
Abstract
Applying infrared thermometry for temperature measurement is recommended for Charcot neuro-osteoarthropathy (CNO) diagnosis and monitoring of its course. Microwave radiometry (MWR) is used for the detection of temperature changes in human tissues. This study evaluates the agreement between these two methods in CNO assessment. Individuals with diabetes mellitus (DM) with and without active CNO were included. MWR measurements were performed by a microwave computer-based system that detects microwave radiation from the area under investigation and temperatures of the internal tissues. Sensors with diameters of 0.8 cm (MWR 0.8), 2 cm (MWR 2), and 5 cm (MWR 5) were used, with larger diameters enabling deeper tissue assessment. Nine individuals (mean age: 54.6 ± 15.7, 2 females) with active CNO and 5 people with DM without CNO were included in the study. The agreement between temperatures measured by infrared thermometry and by MWR 0.8 was high and the average temperature discrepancy between the two methods was 0.034 °C (P = .676). The average temperature discrepancy between infrared thermometry and MWR 2 was −0.323 °C (P < .001) and between infrared thermometry and MWR 5 was −0.315 °C (P = .002). Participants with active CNO were followed-up for a median period of 67 [39, 79] weeks. During follow up, the difference in skin temperature between the affected and the contralateral foot was lower than 2 °C in 7 (77.8%) participants. Three out of 5 individuals had re-activation of CNO in 21, 22 and 65 weeks after the removal of the offloading device, respectively. The decision to gradually start loading would be different only for one person if we had used MWR instead of infrared thermometry for the measurement of temperature difference between the affected and the contralateral foot. In conclusion, infrared thermometry showed high agreement with MWR 0.8 but not with MWR 2 or MWR 5.
Keywords
Introduction
Charcot neuro-osteoarthropathy (CNO) is an inflammatory process that occurs in people with diabetes mellitus (DM) and neuropathy and leads to injury to bones, joints, and soft tissues of the foot or ankle.1,2 Although epidemiological data are limited, the lifetime cumulative incidence for CNO varies from 0.4 to 1.3% in people with DM.3,4 The percentage increases to 13% among individuals who visit specialized diabetic foot clinics.3,5 The spectrum of CNO consists of active CNO and CNO in clinical remission, as well as of CNO re-activation. 1 Active CNO is defined as the presence of a red, warm, swollen foot with osseous abnormalities on imaging in a person with DM and neuropathy and first treatment approach is a non-removable knee-high device in order to immobilize and offload the affected foot until remission is achieved. 1 Several uncertainties exist, however, regarding diagnosis, monitoring, and CNO management.1,3
Various techniques have been used to assess remission in CNO and hence guide the discontinuation of immobilization, such as infrared thermometry, X-rays, magnetic resonance imaging (MRI), nuclear imaging scan (scintigraphy), computed tomography scan, and single photon emission computerized tomography (SPECT-CT).1,6 According to the latest guidelines from the International Working Group on the Diabetic Foot (IWGDF) infrared thermometry for measuring foot skin temperature should be considered to monitor disease activity despite the uncertainty over its diagnostic accuracy. 1 Microwave radiometry (MWR) is a relatively new imaging modality with the ability to detect non-invasively relative changes of temperature in human tissues at microwave frequencies. 7 Therefore, it is a method that could assess local inflammatory activation with high accuracy.7,8 Currently it is being used for detecting breast cancer, carotid plaque vulnerability and risk stratification of asymptomatic people with carotid artery stenosis.9–11
The aim of this preliminary study was to examine the degree of agreement between infrared thermometer and MWR for the assessment of foot temperature in individuals with active CNO and to further investigate which of the two methods should be preferred for the evaluation of CNO course and for the clinical decision to transition the person into footwear.
Material and Methods
Study Population
A total of 9 participants with active CNO were recruited from the Outpatient Diabetic Foot Clinic of our Hospital and 5 people with DM that were followed at the Diabetes Center of our Hospital. DM status was defined according to the American Diabetes Association (ADA) criteria. 12
Exclusion criteria included the presence of foot ulcer and any foot infection including osteomyelitis, peripheral neuropathy of cause other than DM, moderate to severe peripheral arterial disease (ankle-brachial index, ABI <0.7), prior bypass surgery or percutaneous angioplasty of the lower limbs, venous insufficiency, lower limb edema of any cause and active illness in the previous 48 h.
All individuals gave written informed consent before participating in the study, which was conducted according to the principles of the Declaration of Helsinki and approved by the Ethics Committee of our Hospital. The demographic and clinical characteristics of the study participants are shown in Table 1.
Demographic, Clinical and Biochemical Characteristics of the Study Participants.
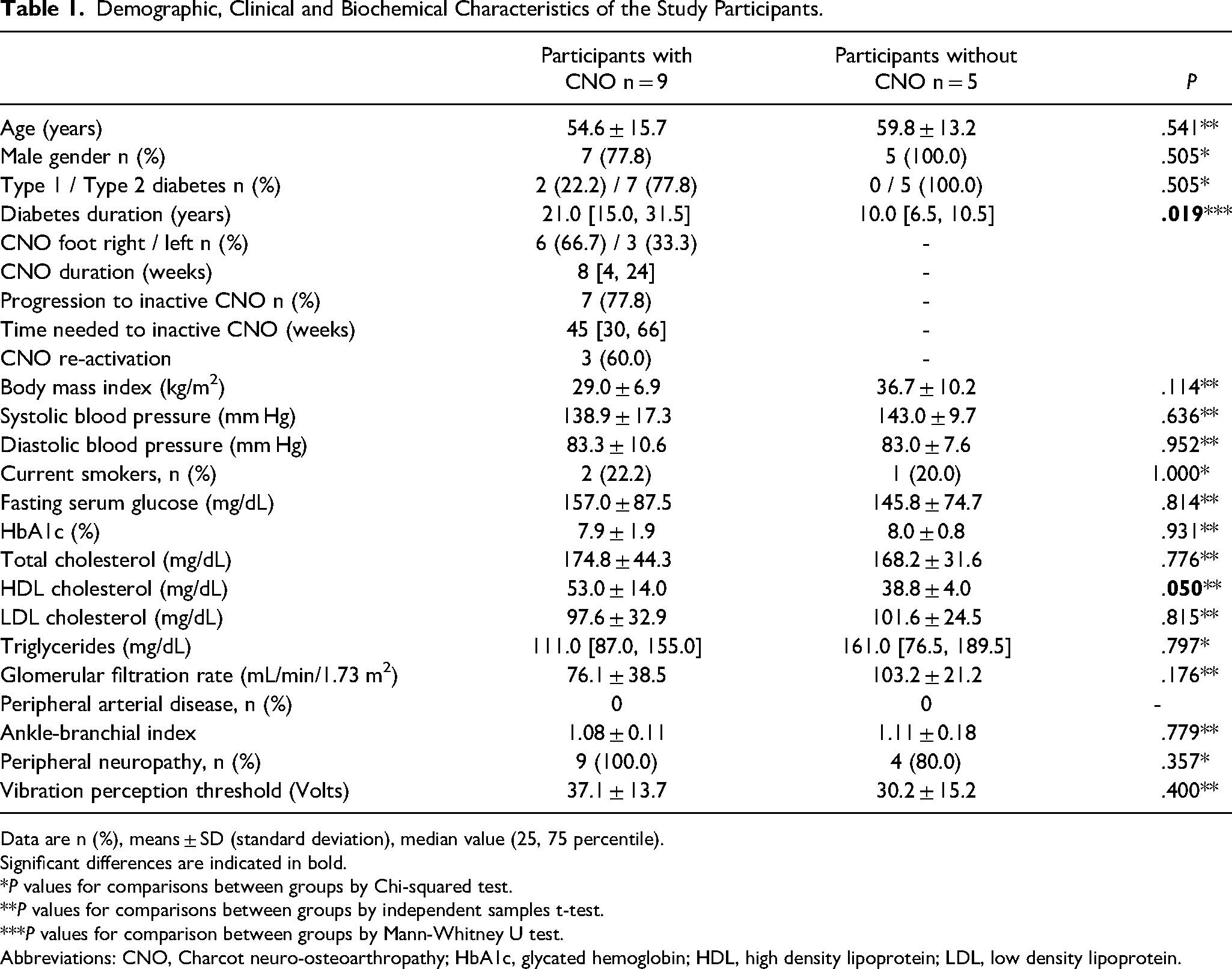
Data are n (%), means ± SD (standard deviation), median value (25, 75 percentile).
Significant differences are indicated in bold.
*P values for comparisons between groups by Chi-squared test.
**P values for comparisons between groups by independent samples t-test.
***P values for comparison between groups by Mann-Whitney U test.
Abbreviations: CNO, Charcot neuro-osteoarthropathy; HbA1c, glycated hemoglobin; HDL, high density lipoprotein; LDL, low density lipoprotein.
Methods
Active CNO was diagnosed by common clinical criteria such as abrupt onset of a red, hot, swollen foot with skin foot temperature 2 °C greater than the corresponding site on the contralateral foot and by appropriate imaging techniques.2,13 All participants underwent standard weight-bearing foot and ankle radiographs and typical radiological changes of subluxation, dislocation and fragmentation of bone were evaluated. 14 MRI was also performed to detect early signs of inflammation, the extent of bone edema and the underlying bone and joint damage when simple radiographs were normal.2,14 Magnetic resonance images of four participants with active CNO is provided in the Supplement. Offloading was recommended and removable walking casts were applied to all people that were frequently monitored. Participants were advised to always wear the offloading device.
All individuals with CNO attended the Diabetes Laboratory every 6 ± 2 weeks until the end of the study. When the swelling resolved and the skin temperature difference between the affected and the contralateral foot measured by infrared thermometry was lower than 2 °C they were advised to gradually start loading and use protective footwear and orthoses according to orthotists recommendation. Foot x-ray was also done to assess fracture healing, bone sclerosis and fusion and increased bone density. People with DM that served as controls attended the Diabetes Laboratory only once.
All measurements were performed in a room with steady temperature (20-24 °C) and after the participants have been rested in a supine position with naked feet for 15 min to equilibrate to the ambient temperature.
A detailed questionnaire was used to assess the presence of previous and current diseases, use of medications and smoking habits. Height and weight were measured in light clothing and body mass index (BMI) was calculated. Arterial blood pressure was measured using an appropriated cuff size 2 times and with the participant in the sitting position and the mean value of the measurement was used in the statistical analysis. Bilateral brachial and ankle pressures were measured using a hand-held Doppler device (doplex II, Huntleigh Healthcare LTD, Cardiff, UK) and ABI was calculated in both feet. ABI used for further analysis was the mean of the 2 measurements and PAD was defined as ABI ≤0.9. Diagnosis of diabetic peripheral neuropathy was based on neuropathy symptom score and neuropathy disability score (assessment of ankle reflexes, temperature sensation, vibration sensation and pain sensation).15,16 Vibration perception threshold (VPT) at the great toe of both feet was also assessed with a biothesiometer (Bio-Medical Instrument Company, Cleveland, OH, USA).
Blood was drawn to determine glycated hemoglobin (HbA1c), serum creatinine, lipids and inflammatory markers. The CKD-EPI 2021 formula was used to calculate estimated glomerular filtration rate (eGFR). 17
Skin Temperature
Surface skin temperature was measured twice by a hand-held infrared thermometer at the highest temperature on the affected foot and at the same anatomic point on the contralateral extremity, as recommended by the IWGDF (Fluke 64 MAX IR Thermometer, Eindhoven, the Netherlands; temperature accuracy 1%, with 20:1 distance to spot ratio, according to the manufacturer). 18 The temperature of each point used for further analysis was the mean of the two measurements. The temperature difference between both legs was then calculated.
Cutaneous temperatures of both the affected and contralateral foot were measured during follow-up visits, conducted every 1-2 months. Surface skin temperatures of both feet of DM participants were measured at the same location at the midfoot on one visit and the difference was calculated.
Internal Temperature
MWR is based on the principle that any object with a temperature above zero emits radiation at all frequencies and in particular at microwave frequencies and that the intensity of the radiation is proportional to the temperature of tissue. 19 Measurements were performed by a microwave computer-based system (RTM-01-RES, Bolton, UK). MWR device has an antenna with a microwave sensor that detects microwave radiation from the area under investigation and temperatures of the internal tissues with an accuracy of ±0.2 °C at various depths depending on the diameter of the sensor used.8,9,11,20 Previous studies have shown that the use of MWR showed good intra- and inter-class correlation coefficients, 0.94 and 0.93, respectively, indicating perfect agreement. 8
Sensors with 0.8 cm diameter (MWR 0.8), 2 cm diameter (MWR 2) and 5 cm diameter (MWR 5) were used for the study.9,11 For measuring the internal temperature, the antenna was placed on the point of the affected foot with the highest temperature. The hottest point on the affected foot was identified using the infrared thermometer. The entire antenna surface was in contact with the naked skin at 90° angle for 10 s (Figure 1). The temperature displayed in the indicator as degrees Celsius was recorded. The internal temperature was also measured at the corresponding point of the contralateral foot and the difference was calculated. The internal temperatures of the affected and the contralateral foot were measured during follow-up visits every 1-2 months.
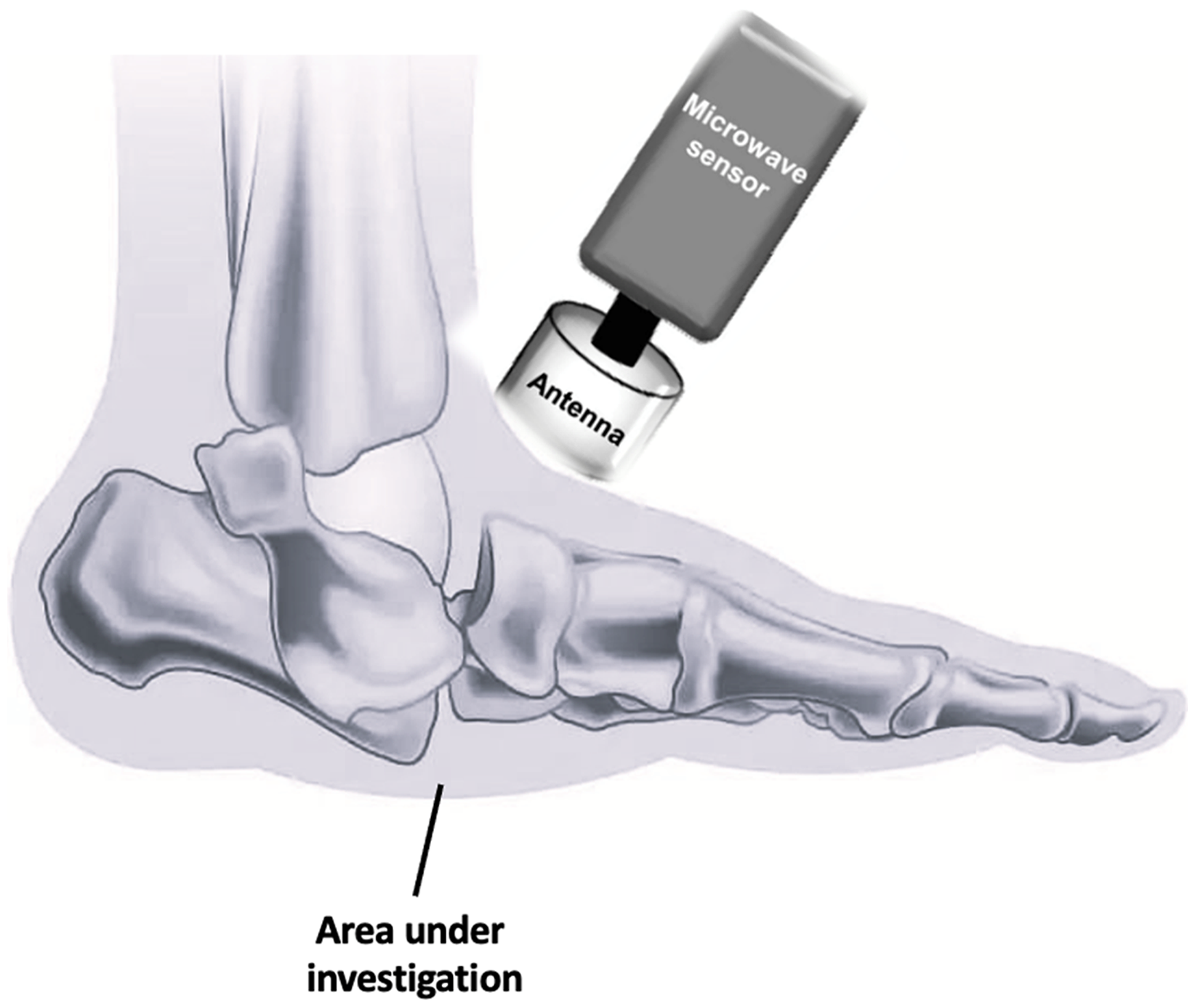
The microwave radiometry system. The antenna for microwave radiometry device placed over the joint.
Internal temperatures of both feet of DM participants were measured at the same location at the midfoot on one visit and the difference was calculated. All temperature measurements were performed 2 times to assess the reproducibility of the method. The temperature of each point used for further analysis was the mean of the two measurements.
Statistical Analysis
The Statistical Package for the Social Sciences (IBM SPSS software version 24.0 for Windows, Armonk, NY, USA) and the MedCalc statistical software (Version 18.9 for Windows, Brussels, Belgium) were used for analyses. The Kolmogorov-Smirnov test was used to test the variable for normal distribution of the data. Chi-square test was used to assess differences between categorical variables, while the student's t-test and the Mann-Whitney test were used to assess differences in parametric and non-parametric continuous variables between the studied groups. Bivariate correlations for continuous variables were tested using Spearman's correlation coefficient.
Bland-Altman plots were used to assess the agreement between infrared thermometry and MWR. For the Bland-Altman plots all measurements performed with the infrared thermometry and the MWR during the study were included. Clinically significant difference between temperatures measured by infrared thermometry and by MWR was defined as a value of ≥0.3 °C before data analysis to avoid any bias in decision. We decided on this value based on the accuracy of MWR and on the clinical criterion of 2 °C temperature difference between the affected and contralateral foot that is used for CNO diagnosis and resolution.
P values <.05 (two-tailed) were considered statistically significant.
Results
A total of 9 individuals with active CNO participated in the study and were seen in the outpatient clinic every 6 ± 2 weeks. Participants were followed-up for a median period of 67 [39, 79] weeks. Τhe median duration that participants reported red, hot and swollen foot was 8 [4, 24] weeks prior to attendance and inclusion in the study. All participants had stage II CNO according to modified Eichenholtz classification system. 21 Five enrollees with DM but without CNO were also included in the study and temperatures were measured on one visit. Participants with DM but without CNO did not differ in terms of age and gender with those with CNO, but they had shorter DM duration. The demographic and clinical characteristics of the study participants are presented in Table 1.
The baseline foot temperatures measured by infrared thermometry and MWR are shown in Table 2. The performance of MWR 0.8, MRW 2 and MWR 5 using the clinical criterion of 2 °C difference between the affected and contralateral foot when compared with infrared thermometry is shown in Table 3.
Foot Temperatures of the Study Participants at Baseline.
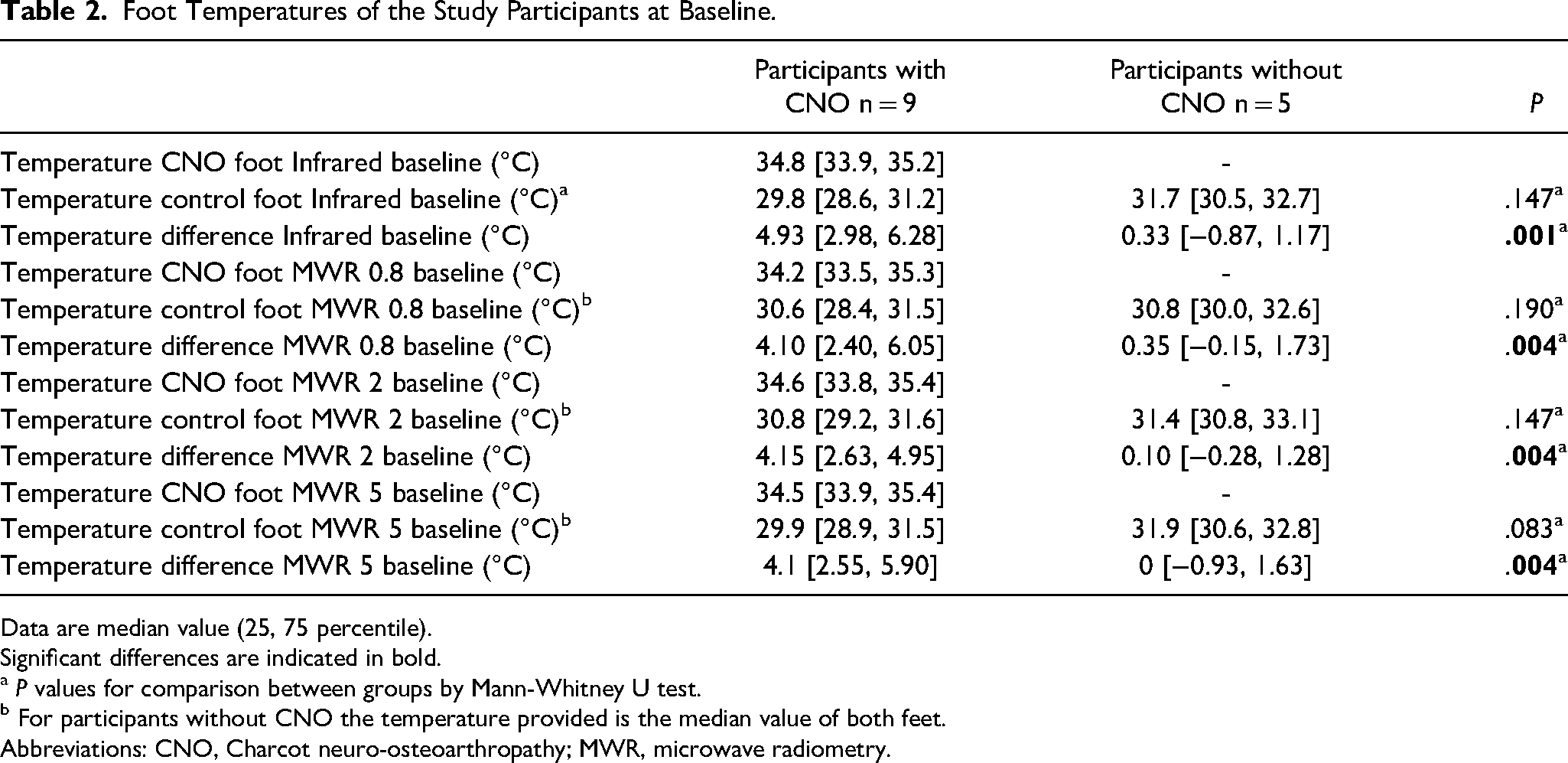
Data are median value (25, 75 percentile).
Significant differences are indicated in bold.
a P values for comparison between groups by Mann-Whitney U test.
b For participants without CNO the temperature provided is the median value of both feet.
Abbreviations: CNO, Charcot neuro-osteoarthropathy; MWR, microwave radiometry.
The Performance (Value, 95% Confidence Intervals) of MWR 0.8, MRW 2 and MWR 5 for the Diagnosis of CNO When Compared with Infrared Thermometry.

a All P values <.001; Abbreviations: AUC, area under the curve; PPV, positive predictive value; NPV, negative predictive value.
When all measurements performed with infrared thermometry and the MWR during the study were included in the CNO cohort (60 participants visits/measurements), there were significant correlations between temperature differences measured by infrared thermometry and MWR 0.8 (Spearman r = 0.959), MWR 2 (Spearman r = 0.965) and MWR 5 (Spearman r = 0.884) (all P < .001). Among the DM without CNO cohort, we found significant correlations between temperature differences measured by infrared thermometry and MWR 0.8 (Spearman r = 1.000, P < .001) and MWR 2 (Spearman r = 0.900, P = .037), but no with MWR 5 (Spearman r = 0.300, P = .624).
The agreement between temperatures measured by infrared thermometry and by MWR 0.8 was high as shown by Bland-Altman plots and the average temperature discrepancy between the two methods was 0.034 °C (P = .676, lower limit of agreement = −1.700 and upper limit = 1.769) (Figure 2). The Bland-Altman plots of agreement between temperatures measured by infrared thermometry and MWR 2 and 5 are shown in Figure 2. The average temperature discrepancy between infrared thermometry and MWR 2 was −0.323 °C (P < .001, lower limit of agreement = −1.788 and upper limit = 1.141) and between infrared thermometry and MWR 5 was −0.315 °C (P = .002, lower limit of agreement = −2.356 and upper limit = 1.727).
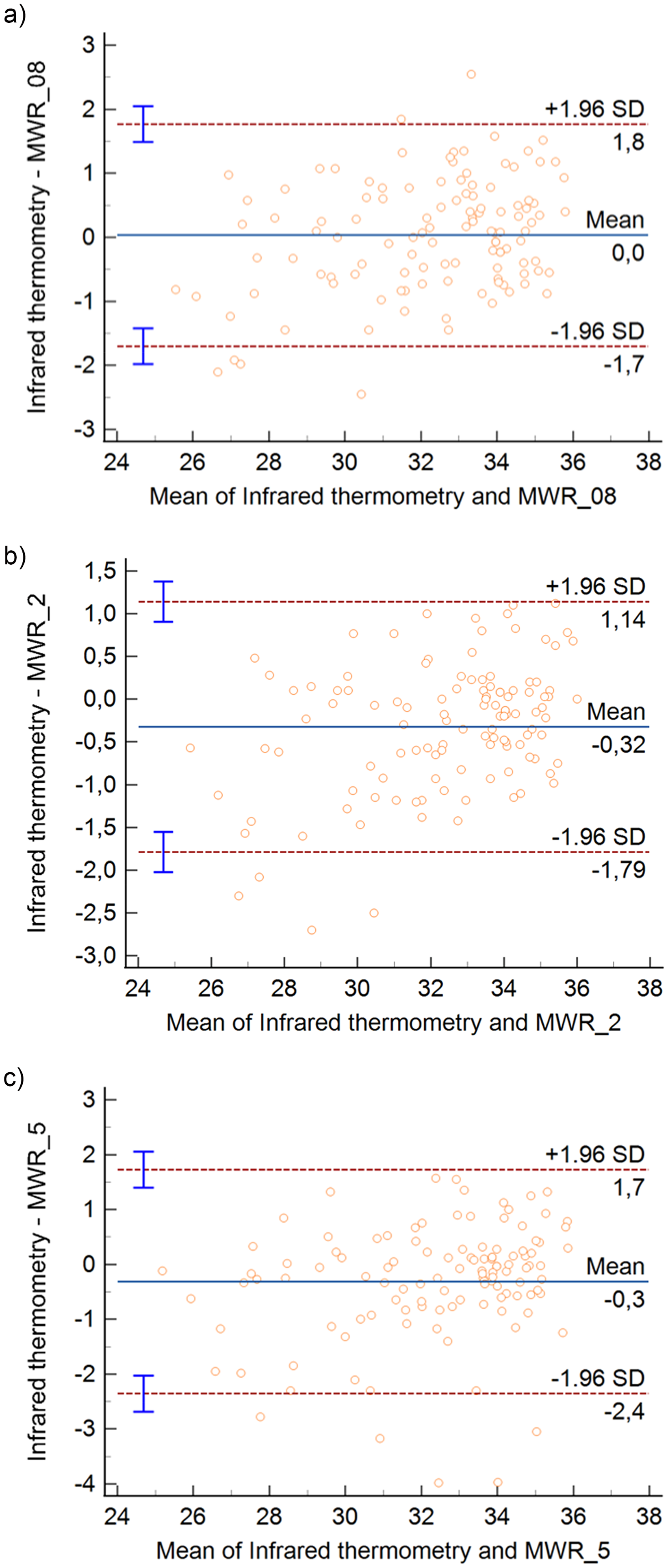
The Bland-Altman plots show the agreement between the foot temperatures measured by infrared thermometry and by MWR 0.8 (A), MWR 2 (B) and MWR 5 (C) in patients with Charcot neuro-osteoarthropathy. The middle horizontal continuous line depicts mean difference between the 2 measurements techniques, and the outer dashed lines represent the 95% confidence interval for both the upper and lower limits of agreement.
During follow-up, the swelling was resolved and the skin temperature difference between the affected and the contralateral foot became lower than 2 °C in 7 out of the 9 participants with active CNO (77.8%), while the median time to remission was 45 [30, 66] weeks from CNO diagnosis. The temperature difference became lower than 2 °C at the last follow-up visit in 2 participants, while 3 out of the remaining 5 participants had a CNO reactivation (60%) at 21, 22 and 65 weeks, respectively, after the end of the removable cast treatment.
We further examined the data of those 5 participants and looked whether the use of the same criterion (temperature difference between the affected and the contralateral foot lower than 2 °C) measured by MWR would change our decision regarding loading. The decision to gradually start loading would be different only for one person, for whom the skin temperature difference was 1.8 measured by infrared thermometry and 2.0 measured by MWR 0.8 and MWR 2.
Discussion
In this prospective study we found high agreement rates in monitoring of active CNO between the infrared thermometry and the MWR 0.8, but not with MWR 2 and MWR 5. This makes sense since infrared thermometry measures skin temperature and MWR 0.8 measures the most “superficial” internal temperature, while both MWR 2 and MWR 5 measure temperature at deeper depths. However, given the lack of evidence about the accuracy of infrared thermometry as well as its efficiency for CNO monitoring, it could be possible that deeper temperatures measured by MWR could be more clinically useful for monitoring CNO and detecting remission.
The first microwave radiometers were used in the 1970s on satellites to measure sea surface temperature.7,8 In 1975, Barrett and Myers demonstrated that the microwave radiometer technology can be applied to medicine; MWR was used to noninvasively detect temperature changes in interior tissues leading to the diagnosis of breast cancer. 19 Lately, MWR has been used in a large spectrum of medical disorders including rheumatoid arthritis for the evaluation of in-depth temperature inflammation of small joints,8,11 synovial inflammation, 22 carotid artery disease for the detection of inflammatory atherosclerotic plaque,9,10,20 critical limb ischemia in people with diabetic foot ulcers, 23 brown adipose tissue activity, 24 as well as urological diseases including acute pyelonephritis, renal colic, inflammatory diseases of the prostate and vesicoureteral reflux.25,26 It represents a safe, noninvasive method that determines the in vivo temperature of internal tissues since microwave sensing depths of up to 7 cm below skin surface are achievable. 11 The main advantages of MWR are the non-invasive nature of the test, the lack of radiation, the low cost when comparing with other methods that assess deep tissue functionality as functional magnetic resonance imaging (fMRI), and the lack of need for consumables. 7 According to our knowledge this is the first time that MWR is used for the assessment of CNO.
CNO is a is a specific manifestation of neuropathy and is mainly found in individuals with DM and neuropathy.2,4 Several recommendations on CNO are included in guidelines from different countries for DM management or diabetic foot management, however, the first guidelines that focus on CNO and define the terms “CNO”, “active CNO”, “CNO in clinical remission”, “re-activation of CNO” were published on May 2023 by the IWGDF. 1 The diagnosis of active CNO requires high degree of suspicion and is based mainly on person's medical history, clinical examination, and imaging methods. The use of infrared thermometry with a standardized approach to the measurement of temperatures to allow for more accurate comparison over time is recommended for both diagnosis and monitoring of CNO activity. 1 Imaging methods such as x-rays, MRI, scintigraphy, computed tomography scan, or SPECT-CT could also be used. 1
The IWGDF guidelines define CNO in clinical remission as “the absence of clinical signs of inflammation, with or without deformity, and radiographic consolidation of fractures, if present, on plain X-ray”. 1 Several clinical trials and case series have reported that the average treatment duration for the full resolution of CNO ranges from 2 to 12 months, with a 6-month period being the most frequently reported.27–30 In our study the median time to remission was around 11 months, which is longer than usually reported. However, all participants in our study had already osseous abnormalities on x-ray when presented in our Unit and most importantly removable offloading devices were used by individuals and not non-removable which are considered the first choice of CNO management due mainly to “forced” compliance.
Nevertheless, uncertainties exist regarding the identification of remission of CNO, which guides the discontinuation of immobilization of the affected foot.1,3,31 A systematic review that was published in 2020 aimed to identify the techniques used in the monitoring of CNO, and evaluate whether different techniques used for monitoring affect the outcomes of CNO. 6 A total of 29 studies with 1132 participants were included in the analysis with 1239 episodes of CNO. Authors conclude that the quality of the studies was low, the risk of bias was high and overall there is a lack of a consistent approach to monitoring in CNΟ. 6 Seven of the twenty-nine studies aimed to assess monitoring techniques, while twenty-two were observational studies that reported treatment outcomes and described the monitoring techniques used to assess the CNO.
In the first study that examined monitoring techniques, a total of 40 people with active CNO were enrolled. 32 MRI was compared to clinical examination that included skin temperature with a handheld infrared temperature scanner and foot circumference. The study demonstrated that the contrast medium uptake rate obtained with dynamic-MRI represents a reliable technique for predicting remission in active CNO. 32
Two studies examined infrared thermometry to identify CNO remission.30,33 In the study by Moura-Neto et al, twenty-eight individuals with active CNO were recruited and temperature was measured using an infrared surface skin scanner. 30 Temperature was measured at seven sites on the foot and values were compared with the contralateral limb every month. The use of cast was discontinued when a reduction/absence of clinical signs of inflammation or radiologic signs of healing were reported as well as when the temperature difference between feet had stabilized with a cut-off point of less than 4 °F (2.2 °C) difference. The authors concluded that skin temperature is a good tool to guide safe immobilization withdrawal. 30 Armstrong and Lavery used another infrared thermometer to measure temperature in people with CNO. 33 Overall, thirty-nine participants presenting with active CNO were recruited. Casting was discontinued when the temperature difference between feet was recorded as less than 2 °C.
In the study by MgGill et al 17 individuals with active CNO were monitored using skin temperature of affected and unaffected feet at baseline and every 3 months for 12 months. 34 Among them, eight participants underwent a three-phase quantitative bone scan at baseline and 3 monthly for 12 months. The ratio of isotope uptake between feet, between the affected foot and the tibia was compared with the clinical indicators of inflammation. There was strong association between temperature difference and the ratio of isotope uptake in the affected versus unaffected foot, the perfusion of the affected foot in the dynamic phase and the isotope uptake in the delayed phase of the bone scans. 34
In 22 observational studies that reported treatment outcomes and described the monitoring techniques used to assess CNO the commonest monitoring techniques used was serial x-ray (16/22 studies), objective temperature measurement with a handheld infrared monitoring device (11/22 studies) and MRI with or without contrast media (7/22 studies). 6 Other diagnostic methods used consist of F-FDG PET/CT scanning, bone scintigram, bone biopsies and isotope bone scans. 6
Regarding skin temperature, the diagnostic accuracy of infrared thermometry to monitor and diagnose remission in CNO is questionable. 3 A contralateral temperature difference of 2 °C or 4 °F (equivalent to 2.2 °C) for 2-4 consecutive weeks before transitioning individuals from cast immobilization to a removable walker or appropriate footwear is used in most studies.1,27 Moreover, the effect of the difference from 2.2 °C to 2 °C on outcomes has not been investigated. 3 A recent systematic review by Jones et al aimed to examine how contralateral temperature difference has been used to monitor healing in CNO in people with type 1 or 2 DM or to assist with the decision-making process around immobilization. 35 A total of 15 studies were included in the meta-analysis. The average contralateral temperature difference at presentation varied from 1.6 to 8.0 °C, quite similar to our study [median infrared temperature difference 4.93 (2.98-6.28 °C)]. There were not enough data to examine whether the contralateral temperature difference was proportional to the severity of CNO. 35 The threshold of contralateral temperature difference used for the discontinuation of immobilization ranged from <1 °C to <2 °C. Most frequently it was <2 °C sustained for 2-3 visits.
MWR is a new device that could overcome some limitations of the infrared thermometer for CNO monitoring. Firstly, it is a relatively new device which measures temperature in several depths. The change in temperature occurs firstly in the deep tissue of the feet and then in the skin. Therefore, the MWR may detect faster changes in the temperature of CNO when compared with skin temperature. Herein we found that the agreement between infrared thermometry and MWR 0.8 was high, but this was not the case when infrared thermometry was compared with MWR 2 and MWR 5. MWR 0.8 measures temperature in less deep surface than MWR 2 and MWR 5, similar to the infrared. A temperature difference of 0.323 °C or 0.315 °C could be clinically significant when evaluating a person with CNO to define the most appropriate time point for starting foot loading. Since currently the cut-off point for starting loading in an individual with CNO is a temperature difference between the affected and the contralateral foot lower than 2 °C, a temperature discrepancy of 0.323 °C between two different methods of assessment could lead to different treatment decisions. Secondly, infrared thermometry devices used for CNO are not validated for the range of temperature measurements recorded on feet as opposed to core body temperatures which many of these devices were originally designed to measure. 3 It should be emphasized though, that the 2 °C temperature difference threshold for defining CNO remission is not evidenced based and this is the case for both infrared thermometry and MWR.
In addition, in our study, 3 out of 5 (60%) participants had a re-activation of CNO at 21, 22 and 65 weeks after the end of the removable cast treatment, respectively. Previous studies have shown that re-activation of CNO occurs in 15%-30% of people with a previous history of CNO.27,28,36 In these 5 participants, we evaluated whether the use of the same criterion (temperature difference between the affected and the contralateral foot lower than 2 °C) measured by MWR would change the decision regarding loading. The decision to gradually start loading would be different only for one person, for whom the skin temperature difference was 1.8 measured by infrared thermometry and 2.0 measured by MWR 0.8 and MWR 2. If the sample size of our study was larger the number of people who would proceed tothe stage of remission according to MWR might be lower when compared to skin temperature and lower numbers of re-activation of CNO could be recorded.
The main strength of the study is the long follow-up of people with CNO. The main limitation of the study was the non-availability of total contact cast in our Diabetic Foot Clinic and the relatively low accuracy of the infrared thermometer used. In addition, the sample size of people with CNO was small and safe conclusions regarding the differences between individuals with and without CNO recurrence could not be drawn. Moreover, MWR is a relatively new tool for the assessment of the temperature of internal tissues and validation data are still limited.
Conclusions
The difference between the two techniques is that infrared radiation comes from a shallow depth and represents the surface temperature, while temperature measured by MWR represents the deep temperature. Agreement between infrared thermometry and MWR 0.8 was high, but this was not the case when infrared thermometry was compared with MWR 2 and MWR 5. Nevertheless, whether skin or deeper tissue temperature should be measured to diagnose or monitor CNO remains to be determined in further clinical studies.
Supplemental Material
sj-docx-1-ijl-10.1177_15347346251329733 - Supplemental material for Reliability of Microwave Radiometry for the Assessment of Charcot Foot
Supplemental material, sj-docx-1-ijl-10.1177_15347346251329733 for Reliability of Microwave Radiometry for the Assessment of Charcot Foot by Ioanna Eleftheriadou, Anastasios Tentolouris, Ourania Kosta, Paraskevi Kontrafouri, Maria Tektonidou, Petros P Sfikakis and Nikolaos Tentolouris in The International Journal of Lower Extremity Wounds
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
All individuals gave written informed consent before participating in the study, which was conducted according to the principles of the Declaration of Helsinki and approved by the Ethics Committee of our Hospital.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.