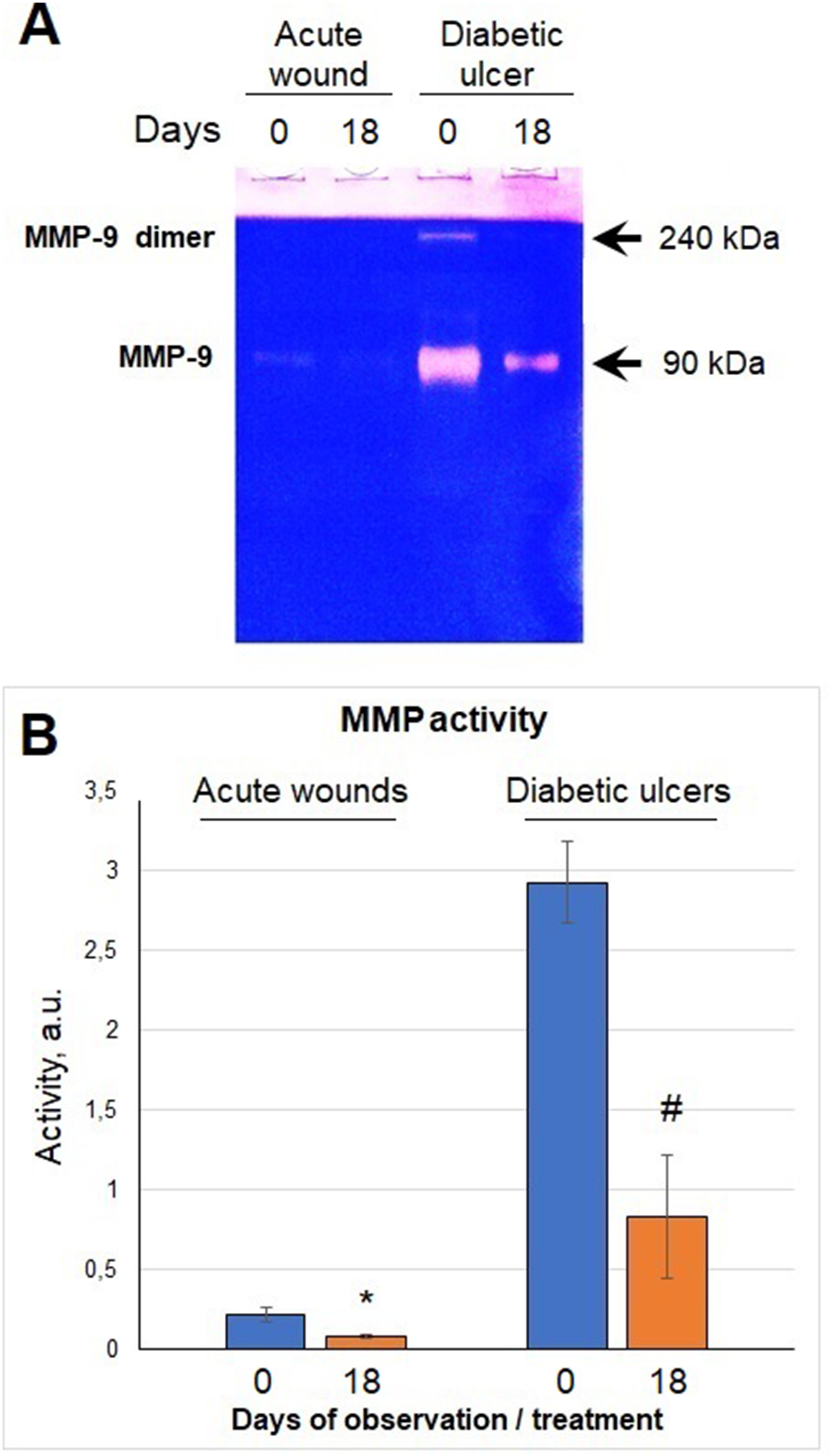
Evaluation of matrix metalloprotease activity (MMP assay) in tissue bioptates obtained from acute (surgery) wounds and diabetic foot ulcers treated with plasminogen topical application: A—typical gelatin zymography of matrix metalloproteases; B—the results of zymogram densitometric analysis (*P < .05; #P < .01, Mann-Whitney U test).
Discussion
Chronic diabetic wounds have great social and financial impact and affect the quality of life of millions of people, so that wound evaluation and management in patients with diabetes has become an actual challenge.1,20 To the best of our knowledge, our pilot study is the first clinical investigation that demonstrates Pg topical application to provide rapid and successful wound healing in type 2 diabetes patients with chronic foot ulcers. Among a plethora of proteins, which are involved in wound repair, Pg plays multifacial roles in the healing processes. It has been currently highlighted that physiological significance of Pg in wound healing is not limited to its conversion to Pm and extends far beyond its fibrinolytic function. However, recent studies have highlighted the importance of Pg in other processes beyond the hemostasis such as ECM remodeling, cell migration and apoptosis, inflammation, and angiogenesis.5,21 At present, more than 12 different cellular receptors for Pg, which are potentially related to wound healing, have been discovered. 22 Plasminogen binding to its cellular receptors contributes to monocyte migration, macrophage responses during inflammation, angiogenesis, and wound healing. Plasminogen is transported to the wounded site being bound to macrophages and neutrophils, where the Pg concentration is locally increased, leading to accelerated wound healing. 23 In turn, Pg stimulates macrophages to M1 phenotype transition. It is an important event in terms of wound healing, because too little inflammation could lead to tissue unhealed. 24 Thus, Pg-mediated macrophage reprograming may stimulate wound to heal by overcoming chronic inflammation. In addition to its role in the activation of inflammation, Pg is also crucial for subsequent steps, including resolution of inflammation and activation of the proliferation phase acting as chemoattractant for cells participating in cutaneous wound repair. 7
Our data extend previously reported information suggesting efficacy of Pg-based treatment of diabetic wounds. For example, Shen et al 23 have demonstrated that injections of Pg to mice with burn cutaneous wounds accelerates the healing process in the case of acute wounds and significantly improves the healing of chronic wounds in mice with hyperglycemia. Other study 10 has shown that local administration of Pg enhances the healing of radiation-induced wounds through reprogramming gene expression and modulating transcriptome in such a way to decrease risk of fibrosis. Plasminogen-deficient mice have been reported to accumulate massive fibrin and neutrophil depositions in the wounded area, resulting in chronic inflammation, improper tissue remodeling, and delayed formation of granulation tissue. 24 In humans, diabetes induces several types of posttranslational modifications in Pg molecules, which may contribute to its functional dysfunctions. 25 Glycation of Pg has been reported in both type 1 and type 2 diabetes mellitus patients that compromise fibrinolysis via decreasing Pm generation and proteolytic activity as well as Pg/Pm-fibrin interaction. 26 Since earlier data obtained in animal studies have shown that Pg supplementation improves wound healing, it would be of particular importance to observe whether application of plasma-derived Pg could accelerate rate of wound closure in persons with chronic diabetic skin defects. In our study, we successfully verified the basic idea that enhanced local delivery of Pg may overcome its functional deficit in poor-healing wounds to pushing them to heal.
Further, it was vital to discover the molecular mechanisms underlying beneficial effects of Pg in foot ulcer healing in patients with diabetes in the given clinical conditions. Such efforts was based on the quantification of the protein healing-related biomarkers related to the key pathophysiological patterns of wound repair, such as hypoxia, angiogenesis, tissue remodeling, and autophagy. It is known that during the first stage of healing, wound sites are under hypoxic condition developed due to the disruption of local vasculature and formation of fibrin deposits covering wound area. Chronic hypoxia can induce prolonged inflammation, deep vascular rupture, enhanced coagulation, disturbances in reepithelialization, and necrosis, resulting in delayed healing. 27 Tissue hypoxia induces a sustained increase in the expression of hypoxia-induced transcriptional factor 1α (HIF-1α), which is considered to be a central regulator of oxygen metabolism and a marker of hypoxia severity. 28 Overexpression of HIF-1α correlates with an enhanced expression of profibrotic factors and excessive fibrogenic response resulting in the development of keloid and hypertrophic scars. 29 We showed that Pg local application reduced HIF-1α level and thus can be used for preventing progressive dermal ischemia by manipulating HIF-1α expression in pathological diabetic cutaneous lesions to diminish risks of keloid formation.
Activation of the reparative angiogenesis has a vital importance for proper wound healing. 30 Since angiogenesis is a tightly regulated balance between activating growth factors and inhibitors, we quantified levels of 2 principal counteracting angiogenesis regulators, VEGF and angiostatins, in wound bioptates prior and after Pg application. Vascular endothelial growth factor is the key pro-angiogenic cytokine responsible for neovascularization and vessel remodeling to enable reoxygenation of damaged tissue and also positively influences wound closure and epidermal repair, granulation tissue formation. Failure of the wound to upregulate VEGF leads to impaired wound healing. 31 Western blot data demonstrate that Pg-based treatment significantly upregulated VEGF tissue level thus triggering pro-angiogenic signaling. It is possible that delay in VEGF expression in diabetic wound tissue could be a result of multiple inhibitory effects of angiostatins, which are known as by-products of limited proteolysis of Pg by several proteases, including MMPs and neutrophil elastase.32,33 It has been demonstrated earlier that these angiosuppressive factors may contribute to insufficient neovascularization and delayed wound healing even in the presence of elevated levels of VEGF and other activators of angiogenesis.19,34,35 In the present study, we showed that bioptates from chronic diabetic wounds contain abundancy of angiostatin isoforms, which can be produced locally by MMP-9. Matrix metalloproteinases are known as “sculptors of tissue remodeling” to play multiple roles in normal healing process. 36 However, uncontrolled and permanently enhanced MMP expression in skin lesions contributes to the pathophysiology of healing disorders and is considered a negative prognosis for wound healing. 37 We showed that specimens from acute wounds contained relatively low levels of active MMP-9 as compared with the bioptates from chronic foot ulcers, while Pg downregulated MMP-9 activity during the course of treatment. It can be hypothesized that decreasing MMP-9 activity observed in diabetic foot ulcers treated with Pg may result in restoring VEGF expression and improving neovascularization in the sites of injury through lowering angiostatin production. Cheng et al 38 has previously found that there is a direct link between Pg signaling and modulation of VEGF synthesis that supports our observations.
Fallah et al 10 have showed that Pg acts as a pleiotropic modulator of transcriptome, improving expression of many genes related to wound healing to their normal levels, including the genes involved in metabolism regulation. Oxygen deprivation and attenuated mitochondrial function induce autophagy, an evolutionary conserve process, which helps to maintain cell survival during metabolic failure or unfavorable conditions through mechanism that can partially degrade and recycle cellular components.39,40 However, dysregulation of autophagy can have detrimental outcomes during diabetic wound healing. Several studies have demonstrated that abnormally enhanced autophagy in hyperglycemia conditions provokes fibroblast apoptosis and autophagic death, inhibits cell proliferation, contributing to delayed healing and stimulation of hypertrophic scar formation.41,42 In agreement with above data, we found elevated LC3-II to LC3-I ratio in diabetic foot ulcers that means enhanced autophagic flux, while Pg exposure decreased autophagy intensity followed by rapid wound closure. It is possible that Pg downregulates autophagosome protein LC3-II expression as a sign of diminished autophagy flux via alleviating hypoxia events and improving oxygenation and nutrients supplementation of cells in a wounded area. Therefore, Pg-mediated targeting autophagy may represent an innovative strategy for the treatment of chronic wounds and prevention of ulcerations and pathological scar formation in diabetic foot syndrome.
Limitations and Perspectives
Our study has some limitations. Firstly, we dealt with relatively small sample size, though Pg-based treatment of diabetic foot ulcers ensured a remarkable curative effect in all recruited patients. Broader and more encompassing assessments of Pg healing effects including follow-up experiments, which were beyond the scope of the present study, are required. Secondly, the results of biochemical examinations should be confirmed by histological analysis, which will be an object of our future research. Thirdly, creation of wound dressing materials, hydrogels, or other carriers with immobilized Pg seems to be perspective with an insight into clinical practice. Finally, the use of autologous Pg is a cost-dependent process, thus repurposing pharmaceutical grade plasma-derived Pg for a rapid wound closure technology can be implemented in an economically more feasible manner.
Conclusion
We report here that topically applied plasma-derived Pg has a pronounced beneficial effect in promoting impaired foot ulcer healing in type 2 diabetes patients. We demonstrate here for the first time that Pg could accelerate wound healing rate through preventing dermal hypoxia, reducing autophagy flux, diminishing excessive MMP activity, and enhancing angiogenic response in a wound area tissue. Plasminogen local supplementation may represent a promising innovative strategy for the development of novel therapeutic approaches for improving wound healing in patients with diabetic foot ulcers, while further Pg testing for the elaboration of treatment tools for skin defects of other pathogenesis is needed.
Supplemental Material
sj-docx-1-ijl-10.1177_15347346241256025 - Supplemental material for Topical Application of Autologous Plasma-Derived Plasminogen Accelerates Healing of Chronic Foot Ulcers in Type 2 Diabetes Patients
Supplemental material, sj-docx-1-ijl-10.1177_15347346241256025 for Topical Application of Autologous Plasma-Derived Plasminogen Accelerates Healing of Chronic Foot Ulcers in Type 2 Diabetes Patients by Oleg Petrenko, Sergiy Badziukh, Victoria Korsa, Ihor Kolosovych and Artem Tykhomyrov in The International Journal of Lower Extremity Wounds
Footnotes
Acknowledgments
The authors would like to thank the patients and staff of the Central Polyclinic of the Ministry of Internal Affairs of Ukraine (Kyiv, Ukraine) for their support and collaboration that made this study possible.
Authors' Contribution
Petrenko O.—project administration, clinical research, formal analysis, manuscript review & editing. Badziukh S.—clinical research, data collection, validation. Korsa V.—plasminogen isolation, western blot, MMP assay, validation. Kolosovych I.—conceptualization, project administration, funding. Tykhomyrov A.—main scientific idea, conceptualization, methodology, laboratory research, data analysis, funding, writing original draft.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The investigation conforms to the principles outlined in the latest revision of the World Medical Association Declaration of Helsinki (Ethical Principles for Medical Research Involving Human Subjects). This study was approved by the local Bioethical Committee of Bogomolets National Medical University, Kyiv, Ukraine (protocol no. 2, October 26, 2022). Written informed consent was obtained from all patients before the commencement of the study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Bogomolets National Medical University of the Ministry of Health of Ukraine, Kyiv, Ukraine (state registration no. 0123U101055) and Palladin Institute of Biochemistry of the National Academy of Sciences of Ukraine, Kyiv, Ukraine (state registration no. 0123U100516).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.