
Abstract
Diabetic foot ulcers (DFU) are associated with impaired wound healing and high morbidity. Er:YAG laser therapy has been proposed as an adjunctive treatment due to its ablative and biostimulatory properties. The aim of this study was to explore the feasibility and preliminary clinical and physiological responses to adjunctive Er:YAG laser therapy in DFUs using hyperspectral imaging (HSI). A pilot study including five patients with DFU was conducted. All patients received Er:YAG laser therapy once weekly for 8 weeks in addition to standard of care. Clinical outcomes included wound area and wound-bed quality assessed using the Wollina wound score. Physiological responses were evaluated using HSI-derived parameters, including tissue oxygen saturation, oxyhemoglobin, deoxyhemoglobin, and total hemoglobin, measured before and after laser treatment sessions. Wound area showed a progressive reduction during follow-up, with a mean percentage wound area reduction of 33.06 ± 44.9% at week 8. Wound-bed condition improved significantly over time, with the Wollina wound score increasing from a median of 5 at baseline to 7 at week 8 (p = 0.024). HSI analysis demonstrated significant and sustained increases in THb and OxyHb at weeks 4 and 8 compared with baseline values (p < 0.05), indicating improved tissue perfusion and oxygen delivery. These preliminary findings suggest that adjunctive Er:YAG laser therapy was feasible and showed promising improvements in wound-bed quality and perfusion-related HSI parameters, alongside clinically meaningful wound size reduction. HSI appears to be a promising tool for the objective assessment of physiological responses to therapy.
Introduction
Diabetic foot ulcer (DFU) is one of the most common and serious complications of diabetes mellitus (DM) and leads to considerable morbidity, elevated mortality risk, and a significant impairment in the quality of life. 1 Globally, the lifetime incidence of DFUs is estimated to range between 19% and 34%, which reflects their considerable epidemiological and clinical burden. 2 The standard of care (SoC) for patients with DFU is grounded in a comprehensive multidisciplinary approach that includes infection control, pressure off-loading devices, assessment and management of peripheral arterial disease (PAD), treatment of comorbidities, metabolic regulation of DM, and appropriate local wound care. 3 In this framework, debridement is a fundamental component of local management as it enables the removal of both viable and non-viable tissue, such as slough, necrotic tissue, biofilm, foreign material, and microorganisms. This process results in better potential and a lower risk of infection. 4
The International Working Group on the Diabetic Foot (IWGDF) identifies sharp debridement as the gold standard for local treatment of DFU due to its rapid and effective removal of devitalized tissue and its overall cost-effectiveness. 5 Nevertheless, it has several important limitations. The procedure is highly operator-dependent and requires substantial technical precision to avoid unnecessary removal of healthy tissue or exposure of deeper structures such as tendons, joint capsules, or bone. 6 Its application is not recommended for patients with poor vascular status or significant procedural pain. 7 In addition, sharp debridement often fails to disrupt biofilm, which is a key factor that contributes to impaired healing of DFUs. 8 These limitations have led to increasing interest in adjunctive techniques that are capable of improving local wound care, including laser-based therapies. 9
Erbium-doped yttrium aluminum garnet (Er:YAG) laser has emerged as a promising adjunctive therapy for the local management of DFUs due to its combined ablative and biostimulative properties. 10 This ablative laser operates at a wavelength of 2940 nm, which is strongly absorbed by tissue water and enables highly selective removal of devitalized tissue. This process occurs through rapid heating of the tissue and explosive vaporization of intracellular water, with surface temperatures exceeding 300 °C.11,12 This mechanism allows effective removal of non-viable tissue and disruption of bacterial biofilm, thereby preserving the integrity of viable structures. 11
In addition, the biostimulation mode with RecoSMA (Reconstructive Spatially Modulated Ablation module for distributing laser radiation into microbeams) technology can be applied to fractionate the laser beam into multiple microbeams, which induces controlled microablation at the wound surface and generates acoustic waves that penetrate deeper tissues.12,13 These effects have been associated with improved microcirculation, fibroblast activation, and stimulation of regenerative mechanisms that are involved in wound healing.10–13 These properties support the use of Er:YAG laser therapy as an adjunctive tool to conventional debridement strategies in the treatment of DFUs.
Conventional assessment of wound healing in DFUs is based on clinical inspection, which may fail to detect early physiological responses to treatment. 14 However, hyperspectral imaging (HSI) based on near-infrared spectroscopy (NIRS) has emerged as a non-invasive technique for the objective evaluation of tissue oxygenation and hemoglobin distribution. 15 The SnapshotNIR system enables real-time assessment of tissue oxygen saturation (StO₂), oxyhemoglobin (OxyHb), deoxyhemoglobin (DeoxyHb), and total hemoglobin (THb) providing quantitative information on perfusion and oxygen delivery in the wound area. 16 Previous studies have demonstrated the potential value of HSI in assessing healing prognosis and microvascular status in patients with DFUs. 17 Given the limited clinical evidence integrating Er:YAG laser therapy with objective physiological monitoring in this population, a pilot study design was chosen to explore feasibility and generate preliminary clinical and physiological data. Therefore, the aim of this pilot study was to explore the feasibility and preliminary clinical and microvascular responses to adjunctive Er:YAG laser therapy in DFUs using HSI.
Materials and Methods
Study Design and Participants
This prospective pilot study was conducted at a specialized diabetic foot unit between May and November 2025. The study included patients with DFUs that were treated with Er:YAG laser therapy as an adjunct to SoC. All participants provided written informed consent prior to inclusion, and ethical approval was obtained from the local ethics committee. The study was also conducted in accordance with the principles of the Declaration of Helsinki. 18
The inclusion criteria were patients over 18 years old with type 1 or type 2 diabetes and adequate metabolic control within 3 months prior to enrollment. Adequate control was defined as HbA1c < 10% (85.8 mmol/mol). Additional eligibility criteria included the presence of DFUs with a duration of 1–24 months and a wound area of 1–30 cm2 at baseline. DFUs were classified according to the University of Texas Wound Classification System and were required to be categorized as IA, IIA, IC, or IIC. 19
Vascular inclusion criteria included an ankle-brachial index (ABI) > 0.9. In cases where ABI ≤ 0.9, inclusion required a Toe-Brachial Index (TBI) > 0.7. If TBI was ≤0.7, patients were elegible only if ankle systolic blood pressure (ASBP) was ≥70 mm Hg or toe systolic blood pressure (TSBP) was ≥50 mm Hg. 20 The exclusion criteria comprised local clinical infection defined by the Infectious Diseases Society of America (IDSA) guidelines, 21 critical limb ischemia, 20 suspected diabetic foot osteomyelitis, or a life expectancy of less than 6 months. Patients were also excluded if they were pregnant or lactating or had hepatitis, human immunodeficiency virus (HIV) infection, or other local/systemic conditions that are known to impair wound healing.
Clinical Assessment
At baseline, all patients underwent a standardized clinical assessment that was performed by the same clinician. Demographic data and relevant medical history were obtained from medical records, including the type and duration of DM, the presence of diabetes-related complications, and history of previous ulcerations or amputations. Glycemic control was evaluated using plasma glucose and HbA1c values from the most recent blood analysis. DFUs were classified at baseline according to the University of Texas Wound Classification System and the SINBAD classification system. 22 Ulcer characteristics, including location and duration of evolution, were documented prior to initiation of laser therapy.
Neurological assessment was performed using a Biothesiometer and a Semmes–Weinstein 5.07/10 g monofilament (Novalab Ibérica, Madrid, Spain). Patients who failed to perceive at least one of the two tests were diagnosed with diabetic peripheral neuropathy. 23 Vascular evaluation included palpation of distal pulses and measurement of the ABI, TBI, and transcutaneous oxygen pressure (TcPO₂). Brachial and ankle systolic blood pressures were measured using an 8-MHz handheld Doppler device (Huntleigh Healthcare Ltd, Cardiff, UK), while toe systolic blood pressure was assessed by digital plethysmography (Systoe, Atys Medical, Madrid, Spain). TcPO₂ measurements were obtained using a TCM4 device (Radiometer, Copenhagen, Denmark). PAD was diagnosed in cases of absent distal pulses with ABI < 0.9 or in cases with non-compressible arteries (ABI > 1.3) or normal ABI values with TBI < 0.7 and TcPO₂ < 30 mm Hg.20,24
Er-YAG laser Intervention (Ablation and Biostimulation)
Er:YAG laser therapy (MultilineTM, LINLINE Medical Systems Ltd, Riga, Latvia), was applied once weekly over an 8-week follow-up period using two sequential modalities. All procedures were performed using standard laser-safety conditions, and both the clinician and the patient wore appropriate protective eyewear. The first stage consisted of the laser ablative mode to remove devitalized tissue and microbial biofilm from the wound bed. Laser radiation was delivered over the wound surface in a controlled scanning pattern with energy density ranging from 5 to 10 J/cm2 and a repetition rate of 3 Hz. The completion of the ablative phase was based on the presence of capillary bleeding, which indicated adequate removal of non-viable tissue.
The second stage was carried out using the laser biostimulation mode with RecoSMA technology. This modality fractionates the Er:YAG laser beam into multiple microbeams and generates laser-induced acoustic waves through controlled microablation of the tissue surface. The purpose of this stage is to stimulate local regenerative processes once the wound bed is free of devitalized tissue. The energy density for the RecoSMA treatment ranged from 2 to 4 J/cm2 and was applied to both the wound bed and the surrounding tissue over an area of approximately 3–5 cm2. 12 After each laser session, a dry gauze dressing was applied to the wound surface.
All patients received SoC for DFUs management in accordance with the IWGDF guidelines. 3 In addition to the laser therapy, sharp debridement was performed using a scalpel when clinically indicated to remove non-viable tissue, peri-wound calluses, or maceration. Local wound care was based on moist wound dressings, and in all cases, a removable knee-high device was used for off-loading.
Hyperspectral Imaging Procedure
HSI was performed using the SnapshotNIR system (Kent Imaging Inc., Calgary, Canada), which is a handheld NIRS-based hyperspectral camera that has been designed for the non-invasive assessment of tissue oxygenation and perfusion. 17 Imaging was conducted at baseline and during follow-up visits at weeks 4 and 8. At each visit, HSI was performed under standardized conditions. The camera was positioned perpendicular to the wound surface at a fixed distance in accordance with the manufacturer's recommendations. Prior to any intervention, a baseline HSI of the wound was acquired. Subsequently, Er:YAG laser therapy was applied according to the study protocol, followed by a second HSI acquisition after the laser session.
The SnapshotNIR software enables real-time image acquisition and analysis. For each image, the periwound area was manually delineated to define a region of interest corresponding to the DFU. Within this predefined region, the software automatically calculates quantitative values of StO₂, OxyHb, DeoxyHb, and THb. 25 In addition to numerical outputs, the system generates colorimetric maps of the spatial distribution, which enable visual assessment of perfusion and oxygenation patterns. All images were stored digitally, and identical acquisition settings and procedures were applied throughout the study to minimize measurement variability.
Outcome Measures
The outcome measures included clinical and physiological variables. The clinical outcomes focused on the DFUs evolution and were assessed through changes in wound area and wound-bed characteristics. Wound area was measured at weeks 1, 4, and 8 using digital planimetry with the SnapshotNIR system. The percentage of wound-area reduction was calculated by comparing baseline measurements with those obtained at week 8: ((wound area week 1 – wound area week 8)/wound area week 1) × 100.
Wound-bed condition was evaluated using the validated Wollina wound-scoring system, which assesses the presence, quality, and consistency of granulation tissue with scores ranging from 0 to 7. 26 Physiological outcomes were evaluated using HSI. StO₂, OxyHb, DeoxyHb, and THb were quantitatively measured in the predefined wound region of interest using the SnapshotNIR system. These parameters were obtained at weeks 1, 4, and 8 both before and after Er:YAG laser therapy at each visit for the evaluation of changes in tissue perfusion and oxygenation.
Statistical Analysis
All statistical analyses were performed using SPSS software version 30.0 (IBM Corp., Armonk, NY, USA). Given the exploratory nature of this pilot study, no formal sample size calculation was performed, and statistical analyses were considered descriptive and hypothesis-generating. Qualitative variables were described using frequency distributions and percentages. The normality of continuous variables was assessed using the Shapiro–Wilk test. Normally distributed continues variables were reported as the mean and standard deviation (SD), while non-normally distributed variables were expressed as the median and interquartile range (IQR).
To compare normally distributed quantitative variables in related samples, a paired Student's t-test and repeated-measures analysis of variance (ANOVA) were performed. For non-normally distributed variables, the Friedman test and Wilcoxon test were implemented. When statistically significant differences were detected, post hoc pairwise comparisons with Bonferroni correction were performed. Statistical significance was established at p < 0.05 with a 95% confidence interval; however, p-values should be interpreted cautiously given the pilot design.
Results
This prospective pilot study included five patients with DFUs. Table 1 summarizes their baseline demographic characteristics, diabetes-related complications, vascular status, and DFUs characteristics.
Baseline Characteristics of Patients and Their DFUs.
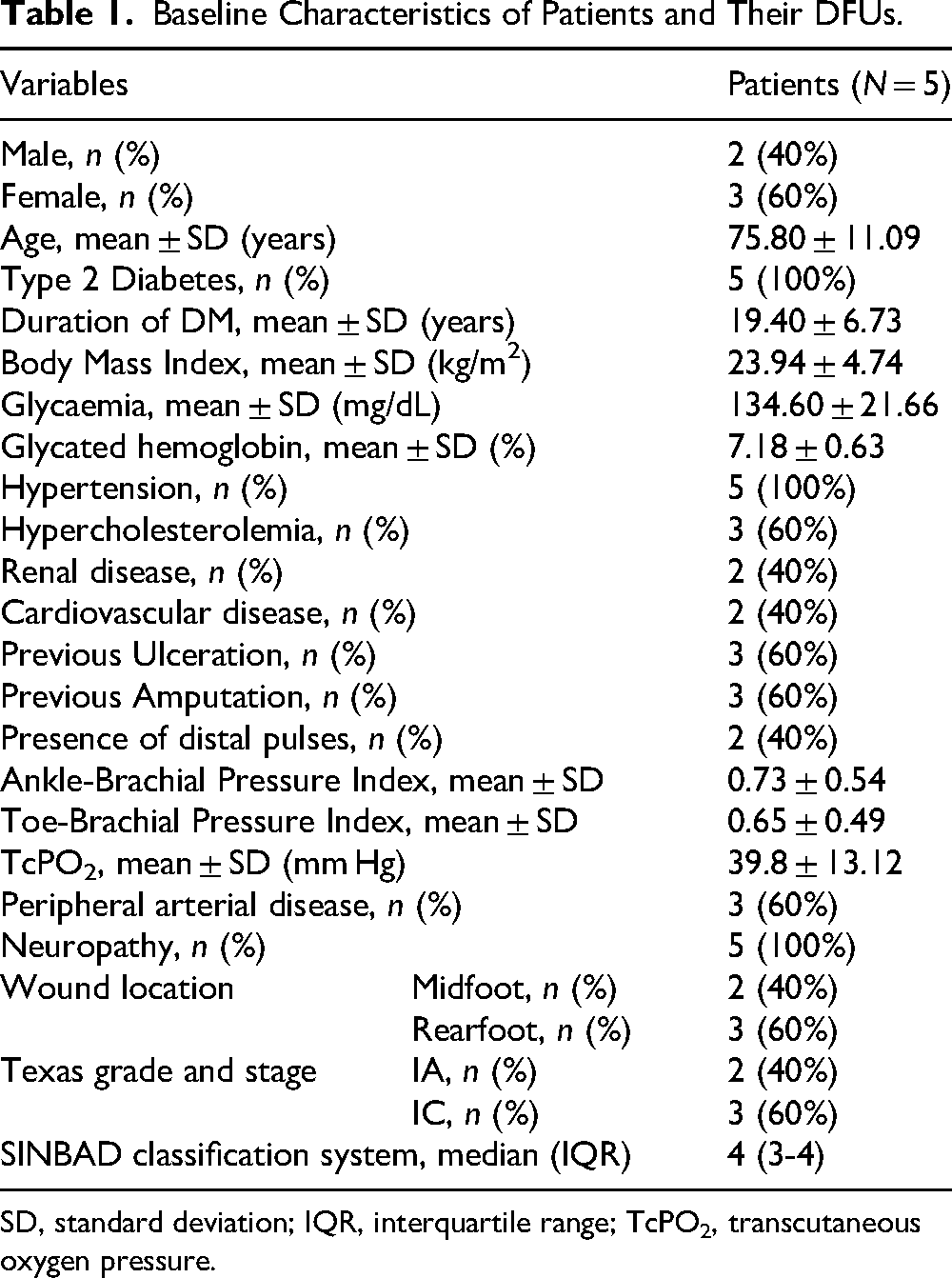
SD, standard deviation; IQR, interquartile range; TcPO2, transcutaneous oxygen pressure.
Clinical Outcomes
The changes in clinical outcomes are presented in Table 2. Wound area showed a progressive reduction from week 1 to week 8, but no statistically significant differences were observed between time points (p = 0.307). Likewise, the paired comparison between baseline and week 8 demonstrated a trend toward wound-area reduction but without reaching statistical significance (p = 0.061). Despite this, a clinically meaningful reduction was observed during follow-up. At week 8, the mean percentage of wound-area reduction was 33.06 ± 44.9%, indicating a relevant decrease in wound size over the study period.
Clinical Outcome Measures During Follow-up.
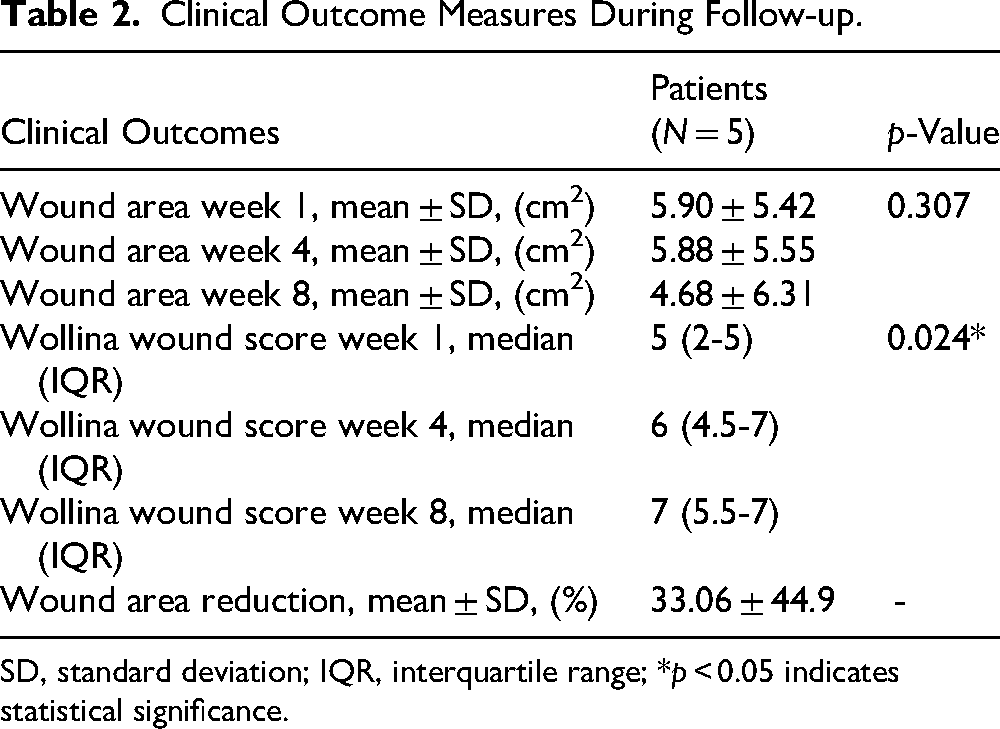
SD, standard deviation; IQR, interquartile range; *p < 0.05 indicates statistical significance.
A significant improvement in wound-bed condition was observed over time. The Wollina wound score significantly increased from 5 (2-5) at week 1 to 7 (5.5-7) at week 8 (p = 0.024). Individual patient trajectories of the Wollina wound score are illustrated in Figure 1, which shows a consistent upward trend across visits that reflects progressive improvement in granulation tissue presence, quality, and consistency.
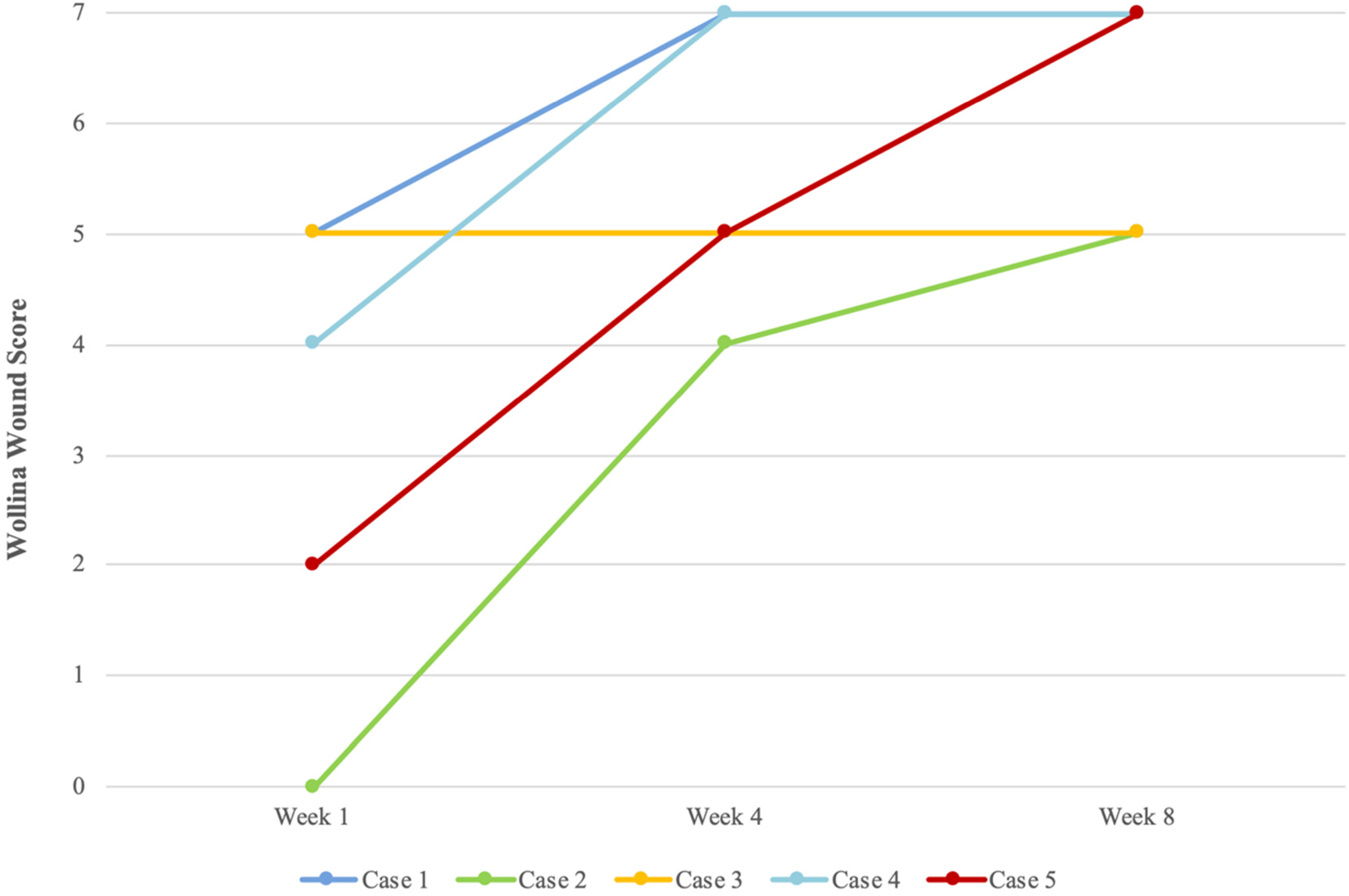
Individual Evolution of the Wollina Wound Score Throughout the Study Period.
The physiological outcomes obtained with HSI are summarized in Table 3. For longitudinal exploratory analysis, values obtained before Er:YAG laser treatment at week 1 were compared with those collected after the laser sessions at weeks 4 and 8. Statistically significant increases in THb and OxyHb were observed, particularly at weeks 4 and 8 compared with baseline values (Table 3).
Physiological Outcome Measures Obtained with HSI During Follow-up.
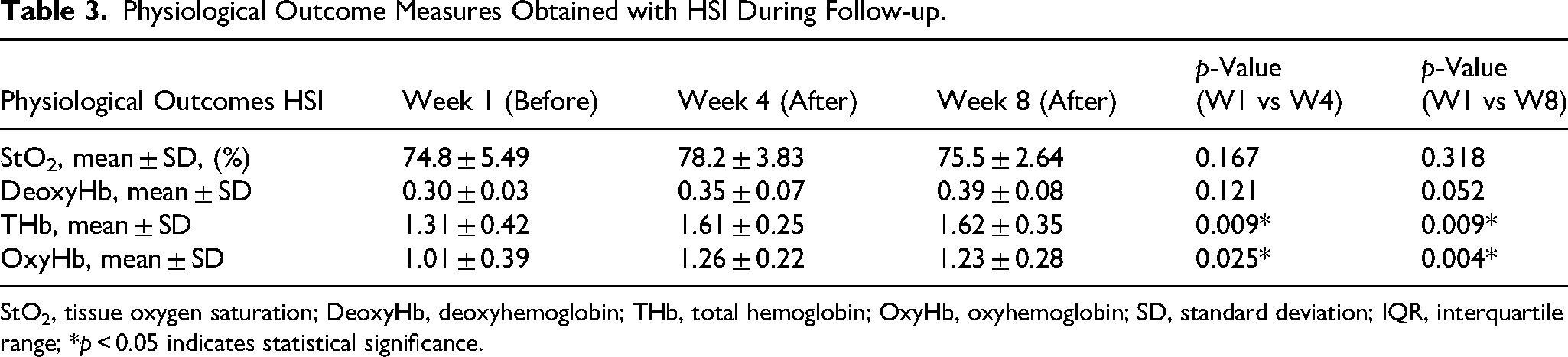
StO2, tissue oxygen saturation; DeoxyHb, deoxyhemoglobin; THb, total hemoglobin; OxyHb, oxyhemoglobin; SD, standard deviation; IQR, interquartile range; *p < 0.05 indicates statistical significance.
In contrast, DeoxyHb showed a non-significant upward trend (week 4: p = 0.121; week 8: p = 0.052), and no statistically significant changes were detected in StO₂ at week 4 (p = 0.167) or week 8 (p = 0.318). The changes in THb and OxyHb values over time are shown in Figure 2, which illustrates a change in perfusion-related parameters following Er:YAG laser therapy. These results are consistent with improved tissue perfusion and oxygen delivery over the course of treatment. Figure 3 presents a representative clinical case with corresponding HSI maps at week 1 and week 8. The maps visually demonstrate an increase in perfusion-related parameters (particularly THb and OxyHb), which aligns with the quantitative findings.
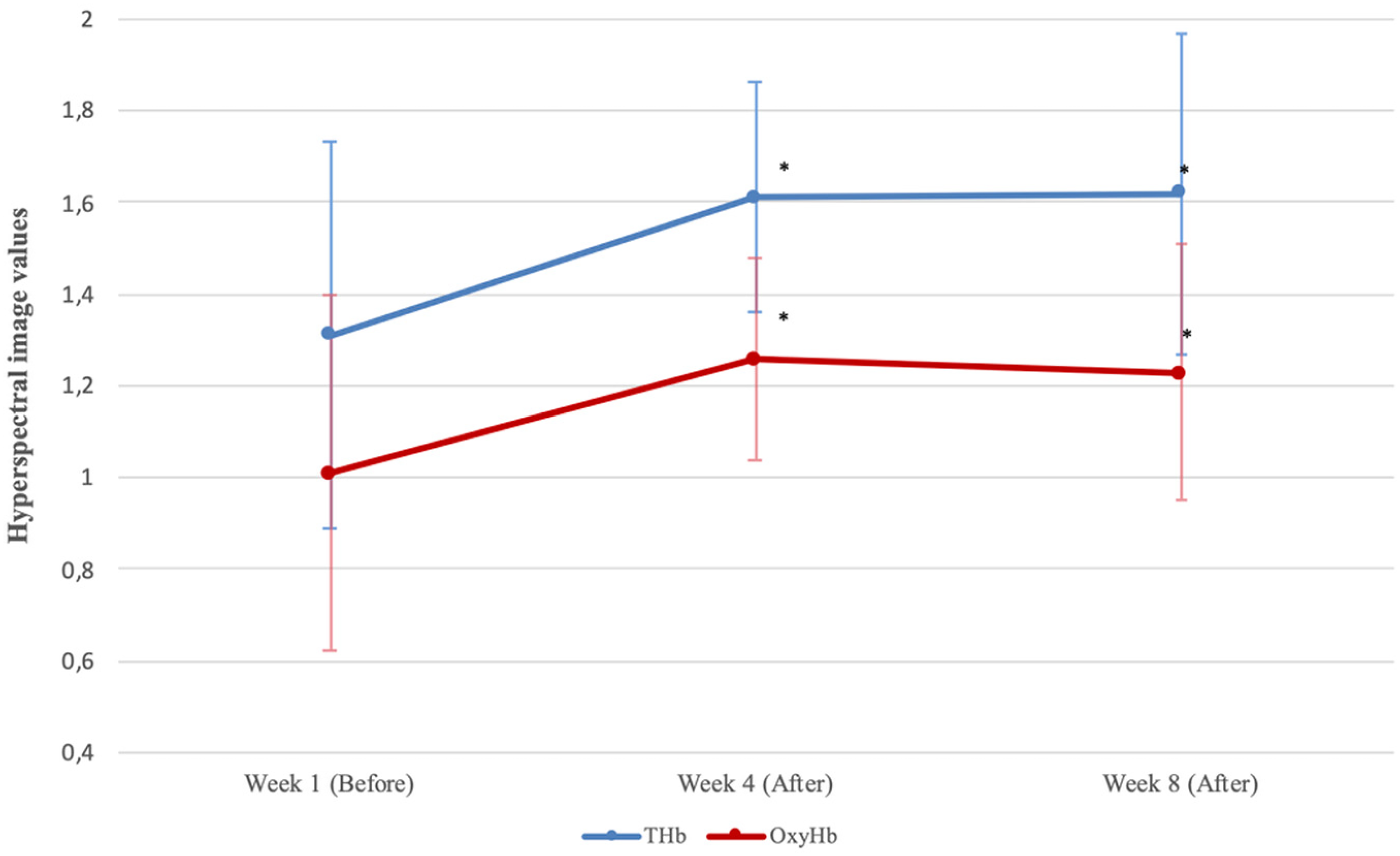
Changes in Perfusion-Relates HSI Parameters (THb and OxyHb). THb, Total Hemoglobin; OxyHb, Oxyhemoglobin. Values were Obtained Before Treatment at Week 1 and After Treatment at Weeks 4 and 8. *p < 0.05 Indicates Statistical Significance.

Representative Clinical Image and Corresponding HSI Maps Obtained at Week 1 and Week 8 Following Er:YAG Laser Therapy THb, Total Hemoglobin; OxyHb, Oxyhemoglobin. a, Clinical Image at Week 1; b, THb Map at Week 1; c, OxyHb Map at Week 1; d, Clinical Image at Week 8; e, THb Map at Week 8; f, OxyHb Map at Week 8. In the HSI Maps, Warmer Colors (Red/Orange) Indicate Higher Perfusion and Oxygenation Values, Whereas Cooler Colors (Blue/Green) Indicate Lower Values.
Discussion
Our findings suggest that Er:YAG laser therapy for DFUs was associated with improvements in wound-bed quality, a clinically meaningful reduction in wound area, and favorable changes in perfusion-related HSI parameters (specifically THb and OxyHb). From a clinical perspective, progressive reduction in wound area was observed throughout follow-up. Although this reduction did not reach statistical significance when analyzed longitudinally, this finding should be interpreted cautiously given the small sample size and the short follow-up period.
Importantly, the mean percentage of wound-area reduction at week 8 of approximately 33% may represent a clinically relevant improvement and appears consistent with reductions reported in previous studies.11,13 In contrast to wound area, wound-bed condition demonstrated a clear and statistically significant improvement over time, as evidenced by the increase in the Wollina wound score (5 (2-5) at week 1, 6 (4.5-7) at week 4, and 7 (5.5-7) at week 8; p = 0.024). These results suggest improvements in the presence, quality, and consistency of granulation tissue. The improvements could potentially be related to the reported biostimulatory effect of Er:YAG laser therapy, which has been associated with fibroblast activation and collagen synthesis in wound areas.12,27
To our knowledge, this is the first study to evaluate the effects of Er:YAG laser therapy for DFUs using HSI. Regarding physiological outcomes, a statistically significant increase in THb and OxyHb were observed when comparing baseline measurements obtained before laser therapy with post-treatment measurements at weeks 4 and 8 (Table 3). Conversely, DeoxyHb and StO₂ didnot show statistically significant changes during follow-up.
From a physiological perspective, THb reflects local blood volume and capillary density, while OxyHb represents effective oxygen delivery to the tissue. Therefore, both parameters may reflect an improvement in microvascular perfusion and vascular activity. Moderate increases in DeoxyHb are consistent with increased metabolic activity associated with tissue regeneration, while stable StO₂ likely reflects a balance between oxygen supply and consumption during early phases of healing. 25
HSI parameters should not be interpreted in isolation but rather as part of a dynamic system that reflects the balance between oxygen supply, consumption, and microvascular distribution. The observed HSI profile characterized by a significant increase in OxyHb and THb with stable StO₂ and changes in DeoxyHb is compatible with physiological patterns described in the literature as being associated with active wound healing.16,25,28 The representative case further supports the quantitative findings and demonstrates visible increases in perfusion-related parameters on HSI maps alongside clinical improvement of the wound (Figure 3). The images highlight the potential role of HSI as an early marker of therapeutic response with the capability of detecting changes in tissue oxygenation and perfusion that may not be readily perceived through standard clinical assessment.
Several limitations of this pilot study should be acknowledged. The small sample size and exploratory design limit the generalizability of the findings and preclude definitive conclusions regarding efficacy or causality. Furthermore, the absence of a control group receiving SoC alone prevents isolation of the specific effects attributable to Er:YAG laser therapy. The limited availability of comparable studies using HSI in this clinical context also restricts direct comparison of physiological outcomes.
Although improvements in wound-bed quality and perfusion-related HSI parameters were observed, complete wound healing was not achieved during the 8-week follow-up period, and wound-area reduction did not reach statistical significance. These findings may be related to the small sample size and relatively short follow-up duration, which may have limited the ability to detect complete epithelialization outcomes.
Despite these limitations, this exploratory pilot study provides preliminary insights into the potential role of Er:YAG laser therapy as an adjunctive treatment in DFUs and supports the feasibility of integrating HSI into clinical assessment. Future research should involve larger controlled trials to confirm these findings, determine whether the early physiological changes detected by HSI are associated with long-term healing outcomes and individualized therapeutic decision-making, and evaluate whether combined approaches integrating laser therapy with other advanced interventions, such as hyperbaric oxygen therapy or regenerative strategies, may further enhance wound healing and epithelialization in DFUs.
Conclusion
Er:YAG laser therapy as an adjunctive treatment in DFUs was associated with improvements in wound-bed quality, clinically meaningful reductions in wound area, and increases in perfusion-related HSI parameters (specifically THb and OxyHb). The observed physiological profiles may reflect changes in tissue perfusion and oxygen delivery that are compatible with patterns described in active wound healing. HSI appears to be a feasible and promising tool for the objective and early assessment of wound response to therapy. This study provides preliminary evidence supporting the potential role of Er:YAG laser therapy in the management of DFUs, but larger controlled studies are needed to validate the findings and elucidate whether early changes in HSI-derived parameters can predict long-term healing outcomes.
Footnotes
Acknowledgments
None declared.
ORCID iDs
Ethics Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of Hospital Clínico San Carlos, Madrid, Spain (protocol code [C.P.-C.I. 25/766-IC_P_CE].
Authorship Contribution Statement
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.