
Abstract
The optimal method for assessing residual osteomyelitis after conservative surgery for diabetic foot infection remains controversial. Microbiological cultures are frequently used due to their rapid turnaround and utility in guiding antibiotic therapy, but their diagnostic reliability is uncertain. This study compared microbiological cultures and histopathology in evaluating bone resection margins, using histopathology as the gold standard. We included 93 patients undergoing conservative surgery for diabetic foot osteomyelitis. Bone samples were obtained from the proximal resection margin for both microbiology and histopathology. A microbiological result was considered contamination when cultures were positive but histopathology was negative. Microbiological cultures at bone resection margins yielded 52 true positives, 23 false positives (contamination), 10 false negatives, and 8 true negatives when compared to histopathology. This resulted in a sensitivity of 83.9%, specificity of 25.8%, positive predictive value of 69.3%, and negative predictive value of 44.4%. Contamination was not associated with the severity of infection, presence of soft tissue involvement, inflammatory markers, or glycemic control. No association was found between contamination and polymicrobial flora in the primary surgical specimen. However, Pseudomonas aeruginosa was the only species significantly associated with contamination (p = .008), suggesting species-specific factors may contribute to microbiological false positives. These findings emphasize that microbiology, while sensitive, is not a specific method for assessing residual bone infection and should not be used in isolation. Histopathology remains the more reliable diagnostic tool. Future research should explore biofilm-targeted strategies and intraoperative antiseptic protocols to reduce contamination of bone biopsy specimens obtained from resection margins.
The optimal method for diagnosing diabetes-related foot osteomyelitis remains controversial. Specifically, there is ongoing debate over whether histopathology or microbiology should be considered the gold standard for confirming bone infection. This controversy is particularly relevant when comparing percutaneous and surgical bone biopsies. In percutaneous biopsies, microbiological analysis is generally reliable because the sample is obtained through intact skin, minimizing the risk of contamination. 1 However, percutaneous biopsies often yield limited tissue, which may be insufficient for histopathological evaluation. In such cases, microbiology provides a definitive diagnosis and enables targeted antibiotic therapy based on susceptibility testing. In contrast, surgical bone biopsies present a higher risk of contamination due to their proximity to infected soft tissues.2,3 This risk is particularly concerning when analyzing bone resection margins, as intraoperative sampling may capture bacteria from surrounding tissues rather than reflecting true bone infection. 4 Consequently, positive cultures from resection margins may not reliably indicate residual osteomyelitis but rather contamination from adjacent soft tissue infection. This raises the question of whether histopathology should be the preferred method for evaluating bone resection margins. However, histopathology also has limitations: it requires several days for processing, delaying clinical decision-making, and its interpretation may vary among pathologists, 5 particularly in centres with limited experience in diabetic foot osteomyelitis. These factors complicate the choice between microbiology and histopathology for guiding postoperative treatment decisions.
Given these considerations, we hypothesize that histopathology is more reliable than microbiology for detecting osteomyelitis in the residual stump after conservative surgery for diabetic foot osteomyelitis, as microbiological analysis is prone to false-positive results, likely due to contamination from bacterial flora persisting in the surgical wound. Furthermore, we hypothesize that this contamination may be associated with polymicrobial infections isolated from the primary surgical specimen.
Methods
This study is based on a previously published prospective cohort of patients who underwent conservative surgery for diabetic foot osteomyelitis. 6 Patients were treated at the Diabetic Foot Unit at San Juan de Dios Hospital (San José, Costa Rica), where all procedures were performed by the same surgical team following a standardized approach. The original study assessed the impact of residual osteomyelitis at resection margins on infection recurrence and healing outcomes. The present analysis specifically focuses on evaluating the diagnostic performance of microbiology versus histopathology for assessing bone resection margins and identifying factors associated with microbiological positivity. For patient selection, we exclusively included individuals who underwent conservative surgery as the first attempt to treat diabetic foot osteomyelitis. Conservative surgery was defined as bone resection preserving as much foot structure as possible without performing a minor amputation. 7 Regarding the classification of osteomyelitis and soft tissue infection, cases were categorized into three groups: OM1, corresponding to osteomyelitis without associated soft tissue infection; OM2a, referring to osteomyelitis with deep abscess, extensive cellulitis, or skin necrosis; and OM2b, describing osteomyelitis detected during the healing process after an initial soft tissue infection. In OM2b cases, the patient initially underwent surgical debridement due to a presumed soft tissue infection, as osteomyelitis was not suspected at the time of the initial intervention. 6 Once osteomyelitis was later identified, conservative surgery was performed electively to remove the infected bone. The presence of soft tissue infection was considered a potential confounding factor for microbiological positivity at resection margins. For the surgical procedure and sample collection, after resecting the infected bone, the wound was thoroughly irrigated with 1 to 2 litres of saline solution. To minimize contamination, the surgeon changed gloves and used a sterile bone nibbler to obtain an additional bone sample from the proximal resection margin, which was macroscopically healthy. This sample was then divided into two portions: one for microbiological analysis and the other for histopathology. Bone samples obtained from the proximal resection margin were divided for microbiological and histopathological analysis. Microbiological cultures were performed exclusively on bone tissue under aerobic conditions using standard laboratory procedures. Histopathological evaluation, also conducted on bone tissue, was carried out by a single pathologist using predefined criteria for the diagnosis of osteomyelitis. 7
False-positive results were defined as cases where histopathology was negative but microbiology was positive. These cases were assumed to represent contamination, and a specific variable was created to analyze its association with clinical and microbiological factors. Regarding the microbiology of the primary surgical specimen, different variables were established: polymicrobial infection was defined as the presence of two or more aerobic bacterial species, while Gram-negative infection was recorded when at least one Gram-negative species was isolated. Additionally, for each of the six most frequently isolated bacteria in the cohort (Staphylococcus aureus, Proteus mirabilis, Streptococcus agalactiae, Enterococcus faecalis, Escherichia coli, and Pseudomonas aeruginosa), an individual binary variable was created (1 = present, 0 = absent). The clinical variables and outcome assessment included HbA1c levels, presence of peripheral arterial disease (PAD), inflammatory markers, and severity of infection according to the International Working Group on the Diabetic Foot (IWGDF) criteria. Additionally, the presence of contamination at bone resection margins was analyzed in relation to the type of osteomyelitis, distinguishing between cases with and without associated soft tissue infection.
Statistical Methods
Descriptive statistics were used to summarize the characteristics of the study population. Categorical variables were expressed as absolute frequencies (n) and percentages (%). Continuous variables were assessed for normality using the Shapiro-Wilk test. Variables with a normal distribution were presented as mean and standard deviation (SD), while non-normally distributed variables were reported as median and interquartile range (IQR). Comparisons between groups were performed using appropriate statistical tests. For categorical variables, the chi-square test (χ²) or Fisher's exact test was applied, depending on the expected frequencies. For continuous variables, normally distributed data were compared using the Student's t-test, whereas non-normally distributed variables were analyzed with the Mann-Whitney U test.
To evaluate the diagnostic performance of microbiological analysis at resection margins, histopathology was considered the gold standard for detecting residual osteomyelitis. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and overall diagnostic accuracy were calculated. False-positive microbiological results were considered contamination, and their association with clinical and microbiological factors was analyzed using the chi-square test (χ²) or Fisher's exact test. The categorical variables assessed included the presence of soft tissue infection, severity of infection, sex, presence of PAD, and microbiological variables, including polymicrobial infection, Gram-negative bacteria, and the presence of any of the six most frequently isolated bacteria in the cohort (Staphylococcus aureus, Proteus mirabilis, Streptococcus agalactiae, Enterococcus faecalis, Escherichia coli, and Pseudomonas aeruginosa) in the microbiological culture of the primary surgical specimen. A p-value < .05 was considered statistically significant. All analyses were performed using jamovi software for macOS [The jamovi project (2021). jamovi (Version 1.6) Computer Software]. Retrieved from https://www.jamovi.org.
Ethics Statement
This study was conducted in accordance with the principles of the Declaration of Helsinki, as revised in 2008. All patients provided written informed consent for the collection of additional bone specimens from resection margins and for the inclusion of their anonymized clinical data in the research database. As this was an observational, non-interventional study that did not modify or extend the standard protocol of care, the Ethics Committee of San Juan de Dios Hospital (Caja Costarricense de Seguro Social), San José, Costa Rica, approved the study protocol (HSJD-CEC-SE 23-2020; n° 11-2020) and determined that no additional consent was required.
Results
The study included a cohort of 93 patients with a mean age of 59.5 years (SD 12.6, range 28-89). Most patients were men (72, 77.4%), while 21 (22.6%) were women. The median duration of diabetes mellitus (DM) was 15 years (IQR: 10-20). Glycemic control was generally poor, with a median HbA1c of 9% (74.9 mmol/mol, IQR: 7.6-10.9% / 59.6-95.1 mmol/mol). A history of prior foot amputation was reported in 36 patients (38.7%). Osteomyelitis without associated soft tissue infection (OM1) was identified in 44 patients (47.3%). Cases presenting with active soft tissue involvement—defined as deep abscess, extensive cellulitis, or necrosis (OM2a)—accounted for 21 patients (22.6%). In 28 cases (30.1%), osteomyelitis was diagnosed during the wound healing process after prior soft tissue infection and initial debridement (OM2b). PAD was diagnosed in 19 patients (20.4%), of whom 7 (7.5% of the total cohort) underwent a revascularization procedure during the current episode.
Microbiological growth was detected in the main resected specimen in 83 out of 93 cases (89.2%). Among these, 42 cases (50.6%) were monomicrobial, while 41 (49.4%) exhibited polymicrobial flora. The bacterial species isolated from both the primary surgical specimen and the bone resection margins are detailed in Table 1, which also includes the number and proportion of isolates associated with false-positive results defined as positive bone margin cultures in the absence of histopathological confirmation of osteomyelitis.
Microbiological Findings in the Primary Resected Specimen and Bone Margins.
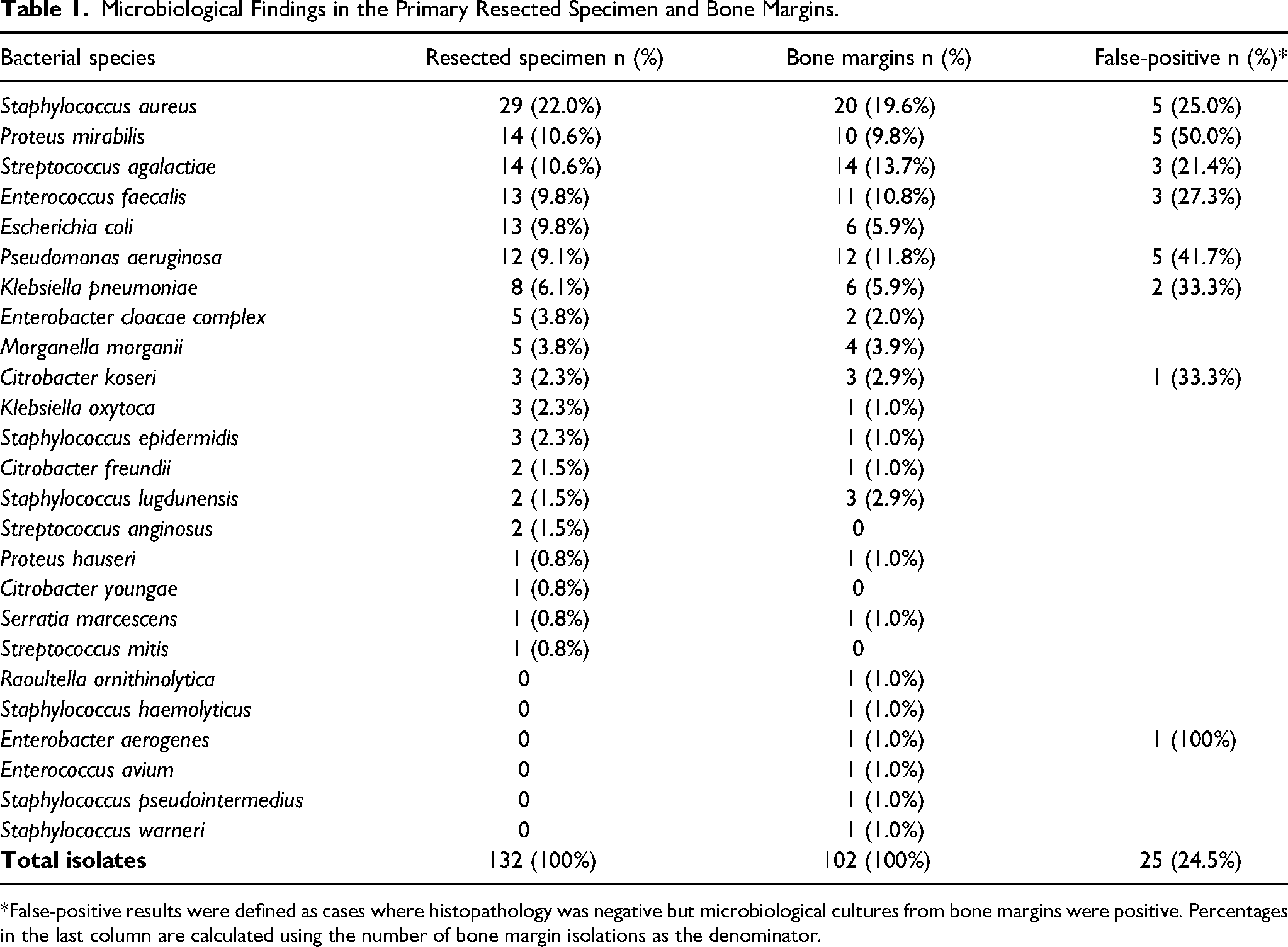
*False-positive results were defined as cases where histopathology was negative but microbiological cultures from bone margins were positive. Percentages in the last column are calculated using the number of bone margin isolations as the denominator.
Microbiological cultures from bone resection margins were positive in 75 of 93 cases (80.6%), while histopathology confirmed residual osteomyelitis in 62 cases (66.7%). Concordant results between both methods were observed in 60 cases, including 52 true positives and 8 true negatives. There were 23 false positives—defined as cases with positive microbiological cultures but negative histopathology, interpreted as intraoperative contamination—and 10 false negatives. Based on these findings, microbiological analysis demonstrated high sensitivity (83.9%) but low specificity (25.8%). The PPV was 69.3%, while the NPV was 44.4%. The overall diagnostic accuracy was moderate (64.5%), reinforcing that, despite its high sensitivity, microbiology remains an unreliable standalone tool for diagnosing residual osteomyelitis at bone resection margins.
We assessed potential factors contributing to false-positive microbiological results, including the presence of polymicrobial infections in the primary surgical specimen. No significant association was found between polymicrobial flora and contamination at bone resection margins (p = .946), suggesting that multiple bacterial species in the primary specimen do not increase the likelihood of false-positive results. When assessing individual bacterial species, Pseudomonas aeruginosa was the only pathogen significantly associated with contamination at bone resection margins (p = .008). No association was found between contamination and the presence of macroscopically evident soft tissue infection (OM2a or OM2b, p = .584), indicating that false-positive microbiological results were not influenced by the initial classification of soft tissue involvement.
Additionally, contamination was not associated with the severity of infection according to the IWGDF classification or with the presence of PAD (p > 0.05). Similarly, no significant differences were observed between contaminated and non-contaminated cases in terms of white blood cell count, erythrocyte sedimentation rate, C-reactive protein levels, or glycated hemoglobin (p > 0.05 for all comparisons).
Discussion
Our study highlights a high rate of false-positive microbiological results at bone resection margins following conservative surgery for diabetic foot osteomyelitis. This finding raises concerns about the reliability of microbiological cultures in distinguishing true residual infection from intraoperative contamination. While we initially hypothesized that contamination would be associated with polymicrobial infections in the primary surgical specimen, our analysis did not confirm this relationship. Instead, contamination at the resection margins appeared independent of the presence of multiple bacterial species in the primary bone sample. However, Pseudomonas aeruginosa was the only bacterial species significantly associated with false-positive cultures at bone margins. This suggests that, rather than being a generalized consequence of polymicrobial infections, contamination might be influenced by specific bacterial characteristics. P. aeruginosa's resilience in hospital environments and resistance to surgical irrigation suggest that its presence in the primary specimen may increase the risk of intraoperative contamination. Importantly, the contamination rate was not associated with the presence of soft tissue infection (OM2a/OM2b) or with markers of infection severity, reinforcing the hypothesis that microbiological positivity at resection margins often reflects contamination rather than true osteomyelitis.
The diagnostic performance of microbiological cultures at bone resection margins underscores their limitations in accurately identifying residual osteomyelitis. Although microbiology is highly sensitive, its poor specificity results in a significant proportion of false-positive findings, complicating clinical decision-making. A positive culture may indicate contamination rather than true infection, whereas a negative result does not reliably exclude persistent osteomyelitis. This diagnostic uncertainty raises concerns about the potential for overtreatment with unnecessary antibiotic therapy or, conversely, the risk of under-treatment if negative cultures are misinterpreted as definitive evidence of infection clearance. These findings confirm that microbiology alone is insufficient for assessing bone resection margins, reinforcing histopathology as the superior diagnostic tool. However, the delayed availability of histopathological results remains a challenge for timely surgical and antimicrobial decision-making.
Several studies have questioned the reliability of microbiological cultures from resection margins. A pilot study analyzing bone margin cultures found that microbiological positivity reached 71.4%, while histopathology confirmed osteomyelitis in only 25% of cases. 4 Despite this, most patients had favorable clinical outcomes, suggesting that positive microbiological margins do not necessarily indicate residual osteomyelitis and may lead to unnecessary prolonged antibiotic therapy. 8 Another study evaluating the predictive value of histopathological and microbiological margins reported that histopathology-negative margins were associated with lower recurrence rates and reduced antibiotic exposure, reinforcing the role of histopathology as a more reliable diagnostic tool. 9 A systematic review and meta-analysis further supports this notion, concluding that residual osteomyelitis after surgery is associated with worse clinical outcomes, 10 but emphasizing that the criteria for defining residual disease remain controversial. 10 Our findings further refine this debate, demonstrating that microbiological positivity at resection margins does not necessarily indicate persistent infection, but rather may reflect intraoperative contamination, particularly in the presence of P. aeruginosa.
The clinical significance of positive bone margins remains a controversial issue. A retrospective analysis found no significant difference in osteomyelitis remission rates between cases with positive versus negative histopathologic margins, questioning the need for prolonged antibiotic therapy in certain cases. 11 Similarly, another study suggested that while positive margins are associated with an increased need for reoperation, they do not universally lead to treatment failure, reinforcing the need for individualized management strategies. 12 A study employing next-generation sequencing and microscopy found bacterial DNA in presumed “clean” bone margins, raising concerns about the limitations of conventional culture-based diagnostics. 13 However, the clinical relevance of these findings remains uncertain, as DNA-based detection methods may identify non-viable organisms without active infection. 13 Our results reinforce the notion that microbiological positivity at resection margins should be interpreted with caution, particularly in the absence of histopathological confirmation of osteomyelitis.
Several investigations have highlighted the need for a standardized approach to intraoperative margin assessment. A study evaluating the clinical utility of intraoperative bone cultures found limited predictive value in determining the need for reoperation or ulcer healing. 14 Another study proposed that intraoperative assessment methods, such as macroscopic bone evaluation and systematic irrigation, may reduce contamination and improve diagnostic accuracy. 2 In our study, rigorous irrigation and sterile sampling techniques were used, yet contamination persisted, further highlighting the challenges of intraoperative diagnostics.
While our initial hypothesis proposed that polymicrobial infections might contribute to contamination, no statistically significant association was found between polymicrobial flora in the primary specimen and contamination at resection margins (p = 0.946). Instead, Pseudomonas aeruginosa was the only species independently associated with contamination (p = 0.008). This novel finding suggests that, rather than being a generalized consequence of microbial complexity, contamination may be driven by specific bacterial traits. We hypothesize that contamination may arise from the persistence of bacteria in the residual soft tissue after bone resection, particularly when these microorganisms are not invading the bone and therefore do not elicit histopathological signs of osteomyelitis. In this context, P. aeruginosa stands out due to its ability to form robust biofilms that enhance resistance to antimicrobial agents and decontamination procedures. 15 These biofilms can also harbour other bacterial species, facilitating interspecies cooperation and further protecting the microbial community from removal.15,16 In addition to its biofilm-forming capacity, P. aeruginosa possesses distinct pathogenic features—including strong adhesion to epithelial and connective tissues, production of extracellular polysaccharides, and persistence in moist environments—that may enable it to remain within the surgical field despite extensive irrigation. 17 Thus, it is plausible that contamination of the bone margin occurs during sampling, when residual bacteria from adjacent soft tissues are inadvertently transferred. Although other common pathogens in diabetic foot osteomyelitis—including known biofilm producers—were frequently isolated from primary specimens, none were significantly associated with contamination. This reinforces the notion that P. aeruginosa may possess unique characteristics that facilitate its persistence and intraoperative transfer despite rigorous lavage before bone margin collection. Further investigation is warranted to elucidate species-specific mechanisms of contamination and to determine whether the use of topical anti-biofilm agents or targeted intraoperative antiseptic protocols 18 may reduce contamination rates in bone biopsies obtained from surgical resection margins.
Our findings have significant implications for the rational use of antibiotics in the management of diabetic foot osteomyelitis. The presence of positive microbiological margins frequently leads to prolonged antibiotic therapy, 8 even though these cultures may not reliably indicate true residual osteomyelitis. This uncertainty raises concerns about overtreatment, exposing patients to unnecessary antibiotic use and contributing to antimicrobial resistance. Given our findings, an alternative approach that warrants further investigation is the discontinuation of antibiotics in cases where microbiological margins are positive but histopathology is negative. Prospective studies are needed to determine whether this strategy could safely reduce antibiotic exposure without compromising patient outcomes.
The association between P. aeruginosa and contamination further emphasizes the need to refine surgical protocols to minimize false-positive cultures. However, since microbiological results are not immediately available, and both primary specimen and margin biopsies are obtained during the same surgical procedure, intraoperative identification of Pseudomonas remains challenging. Although clinical and olfactory recognition of Pseudomonas has been described, its diagnostic accuracy is only moderate. 19 This limitation underscores the importance of developing standardized intraoperative strategies—such as optimized irrigation techniques, the use of topical anti-biofilm agents, or modifications in tissue sampling methods—to reduce contamination risk, particularly in cases where Pseudomonas colonization is suspected based on wound characteristics.
Ultimately, our study reinforces the role of histopathology as the gold standard for diagnosing residual osteomyelitis, despite its delayed availability. The development of rapid intraoperative histopathological techniques or molecular diagnostics could enhance real-time decision-making, reducing both unnecessary antibiotic use and the risk of reoperation. Implementing more precise and efficient diagnostic strategies may help optimize treatment protocols and improve clinical outcomes in diabetic foot osteomyelitis.
This study has certain limitations that should be acknowledged. First, only aerobic cultures were performed, providing an incomplete view of the microbiological profile of bone resection margins. Anaerobic bacteria such as Bacteroides spp. and Finegoldia magna are known to contribute to diabetic foot osteomyelitis, and their exclusion may have influenced the observed rate of false-positive microbiological results. It is possible that incorporating anaerobic cultures would have altered the proportion of contamination detected, either by increasing the false-positive rate or by identifying additional cases of true infection. Second, bacterial load was not quantified in bone margins, as microbiological cultures in this study were qualitative. The use of quantitative techniques, such as assessing colony-forming units per gram of tissue, could have allowed for a better distinction between low-level contamination and clinically relevant infection. Future studies incorporating bacterial quantification may provide a more nuanced interpretation of microbiological positivity at resection margins. Third, while strict aseptic measures were implemented during surgical procedures—including saline irrigation, glove changes, and the use of sterile, single-use bone-cutting instruments—no microbiological surveillance of the remaining surgical tools or environment was conducted. Although the likelihood of contamination from these sources is low, it cannot be completely ruled out. Finally, although a significant association between Pseudomonas aeruginosa and margin contamination was identified, the sample size may have been insufficient to detect associations with other less frequently isolated species. Future studies with larger cohorts may help clarify whether other bacterial species contribute to false-positive microbiological results at resection margins.
Despite these limitations, this study has several notable strengths. First, its prospective design ensures a structured analysis, minimizing selection bias and allowing for a rigorous evaluation of microbiological and histopathological findings. Second, to our knowledge, this is the first study to identify a significant association between Pseudomonas aeruginosa and contamination in bone resection margins, providing a novel perspective on the factors influencing microbiological false positives in diabetic foot osteomyelitis. Third, the use of histopathology as the diagnostic gold standard strengthens the validity of our findings, as previous studies have often relied solely on microbiology. This approach allows for a more accurate assessment of true residual osteomyelitis, reducing the risk of misclassification. Fourth, rigorous surgical protocols—including extensive irrigation and the use of fresh instruments for bone sampling—helped minimize cross-contamination, ensuring a reliable evaluation of microbiological outcomes. Lastly, this study included a detailed analysis of the microbiology of the primary bone specimen, allowing for a comprehensive assessment of the potential influence of bacterial species composition on contamination. This in-depth approach contributes to a better understanding of the interplay between intraoperative contamination and microbiological findings at resection margins.
In conclusion, this study highlights the limitations of microbiological cultures in assessing bone resection margins after conservative surgery for diabetic foot osteomyelitis. While microbiology exhibited high sensitivity, its low specificity resulted in a substantial proportion of false-positive results, reinforcing the superiority of histopathology as the gold standard for diagnosing residual osteomyelitis. The identification of Pseudomonas aeruginosa as the only bacterial species significantly associated with contamination suggests that species-specific factors may contribute to false-positive microbiological findings. These results emphasize the need for cautious interpretation of microbiological cultures at resection margins and support the development of improved intraoperative strategies to reduce contamination. Future research should focus on confirming our hypothesis by directly assessing biofilm formation at bone margins and evaluating whether lavage with anti-biofilm agents reduces contamination rates in bone biopsies obtained from resection margins. Implementing these approaches could lead to more reliable intraoperative diagnostics and optimized antimicrobial management in diabetic foot osteomyelitis.
Footnotes
Authorship Confirmation Statement
J. A-S designed the clinical databases used in this study, conceptualized the study, performed the statistical analysis, analyzed the data, and drafted the manuscript. G. V-M reviewed the database for consistency, evaluated the statistical methods, and contributed to manuscript writing. J. M. R-B reviewed and edited the manuscript and provided critical input to the discussion. All authors reviewed and approved the final version of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.