
Abstract
Context
Diabetic foot disease is the major cause of nontraumatic limb amputations worldwide causing a high socioeconomic and psychological toll and a huge burden to the healthcare system. Currently, standard treatment of diabetic foot ulcer is through multidisciplinary therapy. Foot exercises have been shown to improve healing in diabetic ulcers although evidence is limited and applicability is non-uniform. Our study aimed to generate more evidence regarding the benefit of addition of protocolized foot exercises so that it can be instituted as a standard of care.
Methods and Material
It was an open label Randomized controlled trial with seventy-two patients and study duration of one and half years Patients with diabetic foot ulcers were randomized into two groups. Both groups received standard therapy for diabetic foot ulcer. The intervention group in addition received three months of protocolized foot exercises. At the end of three months ulcer healing and quality of life were m compared among both the groups.
Results
Regular exercises for three months caused significant reduction in ulcer area compared to the non-intervention group [100% versus 45.22%, 95% CI =36.30(16.04—56.56), P-value = 0.001]. Quality of life analyzed by SF-36 score showed significant improvement in components like physical function [69.4 ± 8.9 versus 63.7 ± 11.0, 95% CI = 5.73 (0.97-10.48), P-value = 0.01], emotional well-being [65.2 ± 7.6 versus 60.8 ± 7.9, 95% CI = 4.44 (0.79-8.10), P-value = 0.01], and pain components [55.4 ± 18.5 versus 47.5 ± 14.5, 95% CI = 7.99 (0.16-15.81), P-value = 0.04) at 3 months although change in social functioning, physical health limitation, health change, energy and general health improvement were not significant.
Conclusions
Addition of protocolized foot exercises are beneficial for patients of diabetic foot ulcers in terms of ulcer healing as well as improvement of quality of life provided compliance to exercises can be ensured.
Keywords
Introduction
Diabetes mellitus is a metabolic disease which affect multiple organ systems and is the single most leading cause for non-traumatic limb amputations 1 causing extensive socioeconomic and psychological burden on patient and health care system. Foot complications are usually ignored by patients of diabetes until the last stage. The foot complications of Diabetes mellitus also known as ‘Diabetic foot syndrome’, is defined by the World Health Organization, is an “ulceration of the foot (distally from the ankle and including the ankle) associated with neuropathy and different grades of ischemia and infection”. 2 Globally foot ulcer is present in among at least a quarter of diabetic patients, and is more common among males than females. It is estimated that diabetic limb amputations happen every 30 s and 85% of the amputations will be preceded by Diabetic foot ulcer. 3 Several pathogenic factors like neuropathy, peripheral arterial disease, abnormal foot biomechanics and poor wound healing cumulatively result in foot complications. In diabetic neuropathy, due to lack of sensitivity, there may be constant pressure over the sole for prolonged period which cause ischaemic necrosis in the local area. Sometimes there may be high pressure over the affected area of the foot for short pressure eg, object with less surface area such as nail, needle, sharp stones may cause direct injury. Also, repetitive moderate pressure cause inflammation and autolysis of the tissue which further cause foot ulceration due to trivial trauma. Following it there may be gangrenous changes in the foot and sepsis. 4
The management of diabetic foot 5 traditionally includes multidisciplinary team consisting of surgeons, primary care practitioners, and a patient representative, with inputs from experts in diabetes, diabetic foot rehabilitation, and vascular surgery 6 and the interventions include mechanical control or offloading, wound control, microbiological control, vascular control and metabolic control.
Foot exercises have been found to have a beneficial effect on healing of diabetic foot 7 ulcers by virtue of improvement in joint mobility, blood circulation, neuropathy and muscle strength although such studies are few and the evidence is limited.
The current study was conducted to generate more evidence regarding the role of protocolized foot exercises in healing of diabetic foot ulcers and in turn improving the quality of life diabetic patients.
Materials and Methods
Our study was designed as an open label interventional randomized clinical trial and study duration of eighteen months. Patients presenting with diabetic foot ulcer in outpatient department were enrolled after fulfilling inclusion and exclusion criteria and obtaining informed consent. Adult patients with diabetic foot ulcer Wagner 8 Grade 1 to 3 were included in the study. Patients with Wagner grade 4 or grade 5 ulcers, patients with orthopedic problems of hip, knee or ankle, who cannot perform foot exercises were excluded. Patients were randomized into two groups Foot Exercise group (FEx) (intervention group) and the No exercise groups (NEx). Allocation concealment was done by SNOSE 9 (sequentially numbered, opaque sealed envelopes) technique. Both the groups received standard therapy for diabetic foot wounds which included control of infection, control of hyperglycaemia, regular dressing with antiseptics, wound debridement and off-loading cast if required. All patients were routinely screened for presence of hypertension, chronic kidney disease, coronary arterial disease, chronic liver disease, peripheral arterial disease and smoking status from history, thorough clinical examination and relevant investigations and their management was optimised. Peripheral neuropathy was assessed by Diabetic Neuropathy Symptom (DNS) score. 10 None of the subjects were candidates for revascularization procedures.
In the FEx group, exercises were demonstrated to the patient by the investigator during the first visit and a pamphlet containing pictorial representation of exercise methods were handed over and advised to perform exercise thrice daily. Compliance to exercises was ensured by telephonic calls, done weekly once in addition to maintaining a dairy. Patient who performed foot exercises at least twice a day on an average for 3 months, were categorized as good compliance and less than once a day on an average were categorized as poor compliance and patients who were in between in performance were classified as average compliance. In each visit of the patient, wound area was measured. In subsequent visits amount of physical therapy recorded in diary was analyzed and compliance ensured. For both circumferential and non-circumferential wounds, image of the wound, photograph of the wound were taken using a smartphone camera with flash along with a sterile scale, and area calculated by ImageJ software. 11 For wounds which cannot be photographed in a 2D format, mechanical methods like ruler, calipers and graph paper were used to calculate wound size. Outcome of the intervention was measured by shrinkage in ulcer area, and comparison of complete healing of ulcer in both groups.
For assessing quality of life, online SF-36 calculator 12 was used. Score was calculated at the time of presentation and at the end of 3 months. Each component was calculated as percentage and changes at the end of 3 months determined. The main outcome variables were complete ulcer healing and improvement in quality of life. Clearance of institutional ethics committee was taken before starting the trial and this clinical trial was registered prospectively with the Clinical Trial Registry of India.
Protocol of Foot Exercise (Figure 1)
We followed the exercise protocol described by Goldsmith JR et al as it was methodical and had shown definite benefits.
13
It included
Passive dorsiflexion and plantarflexion of the metatarsophalangeal joints, holding each direction for 10 s Active dorsiflexion and plantar flexion of metatarsophalangeal joint, holding in each direction for 10 s Seated passive dorsiflexion and plantar flexion with application of the partial bodyweight at the metatarsophalangeal joint, holding each direction for 10 s Active dorsiflexion and plantar flexion of the ankles, hold in each direction for 10 s Active supination and pronation of the subtalar joint Standing Gastrocnemius stretch holding for 10 s and soleal stretch for 10 s
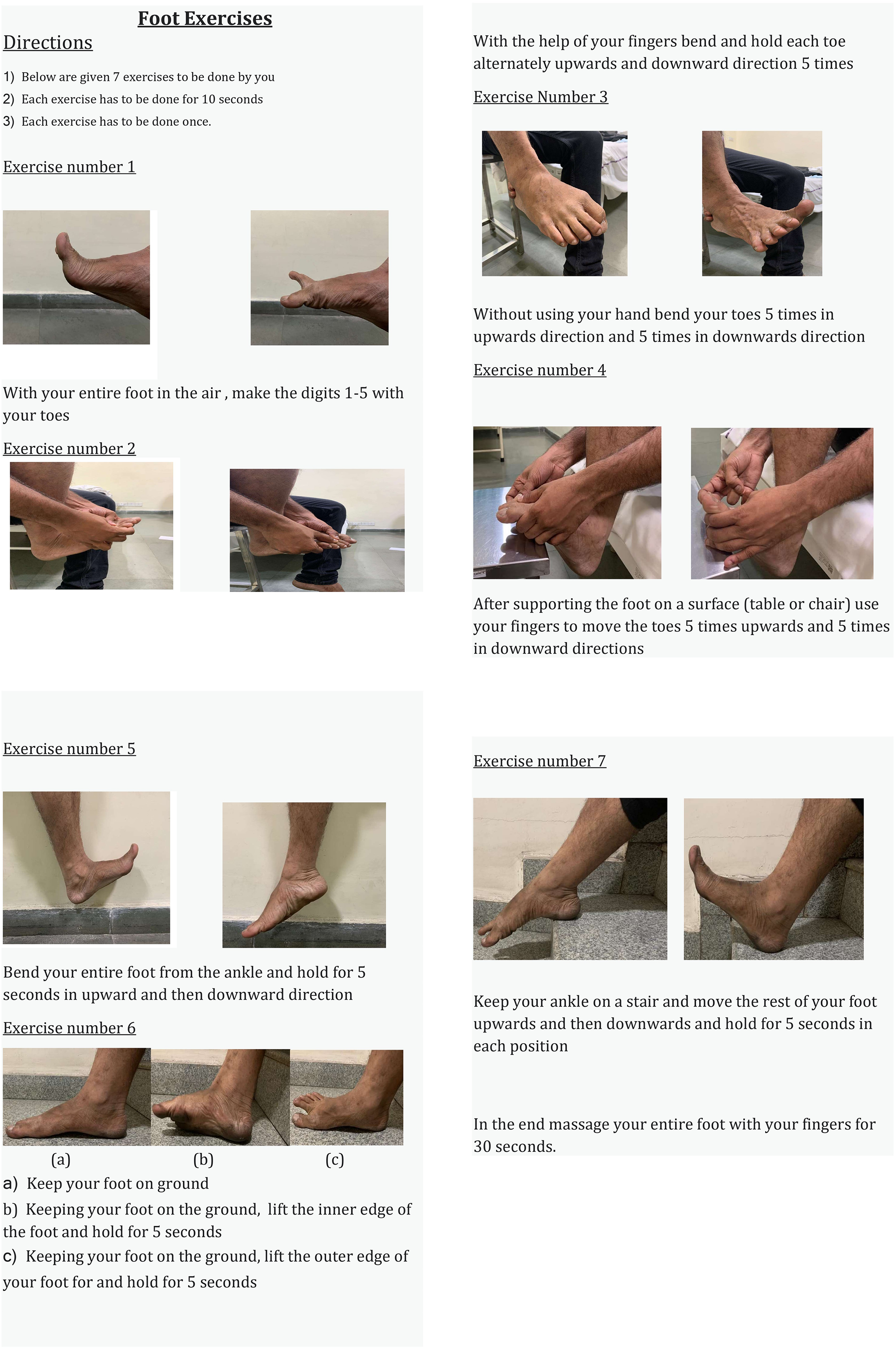
Protocol of foot exercises.
Soft tissue manipulation, 30 s at the forefoot, midfoot, rearfoot, posterior aspect of the distal 1/third of the leg bilaterally
The CONSORT flow diagram is given in Figure 2.
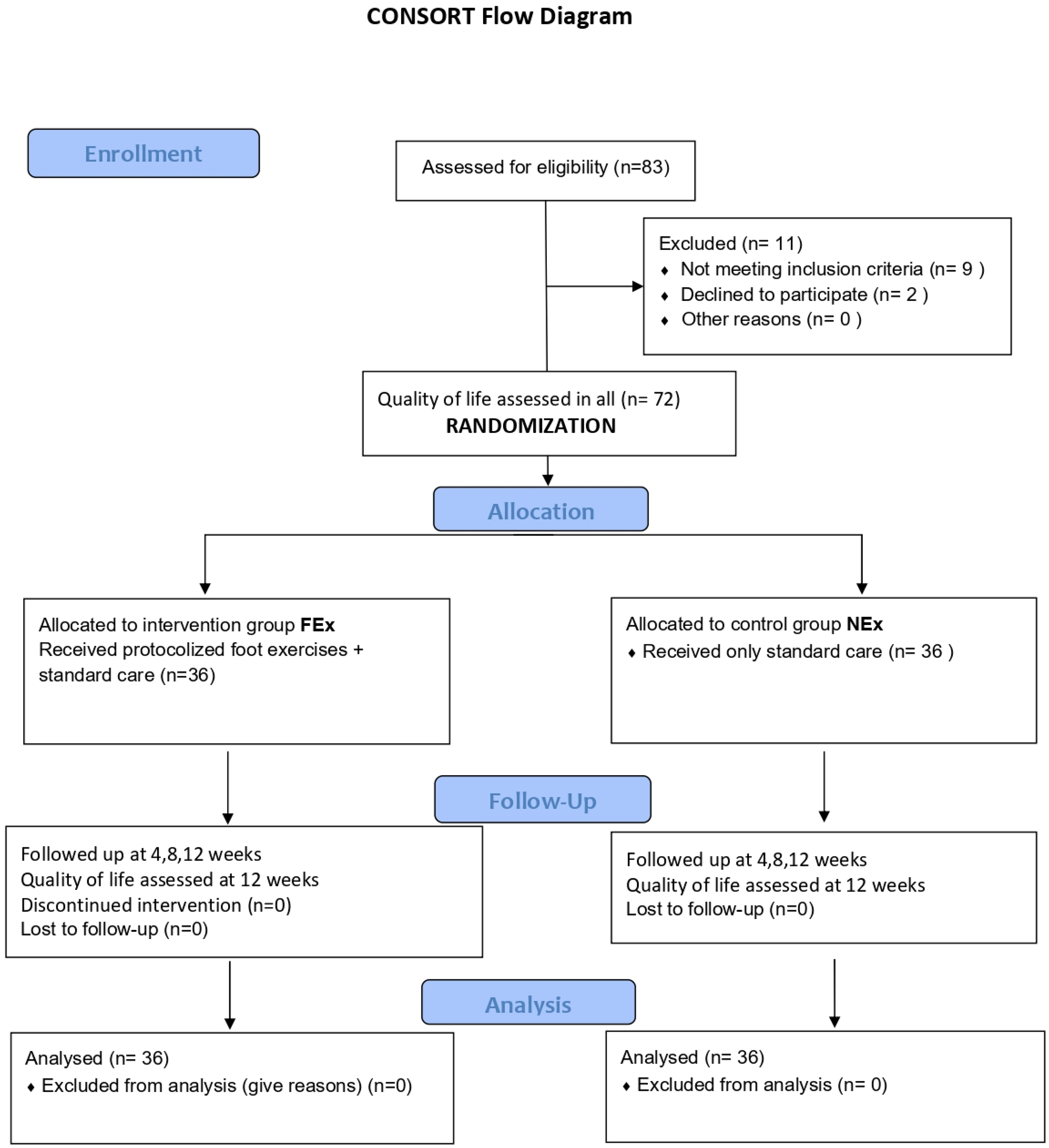
Consort diagram.
Statistical Analysis
Statistical analysis was per-protocol. The data on categorical variables is shown as n (% of patients) and the data on continuous variables is presented as mean and standard deviation (SD) for normally distributed variables and median (min – max) is used for non-normally distributed variables. The inter-group statistical comparison of distribution of categorical variables was tested using Chi-Square test or Fisher's exact probability test if more than 20% cells had expected frequency less than 5. The inter-group statistical comparison of means of normally distributed continuous variables was done using independent sample t test. The inter-group statistical comparison of medians of non-normally distributed continuous variables is done using Mann-Whitney U test. The underlying normality assumption was tested before subjecting the study variables to t test. Calculation of Kaplan-Meier (KM) survival curve was done for comparing ulcer healing rates.
Results
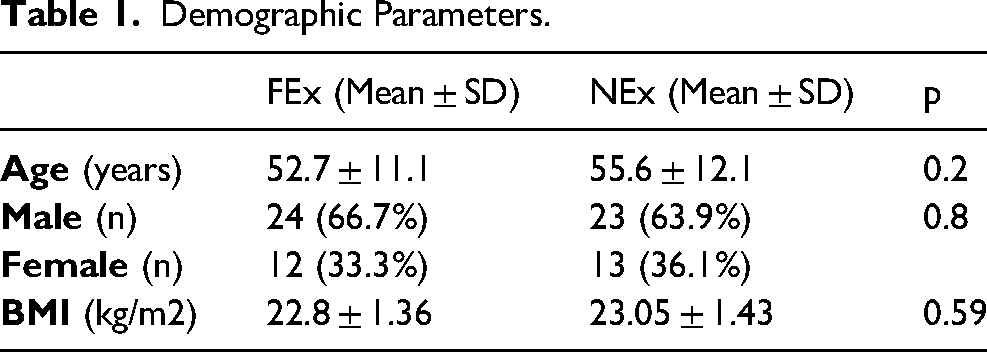
The base parameters of both the groups can be compared from Table 1. Demographic parameters like age, gender distribution and BMI did not differ significantly between two study groups (P-value > 0.05).
Demographic Parameters.
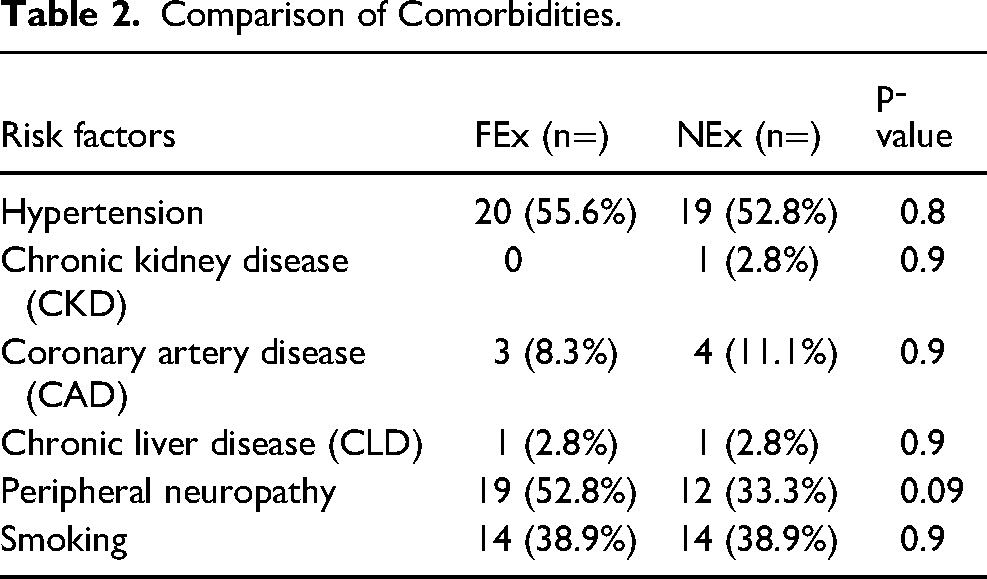
Comparison of comorbidities among both groups is shown in Table 2. Presence of hypertension, chronic kidney disease, coronary arterial disease, chronic liver disease, peripheral neuropathy and smoking status were considered. Distribution of comorbidities was comparable among both groups.
Comparison of Comorbidities.
Laboratory parameters fasting and post prandial blood glucose levels, HbA1c, haemoglobin level and total leucocyte counts are compared in Table 3. At the time of first visit most patients had uncontrolled fasting and post prandial blood glucose with a range of fasting 93–568 mg/dl and 55–404 mg/dl and a range of 142–626 mg/dl and 127–540 mg/dl postprandial blood glucose in the FEx and NEx groups respectively.
Distribution of Biochemical Abnormalities.

Mean fasting blood glucose, postprandial blood glucose HbA1c, hemoglobin and total leucocyte count were compared among the two study groups. These parameters did not differ significantly between two groups (P-value > 0.05).
Distribution of ulcer grades according to Wagner grading, at presentation and complete healing at subsequent follow up is depicted in Table 4. On presentation and after first month there were no significant differences between the two groups, but ulcer healing at the end of second and third months of follow up showed significantly better healing rates in the foot exercise group compared to the group without foot exercises.
Comparison of Complete Ulcer Healing.
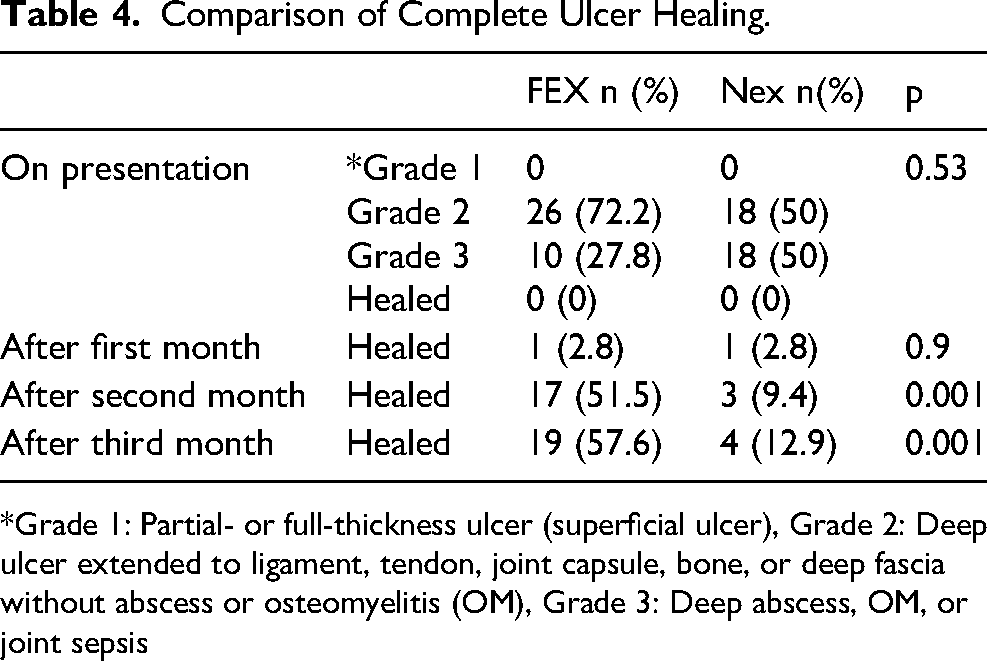
*Grade 1: Partial- or full-thickness ulcer (superficial ulcer), Grade 2: Deep ulcer extended to ligament, tendon, joint capsule, bone, or deep fascia without abscess or osteomyelitis (OM), Grade 3: Deep abscess, OM, or joint sepsis
Median ulcer area at presentation and subsequent follow ups is shown on Table 5. Distribution of median ulcer area after first month, after second month and after third month follow-ups is significantly lower in FEx compared to NEx (P-value < 0.05 for all). Median % reduction in ulcer area after third month follow-up with reference to ulcer area on presentation is significantly higher in FEx compared to NEx (P-value < 0.05). Kaplan Meier curve was calculated to compare the ulcer healing rates in both groups. (Figure 3). After 3 months of follow up 19 subjects in FEx group had complete healing of ulcer, while in NEx group only four subjects had complete healing of ulcer. Also, there were three amputations in FEx and five amputations in NEx group.
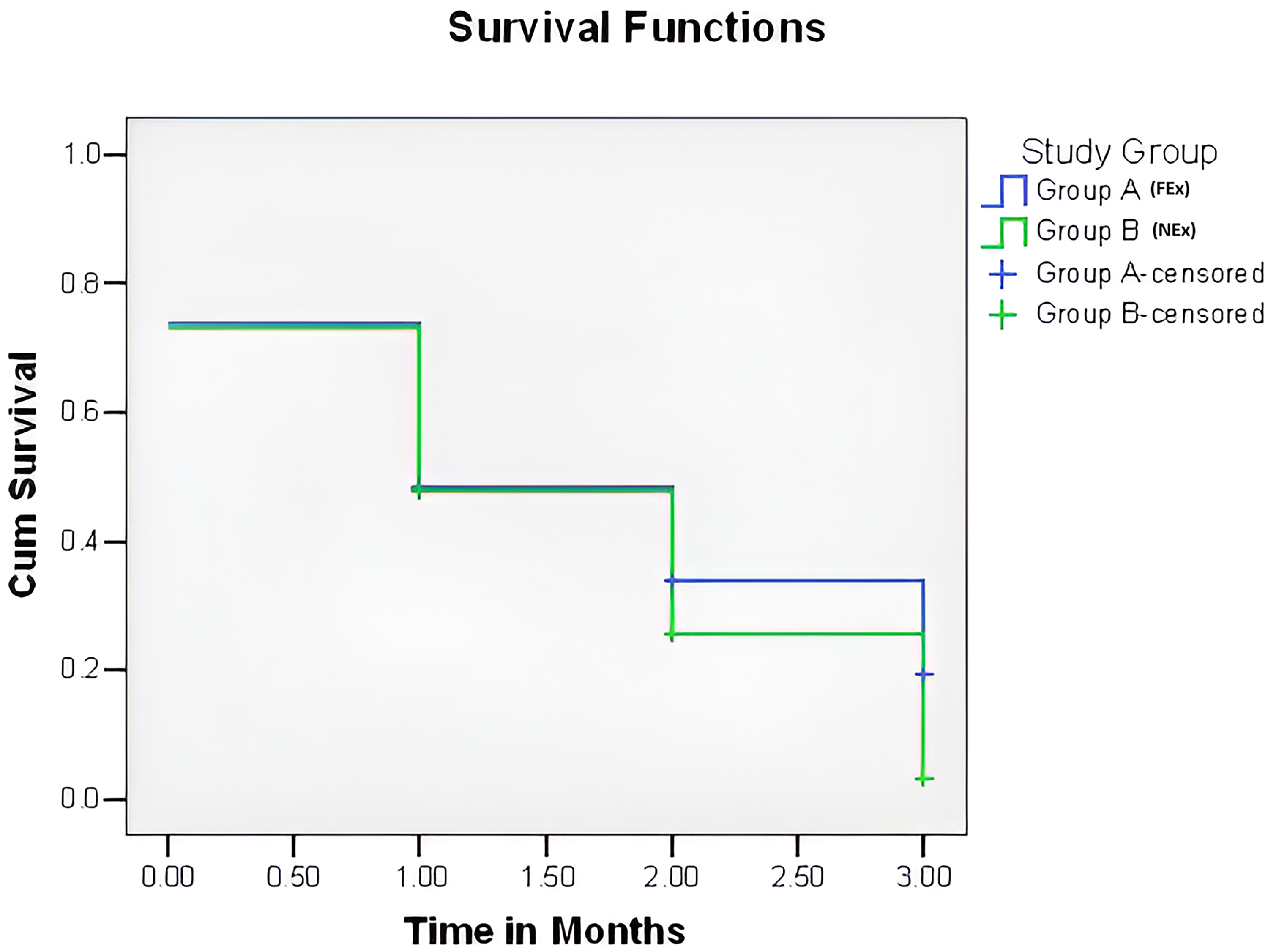
Kaplan-Meier (KM) survival curve for comparing study groups for ulcer healing. Log Rank (Mantel-Cox) value = 18.343, DF = 1, P-value = 0.001. Group A (FEx) has significantly better survival rate compared to Group B (NEx) (P-value < 0.05).
Comparison of Median Ulcer Area.
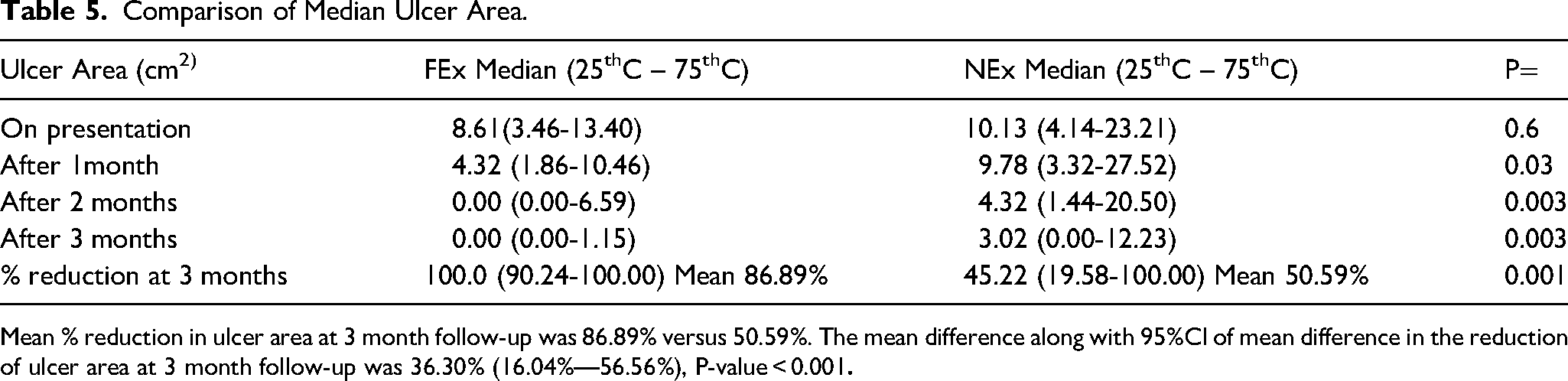
Mean % reduction in ulcer area at 3 month follow-up was 86.89% versus 50.59%. The mean difference along with 95%CI of mean difference in the reduction of ulcer area at 3 month follow-up was 36.30% (16.04%—56.56%), P-value < 0.001
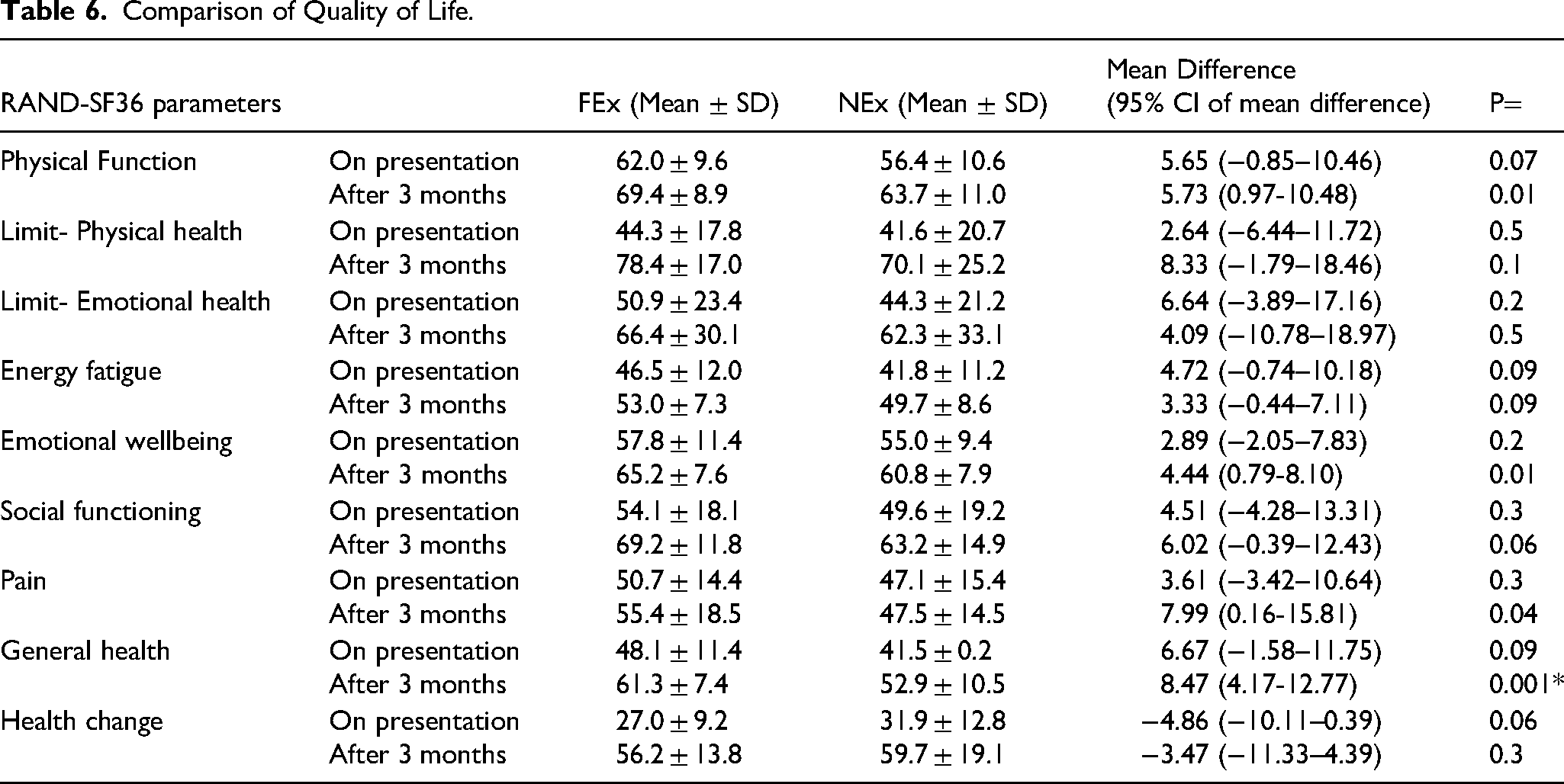
Quality of life was checked using RAND SF-36 questionnaire. Questionnaire was applied to all patients before randomization and at 12 weeks follow up. Comparison of quality-of-life parameters can be found in Table 6. Significant improvement in parameters at the end of three months was found in parameters like physical function, emotional well-being, pain, and general health in the FEx group (P < 0.05). There was improvement in rest of parameters too in the FEx group, however, the difference was statistically not significant.
Comparison of Quality of Life.
Discussion
Foot exercise therapy is a promising approach in patients with diabetic foot disease as it helps to increase joint mobility and blood flow. The definite benefits of foot exercise include improving blood circulation in the legs, strengthening of leg muscles, increasing the neurological status of the legs, and prevention of complications of injuries to the feet. It has been also shown that foot exercises in diabetes mellitus patient caused improvement in foot sensation. 14 Most foot exercise regimes described contain various combinations of exercises including “drawing” the alphabets A-B-C with the foot, passive and active dorsiflexion and plantarflexion of the metatarsophalangeal joint, ankles, active pronation and supination of the subtalar joint, stretching of the gastrocnemius and soleus and soft tissue manipulation of the entire foot. Although evidence of beneficial influence of such exercises exist, usually these exercises are not prescribed often enough, and, if prescribed, it is at random without any fixed protocol and therefore this type of therapy has not yet achieved the “standard of care” status in the multidisciplinary therapy of diabetic foot.
We found only two studies15,16 depicting the effect foot exercises on the healing of diabetic foot ulcer, both the studies have shown promising effect on healing of diabetic foot ulcer. One study 13 had only 19 subjects and 90% of participants in study group had decrease in the wound surface area. But the sample size of the study was small making it as important drawback. Also, none of these studies commented about the quality-of-life post foot exercises among these patients. We discuss the findings of our study under subsequent sections.
Demographic Variables
Most patients of diabetic foot ulcer in our study were male and belonged to the age group fifth to seventh decade. According to Vanherwegen et al 17 the preponderance of male sex to diabetic foot ulcer may be due to poor foot care behaviour and increased smoking.
Half of the patients in our study had normal BMI, 41% were overweight and remaining were obese. Eltilib et al 18 showed high BMI increases the risk of diabetic foot ulceration as high BMI is associated with hyperlipidaemia and peripheral vascular disease. They may also have glucose intolerance due to high BMI which causes severe hyperglycaemia and vascular complications. Indian people have high body fat percentage despite low BMI and hence prone to type 2 Diabetes mellites and its complications.
Comorbidities and Risk Factors
In our study, hypertension was the most common co-morbidity associated with study patients. Strain et al 19 showed increased arterial stiffness among diabetes patients due to atherosclerosis secondary to advanced glycation end products occur at arteriole and capillary levels. These changes are synergised by hypertension and together they have increased rate of arterial stiffness. In our study peripheral neuropathy was checked by DNS score. Almost half of our patients had peripheral neuropathy on presentation.
Blood Sugar, HbA1c Level and Anaemia
The relationship between smoking and healing of diabetic foot ulcer has been widely studied. In our study 28 out of 72 had history of smoking (38%). Smoking induces generation of reactive oxygen species in leucocytes, causes impaired vasodilator response to stimulus in skin and increased adrenergic driven vasoconstriction. 20 A study from Eltilib et al 18 from Sudan showed significant association of smoking with the foot ulceration in diabetics.
Estimation of blood sugar was done at the time of presentation among both study and control groups. In both groups diabetes was completely uncontrolled and might have been one of the important factors in development of diabetic foot disease in these patients. The difference of values was statistically insignificant among the groups however(P > 0.05). There is no relationship between the baseline HbA1C and healing of diabetic foot ulcer in our study, however in a study Xiang et al 21 it was found that ulcer healing was high when HbA1C was between 7 and 8. This result was obtained in the study only after removing the maximum confounding factors like associated hypertension etc Currently it is recommended that patient with diabetic foot ulcer should have HbA1c between 7–8% as more than 8% is associated with increased risk of lower limb amputation. 22
In our study out of 72 subjects 59 had anaemia (82%), in which 35 were males and 24 were females but only one patient required blood transfusion. Since majority of diabetic patients are elderly and have anaemia,23,24 correction of anaemia must be among the standard protocol for treating these patients either via oral medications or blood transfusion.
Ulcer Grades at Presentation and Complete Healing
In our study most of the Diabetic foot ulcers were Wagner grade 2 in study group ie, 26 out of 36 and 10 were in Wagner grade 3. In control group 18 were grade 2 and 18 were grade 3. These differences were statistically not significant at presentation (P value- 0.053). No patient in each group was grade 1 at presentation. After first month one patient in each group showed complete healing of their ulcer. However, at the end of two and three months of therapy considerably more number of patients in the foot exercise group showed healing compared to the other group which was statistically significant. The percentage of reduction of median ulcer area was 49.8% in study group compared to control group where it was 13.5%. It shows that in participants performing foot exercises, the ulcer begins to heal early ie, at first month compared to non-exercise performing group were ulcer start healing at second month. These results were found similar to study by Eraydin et al. 16 At the end of 3-month complete healing of ulcer was found in 19 out of 36 patients in study group compared to 4 in control and amputation was seen in only 3 patients of study group compared to 5 in control group. Compared with area at presentation there was 100% reduction in median ulcer area in study and 45.22% reduction (−63.91–100%) reduction in control group. Calculation of Kaplan-Meier (KM) survival curve shows group FEx has significantly better healing rate compared to group NEx (P-value < 0.05).
Compliance to Protocolized Exercises
Any intervention is ineffective unless compliance is good. In our study 30 out of 36 participants had good compliance with exercise therapy. Two had average compliance and four had poor compliance to study. The subjects who had poor compliance to study underwent amputation later after 2 months. In participants who had average compliance, one had completely healed ulcer at the end of second month owing to good vascularity and low grade at presentation and another had partial healing of ulcer. The participants who had poor compliance had higher grades of ulcer and pain due to which they could not perform recommended exercises.
Effect of foot exercises in reducing the ulcer area is primarily due to increase in blood flow of affected limb. Since most of ulcer grades in the study group were grade 2, without involving the bone, ulcers healing started in the first month itself compared to control group. There was also increase in joint mobility and strength of muscles which acted synergistically. All the patients had regular follow up in OPD and necessary debridement and good glycaemic control. Hence ulcer healing was good and only 8 amputations were done among 72 subjects.
By this study we can conclude that there is improvement in rate of ulcer healing in participants performing foot exercises, and it is advisable to perform foot exercises according to objective of our study for better ulcer healing.
A study by Eraydin et al 16 with 60 patients, had similar results to our study but it is one of the few such studies to date. It had also compared the depth of ulcer and there was significant reduction in ulcer depth in study group than control group. A quasi-experimental pilot study by Flahr et al 25 had increased healing in study group though compliance to exercise was poor. Victor et al 26 used supervised aerobic exercises in their study, with the patients being prescribed exercises three times per week under supervision. The current study adds more concrete evidence to the findings of previous studies with more participants and proper study design. While active supervision is beneficial for compliance with exercises, however it also entails patients with decreased mobility attending the hospital regularly which is inconvenient. It also requires more involvement of healthcare workers and its feasibility in Indian context with a low health care worker to patient 27 ratio is doubtful. Our study demonstrates that adequate compliance without active supervision can be maintained by weekly telephonic consultation and monitoring of the exercise diary during scheduled visits. This also avoids travelling costs for the patient. With the increasing availability of messenger apps, video monitoring can also be tried in future to improve compliance further.
Quality of Life
In our study of comparison of quality of life between FEx and NEx using RAND- SF36 questionnaire, we found significant difference in parameters like physical function, emotional well-being, pain, and general health parameters at the end of 3 months (P < 0.05). Rest of parameters improved at the end of three months, but the difference was statistically not significant(P > 0.05). Significant improvement in physical function may be attributed to improvement in the overall daily activity of the patient like walking, climbing, and lifting weight which was not possible previously. Most of the participants were male and were daily labourers and farmers, who after the healing of ulcer could do previous activities. Improvement of emotional status in our study can be attributed to decreased pain and increased social activity among the participants. Improvement of pain status was due to healing of the ulcer primarily and improvement of diabetic neuropathy following exercise. Improvement in other domains were also seen in both groups, but were comparable and statistically not significant.
A study by Sajel and Saranya 28 comparing the quality of life in diabetic foot ulcer patients before and after structured patient education showed statistical difference in physical health, role of limitations due to physical health and pain component between men and women.
There is no published data measuring the benefits of foot exercises in improving the quality of life in patients with diabetic foot ulcerations. As concluded by previous study diabetic foot ulcer patients will usually have poor quality of life as they have problems primarily in mobility, pain/discomfort. Also, there will be in ability to stand or walk without help are the common reasons. 29 And addition of foot exercise will definitely of benefit as suggested by our results.
Strengths and Limitations of Study
The main strength of our study was that we were able to maintain exercise compliance among the FEx patients. More than 80% of patients had good compliance according to study plan, they were encouraged to maintain the diary which was monitored during every visit. Regular telephonic conversations were also made to ensure adherence. There was no loss to follow ups. There was no heterogenicity in patient demographics, thus indicating proper randomization.
Limitations of our study include non-supervised exercises. All the patients were outpatient based and there is self-reported compliance of foot exercises which is not as reliable in all patients as supervised exercise. Some subjects on FEx were not able to follow the instructions clearly as they were illiterate to read the instructions on pamphlets provided. Another limitation in our study was about Image J software. The mapping of the area by this software is very sensitive and slight change in wound margin tracing would change entire wound area. To overcome this average of 3 areas were taken. It was not able to measure the depth of wound. Studies with larger sample sizes may have better generalizability. To overcome these limitations in future studies direct observation of exercise therapy can be done.
Disclosure and Acknowledgement
There is no conflict of interest and funding was not received from any sources for the above study.
Conclusion
As can be seen from the results, our study has generated important evidence regarding the beneficial effect of addition of protocolized foot exercises to standard care in diabetic foot ulcer patients. Regular exercises for three months caused significant reduction in ulcer area and improvement in ulcer grade in patients compared to not performing exercises. Quality of life was analysed by SF-36 score and there was significant improvement in components like physical function, emotional well-being, and pain components although change in components like social functioning, physical health limitation, health change, energy and general health improvement after 3 months was not significant. Thus we recommend that addition of fixed protocol of foot exercises be made a standardised part of multidisciplinary care for diabetic foot patients.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.