
Abstract
Aim
To clarify the clinical characteristics of autoimmune disease (AID)-related ulcers to improve treatment outcomes.
Materials and Methods
The medical records of 189 patients treated for AID-related ulcers at two tertiary hospitals in Nanjing, China, from January 1, 2018 to December 31, 2022 were retrospectively reviewed. The relevant clinical data included diagnosis, type and severity of wounds, and prescribed medications.
Results
Of the 189 patients with AID-related ulcers, 146 (77.25%) were female and 43 (22.75%) were male. The top four immunological diagnoses were rheumatoid arthritis, systemic lupus erythematosus, Sjogren's syndrome, and vasculitis. The four most common wound sites were the lower limb, foot, hand, and upper limb. Regarding the number of wounds, 81 (42.86%) patients had one ulcer, 43 (22.75%) had two, 30 (15.87%) had three, and 35 (18.52%) had four or more. More than half of the patients (54%, 102/189) were previously treated for AID-related ulcers. Of these 102 patients, 27 (26.47%) had one previous diagnosis, 49 (40.83%) had two, and 26 (25.49%) had three or more. Among all 189 patients, 142 (75%) had clinical symptoms of local infection. Of these 142 patients, bacteria cultures were conducted for 70 (49.30%), of which 63 (90.00%) were positive. The most commonly detected bacteria were Staphylococcus aureus, Pseudomonas aeruginosa, Acinetobacter baumannii, and Klebsiella pneumoniae. The median (interquartile range) duration of AID-related ulcers was 55 (39, 90) days. Most patients (87.3%, 165/189) received systemic therapy with immunosuppressants and hormones.
Conclusions
The most common clinical characteristics of AID-associated ulcers were spontaneous rupture, long duration, multiple wounds, bacterial infection, and recurrence. Clarification of the clinical characteristics of AID-associated ulcers can improve treatment outcomes.
Keywords
Introduction
An autoimmune disease (AID) is a disorder of the immune response to self-antigens resulting in tissue damage and organ dysfunction. 1 To date, there are more than 100 recognized AIDs, which include systemic lupus erythematosus (SLE), rheumatoid arthritis (RA), and dermatomyositis. 2 The global incidence of AIDs has continued to increase over the past 30 years. 3 In the United States, AIDs are the leading causes of death of young and middle-aged women. 4
The pathogenesis of AIDs include the collapse of autoimmune tolerance and abnormal activation of immune cells by autoantigens, resulting in the production of pathological autoantibodies. 5 Autoantibodies in serum can bind to cell-surface autoantigens in the skin, connective tissue, and blood vessels to induce abnormal immune responses, leading to persistent pathological inflammatory damage to tissues and organs.5,6 The skin has more connective tissue and blood vessels than any other organ. Autoimmune responses lead to vasculitis of connective tissue, myxoid edema, fibrinoid degeneration, and inflammatory cell infiltration, which ultimately lead to AID-associated ulcers. 7
AIDs are important causes of chronic atypical wounds. 8 A large epidemiologic study conducted in wound-repair clinics has reported that 20%–23% of chronic wounds are associated with autoimmune conditions. 9 Hence, AIDs should be considered for diagnosis of chronic wounds that do not respond to standard treatment regimens. 10
Severe debilitating fatigue often accompanied by sleep disorders and depression is the most common complaint of patients with AIDs. 11 Long-term disease duration often leads to anemia and hypoproteinemia, which can result in insufficient nutrition and oxygen supply with subsequent poor cell activity, ultimately impairing wound repair.11,12 Besides, early clinical diagnosis of AID-related ulcers is difficult and there is no consensus on the use of immunosuppressants because of the increased risk of infection. 13 Moreover, long-term use of glucocorticoids or immunosuppressants can suppress cell-mediated immunity of local connective tissue and blood vessels, resulting in delayed wound repair.13,14
Therefore, the aim of the present study was to clarify the clinical characteristics of AID-associated ulcers, especially duration, location, frequency, and infection, to improve treatment outcomes.
Materials and Methods
Study Approval
The study protocol was approved by the Ethics Committee of XX (approval no. 202347301). The requirement for written informed consent was waived due to the retrospective nature of this study.
Collection of Patient Data
The medical records of patients treated for AID-associated ulcers at two tertiary hospitals in Nanjing, China, from January 1, 2018 to December 31, 2022 were retrospectively reviewed. The inclusion criteria were (i) age ≥18 years, (ii) confirmed diagnosis of AID-associated ulcers in accordance with the 2010 diagnostic criteria of the European League Against Rheumatism for rheumatic immune diseases, 15 and (iii) impaired skin integrity.
The collected patient data included (i) general demographic information (age, sex, immunological diagnosis, and comorbidities), (ii) wound location, number, duration, causes, reoccurrence, infection, and bacterial culture results, and (iii) use of immunosuppressants and hormones. The collected data were verified by two of the authors (Enterostomal Therapists with 5 + years of experience) to ensure accuracy.
Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics for Windows, version 25.0. (IBM Corporation, Armonk, NY, USA). Normally distributed data are presented as the mean ± standard deviation, non-normally distributed data as the median and quartile range, and counted data as the number and percentage. A probability (p) value < .05 was considered statistically significant.
Results
Patient Characteristics
The study cohort included 189 patients (146 females and 43 males; mean age, 53.68 ± 16.35 years; age range, 18-94 years) with AID-related ulcers. Notably, the proportion of females was significantly greater than males (77.25% vs 22.75%, respectively, p < .05).
Immune-Related Diagnosis
The top four immunological diagnoses were RA, SLE, Sjogren's syndrome (SS), and vasculitis. Others diagnoses included dermatomyositis, scleroderma, pyoderma gangrenosum, and antiphospholipid syndrome. As shown in Table 1, the two most common comorbidities were hypertension and diabetes mellitus.
Patient Information.
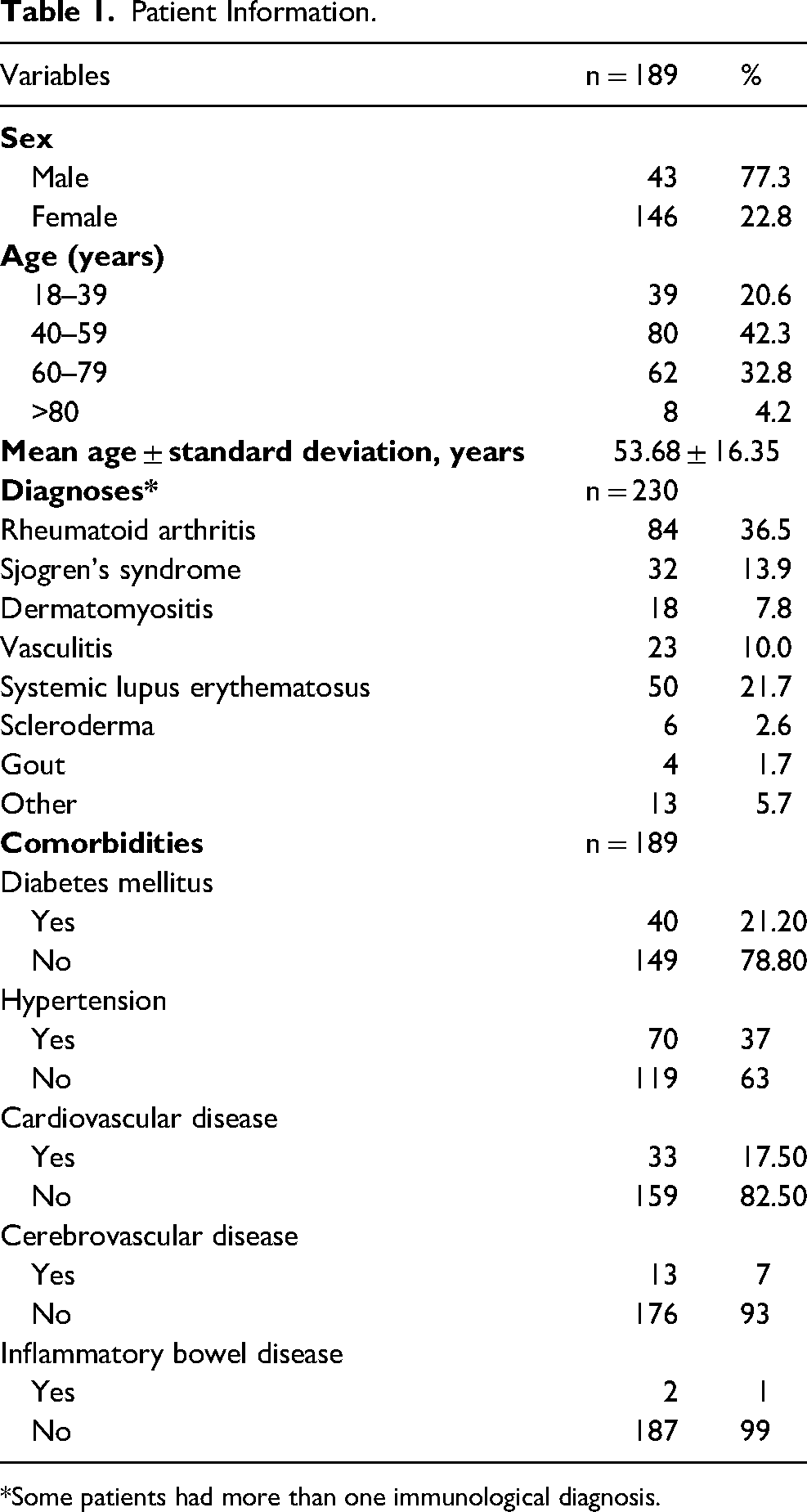
*Some patients had more than one immunological diagnosis.
Wound Characteristics
The 189 patients had 407 wounds. The four most common wound sites were the lower limb (125, 30.71%), foot (100, 24.57%), hand (64, 15.72%), and upper limb (45, 11.19%). Regarding the number of wounds, 81 (42.86%) patients had one ulcer, 43 (22.75%) had two, 30 (15.87%) had three, and 35 (18.52%) had four or more. The causes of the wounds of the 189 patients were spontaneous (140, 74.07%), scratching (20, 10.28%), trauma (13, 6.88%), and other causes (16, 8.47%) (Table 2).
Wound Characteristics.
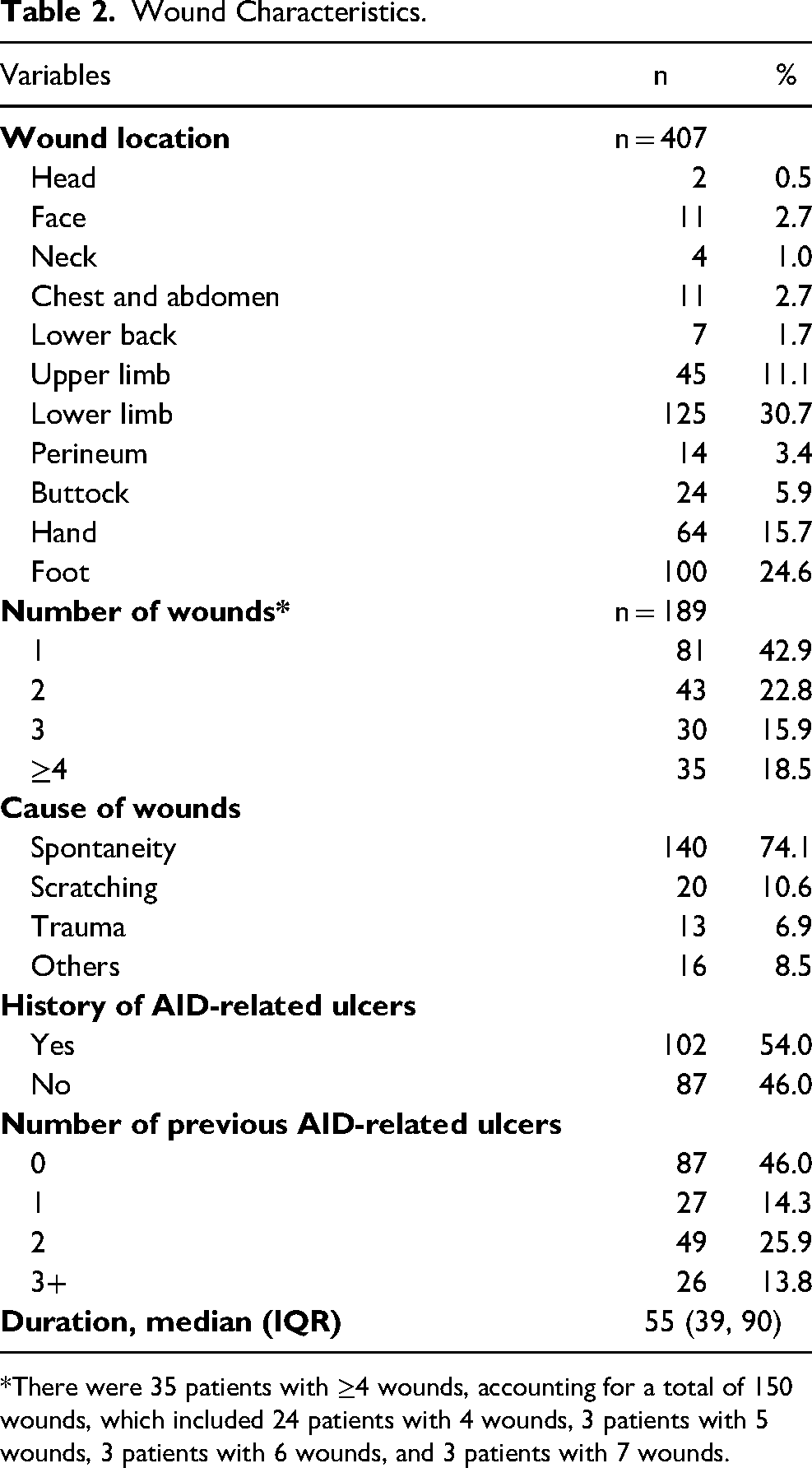
*There were 35 patients with ≥4 wounds, accounting for a total of 150 wounds, which included 24 patients with 4 wounds, 3 patients with 5 wounds, 3 patients with 6 wounds, and 3 patients with 7 wounds.
Of the 189 patients, 87 (46.03%) were diagnosed with AID-related ulcers for the first time. Of the other 102 patients, 27 (26.47%) had one previous diagnosis, 49 (40.83%) had two, and 26 (25.49%) had three or more. The median (interquartile range) duration of AID-related ulcers was 55 (39, 90) days.
Wound Infection
In accordance with the 2010 diagnostic criteria of the European League Against Rheumatism for rheumatic immune diseases,15,16 75.1% (142/189) of the wounds exhibited clinical symptoms of infection, which included fragile granulation, increased effusion, high skin temperature, redness, and purulent discharge. Of the 142 patients with suspected wound infections, bacteria cultures were conducted for 70 (49.30%), of which 63 (90.00%) were positive. In total, of 76 different types of bacteria were detected. The most detected bacteria were Staphylococcus aureus, Pseudomonas aeruginosa, Acinetobacter baumannii, and Klebsiella pneumoniae (Table 3).
Bacterial Cultures.
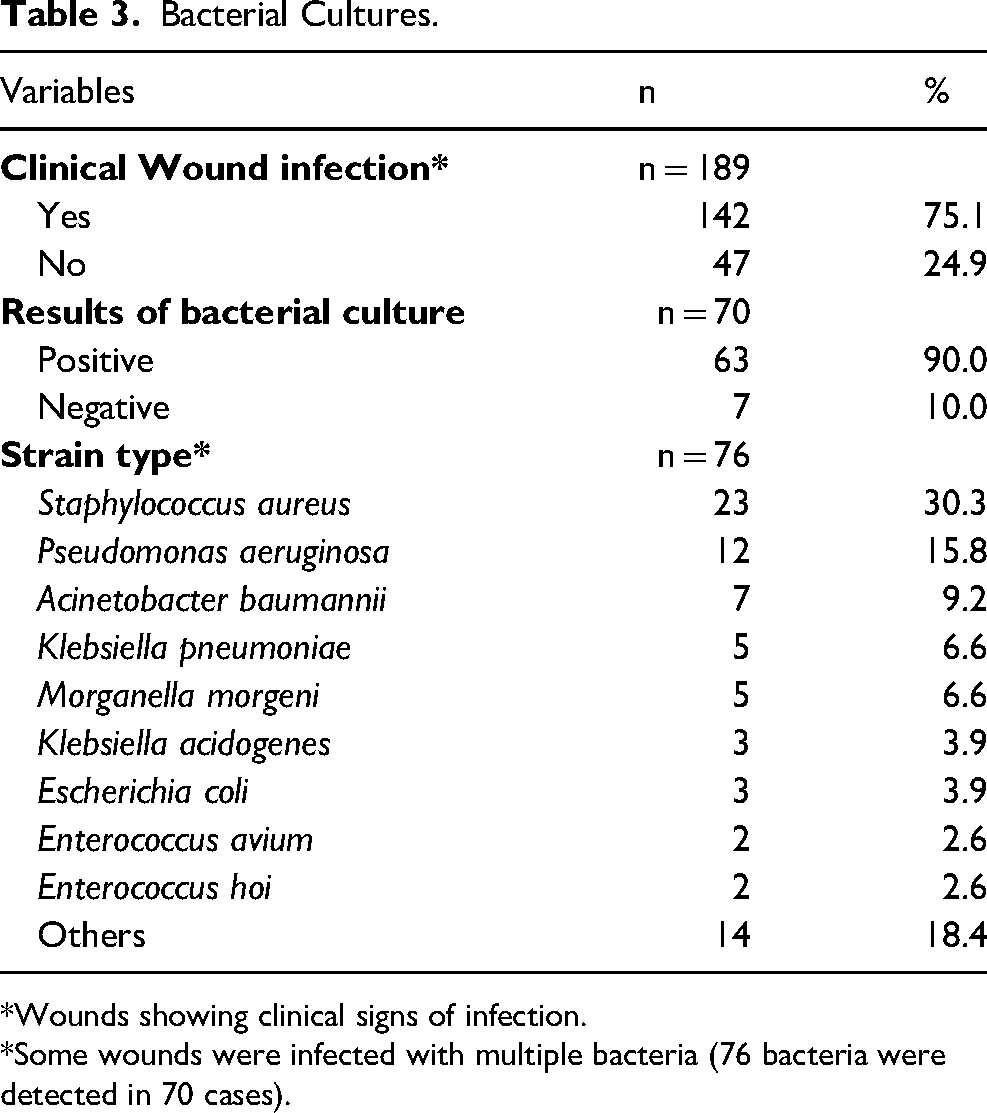
*Wounds showing clinical signs of infection.
*Some wounds were infected with multiple bacteria (76 bacteria were detected in 70 cases).
Use of Immunosuppressants and Hormones
Most patients (87.3%, 165/189) received systemic therapy with both immunosuppressants and hormones. Immunosuppressants or hormones only were prescribed to 17 and 7 patients, respectively.
Discussion
Although AIDs can occur at any age, some age groups are more susceptible to specific diseases. Due to differences in hormone levels, the incidence of AIDs tends to be higher in women. 17 Accordingly, in this study, most patients with AID-related ulcers were female (77.25%, 146/189).
RA, SLE, SS, and vasculitis are the most diagnosed AIDs. RA is an immune-mediated chronic inflammatory disease that primarily affects the joints, although skin involvement is a common clinical manifestation, as about 40% of RA patients will develop skin lesions. 18 RA-associated ulcers usually occur on the anterior calf and are mostly associated with venous and arterial ulcers caused by vasculitis.18–20
SLE is a connective tissue disease characterized by the presence of anti-nuclear antibodies in the blood and involving multiple organs and systems, and involves the skin in 80%–90% of patients. 21 An ulcer of the lower extremity is considered a non-specific manifestation of SLE-associated interface dermatitis, which most commonly appears on the ankle, anterior tibia, and coccyx, and may involve the superficial fascia layer or deeper, and are often characterized by recurrence and delayed wound repair.22,23 A cohort study conducted in Latin American showed that among 449 patients with SLE-associated cutaneous vasculitis, 14.9% had primary ulcers and 30.2% had ulcers secondary to skin lesions associated with lupus erythematosus, such as discoid erythema. 24
About 80% of SS cases involve autoimmune inflammation of the exocrine glands. SS-related lesions mostly appear as purpura on the lower extremities. Urticaria secondary to SS related vasculitis is related to rheumatoid factors and anti-SSA/SSB antibodies.25,26 A previous study of skin manifestations associated with SS found that about 88% of patients had purpura and 8% had skin ulcers, while nodules, finger lesions, and macular papules were relatively rare. 27
Vasculitis is caused by a range of necrotic diseases and usually directly associated with skin ulcers. 28 The skin vasculature of patients with AIDs is often attacked by autoantibodies or immune T cells due to dysregulation of the autoimmune system, leading to vasculitis characterized by inflammation and necrosis of the blood vessel walls, eventually resulting in skin ischemic ulcers, tissue necrosis, and even gangrene of the limbs. 29
The most common sites of AID-related ulcers are the lower extremities and feet. A large multi-center study of more than 3300 patients with chronic wounds conducted in China reported that chronic AID-related ulcers mainly involved the lower extremities (56.1%), followed by the trunk (18.6%). 30 Due to the lack of effective treatment regimens, recurrence is a typical feature of AID-related ulcers.
In the present study, 75.1% (142/189) of wounds exhibited clinical symptoms of infection and 90% (63/70) of cultures were positive for at least one type of bacteria, which was a higher rate than reported in a previous study of 76.4% (136/178). 31 This difference might be due to the use of immunosuppressants or other biological agents, which can reduce resistance to infection. 32 In this study, the most common causes of wound infection were Staphylococcus aureus and Pseudomonas aeruginosa, which was consistent with previous reports.31,33,34 In addition, Acinetobacter baumannii and Klebsiella pneumonia were commonly encountered, which is important because these bacteria are known to be resistant to multiple antibiotics. The choice of drugs for treatment of AIDs could delay wound repair. AIDs are mostly treated with glucocorticoids and immunosuppressants. However, long-term use of glucocorticoids can inhibit the proliferation and migration of keratinocytes, and reduce the lipid bilayer of the stratum corneum of the epidermis, while inhibiting proliferation of fibroblasts, resulting in diminished collagen and elastin synthesis, rearrangement of the fibrotic network, atrophy, reduced elasticity, and decreased barrier function of the dermis. 35 The use of immunosuppressants can inhibit the immune response, thereby increasing the risk of infection, and delay wound repair.
Strengths and Limitations
A literature review found relatively few epidemiological studies on AID-related ulcers. This study included a total of 189 AID patients treated at two hospitals. These representative findings reflect the epidemic characteristics of AID-related ulcers to a certain extent and provide a basis for further intervention. As a limitation to this study, factors related to AID-related ulcers infection and recurrence were not investigated. Thus, further research in this area is warranted.
Conclusion
The results of this retrospective study clarified that the main clinical features of AID-related ulcers were spontaneous rupture, long duration, multiple lesions, bacterial infection, and recurrence. Early diagnosis and treatment of AID-related ulcers is important, new treatment strategies are urgently needed. Hence, future research should focus on clarification of the clinical characteristics and management of AID-associated ulcers to improve treatment outcomes.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Modern Hospital Management and Development Institute, Nanjing University (grant no. NDYG2022022) and the Nanjing Drum Tower Hospital Nursing Research Project, (grant number (grant no. 2022-H124).).