
Abstract
Introduction
The treatment of chronic non-healing wounds represents a great challenge in healthcare, especially in rehabilitation medicine, as it contributes significantly to increased patient mortality and morbidity. Various types of laser therapies have shown to enhance wound- healing potential while remaining safe and easy to administer.
Objective
This prospective comparative study aimed to evaluate the efficacy of the Safe Laser 1800 Infra therapy compared with conventional wound treatment protocols in cases of patient with impaired wound healing.
Methods
Patients in the control group received conventional wound care, consisting of wound toilette and the application of hydro- responsive wound dressings (Hydro- Clean Advance, Hartmann) for both groups. Patients in the Safe Laser group received laser treatment at least three times per week, with 1-3 minof exposure per treatment point.
Results
In the Safe Laser group 7 out of 10 patients became free of inflammation, while inflammation was markedly reduced in the remaining 3 cases. In 90% of patients in the Safe Laser group wound dimensions were substantially reduced or complete wound healing was achieved. Wound depth decreased in all cases. In contrast, in the control group inflammation did not improve, while wound dimensions showed only minimal reduction in only one case.
Conclusion
Despite the small sample size and heterogeneous wound characteristics, Safe Laser 1800 Infra therapy demonstrated significant benefits in reducing both wound dimensions and inflammation when compared to conventional treatment protocols used in our facility.
Keywords
Introduction
Chronic non-healing wounds, including diabetic foot ulcers (DFUs), amputation wounds and pressure ulcers represent a major burden for healthcare systems, especially in rehabilitation medicine.
Normal wound healing consists of four distinct phases: hemostasis, inflammation, proliferation and remodeling. Specific cell types play key roles in each phase, ultimately leading to scar tissue formation. 1 In chronic non-healing wounds, one or more steps of this process become impaired. In diabetes mellitus, advanced glycosylation end products (AGEs) reduce cellular activity, resulting in a prolonged inflammatory phase, delaying healing, thereby resulting in chronic wounds. 2 DFUs are among the most common and serious complications of diabetic patients caused by the classical triad of neuropathy, trauma and ischemia, combined with impaired healing capacity.2,3 Infection frequently develops during the course of the diabetic foot disease, often leading to amputation.4-6
The healing of amputation wounds is challenging due to already compromised peripheral circulation and reduced regenerative capacity- the same factors that often necessitated the amputation in the first place. 7 Early prosthetic use is widely regarded as beneficial, as it lowers morbidity and improves quality of life and productivity. 8 However poor post-amputation scar healing can delay prosthetic fitting, and prolong rehabilitation, increase healthcare cost, and reduce both quality of life and productivity. 9 While conventional treatment may eventually result in wound closure, adjuvant low level laser therapy (LLLT)has been reported to significantly shorten healing time. 10 Thus allowing faster prosthetic use and earlier discharge.
Pressure ulcers typically develop in chronically ill or immobilized patients due to prolonged pressure and shear stress leading to local hypoxia and tissue necrosis especially over bony prominences, where external pressure exceeds capillary pressure. 11
Conventional bandage therapies often result in minimal improvement, and only prevent further deterioration. 12 In contrast, the addition of LLLT to standard wound care has been shown to be an effective, safe and easy to administer option for such chronic wounds. 13
LLLT, also commonly referred to as photobiomodulation uses monochromatic, low intensity light in the 300 to 10.600 nm wavelength range, with maximum power output between 0.001 to 0.1 W, a pulse rate of 0 (continuous) to 5000 Hz and a maximum intensity of 0.01 to 10 W/cm2 and dose of 0.01 to 100 J/cm2. 14 Doses between 3–6 J/cm2 are generally more effective than higher doses, and wavelengths of 630 and 1000 nm are most consistently associated with enhanced healing effect. 15 The Safe Laser 1800 Infra device uses infrared light at 808 nm, which falls within this optimal range.
Various types of lasers have been used to administer LLLT, including Argon (488 and 514 nm), Helium-Neon (632.8 nm) and Gallium-Aluminum-Arsenide (805 or 650 nm) lasers. 14
The mechanism of action of LLLT can be found on the cellular level: it reduces inflammatory mediator release, enhances epithelial cell motility, stimulates lymphocyte, and macrophage activity, -leading to better phagocytosis- and improved fibroblast proliferation, resulting in faster granulation tissue formation. 15 On a subcellular level, LLLT increases mitochondrial adenosine triphosphate (ATP) production, thereby enhancing the activity of cells essential to wound repair and accelerating healing, thus resulting in faster healing times.16,17 Furthermore increased collagen production contributes to tissue regeneration, while the reduction of inflammatory mediators may explain the associated pain relief. 16
Beyond chronic wound treatment, LLLT has also been applied successfully in bone fracture treatment, as well as in maxillofacial surgery.18,19
Our study aimed to evaluate the efficiency and effectiveness of Safe Laser 1800 Infra low- level laser therapy in the biomodulation and healing of various chronic non-healing wounds, including DFUs, amputation scars and other ulcers.
Patients and Methods
A total of 20 patients were prospectively enrolled and divided into two groups of 10 each: a Safe Laser and Standard treatment group, both comprising of patients with various types of chronic wound- healing defects. Patients in the Safe Laser group received treatment using the Safe Laser 1800 Infra device, which operates at an 808 nm wavelength with a maximum power output of 1800 mW. Patients in both groups received conventional wound care consisting of wound debridement and the application of hydro- responsive wound dressings (Hydro- Clean Advance, Hartmann). Laser treatment was administered at each dressing change for the laser group, with a minimum frequency of 3 times per week, which corresponded to a total of 12–20 treatment sessions per patient during this 4- 8-week treatment period. Each treatment lasted 1–3 min per treatment point delivering approximately a total of 110J per 11,22 cm2 of tissue area per minute. All patients were treated in the same facility (Rehabilitation Centre of the Central Hospital of Northern Pest–Military Hospital), by the same team of trained nurses, who also performed standardized photographic documentation of wounds before and after the treatment period. Wound size was calculated using artificial intelligence (AI)-based algorithms integrated in Adobe Photoshop (PS) AI cloud (Adobe Inc., 2025), while wound depth was estimated through using visual approximation by the clinical staff. Data collection and treatment protocol was carried out in the above-mentioned Rehabilitation Centre of the Central Hospital of Northern Pest–Military Hospital of Hungary Rehabilitation Centre.
Statistical analysis was carried out using scipy.stats, python package (SciPy v.1.16.2).
Results
Patient demographics: in the Safe Laser group, the female-to-male ratio was 9:1, while in the control (standard treatment) group it was 7:3. The mean age of patients in the Safe Laser group was 73.1 years (min-max range: 54–89) while in the standard treatment group it was 72.8 years (min-max range 57–93).
Statistical analysis strongly supports the effectiveness of the treatment. The Safe Laser group showed significantly greater improvement than the conventionally treated control group.
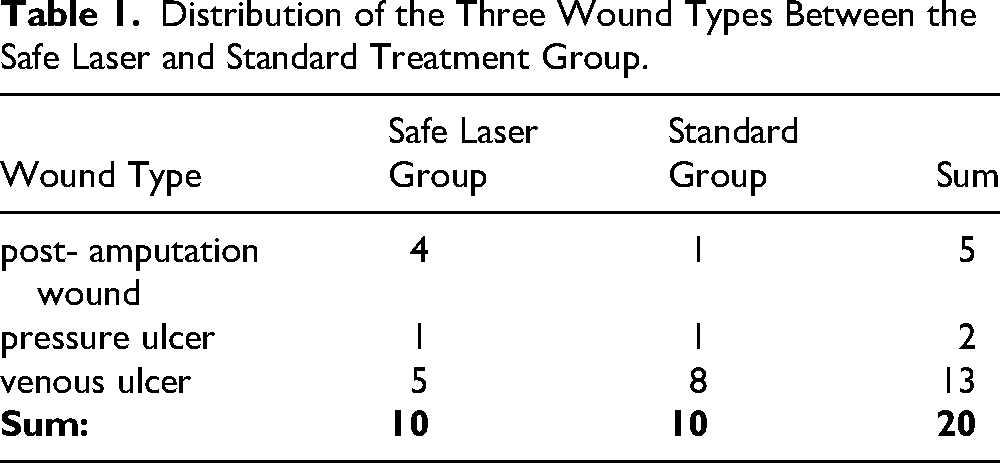
Three types of wounds were included in both groups: post- amputation wounds, pressure ulcers and chronic venous ulcers in both groups adding up to the total of 20 patients included. (Table 1)
Distribution of the Three Wound Types Between the Safe Laser and Standard Treatment Group.
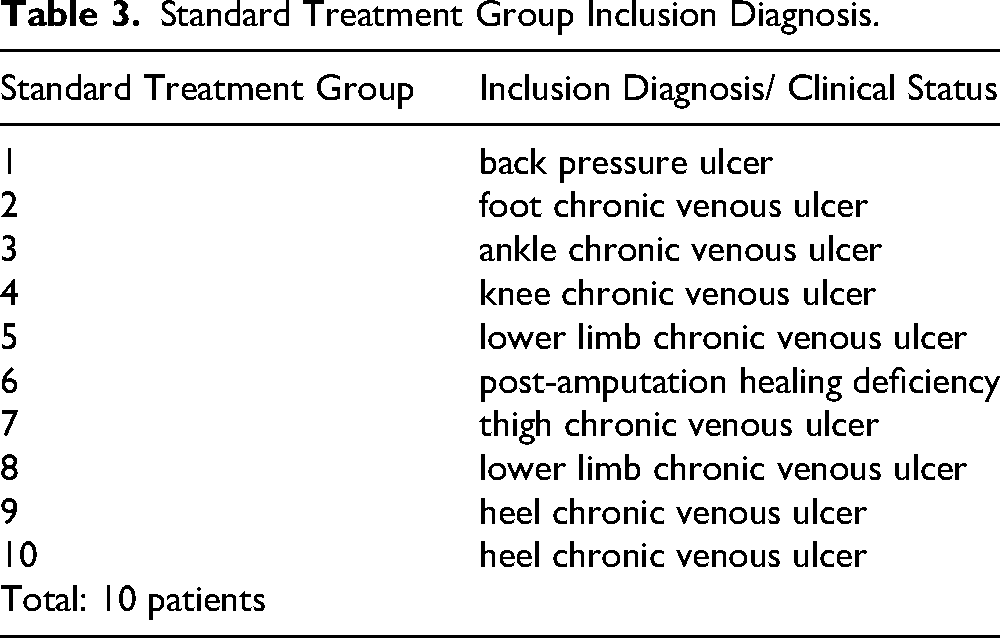
Tables 2 and 3 contain would types for each group.
Safe Laser Group Inclusion Diagnosis.
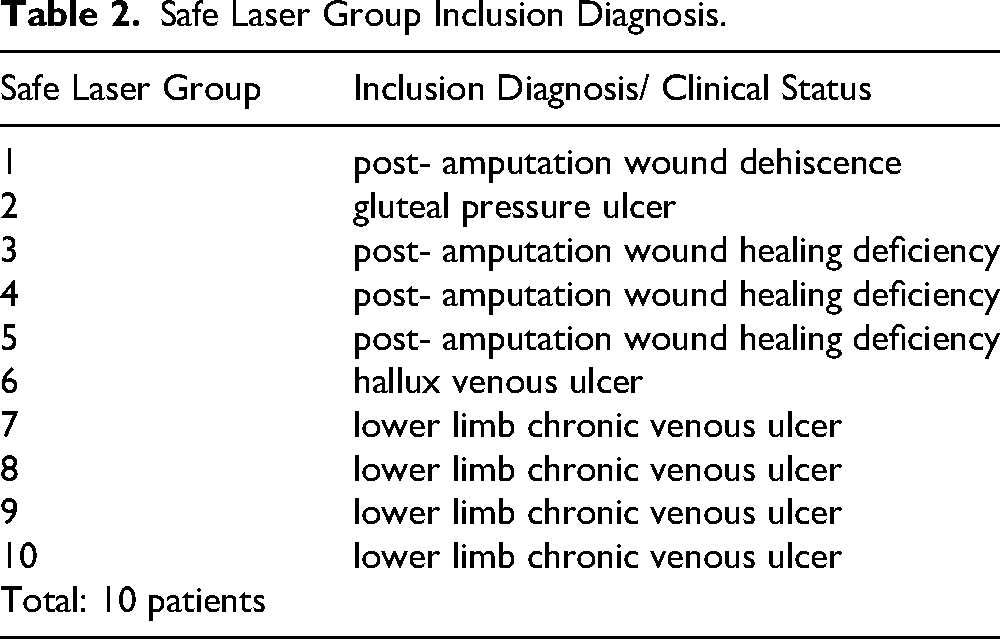
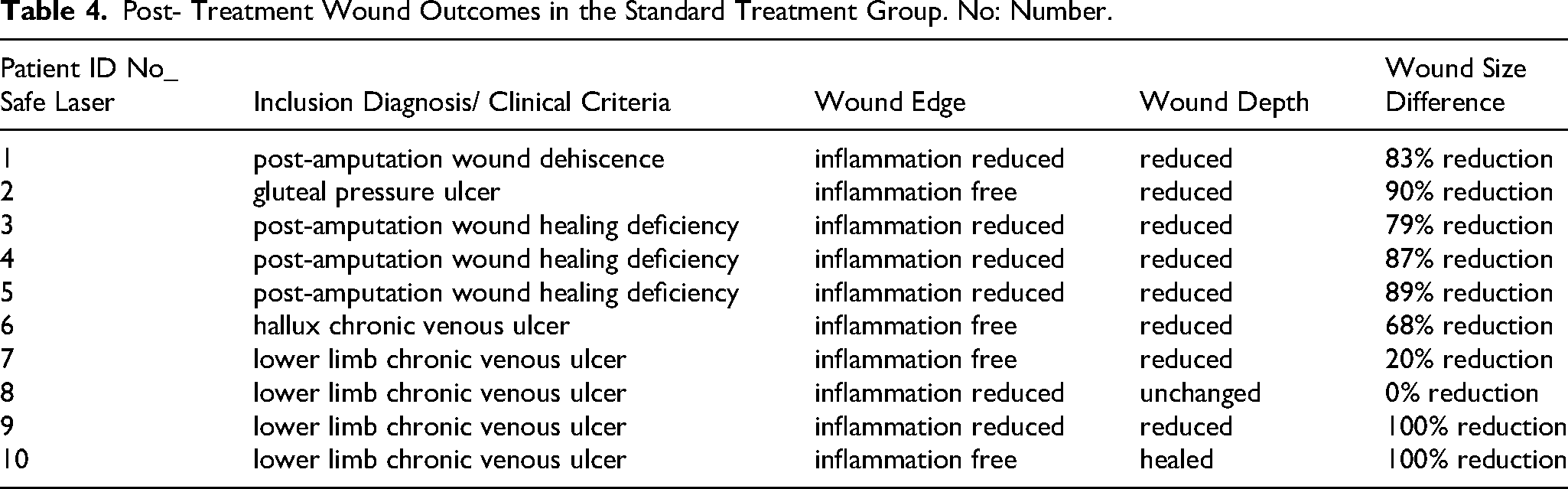
Tables 2 and 3 contain pre-treatment status and diagnosis, while table 4 contains post-treatment status. 4 out of 10 patients’ wounds in the Safe Laser group became inflammation free, while in 6 out of 10 patients’ inflammation was reduced based on visual estimation. A substantial reduction in both wound depth and size could be achieved. Specifically wound depth was reduced or completely healed in 9 out of 10 patients in the Safe Laser group, compared with only 1 out of 10 cases in the control (standard treatment) group. The average wound size decreased by 71.6% in the Safe Laser group, whereas it showed a mean change of −4% in the control group. Although some patients in the control group exhibited mild improvement, several experienced worsening of their wounds during the study period.
Standard Treatment Group Inclusion Diagnosis.
Treatment efficiency on wound area was assessed by comparing wound area pre- and post-treatment in the Safe Laser and control groups respectively. Since there is an outlier in the Safe Laser group, it is worth calculating the median in addition to the mean. The Safe Laser group demonstrated significantly greater wound reduction, with a mean final wound area percentage of 28.4% (35.1 SD) and a median of 15.0%. In contrast, the standard treatment group showed an average increase in wound size, with a mean final percentage of 103.7% (32.7 SD) and a median of 96.5%. Since we have a small sample size (n = 10) and the data is not normally distributed, we use the Mann-Whitney U test. This test compares the ranks of the two groups. The result of the analysis is statistically significant. The p-value is p = 0.0085, which is less than 0.05. Statistical analysis strongly supports the effectiveness of the treatment. The Safe Laser group showed significantly greater improvement than the conventionally treated control group (Tables 4–5).
Post- Treatment Wound Outcomes in the Standard Treatment Group. No: Number.
Post- Treatment Wound Outcomes in the Standard Treatment Group. No: Number.
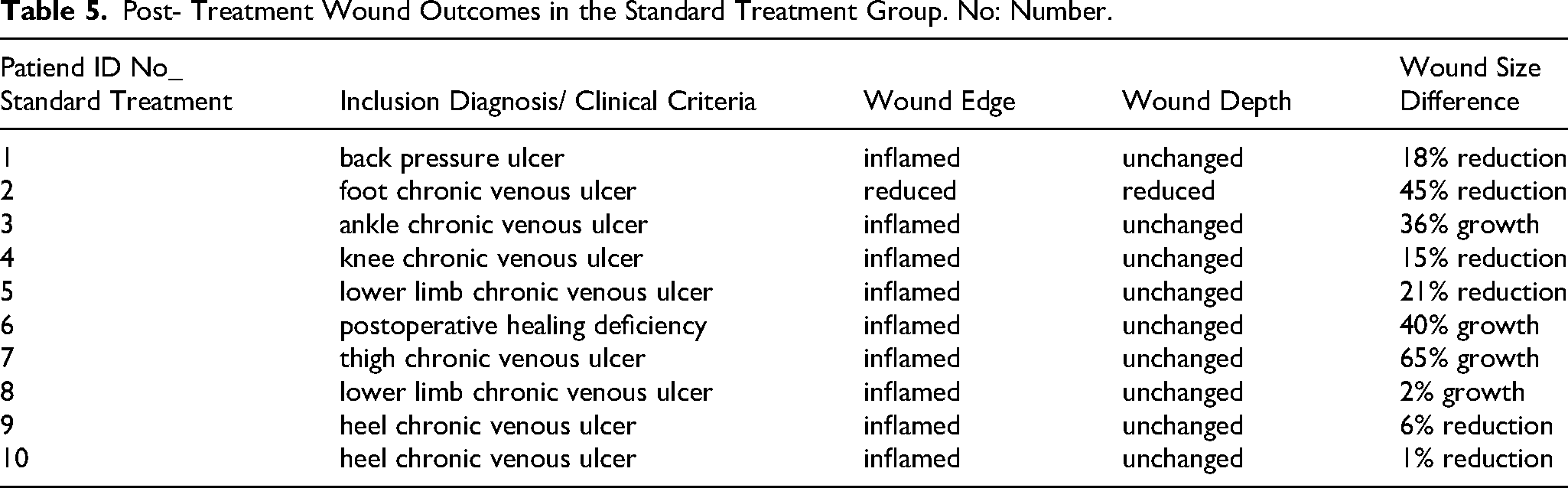
Photo Documentation
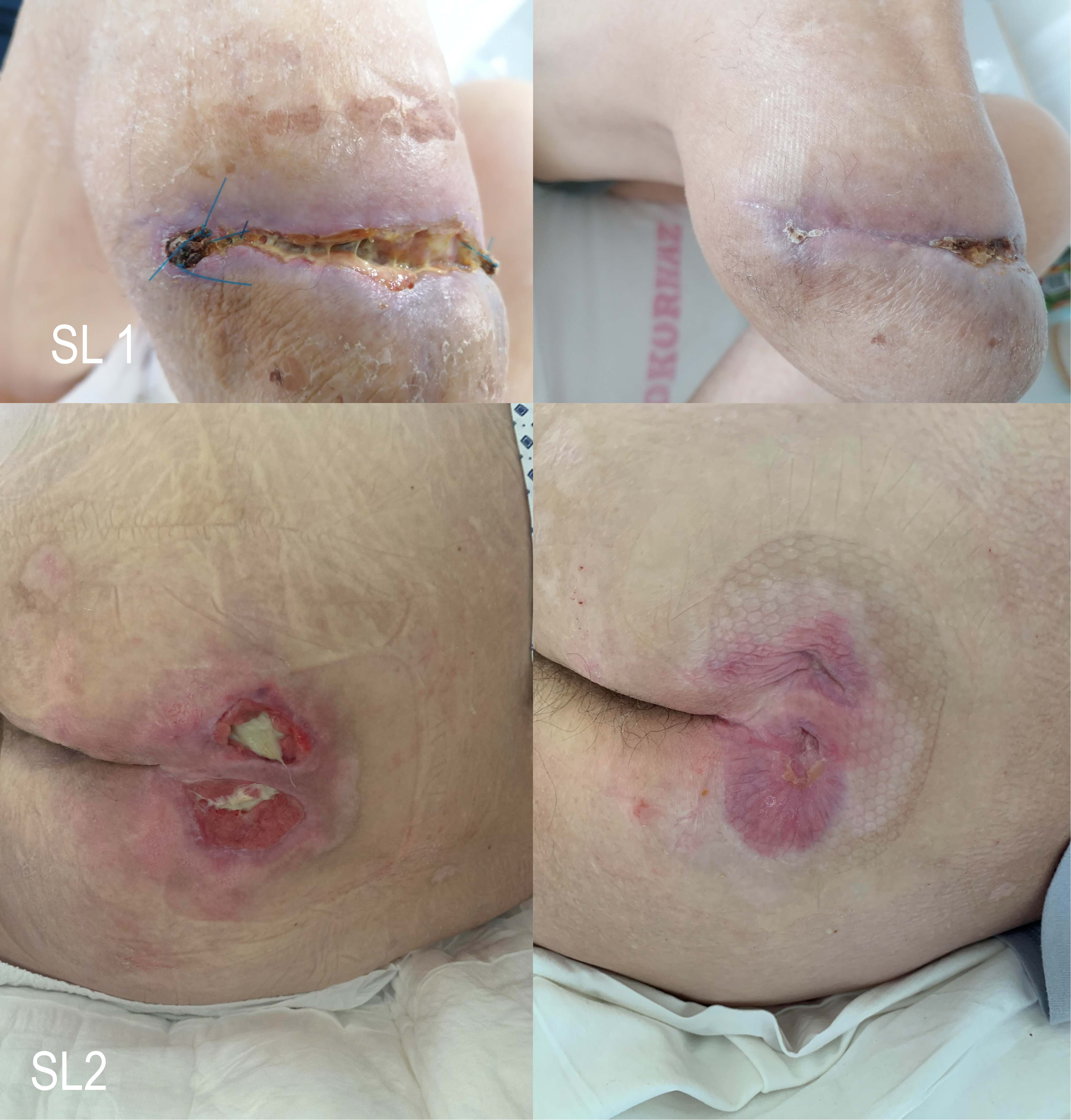
Images below show wound status before (on the left) and after (on the right) the treatment period in the standard treatment group, with patient ID No_ shown in each row (Figures 1 to 5).

Before (left) after (right) status for patients 1–2 in the standard treatment group.

Before (left) after (right) status for patients 3–4 in the standard treatment group.

Before (left) after (right) status for patients 5–6 in the standard treatment group.

Before (left) after (right) status for patients 7–8 in the standard treatment group.

Before (left) after (right) status for patients 9–10 in the standard treatment group.
Images below show wound status before (on the left) and after (on the right) the treatment period in the Safe Laser group, with patient ID No_ shown in each row (Figures 6 to 10).
Before (left) after (right) status for patients 1–2 in the safe Laser group.

Before (left) after (right) status for patients 3–4 in the safe Laser group.

Before (left) after (right) status for patients 5–6 in the safe Laser group.

Before (left) after (right) status for patients 7–8 in the safe Laser group.

Before (left) after (right) status for patients 9–10 in the safe Laser group.
Discussion
Treatment of chronic non-healing wounds, diabetic foot ulcers, and amputation wound deficiencies remains a significant challenge in modern medicine, with conventional bandage treatment often showing limited effectiveness. 12 Thus, a numerous adjuvant modalities have been proposed, including low level laser therapy (LLLT). 13 LLLT has consistently superior outcomes compared with transcutaneous electrical nerve stimulation (TENS) or pharmacological interventions. 19
This study demonstrates that LLLT, when used in conjunction with conventional bandage therapy can accelerate wound healing in cases of diabetic foot ulcers, amputation wound healing deficiencies and pressure ulcers. LLLT targets the cellular level of wound healing, by enhancing mitochondrial adenosine triphosphate production, which in turn improves fibroblast, macrophage and lymphocyte activity. These effects collectively contribute to faster collagen synthesis, accelerated granulation tissue formation, improved phagocytosis, improved epithelial cell migration, and vascularization, as well as reduced production of inflammatory mediators.15-17
Diabetic foot ulcers and chronic peripheral vascular insufficiency are among the leading causes of non-traumatic lower limb amputations, alongside malignancies. 20 This underscores the importance of early treatment, and the urge to find effective alternative adjuvant therapies. LLLT has been shown as effective, safe and easily administered option for these cases.12,15,16
In our study, the use of LLLT in addition to conventional bandage therapy resulted in significant reductions in inflammation, wound depth, and wound area, in some cases leading to complete healing. Conventional therapy alone generally resulted in stagnation, and some cases showed worsening of wound status during treatment. No severe adverse effects were reported throughout the study.
The Safe Laser 1800 Infra device proved to be effective in facilitating wound healing in chronic non-healing wounds, resulting in lower inflammation, decreased wound depth and area. This treatment can stimulate and accelerate wound healing without any thermal damage, discomfort or any major complications. Additionally, it also reduces the healthcare costs by shortening hospitalization.
Our study was limited by the heterogeneity of wounds and patient characteristics included, which precluded the establishment of a uniform and proper control group for each wound type Another limitation was the relatively short follow-up period imposed by the COVID-19 pandemic.
Limitations
This study has several limitations that should be acknowledged. First, the small sample size limits the statistical power of the analysis and reduces the generalizability of the findings. Second, the study population was heterogeneous with respect to wound etiology, size, and patient comorbidities, which may have introduced variability in treatment response and makes it difficult to draw definitive conclusions for specific subgroups.
Despite these limitations, the consistently favorable trends observed—particularly in the reduction of wound dimensions and inflammation—suggest a potential therapeutic benefit of the intervention across a diverse patient population. These promising results support the need for larger, more homogeneous, and controlled studies to confirm efficacy and further define optimal patient selection.
Conclusions
LLLT significantly improves wound healing outcomes in chronic non-healing conditions such as diabetic foot ulcers, amputation wounds and pressure ulcers, when applied alongside with conventional bandage treatment. The photobiomodulatory effects of LLLT promote cellular regeneration, angiogenesis, pain relief and faster granulation tissue formation, resulting in faster and more complete wound closure. As a non-invasive, cost-effective and clinically beneficial adjunct, LLLT represents a valuable addition to the management of complex chronic wounds.
Footnotes
Aknowledgments
We would like to express our sincere gratitude to Brigitta Szilágyi for her expert statistical support throughout this work.
Ethical Approval
Ethical approval was granted by the Hungarian National Institute of Pharmacy and Nutrition (OGYÉI) under reference number: OGYÉI/8363/2020.
Consent to Participate
Written informed consent was obtained prior to inclusion in this research.
Consent for Publication
Written informed consent was obtained prior to inclusion in this research together with the consent to participate.
Author Contributions
SzT: Writing – original draft, Writing – review & editing, Investigation.
HGy: Writing – review & editing, Conceptualization, Data curation, Methodology, Validation, Resources, Supervision.
MK: Writing – review & editing.
MA: Writing – review & editing, Conceptualization
MSz: Writing – review & editing, Supervision, Validation.
All authors certify that their participation is deemed sufficient in the work to take public responsibility for the content, including participation in the concept, design, data analysis, writing, or revision of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data supporting the findings of this study are included in the article and its Supplemental materials.