
Abstract
Purpose
To evaluate the safety and efficacy of cadaveric skin and dermal grafts from skin banks in the management of hard-to-heal wounds (HHWs), particularly of vascular etiology, in a frail patient population.
Methods
This prospective, single-center study enrolled 48 patients with HHWs unresponsive to conventional care. Patients underwent vascular assessment, revascularisation if indicated, and wound bed preparation prior to application of cryopreserved, glycerol-preserved, or lyophilized cadaveric grafts. Outcomes were assessed at predefined intervals up to 10.5 months.
Results
A total of 48 patients were enrolled. Arterial etiology was the most prevalent (33 patients, 68.7%). Complete wound healing was achieved in 47.9% of patients, with a mean time to re-epithelialization of 106.6 days. Limb salvage was attained in 97.9% of cases. Significant pain reduction was observed, with VAS scores dropping from 6.8 ± 1.9 at baseline to 1.5 ± 2.7 at six months (p < 0.0001). The Falanga A wound bed category increased from 42.5% at baseline to 84% at 6 months, and infection rates declined from 42.5% to <12% during follow-up. Subgroup analysis showed superior healing outcomes among arterial HHWs compared to non-arterial HHWs (p < 0.05).
Conclusion
Cadaveric skin bank bioproducts offer an effective and safe option for the treatment of hard-to-heal wounds, particularly in patients with vascular disease. In this cohort, the approach led to a high rate of complete healing and limb salvage with significant pain reduction and enhanced wound bed quality. These results highlight the therapeutic value of allografts when used as part of an integrated protocol that includes revascularisation and meticulous wound bed preparation.
Keywords
Introduction
Effective management of HHWs is therefore essential to ensure the sustainability and efficiency of healthcare systems, by reducing healing times and associated expenditures. 7 However, HHWs present a complex therapeutic challenge, as they often fail to respond to standard treatments. As a result, they require advanced wound care strategies, including innovative dressings and integrated approaches that combine biological and synthetic or semi-synthetic dermal substitutes.8,9
Autologous skin grafting (autografting) remains the gold standard for achieving definitive wound closure. 10 Nevertheless, this option is frequently unfeasible in elderly patients or those with multiple comorbidities, especially with concurrent peripheral artery disease. 11 In such cases, homologous (allogeneic) skin and dermal grafts obtained from cadaveric donors offer a viable alternative. These grafts have been used for over five decades to treat wounds of various aetiologies and morphologies, due to their clinical benefits, including promotion of re-epithelialisation, accelerated healing, pain reduction, and protection of subcutaneous structures.12,13
This study aims to demonstrate that cadaveric skin and dermal grafts are a safe, effective, and reliable treatment option for HHWs of diverse origins, particularly those with healing trajectories that extend beyond the standard timeframe and with a vascular aetiology.
unresponsive to conventional care.
Material and Methods
Study Population
The study is a prospective analysis of a cohort of consecutive patients admitted to the Vascular Surgery Unit of the University of Siena between February 2024 and November 2024 undergoing skin grafting for HHW management. During the study period, 134 lower extremity wounds were treated at our center. The 48 patients included in this study represent 35.8% of cases, all of which were classified as hard-to-heal wounds unresponsive to standard care.
Patients’ data were retrieved from hospital electronic data. Every patient was retrospectively analysed in terms of the anamnestic features: coronary artery disease (CAD) (previous history of coronary-artery-related events with or without surgical or endovascular interventions), hypertension (blood pressure higher than the guidelines suggested cutoff value or antihypertensive drug assumption), diabetes mellitus (DM) [defined as occasional plasma glucose value of ≥200 mg/dL (≥11.1 mmol/L), or fasting plasma glucose of ≥126 mg/dL (7.0 mmol/L) (fasting time 8-12 h), or OGTT (oral glucose tolerance test) 2-h value in venous plasma ≥200 mg/dL (≥11.1 mmol/L) or assumption of insulin or antidiabetic drugs], chronic kidney disease (CKD) (chronic renal insufficiency defined by serum creatinine >1.2 mg/dL), dialysis (any patient undergoing hemodialysis or peritoneal dialysis), smoking history (any current or past regular use of tobacco), congestive heart failure (CHF), history of cerebrovascular events (stroke and/or transient ischemic attacks), history of cancer (any current or past incidence if malignancy), dyslipidemia, and atrial fibrillation (AF).
HHW Characteristics
Each wound was evaluated during the first clinical visit in terms of location (including forefoot, heel, ankle, or leg), wound area (measured in cm²), and wound bed characteristics, based on the appearance score defined by Falanga (A, B, C, D) 14
An analysis of aetiology was also conducted, classifying wounds into five categories: arterial malperfusion, venous insufficiency, mixed aetiology, post-traumatic ulcers, and diabetic-only ulcers.
During the wound assessment, the potential presence of infection was evaluated. Infection was defined as a positive deep wound swab culture obtained under sterile conditions within the preceding 30 days. In cases of confirmed infection, microbial cultures were analysed for mono- or polymicrobial growth, and the administration of antibiotics for infection management was recorded.
Pain was assessed using the Visual Analogue Scale (VAS), and any analgesic therapy prescribed at the time of the initial evaluation was documented.
For patients diagnosed with lower extremity artery disease, arterial revascularisation was performed prior to the application of the skin graft. The procedure aimed to assure the direct blood flow to the wound 15 or, in case of failure, increase the flow following angiosome theory 16
Skin Grafting Positioning
Patients were eligible for inclusion if they presented with an HHW of at least two weeks’ duration. Prior to enrollment, all patients underwent a minimum of 10 days of treatment with standard dressings, which failed to achieve a ≥ 20% reduction in wound area. Only wounds that demonstrated resistance to conventional care were selected for cadaveric skin allografting.
Wound Bed Preparation
Effective management of HHWs using cadaveric skin bank bioproducts requires a well-prepared wound bed to facilitate graft engraftment. Adequate tissue perfusion is essential. In cases of arterial insufficiency, revascularisation of the affected limb was systematically performed prior to study inclusion and wound bed evaluation. Adequacy of perfusion was assessed by completion angiography and confirmed by post-procedural duplex ultrasound. Ankle-brachial index was not routinely used, given its limited reliability in patients with extensive arterial calcification. After vascular restoration, the wound bed was evaluated for the presence of necrotic, infected, or fibrinous tissue, which was removed to create an optimal substrate for graft acceptance. In the case of particularly large or deep wounds, Vacuum-Assisted Closure (VAC) therapy was employed to expedite the formation of granulation tissue and reduce exudate. Final wound bed preparation was conducted in a sterile environment and involved meticulous cleansing and surgical debridement to stimulate granulation and ensure wound viability.
Grafting Procedure
Allografting was performed once the wound bed was deemed suitable. The selection of grafting materials was based on wound depth, morphology, and anatomical location. A range of cadaveric skin and dermal substitutes from the skin bank were utilized, including: deep-frozen dermis or skin, glycerol-preserved dermis or skin, lyophilized, gamma-irradiated dermis.
In some cases, combinations of these bioproducts were employed to maximize coverage and healing potential. The objective of grafting was to promote epithelialization through secondary intention and to provide temporary coverage, protection of underlying structures, and stimulation of wound healing dynamics.
17
Cryopreservation: Skin tissue (epidermis and dermis) undergoes a disinfection process and is then stored at −80 °C. The cryopreserved tissue retains its osmotic, structural, and mechanical properties, along with a certain level of cellular vitality. Their use has been preferred in lesions with arterial etiology as well as in post-traumatic ulcers, where the primary objective was engraftment with the tissue and wound healing Glycerol Preservation: The tissue is incubated with solutions containing physiological saline and glycerol at increasing concentrations (50%, 70%, and 87%), then packaged and stored at +2/+10 °C. The tissue is no longer viable but retains its mechanical and structural properties. The use of this product has been particularly preferred for venous ulcers, owing to its analgesic and antimicrobial properties. Decellularization, Freeze-Drying, and Gamma Irradiation of Dermal Matrices: It consists of a first freezing phase followed by a second sublimation phase, and sterilization using γ radiation through radioactive isotopes. The use of homologous acellular dermal matrices is particularly indicated in the treatment of cavitary wounds with exposure of fragile structures such as bones and tendons. In these cases, the application of homologous acellular dermal matrices facilitates tissue integration at the wound bed and stimulates the formation of a new dermis while maintaining physiological and functional properties.
They can also be classified into mesh and non-mesh grafts. The mesher is a special roller with blades that transforms the graft into a tissue mesh, allowing coverage of larger areas by expanding the tissue. Furthermore, it facilitates fluid drainage (hematomas, exudate, etc) through the mesh openings, promoting graft engraftment in particularly exudative wounds
Follow-up Protocol
Following the initial skin grafting procedure, patients were monitored at least once per week in the outpatient clinic of our hospital. Wound dressings were changed at least twice weekly, either in the hospital or at the patient's home, depending on clinical circumstances. At each follow-up visit, a comprehensive reassessment of the patient and the wound was performed. This included measurement of the wound area (cm²), evaluation of the wound bed using the Falanga score, and assessment for signs of infection.
In addition to evaluating for clinical signs of infection, the use of antibiotics was systematically recorded. All clinical data were prospectively collected and entered into an electronic database at predefined intervals: 30 days, 60 days, 4 months, 6 months, and at the final follow-up visit.
Treatment was discontinued in cases of insufficient wound healing, lesion progression, or increasing pain. Additional reasons for treatment interruption included compromised limb perfusion, need for major amputation, development of infection with extension to surrounding tissues, or patient refusal to continue therapy.
Outcomes Definition
The primary outcomes were complete healing of the wound and limb salvage.
Ulcer healing was defined as complete (100%) re-epithelialization of the wound without drainage and/or the need for dressing.
Limb salvage was defined as the absence of major amputation, which includes any amputation proximal to the ankle joint. Secondary endpoints included the evaluation of pain reduction (assessed using VAS, reported as mean ± standard deviation), absolute and percentage wound area reduction, wound bed assessment using the Falanga score, and the occurrence of infection and/or antibiotic use. These outcomes were monitored at 1, 2, 4, and 6 months, as well as at the end of the follow-up period. (Figure 1).
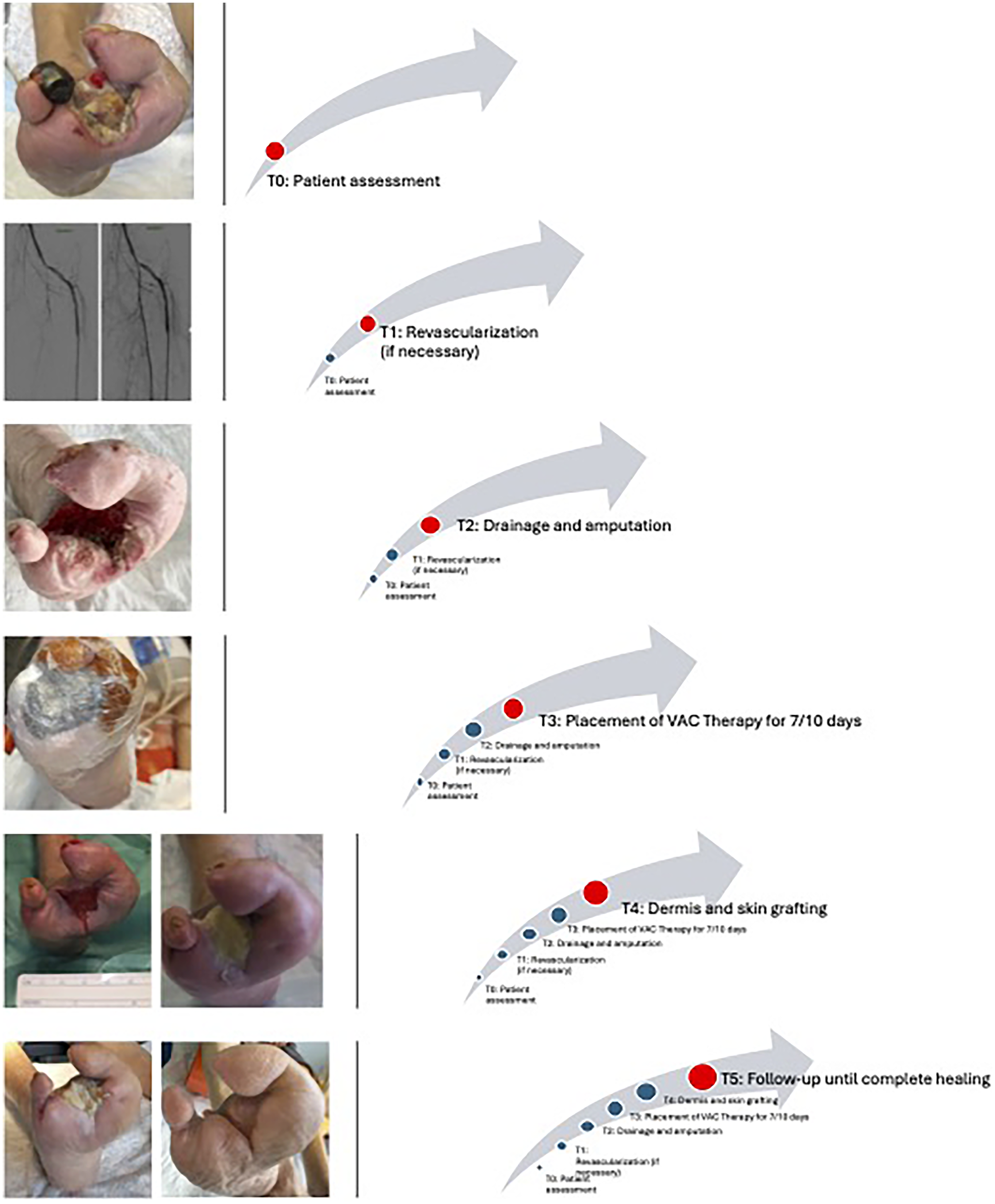
Protocol of HHW Management.
Statistical Analysis
Continuous data were shown as mean values ± standard deviation (SD). Categorical variables were expressed as fractions. Analysis of variance was used for independent tests to compare groups on continuous variables after demonstrating a normal distribution of the data. One-way analysis of variance (ANOVA) analysis was performed within and between-group comparisons for continuous data. Chi-square tests were performed for categorical data analysis. The Kaplan Meier curve analysis were used to evaluate cumulative complete and >50% wound healing probability. Log-Rank test was used to compare Kaplan Meier curves. A p-value inferior to 0.05 has been considered statistically significant in all the statistical tests. All statistical analyses were performed with GraphPad Prism 10.1.1 (GraphPad Software Inc, San Diego, Calif) and Jamovi 2.3.18.0 (Sydney, Australia).
The study was conducted according to the Declaration of Helsinki (as revised in 2013). Wound management, as presented, is part of our centre's daily clinical practice. The ethical committee was informed of the non-experimental design of the study and approved an informed consent waiver.
Results
Study Population
The study included 48 patients, with a mean age of 79 ± 10.6 years, and a male-to-female ratio of 1:1. All patients enrolled in the study provided written informed consent for the treatment, after receiving detailed information regarding the procedures involved.
As illustrated in Table 1, the predominant comorbidity was hypertension (35 cases, 72.9%), followed by diabetes mellitus (19 cases, 39.6%).
Baseline Population Characteristics.
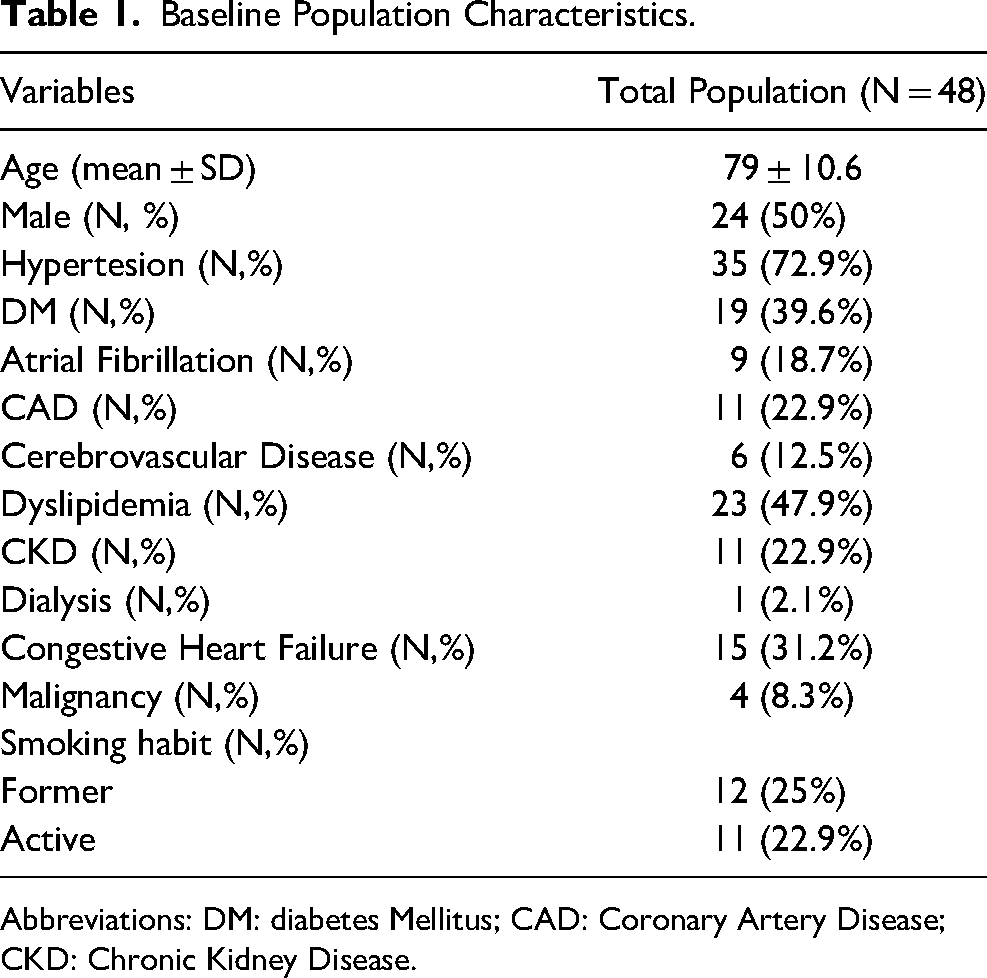
Abbreviations: DM: diabetes Mellitus; CAD: Coronary Artery Disease; CKD: Chronic Kidney Disease.
HHW Characteristics
Lesions exhibited considerable heterogeneity in terms of anatomical location, aetiology, and extent (Table 2). The most common site was the forefoot, affected in 47.9% of patients (n = 23), followed by the lower leg in 31.2% of cases (n = 15). Arterial aetiology was the most prevalent (33/48, 68.7%), followed by post-traumatic (7 patients, 14.6%). Purely venous and diabetic etiologies were observed in 4(8.3%) and 2 (4.2%) patients, respectively. A mixed aetiology (venous ulcers with arterial impairment) was identified in 2 cases (4.2%). The extent of the treated area varied greatly, with a mean surface area of 58.2 ± 49.5 cm². At the beginning of the treatment, the vast majority of patients did not have adequate control of pain symptoms; the mean pain score, assessed using the VAS scale prior to the first treatment, was 6.8 ± 1.9. Regarding wound bed characteristics, 42.5% of cases (n = 20) were classified as Falanga A, 35.4% (n = 17) as Falanga B, and 22.9% (n = 11) as Falanga C. In 42.5% of the treated ulcers, wound swabs yielded a positive bacterial culture, while systemic antibiotic therapy was initiated in 29.2% of cases (n = 14). VAC therapy, aimed at promoting granulation tissue formation and wound bed preparation, was applied in 15 patients (31.2%).
Hard-to-Heal Wounds Characteristics at Presentation and Revascularization Procedures Details.
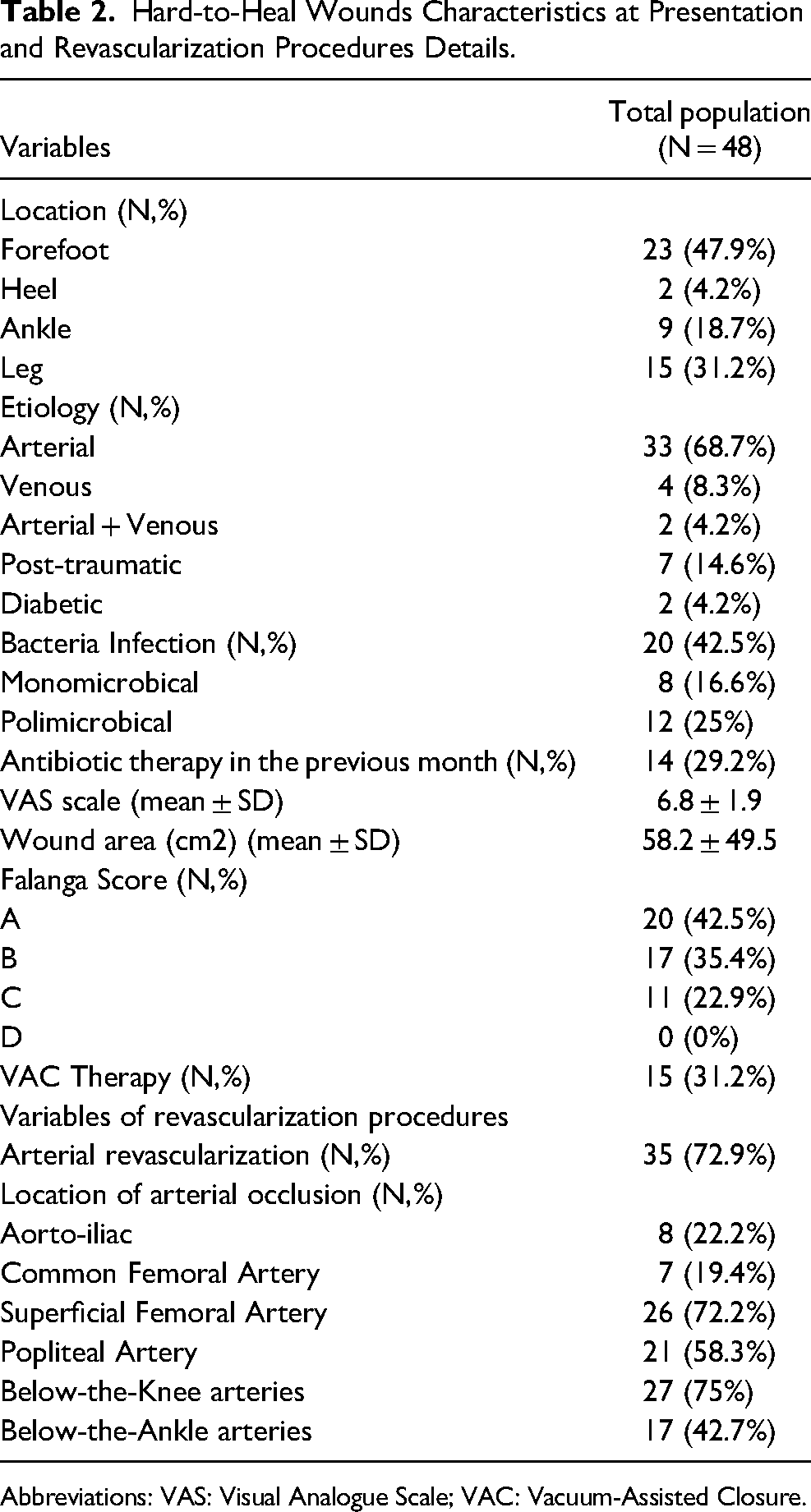
Abbreviations: VAS: Visual Analogue Scale; VAC: Vacuum-Assisted Closure.
Given that the majority of ulcers included in the study were of arterial aetiology, revascularisation of the affected limb was considered necessary and mandatory prior to proceeding with treatment using cadaveric skin and dermal homografts. A revascularisation procedure was performed in all patients. In 94.2% (33/35), the revascularisation assured a direct flow to the wound, while in the remaining two, an indirect revascularisation was performed. The locations of arterial occlusions and the vessels targeted for revascularisation were heterogeneous, as detailed in Table 2. The most commonly affected and treated vascular segments were the superficial femoral artery (SFA) and the below-the-knee (BTK) district: SFA occlusions were observed in 72.2% of cases, with SFA revascularization performed in 66.7%, while BTK involvement was present in 75% of cases, with BTK revascularization performed in 55.6%. Twenty-two patients were treated with percutaneous transluminal angioplasty (PTA) alone, 11 with PTA and stenting, 2 with intravascular lithotripsy, and 4 underwent surgical femoral endarterectomy.
Skin Graft Analysis
The selection of bank-derived bioproducts was based on the specific characteristics of each lesion. During the initial skin graft procedure, most patients received cryopreserved dermis and cryopreserved skin homografts (45.8%, n = 22), with the aim of promoting graft take and achieving wound healing by secondary intention. In 20.8% of cases (n = 10), the initial approach involved the use of glycerol-preserved dermis and skin. In these cases, the primary objective was pain reduction and safe management of local infections. These data are presented in detail in Table 3.
First Skin Grafting Characteristics.
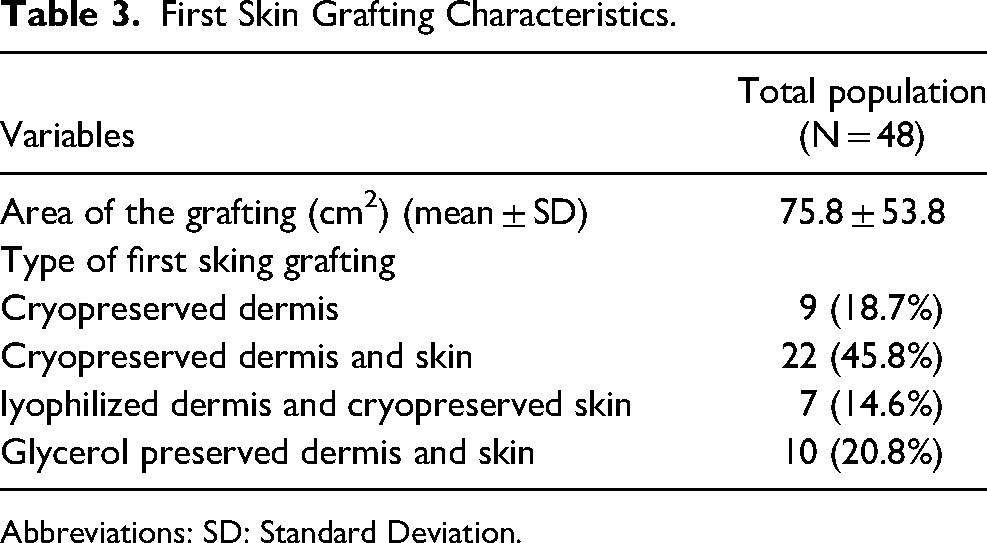
Abbreviations: SD: Standard Deviation.
Follow-up
The patients included in our study had a mean follow-up of 184 ± 98.1 days. Only patients with a minimum follow-up of at least 30 days were included, with the maximum follow-up extending to 316 days (10.53 months). A total of 313 homograft sessions were performed with a mean number of implantation sessions of 6 per patient. No intolerance/allergic reactions were registered. The patients were followed prospectively, and the data were analysed at 30 days, 60 days, 4 months, 6 months, and at the end of the follow-up period.
Treatment was discontinued in 17 cases (35.4%). The causes were inadequate wound healing (6/48), poor compliance (3), major amputation (1), worsening of arterial malperfusion (1) and 1 patient was lost on follow-up. Five patients died during follow-up from causes unrelated to wound management, including cardiovascular events (n = 3), pneumonia (n = 1), and malignancy (n = 1).
Primary Outcomes
The primary outcome assessed was complete wound healing, achieved in 23 patients, representing 47.9% of the study population. The average time to complete healing was 106.65 days, with a mean healed surface area of 43.86 ± 41.5 cm². Kaplan-Meier analysis (Figure 2) illustrates the cumulative healing probability over time, with rates of 10.4% at 30 days, 17.8% at 60 days, 38.5% at 4 months, and 57% at 6 months of follow-up.
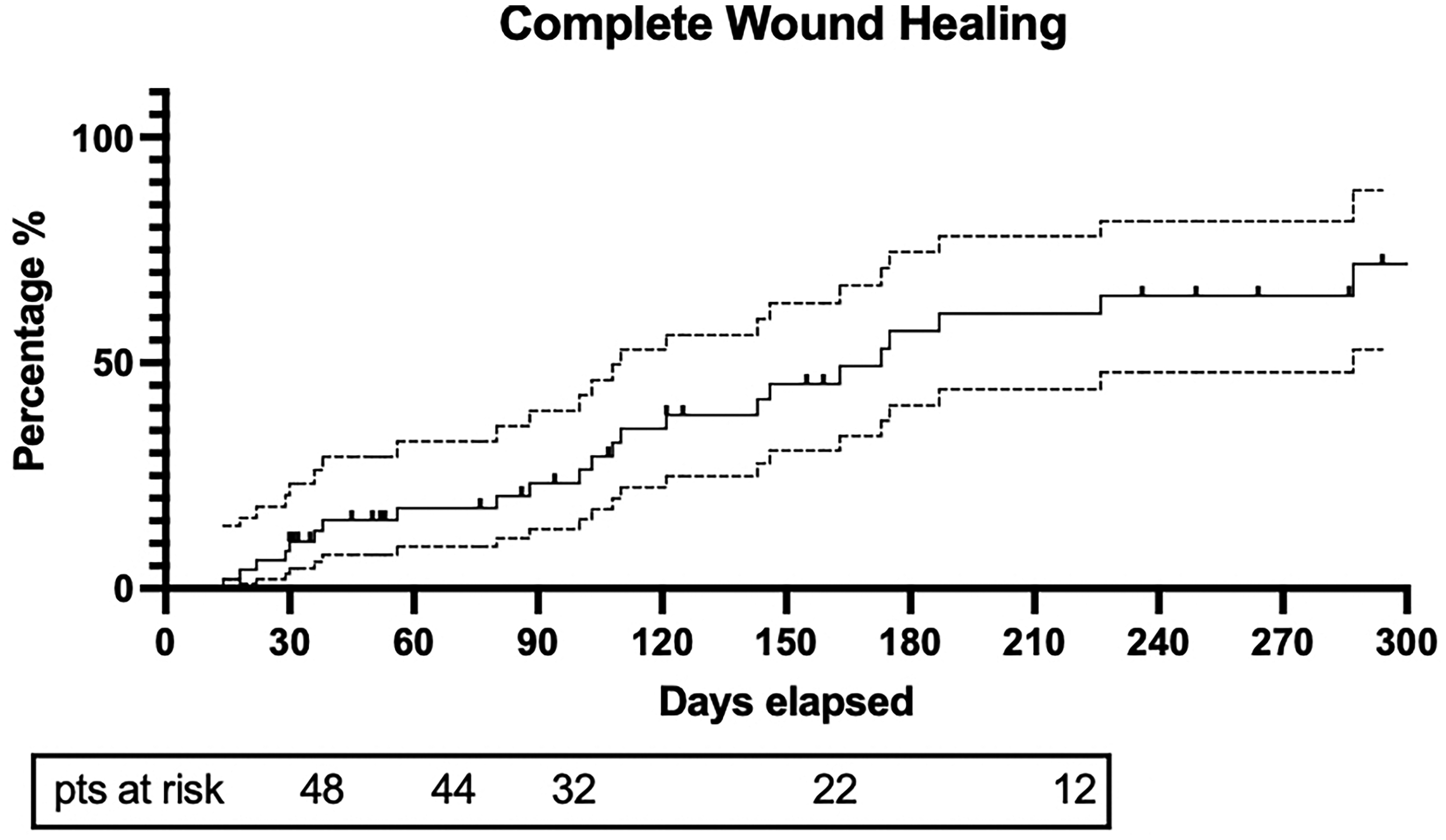
Kaplan-Meier analysis illustrates the cumulative healing probability over time. Dotted lines indicate 95% confidence intervals around the Kaplan–Meier survival estimates.
Limb salvage, was achieved in 47 patients, corresponding to a rate of 97.9% with one case of major limb amputation occurring due to infectious complications and progression of osteomyelitis, which required a transfemoral amputation
Secondary Outcomes
Pain perception was deeply influenced by the treatment with a significant reduction of VAS throughout the follow-up (p < 0.0001). From baseline 6.8 ± 1.9 towards 1.5 ± 2.7 at 6 months follow up with a major drop during the first 30 days of treatment (3.5 ± 2.2). (Figure 3A)
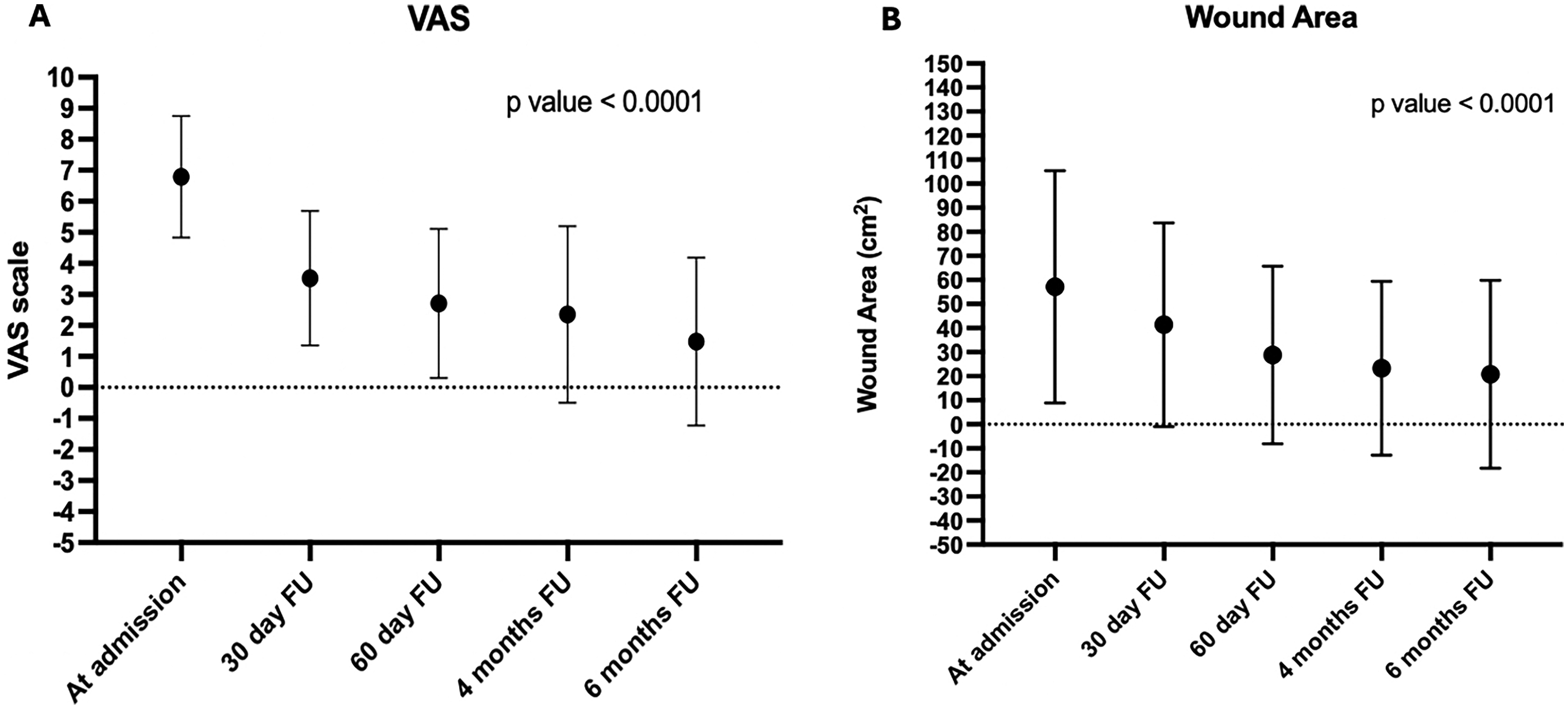
(A) VAS Trend Over Time; (B) Wound Area Reduction Over Time.
Wound area reduction was gradual (Figure 3B): 58 ± 49.5 cm2 at admission versus 20.8 ± 39 cm2 at 6 months follow-up of the remaining (12/48) that concluded the follow-up without complete healing (p < 0.0001). Kaplan Meier curves highlight the cumulative > 50% healing probability over time with rates of 20.8% at 30 days, 39.9% at 60 days, 71% at 4 months, and 79.3% at 6 months of follow-up. (Figure 4).
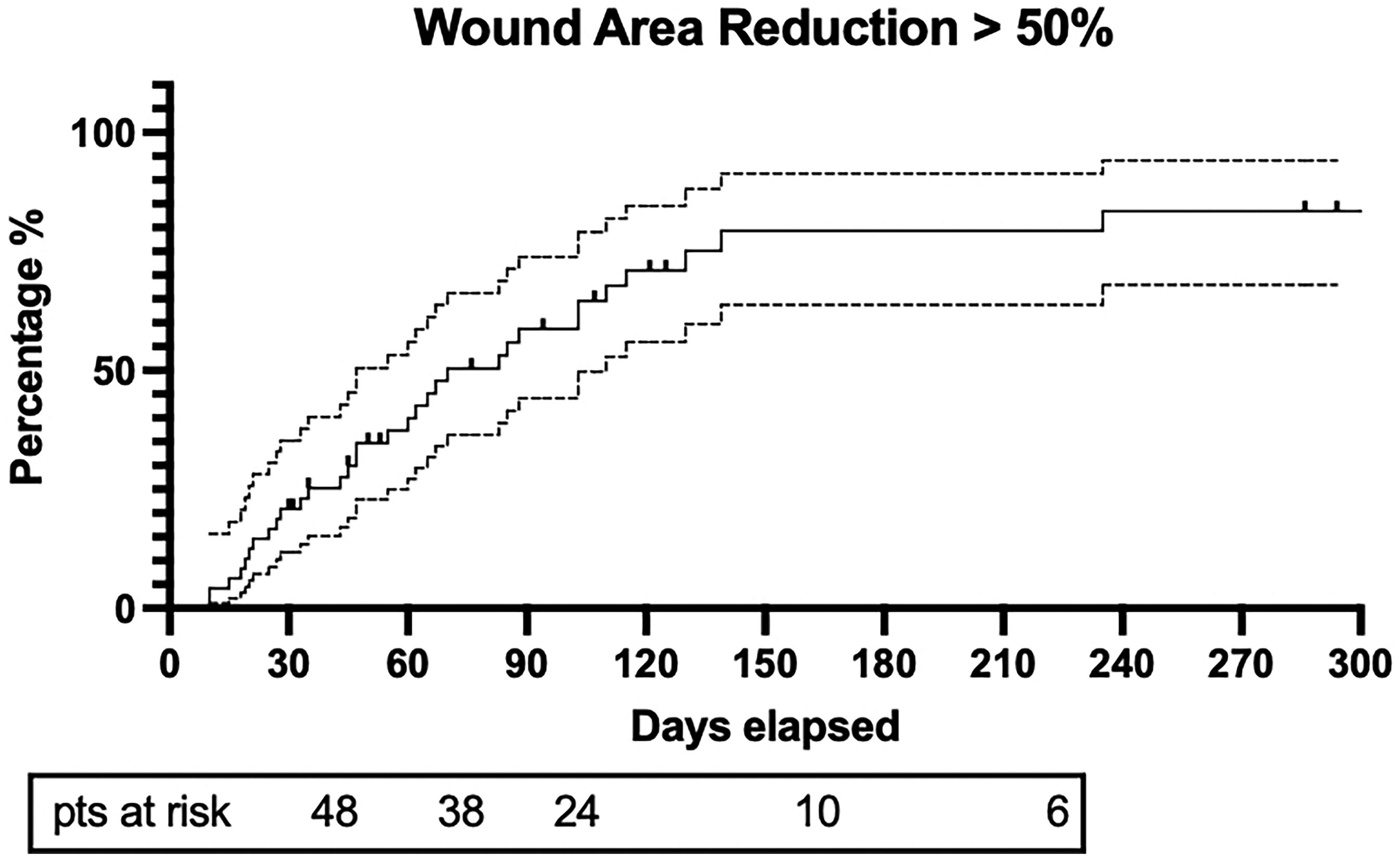
Kaplan Meier curves highlight the cumulative > 50% healing probability over time. Dotted lines indicate 95% confidence intervals around the Kaplan–Meier survival estimates.
A sub-analysis was performed in order to evaluate complete would healing and wound area reduction based on the HHW etiology. Arterial HHWs marked a substantial better outcomes compared to Non-arterial ones as highlighted in Figure 5 (A-B) (log-rank test p < 0.05 for both outcomes).
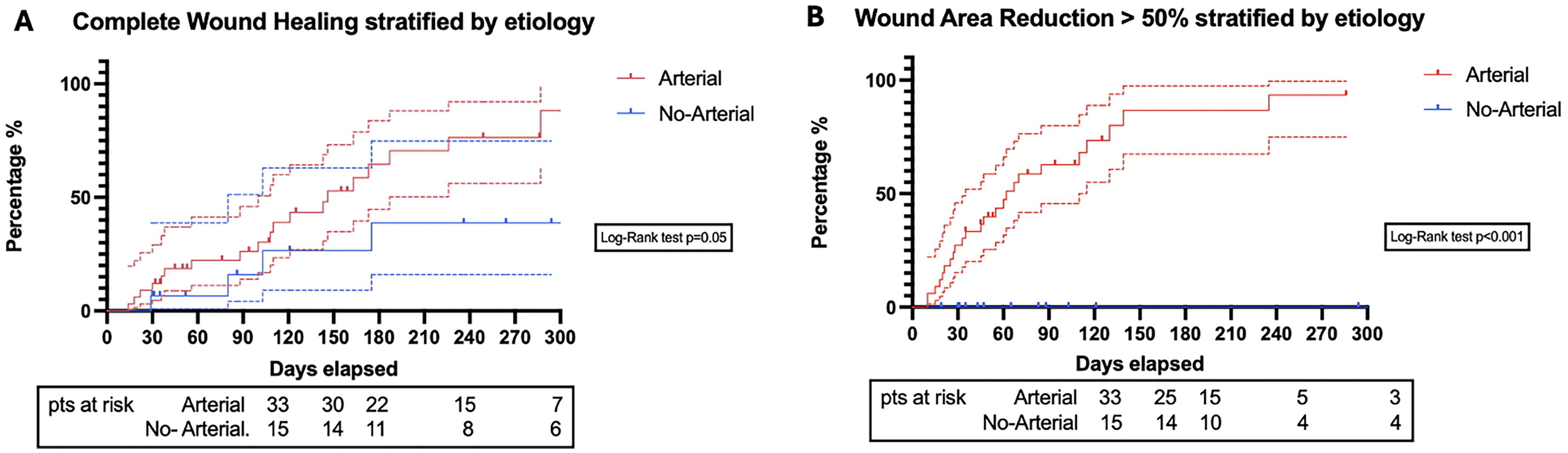
Kaplan Meier Curves Subanalysis Stratified by HHW Etiology. (A) Cumulative Healing Probability Over Time; (B) Wound Area Reduction Over Time. Dotted Lines Indicate 95% Confidence Intervals Around the Kaplan–Meier Survival Estimates.
The graph of the Figure 6 illustrates the trend in wound bed quality over time, as assessed using the Falanga Score, from admission through six months of follow-up. At admission, only 42.5% of wounds were classified as Falanga A (indicating a healthy granulating wound bed), while 35.4% and 22.9% were scored as Falanga B and C, respectively, suggesting suboptimal healing conditions. Notably, no wounds were classified as Falanga D (necrotic tissue).
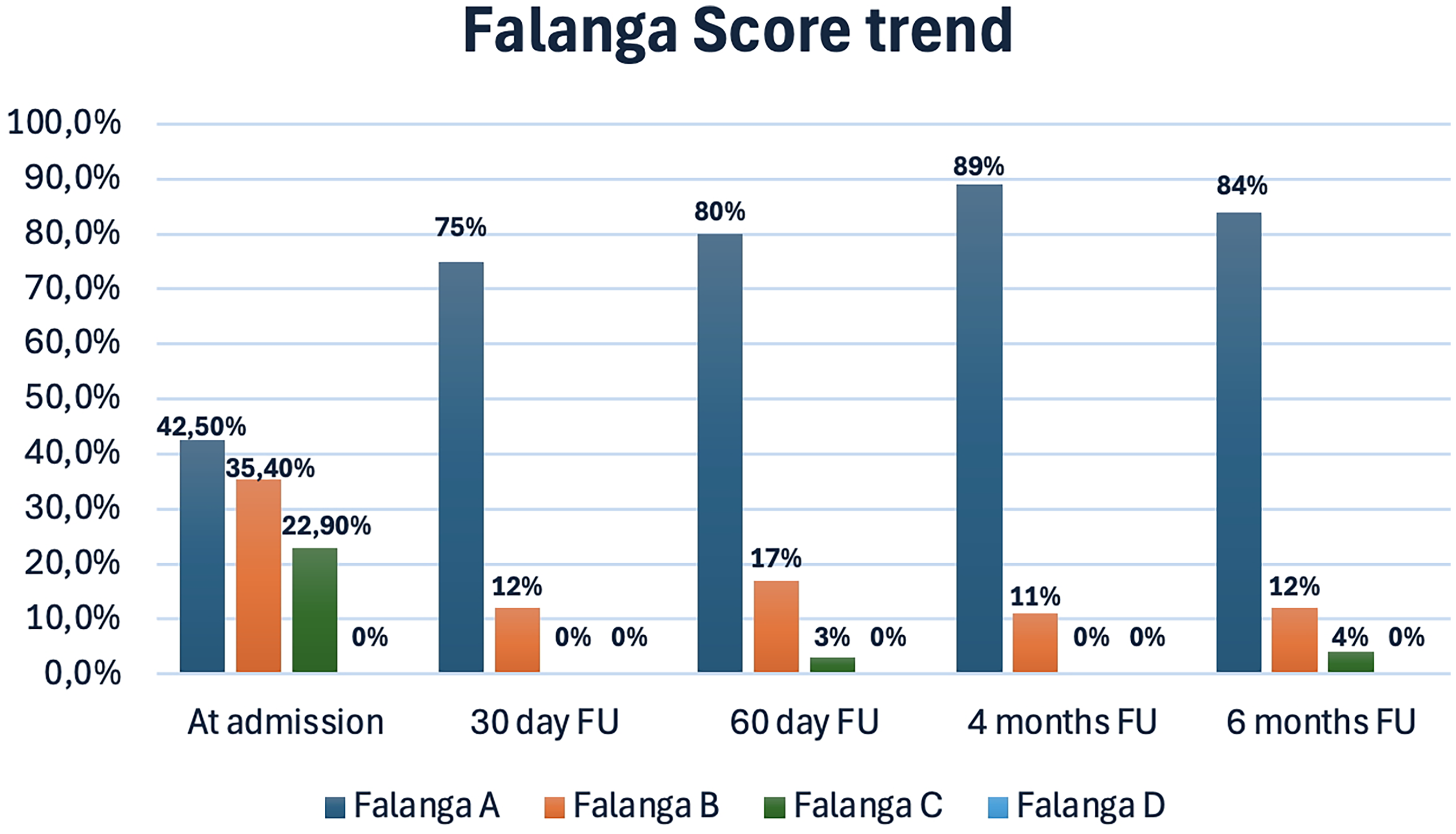
Falanga Score trend over time.
By the 30-day follow-up, a substantial improvement was observed, with 75% of wounds reaching Falanga A and complete elimination of category C and D wounds. Continued improvement was recorded at 60 days (80% Falanga A), peaking at 4 months with 89% of wounds in category A. At the 6-month mark, 84% of wounds remained in category A, confirming sustained enhancement of the wound bed.
At baseline, 42.5% of patients (n = 20) presented with wound infections, and 29.2% (n = 14) were receiving systemic antibiotic therapy. By the 30-day follow-up, infections had dropped to 6.2% (n = 3), and antibiotic use decreased to 4.2% (n = 2). This trend continued at 60 days, with only 7.3% of wounds infected and 2.4% of patients still requiring antibiotics. Notably, by 4 and 6 months, no patients required antibiotic treatment, and infection rates remained low at 2.8% and 12%, respectively. Table 4 summarize timeline evolution of primary and secondary outcomes during follow-up. Figure 7 represents an example of HHW with complete healing.
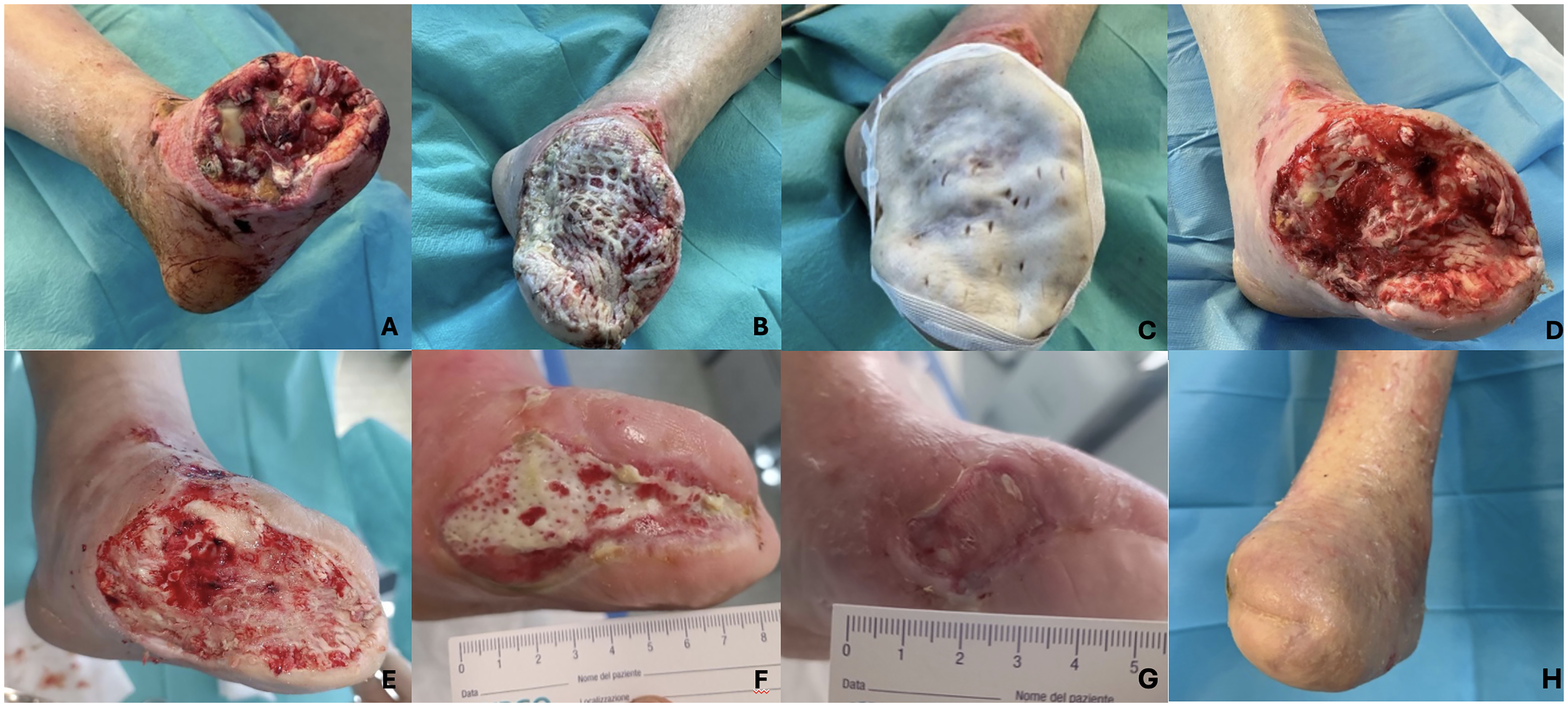
Example of a Complete HHW in the Cohort of Study: (A) Transmetatarsal Amputation in CLTI Patients; (B) Criopreseved Dermis Grafting; (C) Criopreserved Skin Grafting; (D-E-F-G-H) Wound Evolution Until Complete Healing.
Timeline Evolution of Primary and Secondary Outcomes in the Whole Study Population.
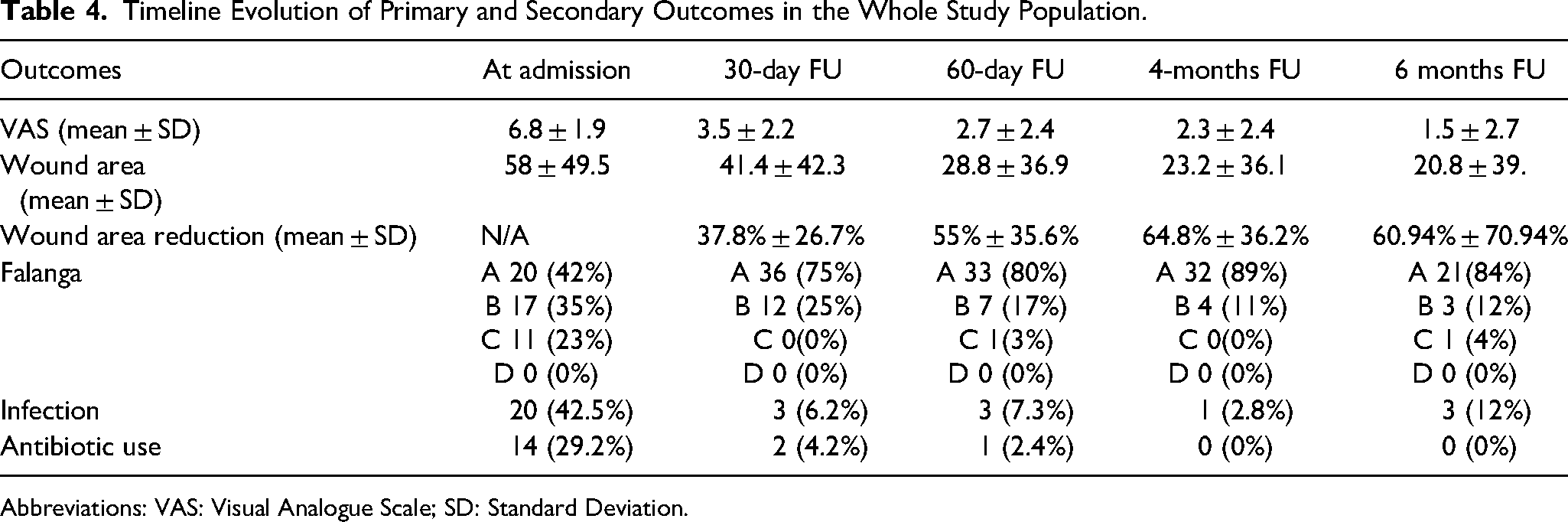
Abbreviations: VAS: Visual Analogue Scale; SD: Standard Deviation.
Discussion
This prospective single-center study evaluated the use of cadaveric skin bank bioproducts for the treatment of HHWs, with a particular focus on ischemic ulcers due to CLTI (Chronic Limb-Threatening Ischemia). The findings demonstrate that allogeneic skin and dermal grafts can serve as a reliable therapeutic option in complex wound scenarios, especially when conventional wound care has failed and autologous grafting is contraindicated due to patient frailty or comorbidity burden.
CLTI is a progressive atherosclerotic condition characterised by critical reductions in blood flow to the lower extremities, and it remains a leading cause of non-healing ulcers and major amputations worldwide. In our cohort, 77.1% of wounds were of arterial aetiology, and 76.6% of these patients underwent successful revascularisation prior to grafting. This aligns with established principles emphasising the restoration of adequate perfusion as a prerequisite for wound healing in CLTI patients.18,19 The technical success rate of revascularisation in our series was high (91.4%), targeting commonly affected segments such as the superficial femoral artery (SFA) and below-the-knee (BTK) vessels, consistent with current endovascular treatment strategies. 20
Our overall wound healing rate of 47.9%, achieved over an average of 106.6 days, is comparable with healing rates reported in studies using bioengineered skin substitutes, which typically range from 35% to 60% depending on the wound aetiology, follow-up duration, and patient selection. 21 Notably, our cohort included patients with large, polymorbid wounds (mean wound area 58.2 ± 49.5 cm²), which are associated with poorer prognoses. Despite this complexity, limb salvage was achieved in 97.9% of patients—an outcome that compares favourably with studies of similar populations, where major amputation rates can exceed 20% in cases of refractory ischemic wounds. 22
Another critical finding is the substantial improvement in wound bed quality over time, with Falanga A classification increasing from 42.5% at baseline to 84% at six months. This suggests that cadaveric grafts may play an active role not only in providing temporary coverage but also in stimulating granulation tissue and promoting a more favourable healing environment. These outcomes support previous reports suggesting that allogeneic dermal matrices facilitate dermal regeneration, neovascularisation, and re-epithelialization, particularly when used in combination with optimised perfusion and debridement strategies. 23
Pain reduction was also significant, with VAS scores dropping from 6.8 ± 1.9 to 1.5 ± 2.7 at six months (p < 0.0001). This aligns with earlier findings on the analgesic properties of glycerol-preserved and cryopreserved allografts, which are thought to provide occlusive protection to exposed nerve endings and reduce inflammatory mediator exposure. 24 Furthermore, infection rates declined from 42.5% at baseline to 12% by six months, with no patients requiring systemic antibiotics beyond the fourth month. This supports literature suggesting that cadaveric grafts may have antimicrobial barrier properties and reduce bacterial colonisation in open wounds. 25
Tailored graft selection was a key component of our protocol. Cryopreserved tissues, retaining viable dermal cells and mechanical integrity, were favoured in ischemic and traumatic wounds, consistent with prior recommendations for biological integration in well-prepared wound beds.. 26 Glycerol-preserved and lyophilised dermal matrices were applied in venous or cavitary lesions, providing mechanical coverage and supporting tissue remodelling without reliance on cellular viability. Such personalisation of grafting strategies aligns with emerging precision medicine approaches in wound care. 27
The heterogeneity in wound aetiology and anatomical location within our cohort, ranging from ischemic ulcers in patients with chronic limb-threatening ischemia to post-traumatic, diabetic, and mixed-aetiology lesions, reflects the clinical complexity of real-world hard-to-heal wounds. This variability in wound depth, vascular status, and infection risk presents a challenge for standardised treatment approaches. In this context, cadaveric allografts demonstrated consistent efficacy across a broad spectrum of wound types, highlighting their adaptability and versatility in multidisciplinary wound care. Compared to bioengineered skin substitutes and synthetic matrices or cell-based constructs, cadaveric grafts offer several practical advantages: they are biologically active, structurally intact, and more accessible, particularly in public healthcare systems. While engineered products may deliver regenerative stimuli, they are often cost-prohibitive, require complex handling, and are less suited to infected or ischemic environments.28,29 Cadaveric allografts, in contrast, provide immediate coverage, preserve essential extracellular matrix components, and support granulation, revascularization, and re-epithelialization. Their ease of application and compatibility with contaminated or poorly perfused beds make them an attractive option for frail, polymorbid patients where flexibility, safety, and clinical pragmatism are paramount.
Limitations
Despite the promising results, several limitations should be acknowledged. This study was designed as a prospective, single-arm observational analysis reflective of routine clinical practice. The absence of a control group limits direct comparison with other wound care modalities, but allowed for the inclusion of frail and polymorbid patients typically excluded from randomized trials. Further controlled studies are needed to validate these findings against other advanced therapies, that is the future direction of our research The follow-up period, though adequate to assess initial healing, may not fully capture long-term outcomes such as ulcer recurrence or functional recovery.
Conclusion
This study demonstrates that the use of cadaveric skin bank allografts in patients with hard-to-heal wounds, predominantly from arterial aetiology, is associated with substantial clinical benefits, including high rates of wound healing and limb salvage. The treatment was also linked to significant reductions in pain and infection rates, along with improved wound bed conditions, particularly in cases following successful revascularization. These findings support the integration of skin bank bioproducts into multidisciplinary wound care pathways for frail, polymorbid patients who are unfit for autologous grafting or unresponsive to standard therapies.
Footnotes
Abbreviations
Authors’ Contribution
Conception and design: EP, GF; Analysis and interpretation: EP, GF; Data collection: EL, BG, CM, LP; Statistical analysis: EP, GF; Writing the article: EP, GF, GdD; Critical revision of the article: EP, GF, EL, BG, CM, LP, GdD; Overall responsibility: EP, GdD ; All authors read and approved the final version of the article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.