
Abstract
Background and Aims
The aim of the study was to evaluate the prevalence of recurrent diabetic foot ulcers (DFUs) requiring hospital admission and to assess their impact on mid-term clinical outcomes.
Methods and Results
It is a single-center retrospective observational study including a population of patients with DFUs requiring hospitalization managed between January and September 2024 in a tertiary level diabetic foot service. All patients were treated by a local multidisciplinary team in accordance with international guidelines. The study cohort consisted of two groups: patients with a recurrent DFU and those with a first-time DFU. After discharge, all patients were regularly followed as outpatients. After six months of follow-up, the following outcomes were evaluated and compared between groups: healing, major amputation, and mortality. Overall, 205 patients were included (31.7% recurrent DFU vs 68.3% first-time DFU). The mean age was 68.9 ± 12.3 years, the majority had type 2 diabetes (93.4%) with a mean diabetes duration of 20.9 ± 12.6 years; 155 (75.6%) patients presented with ischemic DFUs, and 158 (77.1%) patients had diabetic foot infections. There were no significant differences between the two groups at the assessment, except for the higher rate of ischemic heart disease in recurrent patients when compared to not recurrent (50.8 vs 30.7%, P = .006).
Conclusion
Six-months outcomes (recurrent DFU vs first-time DFU) were as follows: wound healing (47.7 vs 62.8%, P = .04), major amputation (4.6 vs 5%, P = .2), and mortality (12.3 vs 4.3% P = .03), respectively. Multivariate logistic regression analysis showed that ulcer recurrence was an independent predictor of non-healing, while it did not significantly influence the risk of major amputation or mortality.
Introduction
Diabetic foot ulcers (DFUs) affect approximately 18.6 million people worldwide. 1 DFUs are associated with impaired physical function, reduced quality of life, and increased health care utilization.2‐4
The likelihood of experiencing a foot ulcer rises with the duration of diabetes 5 and the risk of death at 5 years for a patient with a DFU is 2.5 times as high as the risk for a patient with diabetes without a foot ulcer. 6 The risk of death at 10 years for a patient with DFUs is twice higher compared to a patient with diabetes without a foot ulcer. 7
The direct costs of treating diabetic foot complications exceed the treatment costs for many common cancers and chronic conditions.8,9
Unfortunately, even after the resolution of a foot ulcer, recurrence is a common issue. 10
Recurrent foot ulcer is defined as the development of a new foot ulcer in a person who has a history of foot ulceration, regardless of the previous ulcer site or the interval since healing. 10
The reasons for ulcer recurrence seem to depend on biological factors, behavioral conditions, or both. Many precipitating factors that led to the ulcer in the first place, such as peripheral neuropathy, foot deformity, increased plantar stress, and peripheral arterial disease (PAD), are generally not resolved after healing. 11
It has been reported that 40% of patients with DFUs had a recurrence in 1 year and near 60% in 3 years. 12
Nonetheless, there are not many data about the impact of DFU recurrence on the clinical outcomes, including specifically healing, major amputation and mortality.
Consequently, the aim of this study was to evaluate the prevalence of DFU recurrence in patients admitted for DFUs and to assess its impact on mid-term clinical outcomes.
Methods
Patient's Selection
The study is a retrospective observational study including a population of patients with DFUs requiring hospitalization, managed between January 2024 and September 2024 in a tertiary level diabetic foot service. All patients were treated through a limb-salvage protocol in accordance with international guidelines of International Working Group on the Diabetic Foot (IWGDF). 13 This protocol included lower limb revascularization for ischemic or neuro-ischemic DFUs, antibiotic therapy in the case of infection, and appropriate offloading of the affected foot. 13 This protocol encompassed key interventions: surgical procedures were tailored to the specific clinical needs of each case and could include necrosectomy, minor amputations, bone resections, negative pressure therapy, and the application of dermal-epidermal substitutes, among other techniques. 14
The study cohort consisted of two groups of admitted patients: those with a history of DFU requiring hospitalization for a new ulcer (recurrent DFU) and those without prior DFU history, hospitalized for the onset of their first ulcer (first-time DFU). Recurrent DFU was defined regardless of the previous ulcer site or the interval since healing. 10
Inclusion and exclusion criteria are reported in Table 1.
Inclusion and Exclusion Criteria for the Study Enrollment.
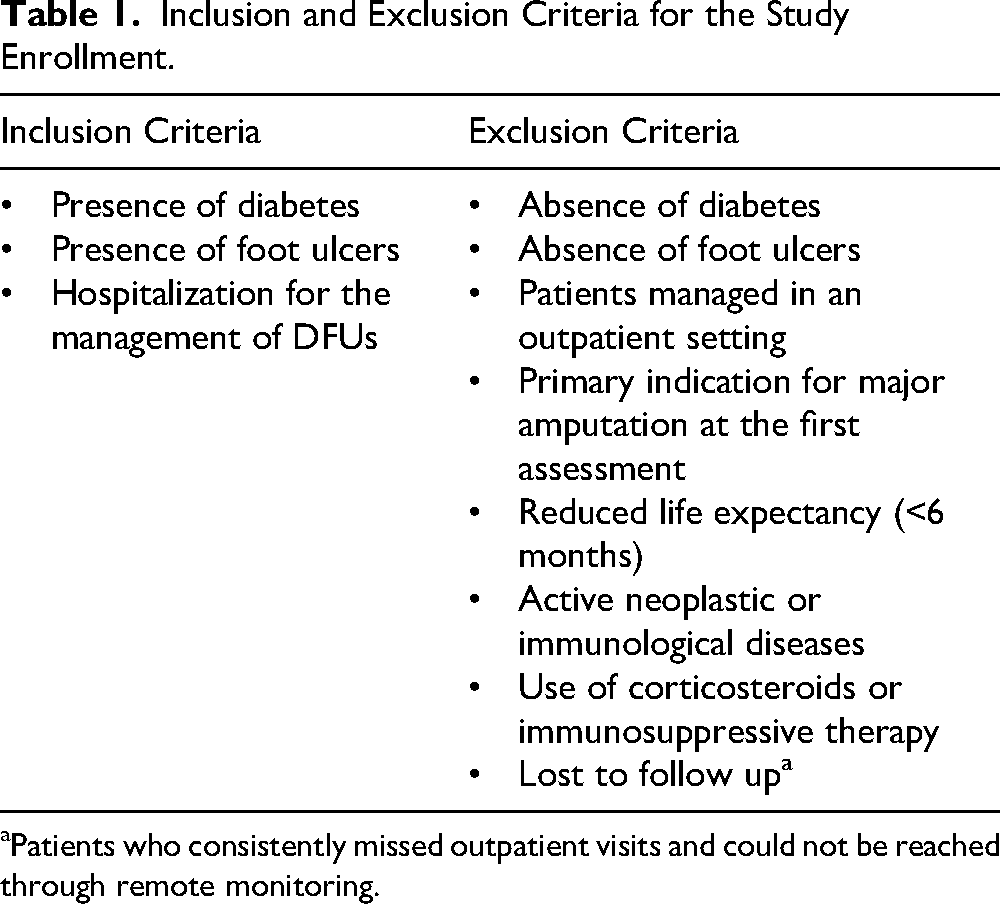
Patients who consistently missed outpatient visits and could not be reached through remote monitoring.
At baseline, clinical and wound characteristics were recorded.
After discharge, all patients were followed as outpatients for 6 months, and the following outcomes were evaluated: healing, major amputation, mortality.
Clinical Features
Hypertension was considered in the case of current antihypertensive therapy. Dyslipidemia was considered in case of statin therapy or impaired low-density-lipoproteins (LDL) (>55 mg/dL) requiring statin therapy. Obesity was defined as a body mass index (BMI) greater than 30 kg/m2. The presence of ischemic heart disease (IHD) was defined in the case of previous acute coronary syndrome or coronary revascularization, evidence of angina, and significant changes on electrocardiography (above or under-levelling ST, q wave, inversion of T wave, new left bundle branch block). Heart failure (HF) was considered in the case of typical symptoms and echocardiographic signs of HF: reduced left ventricular ejection fraction (LVEF) (<40%) or normal or only mildly reduced LVEF and elevated levels of brain natriuretic peptides (BNP > 35 pg/mL and/or NT-proBNP > 125 pg/mL) with not dilated left ventricle (LV) associated with relevant structural heart disease (LV hypertrophy/left atrial enlargement) and/or diastolic dysfunction.
The rate of end-stage renal disease patients requiring dialysis was reported.
Wound Assessment
Wound features were recorded at the first assessment according to IWGDF definitions. 15
Included DFUs comprised neuropathic infected wounds, ischemic non-infected, and ischemic infected wounds regardless of depth (superficial or deep to tendons, muscles and bones).
Infection diagnosis was done according to clinical signs (redness, warmth, swelling, induration, tenderness, pain, purulent secretion). 16 Infected DFUs considered for the current study were only moderately or severely infected wounds according to the IWGDF/Infectious Diseases Society of America classification requiring hospitalization. 16
Osteomyelitis was considered in the case of deep ulcer involving the bone, confirmed by radiological evaluation (x-ray and/or magnetic resonance) and/or positive microbiological analysis. 16
Inflammatory lab markers were also assessed at baseline.
Neuropathic Assessment
Peripheral neuropathy was assessed by evaluating both sensory and, when applicable, motor components. Sensory testing included vibration perception using a 128-Hz tuning fork and light touch sensation assessed through the Semmes-Weinstein 10-g monofilament at standardized plantar sites. Loss of protective sensation was recorded when patients were unable to perceive at least one of the applied stimuli. 13
Vascular Assessment
Neuro-ischemic/ischemic DFUs included in the current study were considered in the case of absent palpable foot pulses and ankle–brachial index (ABI) < 0.9 and/or transcutaneous oxygen pressure (TcPO2) < 30 mm Hg. 17 An ultrasound duplex scan was used on all patients with suspected neuro-ischemic/ischemic DFUs to evaluate the morphology of the lower limb vascular tree, confirm the diagnosis of PAD, and assess the need for and type of lower limb revascularization. Additional imaging, such as computed tomography (CT) or magnetic resonance imaging (MRI), was reserved for cases where there was uncertainty regarding the characteristics of vascular plaques or the appropriate type of intervention.
Vascular examinations were performed in all included patients. The vascular assessment at bedside was carried out exclusively by highly experienced professionals, such as interventional radiologists or vascular surgeons, to minimize the potential for inter-observer variability. In the case of significant PAD, patients underwent lower limb revascularization. The main aim of revascularization procedures was to open all occluded arteries or, if technically not possible, the revascularization of a targeted artery (wound related artery). Patients were treated with dual antiplatelet therapy (acetylsalicylic acid 100 mg and clopidogrel 75 mg once a day) before the procedure and for at least 1-month after. 14
Offloading
All patients received specific offloading based on ulcer location (forefoot/midfoot or hindfoot), in accordance with international guidelines. 13
Particularly, in the case of forefoot and midfoot DFUs, a removable knee-high or ankle-high offloading device was used; in the case of hindfoot DFUs, specifically in the plantar surface, a knee-high offloading device or a specific acute phase device for relieving heel pressure was used. In addition, mainly in the case of extensive surgical approach, total offloading was prescribed by using wheelchairs.
Outcome Measures
After six months of follow-up, the following outcomes were evaluated and compared between groups (recurrent DFU vs first-time DFU): healing, major amputation, and mortality.
Healing was defined as complete wound closure without major amputation, including wounds that healed following a minor amputation and those that healed without any minor amputation. A minor amputation was considered healed when the stump showed complete and stable epithelialization, with no discharge, signs of infection or necrosis, and required no further surgical procedures. Otherwise, an unhealed wound was considered in case of absence of complete or stable epithelialization for at least 2 weeks. Major amputation was defined as any amputation above the ankle.
Statistical Analysis
Statistical analysis was performed using SAS software (JMP13.1; SAS Institute). Data were expressed as means ± SD. Comparisons between groups were reported by chi-square test (frequency data) or Student's t test (continuous data). Univariate logistic regression analysis was performed for all potential predictor variables (age, sex, duration of type 2 diabetes mellitus, glycated hemoglobin, obesity, infection, dialysis, heart failure, ischemic heart disease, dyslipidemia, wound characteristics, wound location, lab inflammatory markers), and odds ratios (ORs) with 95% CIs were given to measure the association with outcomes of interest (healing, major amputation, mortality). Then, all potential predictors were entered simultaneously in a multivariate logistic regression model. These models yielded a set of variables that best predict the outcome. For all analyses, a P-value <.05 was considered statistically significant.
The current study did not require ethical approval according to the local policy being a retrospective observational study. All patients provided their consent for data recording and being considered for the study.
Results
Overall, 220 patients were initially selected for the study; 15 (6.8%) were lost to six-month follow-up, resulting in a final sample of 205 patients. Patients were considered lost to follow-up if they consistently missed outpatient visits and could not be reached through remote monitoring.
The mean age was 68.9 ± 12.3 years, and the majority of patients had type 2 diabetes (93.4%) with a mean diabetes duration of 20.9 ± 12.6 years. In total, 155 (75.6%) patients presented with ischemic DFUs, and 158 (77.1%) patients had diabetic foot infections.
Overall, 65 patients (31.7%) were admitted for a recurrent DFU, while 140 patients (68.3%) were admitted for a first-time DFU.
At assessment, patients with a recurrent DFU did not report any significant difference in terms of clinical and wound characteristics when compared to those with a first-time DFU, except for a higher rate of IHD (50.8 vs 30.7%, P = .006) (Table 2).
Baseline Demographic and Clinical Data.
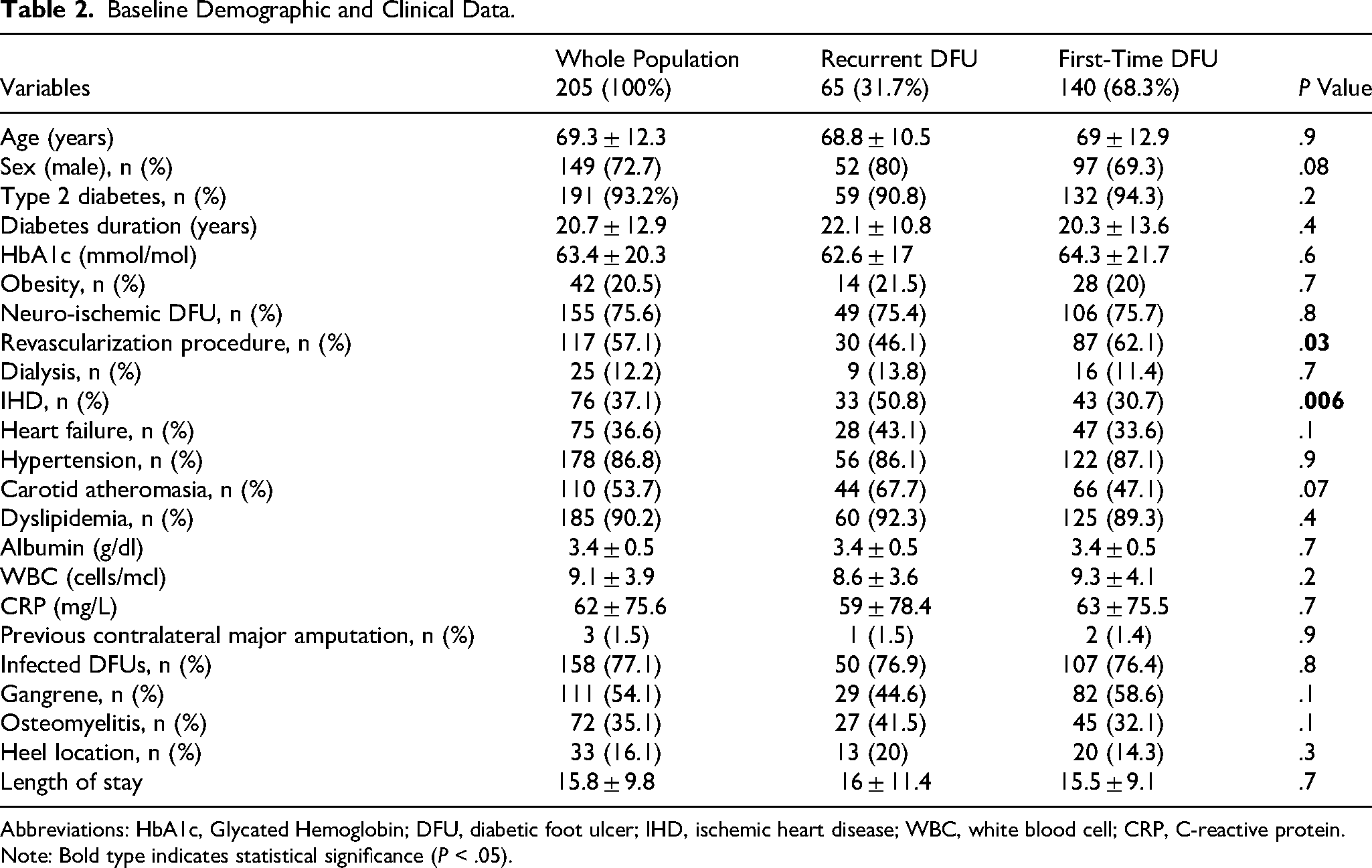
Abbreviations: HbA1c, Glycated Hemoglobin; DFU, diabetic foot ulcer; IHD, ischemic heart disease; WBC, white blood cell; CRP, C-reactive protein.
Note: Bold type indicates statistical significance (P < .05).
At six months, 119 patients (58%) achieved wound healing (84 patients healed without minor amputation while 35 healed after minor amputation), 10 patients (4.9%) underwent major amputation, and 14 patients (6.8%) died (Table 3). Notably, 62 patients (30.2%) remained unhealed at six months without undergoing major amputation or death.
Outcomes of All Patients Admitted with DFUs, Those with a Recurrent DFU and Those with a First-Time DFU, Respectively.
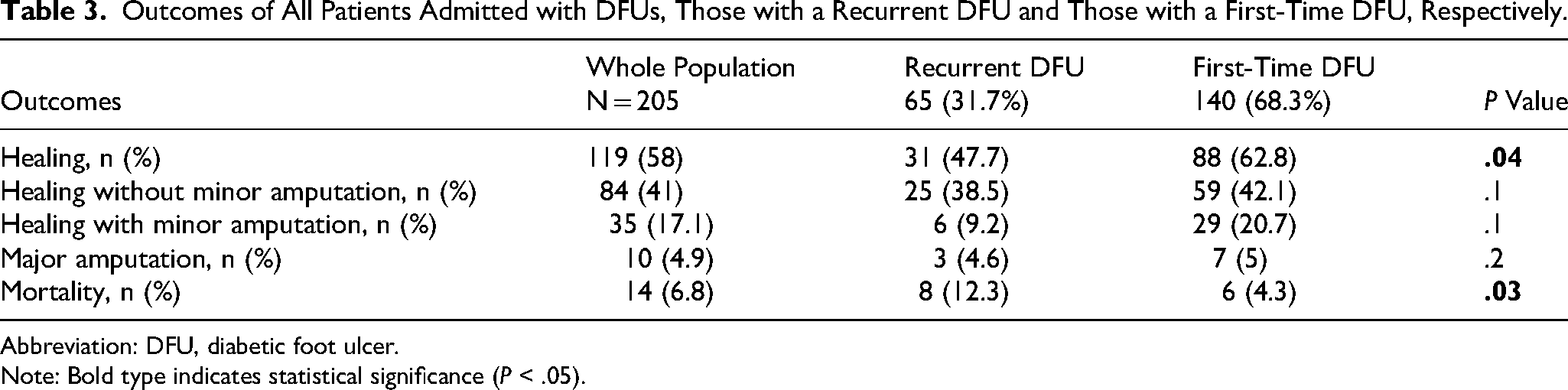
Abbreviation: DFU, diabetic foot ulcer.
Note: Bold type indicates statistical significance (P < .05).
Compared with patients experiencing a first-time DFU, those with a recurrent DFU had a significantly lower healing rate (31 [47.7%] vs 88 [62.8%], P = .04) and a higher mortality rate (8 [12.3%] vs 6 [4.3%], P = .03). No statistically significant difference between the two groups was observed in terms of major amputation (3 [4.6%] vs 7 [5%], P = .2) (Table 3).
Multivariate logistic regression analysis, including all variables identified as potential predictors in the univariate analysis, demonstrated that IHD was independently associated with mortality (OR 2.0, 95% CI 1.6-8.1, P = .009), whereas DFU recurrence was independently associated with non-healing (OR 1.3, 95% CI 1.1-4.7, P = .01) (Table 4).
Multivariate Analysis on Outcomes of Interest of Independent Factors Found at the Univariate Analysis.
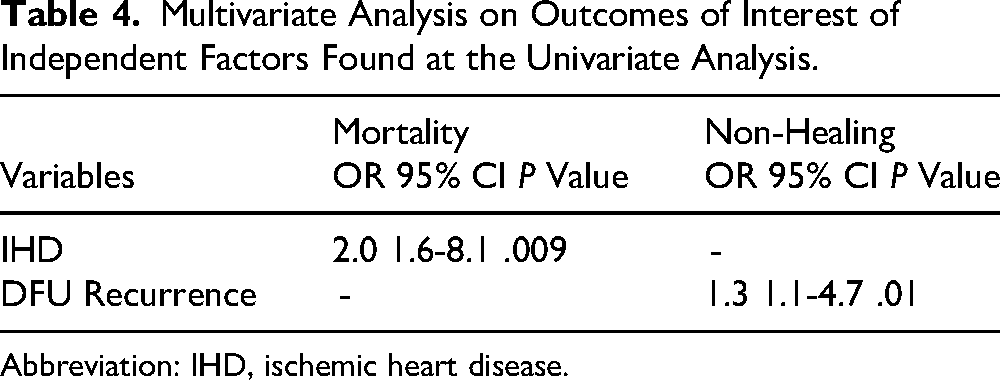
Abbreviation: IHD, ischemic heart disease.
Discussion
In the study cohort, which included patients with DFUs requiring hospitalization, approximately 32% were admitted for a DFU recurrence. Recurrent patients did not differ substantially from those without recurrence for most baseline characteristics, except for a higher prevalence of ischemic heart disease in the recurrent group (50.8 vs 30.7%, P = .006).
Previous studies have consistently shown that ulcer recurrence is a common and serious event in people affected by diabetes.
Armstrong et al described a recurrence rate of approximately 40% in the first year and nearly 65% at five years. 2
In a single-centre follow-up of the Eurodiale study, 18 Dubsky et al reported an overall recurrence rate of 58% among enrolled patients during the subsequent three years of follow-up. Recurrence rates at one, two and three years were 40%, 18% and 13% respectively.12,18
Despite the presence of similar clinical and wound characteristics at the assessment, patients with a recurrent DFU experienced significantly worse outcomes, including reduced healing rate (47.7 vs 62.8%, P = .04), and increased mortality (12.3 vs 4.3%, P = .03), compared to patients presenting a first-time DFU after six months of follow up. In addition, DFU recurrence was an independent predictor of non-healing over the short- to mid-term (6-month follow-up), conferring a 1.3-fold higher risk of non-healing compared with a first-time ulcer.
Although no specific baseline clinical or biochemical variables were identified to fully explain this association, a plausible pathophysiological explanation may involve the cumulative effects of surgical and tissue stress. From a clinical perspective, recurrent ulcers often develop in tissues that have already been exposed to inflammation, ischemia, and previous surgical procedures with prolonged mechanical stress. These factors may lead to structural alterations, such as reduced tissue elasticity and impaired local reparative capacity, resulting in delayed or incomplete wound healing.
Furthermore, it should be noted that although neuro-ischemic DFUs were similarly distributed between the two groups (75.4% vs 75.7%, P = .8), lower-limb revascularization during hospital stay was performed less frequently in patients with recurrent DFUs compared to those with first-time DFUs (46.1% vs 62.1%, P = .03). This finding may be explained by the fact that recurrent patients were more likely to have already undergone revascularization procedures than non-recurrent patients. Nevertheless, this difference may have influenced healing outcomes, as restoration of blood perfusion to the wound enhances the healing process.
Patients with DFU recurrence reported also a higher mortality rate compared to those with a first-time ulcer (12.3 vs 4.3% P = .03) after 6 months of follow up. Nonetheless, DFU recurrence was not independently related to the mortality outcome, whereas cardiovascular disease (specifically ischemic heart disease) was found to be associated with mortality.
Nonetheless, most of the studies investigating DFU recurrence did not find any correlation between cardiovascular disease and DFU recurrence; instead, the risk of recurrence has been primarily attributed to wounds and foot characteristics (deformity, reduced sensitivity, previous osteomyelitis, previous infections).2‐18,12,19
Regardless of the presence of DFU recurrence, the current study documented a notable overall mortality risk (approximately 7%) after 6 months of follow-up among patients previously admitted for DFU. As reported in previous studies, cardiovascular disease (specifically heart failure and ischemic heart disease) emerged as the main risk factor for mortality in patients with DFUs, especially among those with ischemic DFUs requiring hospitalization.20,21
Our data supports the great impact of cardiovascular disease on survival; therefore, it should be emphasized that the increased mortality observed in patients with diabetic foot ulcers is not only attributable to ulcer recurrence but rather reflects the patient's overall systemic condition and comorbid burden. Advanced atherosclerotic disease, including peripheral artery disease and ischemic heart disease, is highly prevalent in this population and represents a major determinant of long-term outcomes.22,23
In fact, beyond the recurrence risk, vascular disease in lower limbs seem to be associated with coronary artery disease. Meloni et al demonstrated that the presence of PAD (mainly below-the-ankle arterial disease) in patients with DFUs is a strong marker of coronary artery disease, suggesting that local ischemia in the foot reflects ischemic processes also in other vascular districts. 24
This finding is easily found in our current data, with over 75% of our cohort affected by DFU and some form of PAD.
Several studies have demonstrated that patients with DFU have a significantly higher risk of cardiovascular events and all-cause mortality compared with diabetic patients without foot ulcers, indicating that DFU is not merely a local complication but a marker of systemic vascular disease and clinical frailty. 23
In the current study, no significant differences were observed in the rate of major amputations between recurrent and non-recurrent patients, which were 4.6% and 5%, respectively (P = .2).
Data from the present study are slightly different from those reported in the existing literature on the topic. A meta-analysis including nearly 10.000 patients reported that patients with recurrent DFUs had a 2.23-fold higher risk of amputation compared to patients with a first-time ulcer. 25 Other strong risk factors included osteomyelitis, gangrene, previous history of ulceration, and smoking. 25
Long-term follow-up studies confirmed the cumulative risk of DFU recurrence: in a Japanese cohort, recurrence rates reached 40.3% at 1 year and 77.1% at 5 years. Importantly, prior amputations (toe or transmetatarsal) increased the likelihood of further ulceration and subsequent amputations, while patients on hemodialysis were also at significantly higher risk. 26
Similarly, a 6.5-year prospective follow-up of patients hospitalized for DFUs showed that 39.8% of those who healed experienced re-ulceration, and 43.8% eventually required an amputation, underscoring the strong link between recurrence and limb loss. 27
Our findings may be partly explained by the implementation of a multidisciplinary management approach and the adoption of advanced surgical and medical strategies aimed at limb preservation.
In particular, the use of modern revascularization techniques, skin grafts, and negative pressure wound therapy has been shown to promote wound healing and reduce the need for major amputations in patients with DFUs.28,29
Therefore, the absence of a higher major amputation rate in our series likely reflects the benefit of an integrated, evidence-based care model that combines advanced wound management techniques with optimized infection control and revascularization strategies, ultimately improving limb salvage outcomes.
These findings have important clinical implications. The high recurrence rates observed, even after apparently successful healing, underscore the need for structured and continuous follow-up of patients with DFUs.
The present study therefore reinforces the concept that ulcer recurrence is not an accidental event, but rather a marker of clinical vulnerability that identifies patients at risk for delayed healing. An inherent limitation of the study is that, beyond location, etiology, and infection status, certain relevant wound characteristics, such as ulcer duration, ulcer size, and the prevalence of previous minor amputations, were not collected; this may limit the ability to fully assess and compare ulcer severity between the two groups and to evaluate its potential impact on clinical outcomes. Additionally, for this study purpose, diabetic peripheral neuropathy was assessed solely using qualitative measures (loss of protective sensation) rather than quantitative evaluation based on specific validated scoring systems (Neuropathy Disability Score or the Michigan Neuropathy Screening Instrument).
While the single-centre retrospective study design, the relatively small sample size, and the mid-term follow-up period may limit the robustness and generalizability of these results, the consistency with previously published data strongly supports the importance of recurrence as a prognostic factor for reduced healing in diabetic foot disease.
Future prospective studies with longer follow-up should aim to further elucidate the mechanisms linking an early intervention, with timely recognition of recurrence risk factors, and a multidisciplinary team approach to develop targeted strategies to reduce burden of DFUs.
Conclusions
Ulcer recurrence in diabetic foot patients requiring hospitalization is significantly associated with reduced chance of healing, while mortality is likely associated with cardiovascular reasons. These findings emphasize the need for intensive follow-up, comprehensive management of cardiovascular comorbidities, and a multidisciplinary approach to improve long-term prognosis in this vulnerable population. Reduction of ulcer recurrence should be a key objective for both clinicians and the scientific community.
Footnotes
Acknowledgements
The global staff of the Unit of Endocrinology and Diabetes, nurses, podologists; University of Rome Tor Vergata, Project Analysis, of new molecular markers in the pathophysiology of diabetes mellitus E82F17000410005 Funded by the European Union - Next Generation EU - NRRP M6C2 - Investment 2.1 Enhancement and strengthening of biomedical research in the NHS
Ethical Considerations
The current study did not require ethical approval according to the local policy.
Informed Consent
Verbal informed consent was obtained from all patients included in the study.
Author Contributions
Salvi and Meloni M. made a substantial contribution to the design of the work; Salvi M. and Bonanni FR made a substantial contribution to the acquisition of data; Meloni M., Salvi M., and Bonanni F.R. made a substantial contribution to the analysis and interpretation of data; Salvi M. wrote the manuscript; Meloni M, Bonanni FR, Uccioli L, Andreadi A., Bellia A, Lauro D. revised critically for important intellectual content.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
Authors have the copyright.