
Abstract
Background
Clinical guidelines conventionally define nutritional adequacy using a 35 g/L serum albumin threshold. However, its biological sufficiency for driving diabetic foot ulcer (DFU) regeneration remains unvalidated. This investigation utilized a structural modeling framework to interrogate the non-linear relationship between albumin and DFU repair and to identify the precise physiological threshold required for active healing.
Methods
This prospective, dual-center cohort study of 733 DFU patients utilized a 20-week observation window anchored to baseline enrollment (Time Zero, T0). To isolate the independent metabolic effect of albumin from systemic inflammatory confounding, we implemented a doubly robust framework integrating generalized propensity score (GPS) weighting with restricted cubic spline (RCS) modeling. The primary endpoint was Percentage Area Reduction (PAR) at 20 weeks.
Results
Baseline albumin was identified as a significant independent driver of wound reduction (β = 3.25; 95% CI: 0.76-5.73; P = 0.01) and a protective factor against major amputation (OR = 0.89; 95% CI: 0.79-0.99; P = 0.037). RCS analysis revealed a highly significant non-linear trajectory (P for non-linearity < 0.001) with a biological inflection point at 37.9 g/L. No significant regenerative progress occurred within the 31.4–37.9 g/L stagnation plateau. Sensitivity analysis confirmed the conventional 35 g/L cutoff failed to differentiate healing outcomes (P = 0.869), resulting in 45.8% of normoalbuminemic patients being misclassified within a state of regenerative arrest. The calculated E-value of 3.40 confirms profound robustness against unmeasured confounding.
Conclusions
The conventional 35 g/L albumin threshold is clinically inadequate to sustain the metabolic demands of DFU repair. To breach the identified stagnation plateau and transition the wound bed toward active regeneration, clinicians should prioritize a new physiological target of 37.9 g/L (clinically operationalized as ≥ 38 g/L). This necessitates a strategic shift toward metabolic intensification in limb salvage protocols.
Keywords
Introduction
Diabetic foot ulceration (DFU) represents a severe clinical manifestation of systemic metabolic dysregulation, acting as the primary precipitating factor for approximately 84% of non-traumatic lower-extremity amputations. 1 Despite multidisciplinary interventions, the five-year mortality rate following a DFU diagnosis exceeds 45%, a survival profile comparable to several aggressive neoplastic diseases. 2 Transitioning from a state of chronic inflammation to active extracellular matrix deposition necessitates massive physiological reservoirs, with circulating serum albumin acting as an indispensable, rate-limiting metabolic substrate for this energy-intensive repair cascade. 3
Serum albumin is the primary determinant of plasma colloid osmotic pressure (COP) and a critical regulator of transcapillary fluid dynamics according to Starling forces. 4 While clinical guidelines conventionally utilize a universal threshold of 35.00 g/L to define nutritional adequacy, this historical benchmark was primarily calibrated for perioperative mortality risk in general surgery rather than the specific regenerative demands of neuroischemic tissue. 5 A critical knowledge gap remains regarding whether this 35.00 g/L threshold is biologically sufficient to resolve the severe interstitial edema and hypoxia typical of recalcitrant Wagner grade 2 or 3 lesions, or if it inadvertently traps patients in a state of regenerative arrest. 6
Existing literature evaluating albumin in DFU management suffers from substantial methodological limitations. Most investigations rely on traditional associative models that assume a constant linear effect across all concentrations, thereby obscuring the staged, multi-phasic nature of biological tissue repair. 7 Furthermore, as a classic negative acute-phase reactant, albumin synthesis is deeply modulated by the systemic inflammatory burden, making it difficult for standard regression models to isolate its independent structural contribution from overall disease severity. 8 These analytical deficits often lead to information loss and reduced statistical power, preventing the identification of precise physiological targets.
To address these deficits, this prospective, dual-center cohort study implemented a doubly robust structural modeling framework within a prospectively recruited, a priori powered cohort of 733 patients. By rigidly anchoring the study baseline to Time Zero (T0) and integrating generalized propensity score weighting with restricted cubic spline modeling, we sought to isolate the independent effect of serum albumin from systemic inflammatory confounding. 9 This investigation aimed to move beyond arbitrary clinical dichotomization and empirically identify the precise biological inflection point required to switch the DFU microenvironment from metabolic stagnation to active limb repair. 10
Methods
Study Design and Population
Structural Framework
This prospective, dual-center cohort study utilizes a structural modeling framework to evaluate the impact of baseline serum albumin on tissue regeneration. Traditional associative estimates often fail to isolate independent structural contributions from systemic inflammatory interference. To address this, our framework isolates the independent metabolic influence of albumin from measured confounders. We anchored the study baseline to Time Zero (T0), defined as the date of formal clinical enrollment and biochemical sampling. 11 This temporal synchronization ensures strictly unidirectional tracking. It eliminates immortal time bias and mitigates reverse causality during the 20-week healing trajectory. 12
Clinical Setting and Recruitment
Participants were prospectively recruited between October 2024 and October 2025 from two independent medical centers: the University Malaya Medical Centre (UMMC) and the University Malaya Specialist Centre (UMSC). Recruitment spanned three specialized disciplines including Foot and Ankle Orthopaedic Surgery, Trauma Surgery, and the Diabetic Care Unit to capture a representative spectrum of diabetic foot pathology. The protocol adhered to the Declaration of Helsinki and STROBE guidelines. 13 Ethical oversight was provided by the Medical Research Ethics Committee (MREC) of Universiti Malaya, which granted site-specific approvals for UMMC (Ref: 20241023-14342) and UMSC (Ref: 2025113-14583). All participants provided written informed consent before enrollment.
Eligibility Criteria
Clinical Protocol and Outcome Measures
Standard of Care and Clinical Protocol
All participants were managed under a standardized multidisciplinary team (MDT) framework in strict accordance with the 2023 IWGDF guidelines. 6 This MDT integrated specialized expertise from orthopaedic surgeons, podiatrists, and wound care nurses across both clinical sites. Procedural consistency between UMMC and UMSC was structurally assured by their shared institutional governance: both centers operate under the Department of Orthopaedic Surgery, Faculty of Medicine, University of Malaya, with the majority of treating clinicians holding concurrent appointments at both sites. Clinical data collection and protocol oversight across both centers were coordinated by the Tissue Engineering Group (TEG), a dedicated research unit embedded within the same department, ensuring that wound assessment, debridement, offloading prescription, and infection management were executed under a unified operational framework throughout the enrollment period.
Procedural equivalence was further reinforced through a joint standardized training program completed by all clinical and research personnel prior to the commencement of recruitment. This program aligned wound assessment protocols, debridement techniques, offloading prescription criteria, and infection management pathways uniformly across both sites. Periodic cross-site protocol review meetings were conducted throughout the enrollment period to identify and rectify any operational drift.
Therapeutic interventions prioritized regular sharp debridement, aggressive infection control, and standardized pressure offloading. In accordance with IWGDF 2023 recommendations, total contact casting (TCC) was designated as the primary offloading modality and was employed in 300 patients (40.9%). TCC devices were inspected and replaced at each scheduled clinic visit, typically at two-week intervals, to maintain casting integrity and monitor for skin complications. Non-removable orthotic devices were utilized in 280 patients (38.2%) as an equivalent fixed offloading alternative where TCC application was technically challenging or patient-specific anatomical factors precluded standard casting. In the remaining 153 patients (20.9%), alternative offloading modalities were implemented where both TCC and non-removable orthotics were contraindicated, including cases with active deep infection requiring frequent wound access, compromised peripheral vascular status, or wound morphology incompatible with circumferential casting. Systemic corticosteroid administration was prohibited throughout the 20-week observation period to eliminate pharmacological interference with the biological regenerative trajectory. These measures collectively ensure that observed variations in healing outcomes are attributable to differences in baseline metabolic status rather than discrepancies in clinical management between sites.
Exposure Assessment
The primary exposure was fasting serum albumin measured at T0 via the bromocresol green (BCG) assay. Unlike traditional studies utilizing arbitrary clinical cutoffs, we analyzed albumin as a continuous variable to preserve biological granularity. This strategy facilitates the data-driven identification of physiological thresholds through restricted cubic splines (RCS), effectively avoiding the information loss and reduced statistical power inherent in binary classification. 15 Evaluating albumin as a continuous structural driver allows for precise identification of the concentration required to trigger extracellular matrix deposition.
Outcome Measures and Adjudication
The index ulcer was defined as the lesion with the largest surface area or the highest Wagner grade at enrollment. To ensure objective quantification, two independent assessors blinded to baseline albumin levels performed ulcer planimetry by manually tracing the wound perimeter on standardized digital images. Any measurement discrepancies exceeding 10% were formally adjudicated by a senior consultant orthopaedic surgeon from the Foot and Ankle Unit to maintain maximal procedural consistency.

For participants who did not reach the 20-week milestone, Area 20w was defined as the last recorded ulcer area before termination. Clinical failures, including major amputation, unplanned surgical revascularization, or mortality, were adjudicated as treatment failures and assigned a PAR of −100%. To stabilize the impact of extreme outliers, PAR values were Winsorized to a restricted range of −100% to 100%. 16
Data Integrity and Attrition Control
To mitigate potential attrition bias from non-medical loss to follow-up, Inverse Probability of Censoring Weighting (IPCW) was implemented within the structural models. This weighting procedure protects the validity of causal estimates against informative censoring caused by longitudinal participant dropout.
Statistical Analysis Strategy
Descriptive Statistics and Distribution
All computations were performed using R version 4.3.2. Continuous variables were evaluated for normality using the Shapiro-Wilk test. Normally distributed data are reported as mean ± standard deviation, while non-normal variables are presented as median with interquartile range (IQR). Categorical data are summarized by frequencies and percentages. Baseline inter-group comparisons utilized Student's t-tests, Wilcoxon rank-sum tests, chi-square tests, or Fisher's exact tests depending on data distribution. All statistical tests were two-tailed with a significance threshold of α = 0.05.
Covariate Selection and Causal Architecture
Baseline covariates were selected based on clinical relevance and structural modeling principles to prevent collider bias or over-adjustment. The adjustment set was restricted to variables measured at T₀ to maintain a strictly pre-exposure baseline. Log-transformation stabilized numerical variance in skewed parameters. The final structural model incorporated four confounding domains: (1) demographics including age, sex, body mass index, and smoking history; (2) systemic and metabolic burden comprising ankle-brachial index, diabetes duration, glycated hemoglobin, and estimated glomerular filtration rate; (3) inflammation and oxygenation consisting of C-reactive protein and anemia status, included to mitigate the confounding effects of the acute-phase inflammatory response on albumin synthesis ; and (4) wound characteristics including ulcer duration, Wagner grade, and baseline area.
Structural Weighting
To isolate the exposure effect from baseline confounding and selection bias, we implemented a composite weighting framework. For the continuous exposure of serum albumin, stabilized inverse probability of treatment weights (sIPTW) were estimated via a normal density function using the generalized propensity score (GPS) method. 17 Simultaneously, stabilized inverse probability of censoring weights (IPCW) were generated to adjust for informative dropout. A composite weight was calculated as the product of sIPTW and IPCW. To ensure estimate stability against extreme probability values, these weights were truncated at the fifth and 95th percentiles after verifying the common support domain. Covariate balance was assessed using absolute treatment-covariate correlations, where a threshold below 0.1 indicated optimal structural balance, and visualized via Love plots. 18
Sample Size and Power
Sample size was determined a priori for the primary outcome of Percentage Area Reduction at 20 weeks, evaluated within a doubly robust weighted linear regression framework. The effect size estimate was anchored to the observed distribution of baseline serum albumin in the recruitment population (median 35.10 g/L; IQR: 31.20-38.40) and corroborated against published albumin-healing associations in comparable diabetic foot ulcer cohorts. A per-unit albumin effect on PAR of approximately 3.0 to 3.5 percentage points per g/L increment was projected, with a pooled residual standard deviation of approximately 27%. At a two-tailed significance threshold of α = 0.05 with 90% power (β = 0.10), a minimum of 680 evaluable participants was required to detect this structural effect within the full multivariable adjustment set.
Longitudinal attrition over a 20-week observation window was anticipated at approximately 7%, consistent with published dropout rates in prospective diabetic foot ulcer trials. Enrollment was therefore targeted at 733 participants to preserve analytic adequacy after expected losses. The final cohort of 733 participants satisfies the a priori power requirement, providing greater than 90% power to interrogate the non-linear dose-response relationship between baseline albumin and the 20-week regenerative trajectory.
Outcome Modeling and Quality Assurance
Outcome Modeling and Doubly Robust Estimation
Within the weighted framework, a doubly robust estimation strategy was employed to provide a secondary layer of protection against residual confounding and potential model misspecification. 9 For the primary outcome, weighted linear regression evaluated the association between albumin and PAR. Restricted cubic splines (RCS) with four knots interrogated non-linear dose-response dynamics, with Wald tests assessing the significance of non-linear terms. This methodology identified physiological inflections and clinical targets based on spline curvature. Weighted logistic regression examined the relationship between albumin levels and ipsilateral major amputation. All models utilized robust sandwich estimators to provide conservative variance and standard error correction. Effect sizes are reported as regression coefficients (β) or odds ratios (OR) with corresponding 95% confidence intervals (CI).
Sensitivity Analyses and Bias Quantification
Pre-specified sensitivity analyses evaluated core structural assumptions and estimate robustness. Following the identification of physiological inflection points, the continuous albumin variable was converted into a binary indicator to compare optimized metabolic status against standard hypoalbuminemia. We re-evaluated the effect on healing using stabilized IPTW to verify the validity of these clinical targets. To quantify the potential impact of unmeasured confounding, E-values were calculated for the primary outcome. 19 This metric defines the minimum strength an unmeasured factor would require to nullify the observed structural association between albumin and tissue regeneration.
Procedural Integrity
To maintain internal validity, research personnel completed a standardized training program to synchronize operational protocols before recruitment. Data integrity was supported by a dual-entry architecture and periodic logical audits to rectify clerical inconsistencies. As detailed in the adjudication protocols, ulcer quantification relied on independent double-assessments and masked expert review to minimize detection bias. These systemic safeguards were implemented to reduce operational variability, allowing the derived estimates to more closely represent underlying biological signals. Statistical analyses were conducted by personnel independent of clinical data collection. All analytical decisions, including covariate selection, knot placement for restricted cubic splines, and weight truncation thresholds, were prespecified and documented prior to outcome unblinding, precluding post-hoc modification of the analytic strategy.
Results
Baseline Demographic and Clinical Characteristics
The final cohort comprised 733 patients (Table 1). The median age was 62.00 years (IQR: 52.00-71.00), with a 41.5% (n = 304) female representation. The median BMI was 25.50 kg/m2 (IQR: 22.00-27.80), and active smokers accounted for 52.1% (n = 382) of the population. Participants presented with a median diabetes duration of 15.12 years (IQR: 9.14-20.12) and a median HbA1c of 8.20% (IQR: 7.80-9.10).
Baseline Demographic, Clinical, and Biochemical Characteristics of the Study Cohort with Diabetic Foot Ulcers.
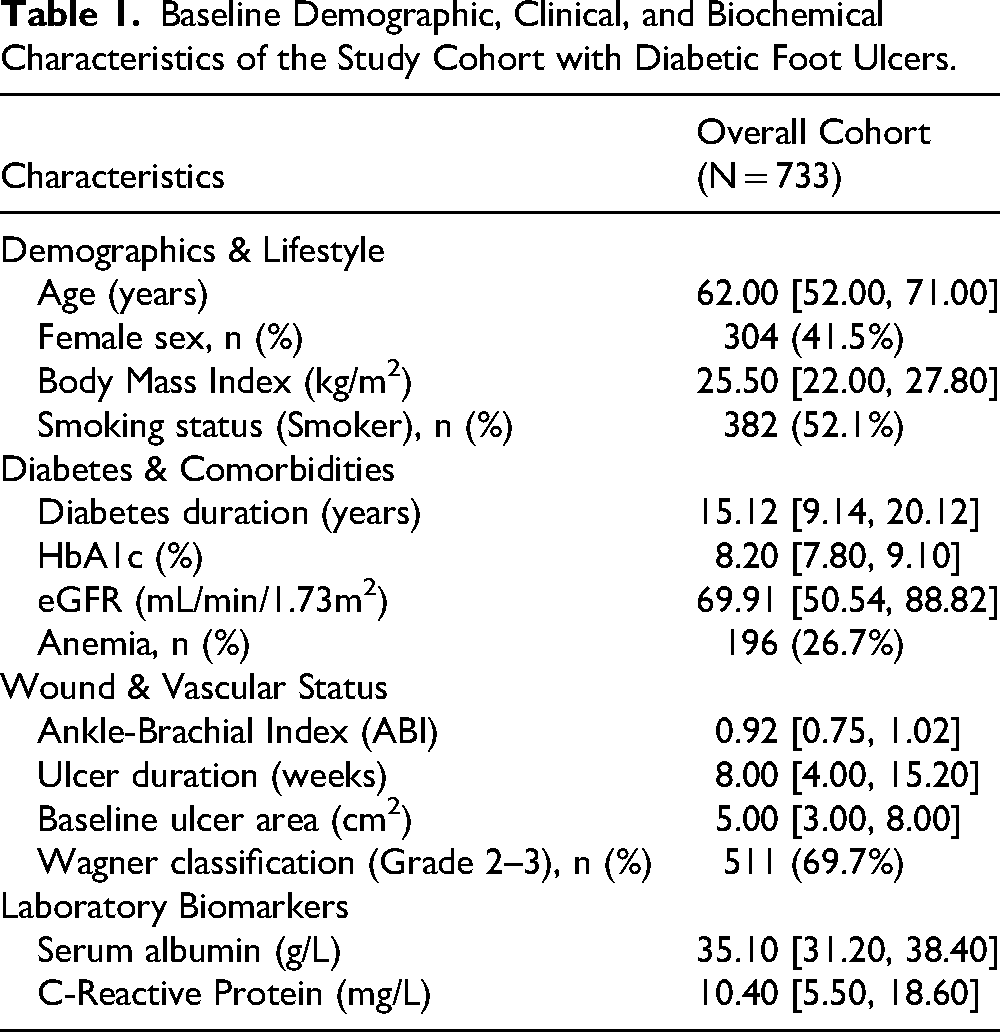
Baseline laboratory parameters demonstrated a median eGFR of 69.91 mL/min/1.73 m2 (IQR: 50.54-88.82), a 26.7% (n = 196) prevalence of anemia, a median serum albumin of 35.10 g/L (IQR: 31.20-38.40), and a median CRP of 10.40 mg/L (IQR: 5.50-18.60). At enrollment, 69.7% (n = 511) of the index ulcers were classified as Wagner grade 2 or 3, with a median surface area of 5.00 cm2 (IQR: 3.00-8.00).
Weighting Performance and Covariate Balance
Baseline albumin correlated with multiple clinical covariates in the unadjusted cohort. The application of the composite GPS weighting framework significantly enhanced global covariate balance (Figure 1). While most absolute treatment-covariate correlations were reduced below the pre-specified 0.1 threshold, minor residual imbalances persisted for age, eGFR, and ABI. Consequently, the primary analyses utilized doubly robust models to formally adjust for these specific variables within the weighted framework, thereby isolating the structural effect of albumin from baseline physiological disparities.
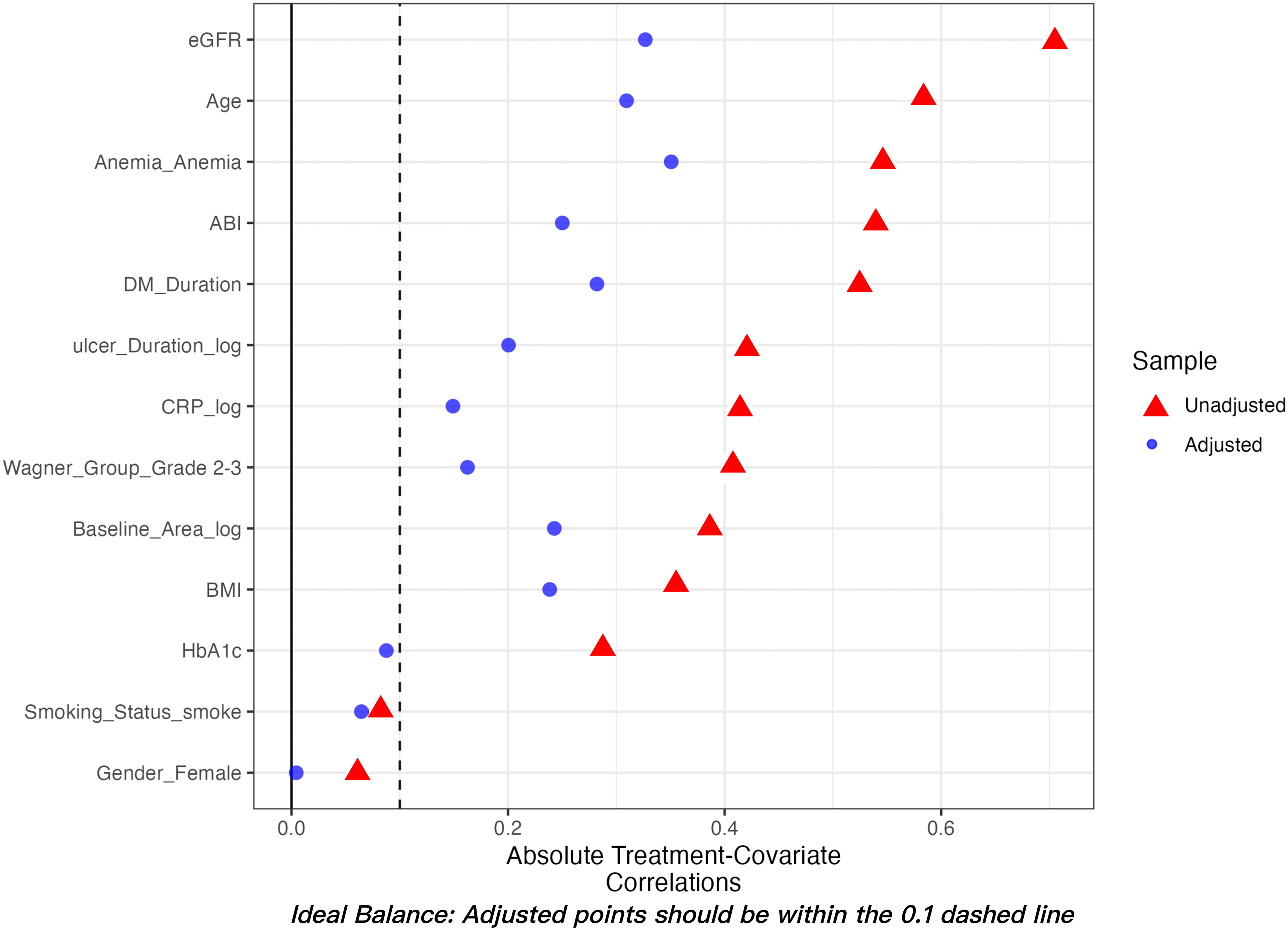
Love plot displaying the absolute treatment-covariate correlations before and after generalized propensity score (GPS) weighting. The Love plot illustrates the absolute treatment-covariate correlations to assess the structural adequacy of the balancing procedure. Solid triangles depict significant baseline imbalances across the raw cohort, particularly for renal function (eGFR), chronological age, and anemia status. Solid circles represent the correlations following the application of the composite GPS-weighting framework. While the weighting procedure substantially neutralized confounding for most variables (shifting them to the left of the 0.1 threshold), minor residual imbalances remained for eGFR, age, and ankle-brachial index (ABI). These specific residual heterogeneities were subsequently addressed by implementing a doubly robust adjustment in the final causal models, ensuring the internal validity of the effect estimates.
Albumin-Healing Association
The structural association between baseline albumin and 20-week PAR was evaluated across three hierarchical models (Table 2) to progressively isolate the independent biological effect:
Causal Association Between Baseline serum Albumin and 20-Week Percentage Area Reduction (PAR) in Diabetic Foot Ulcers.

Amputation Risk Analysis
The structural association between baseline albumin and the risk of major amputation was evaluated across the hierarchical framework (Table 3). In the unadjusted Model 1, higher baseline albumin was significantly associated with a reduced risk of limb loss (OR = 0.81; 95% CI: 0.77 to 0.85; P < 0.001). This protective effect remained robust in the weighted Model 2 (OR = 0.85; 95% CI: 0.79 to 0.91; P < 0.001) following composite weighting for confounding and informative censoring. The final doubly robust Model 3 confirmed a significant inverse association, where each 1.00 g/L increment in baseline albumin corresponded to an 11% relative reduction in the risk of major amputation (OR = 0.89; 95% CI: 0.79 to 0.99; P = 0.037).
Causal Association Between Baseline serum Albumin and 20-Week Risk of major Amputation in Diabetic Foot Ulcers.

Non-Linear Threshold Dynamics
Restricted cubic spline (RCS) modeling identified a highly significant non-linear relationship between baseline albumin and 20-week PAR (P for non-linearity < 0.001; Figure 2). Based on the biological response trajectory, the regenerative continuum was delineated into three distinct functional domains:
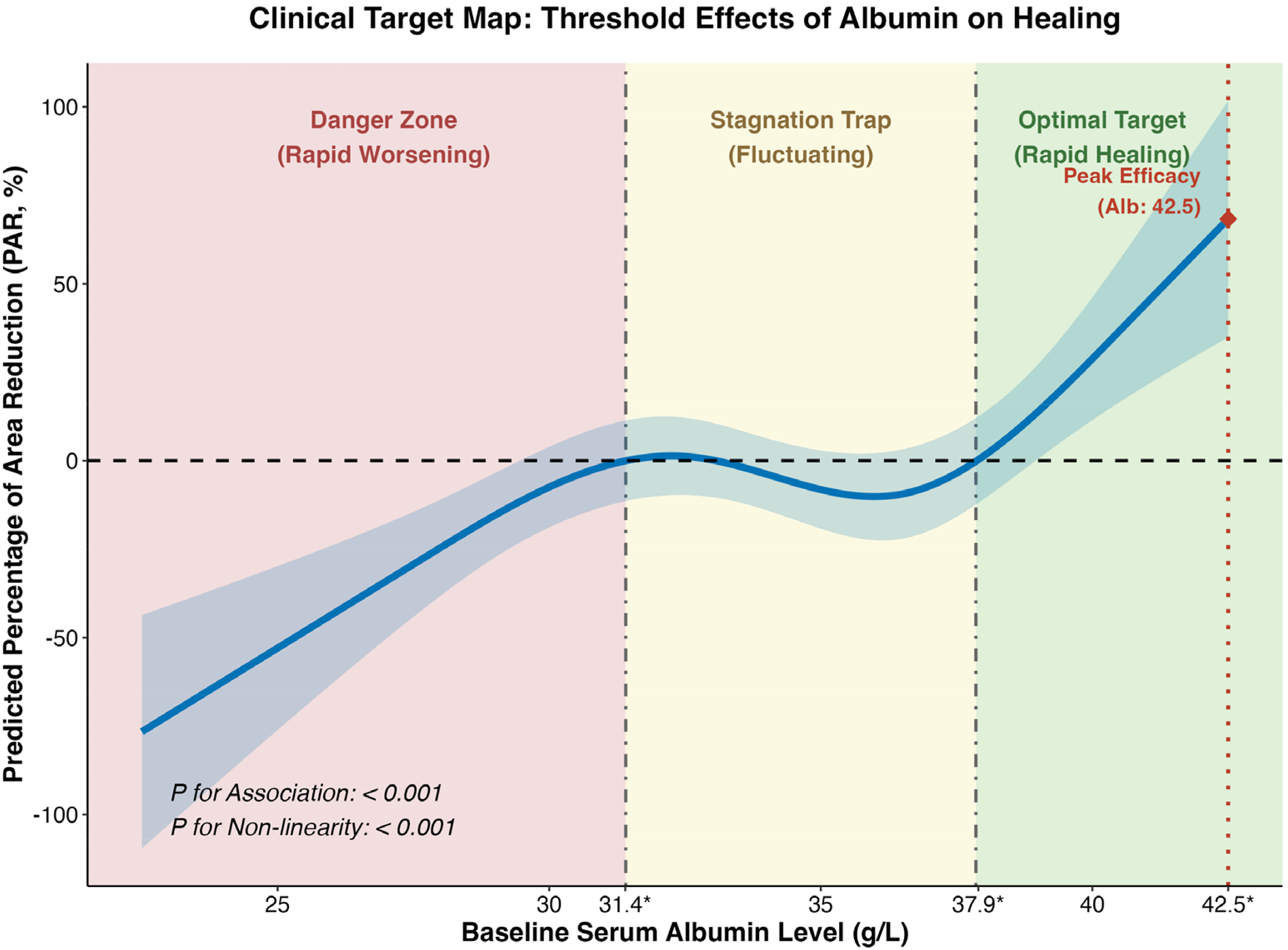
Non-linear dose-response relationship between baseline serum albumin and predicted 20-week wound healing percentage area reduction (PAR). Restricted cubic spline (RCS) analysis characterizing the multi-phasic impact of systemic albumin reserves on the predicted tissue regeneration trajectory. The solid blue line denotes the predicted causal response, while the shaded region represents the 95% confidence interval. The biological response is categorized into three distinct functional domains defined by the model's inflection points: (1) a “Danger Zone” (Deterioration Range, <31.4 g/L) where rapid wound expansion is predicted; (2) a “Stagnation Trap” (Stagnation Plateau, 31.4-37.9 g/L) characterized by metabolic arrest and fluctuating regenerative progress; and (3) an “Optimal Target” (Accelerated Healing Range, >37.9 g/L) where tissue repair accelerates exponentially toward peak efficacy at 42.5 g/L. The highly significant P for non-linearity (P < 0.001) demonstrates that baseline albumin functions as a non-linear driver of chronic wound closure.
Sensitivity Analysis
Sensitivity analyses validated the structural robustness of the primary estimates and the clinical utility of historical benchmarks. Applying the conventional 35.00 g/L clinical threshold failed to demonstrate significant discrimination in healing outcomes (β = -1.24; 95% CI: −16.00 to 13.52; P = 0.869). This lack of statistical significance strictly aligns with the observed stagnation plateau, confirming that the 35.00 g/L benchmark is insufficient to catalyze active wound reduction. Furthermore, the calculated E-value for the primary structural effect was 3.40, indicating the substantial strength an unmeasured confounder would require to entirely nullify the observed association between albumin and tissue regeneration.
Metabolic Risk Distribution
Applying the identified structural thresholds to the study population revealed the clinical magnitude of metabolic inadequacy. At baseline, only 27.1% (n = 199) of patients achieved the Accelerated Healing Range (> 37.90 g/L). In contrast, 49.8% (n = 365) of the cohort was situated within the Stagnation Plateau (31.40-37.90 g/L), and 23.1% (n = 169) fell within the Deterioration Range (< 31.40 g/L).
Crucially, applying the new structural threshold reveals a substantial clinical misalignment: among patients conventionally classified as normoalbuminemic (≥ 35.00 g/L), approximately 45.8% (n = 168) were situated within the stagnation plateau, possessing insufficient systemic reserves to bypass the state of therapeutic arrest. This identifies a critical false-negative rate in current nutritional benchmarks, where nearly half of the patients deemed clinically adequate are, in fact, trapped in a state of regenerative stagnation (Figure 2).
Discussion
By implementing a doubly robust structural framework across a cohort of 733 patients, this study isolates baseline serum albumin as an independent driver of diabetic tissue regeneration rather than a passive correlate of metabolic decline. Traditional linear models presume a constant effect across all biomarker concentrations, which can obscure the multi-phasic nature of biological repair. In contrast, restricted cubic spline modeling reveals a segmented trajectory characterized by a physiological inflection point at 37.90 g/L. The predicted percentage area reduction exhibits exponential acceleration above this threshold, whereas levels below this point correspond to wound expansion or therapeutic stagnation. Identifying this stagnation plateau between 31.40 and 37.90 g/L redefines the biological boundaries of therapeutic success in diabetic foot ulcer management. Albumin levels within this range may sustain basal systemic maintenance but appear fundamentally inadequate to trigger the substantial extracellular matrix remodeling required for chronic wound closure. 20
Pinpointing 37.90 g/L as a physiological requirement provides a mechanistic rationale for the observed limitations of conventional nutritional targets. Our pre-specified sensitivity analyses demonstrated that the traditional 35.00 g/L clinical cutoff failed to differentiate healing outcomes (β = −1.24; 95% CI: −16.00 to 13.52; P = 0.869). This lack of statistical discrimination exposes a critical false floor in current clinical practice, where historical guidelines utilize 35.00 g/L as a generic indicator of malnutrition or perioperative risk. 21 The clinical misalignment identified in this cohort is substantial: among patients conventionally classified as normoalbuminemic (≥ 35.00 g/L), approximately 45.8% (n = 168) were situated within the stagnation plateau, possessing insufficient systemic reserves to bypass the state of therapeutic arrest. Consequently, clinicians targeting this conventional threshold may inadvertently prolong regenerative arrest, as the provided metabolic support prevents rapid systemic deterioration but fails to generate the surplus protein reserves required to transition into the proliferative phase of repair. 22 Collectively, our metabolic risk distribution indicates that 72.9% of the presenting population possessed systemic reserves within the stagnation or deterioration range, highlighting a substantial gap in current clinical intensification efforts.
The acceleration of healing observed once albumin exceeds 37.90 g/L likely represents a transition in microenvironmental hydrodynamics alongside its biochemical role. Albumin acts as the primary determinant of plasma colloid osmotic pressure (COP), regulating capillary transmural fluid balance governed by the Starling equation. 23 In the gravitationally dependent diabetic foot, local hydrostatic pressure and inflammatory permeability are elevated. Albumin concentrations below the 37.90 g/L threshold provide insufficient oncotic drive to counteract this outward pressure, leading to net ultrafiltration and interstitial edema. 24 This edema expands the physical distance between the capillary endothelium and basal keratinocytes, potentially degrading oxygen delivery according to Fick's law of diffusion. 25 Crossing the 37.90 g/L threshold represents an oncotic equilibrium necessary to reverse fluid extravasation, actively draining the edematous interstitium and restoring effective capillary perfusion. Beyond this hydrodynamic mechanism, albumin serves as a primary carrier for essential wound-healing cofactors, including zinc and systemic growth factors. 26 Furthermore, its abundant sulfhydryl groups, particularly the Cys34 residue, function as a massive systemic sink for reactive oxygen species (ROS). 27 In the highly oxidative microenvironment of a diabetic wound, this antioxidant capacity prevents the premature proteolytic degradation of newly synthesized extracellular matrix proteins and protects proliferating fibroblasts from oxidative stress-induced apoptosis, thereby firmly reactivating the dormant regenerative cascade. 28 Peak efficacy observed at 42.50 g/L likely represents the optimal biological saturation of these dual physical and biochemical repair pathways.
Managing patients with advanced diabetic nephropathy or decompensated cirrhosis presents a complex clinical challenge, as endogenous albumin synthesis often cannot be elevated to the 37.90 g/L target. 29 These scenarios underscore the utility of microenvironmental compensation strategies within a multidisciplinary team (MDT) framework. When the endogenous COP drive is deficient, biophysical interventions such as negative pressure wound therapy (NPWT) or compression systems can mechanically extract interstitial fluid to emulate the drainage effects of optimal oncotic pressure. 30 Additionally, because albumin is a negative acute-phase reactant, systemic inflammation suppresses its synthesis. 8 The elevated CRP levels observed in our cohort (median 10.40 mg/L) reflect this catabolic stress, indicating that targeted infection control and anti-inflammatory management are necessary to prevent further depletion of metabolic reserve. 31
The protective effect of optimal albumin extends beyond wound closure to the prevention of major amputation. Doubly robust adjustment demonstrated that each 1.00 g/L increment in baseline albumin was associated with an 11% relative reduction in the risk of limb loss (OR = 0.89; 95% CI: 0.79 to 0.99; P = 0.037). The calculated E-value of 3.40 solidifies the causal stability of this finding, indicating that an unmeasured confounder would require a strong magnitude of association with both the exposure and outcome to nullify the observed protective effect. 19 Achieving a threshold above 37.90 g/L appears critical to transition the microenvironment toward active limb repair. Future research should transition from observational designs to prospective interventional trials. 32 Studies comparing targeted medical nutrition, aiming for ≥ 38.00 g/L, against standard 35.00 g/L care are needed to validate this elevated metabolic target for limb salvage. 33 Given that elevating serum albumin alters plasma oncotic pressure and may redistribute intravascular fluid volume, interventional trials should incorporate prospective cardiovascular safety monitoring, particularly in patients with pre-existing cardiac dysfunction or chronic kidney disease, in whom fluid overload risk is substantially elevated. Relevant monitoring parameters should include serial fluid balance assessment, plasma B-type natriuretic peptide or N-terminal pro-BNP, and echocardiographic evaluation where clinically indicated. These safety endpoints will establish the physiological boundaries within which metabolic intensification can be pursued without incurring cardiopulmonary risk.
Strengths and Limitations
This study leverages a large, prospective 733-patient cohort and implements a doubly robust causal framework to isolate the independent metabolic contribution of serum albumin to tissue regeneration. By utilizing restricted cubic spline modeling to evaluate albumin as a continuous variable, this approach mitigates the structural information loss inherent in arbitrary clinical dichotomization, thereby identifying a data-driven 37.90 g/L physiological inflection point. 34 Furthermore, the calculated E-value of 3.40 demonstrates substantial causal stability, indicating that the observed associations are resilient to unmeasured confounding from factors such as undocumented dietary variations or genetic predispositions. Despite these methodological strengths, the observational design cannot entirely eliminate residual bias. Additionally, although the reliance on strictly anchored baseline measurements is essential for preventing immortal time bias, this approach limits the assessment of temporal albumin fluctuations and the cumulative impact of interval nutritional interventions during the 20-week trajectory. 12 Finally, recruitment was concentrated within metropolitan tertiary centers across Kuala Lumpur, Selangor, and Negeri Sembilan. While capturing a representative Southeast Asian demographic, this geographical homogeneity may restrict broader extrapolation. 35 Consequently, external validation across diverse global healthcare infrastructures and ethnic populations remains necessary to confirm the clinical utility of the 37.90 g/L threshold prior to international guideline integration.
Conclusion
This prospective analysis suggests that the conventional 35.00 g/L serum albumin threshold is clinically insufficient to sustain active tissue repair within the hypercatabolic microenvironment of diabetic foot ulcers. Our findings identify 37.90 g/L as a potential biological inflection point, marking a transition from metabolic stagnation toward sustained regenerative progress. These data support the necessity of exploring metabolic intensification in limb salvage protocols. Consequently, achieving a systemic albumin level exceeding 37.90 g/L, clinically operationalized as ≥ 38.00 g/L, should be considered a primary physiological target to optimize microenvironmental hydrodynamics and facilitate chronic wound closure.
For patients with advanced diabetic nephropathy or decompensated hepatic disease, endogenous albumin synthesis frequently cannot be elevated to the 37.90 g/L target through nutritional or pharmacological intervention alone. In these cases, the deficit in endogenous colloid osmotic pressure does not preclude active wound management. Biophysical interventions, including negative pressure wound therapy and graduated compression systems, provide a mechanically mediated alternative by actively extracting interstitial fluid and reducing edema burden, thereby partially compensating for the insufficient oncotic gradient. These modalities should be regarded as necessary adjuncts to metabolic intensification rather than independent substitutes. The clinical framework emerging from these data therefore supports a stratified approach: metabolic intensification targeting ≥ 38.00 g/L for patients with adequate synthetic reserve, and concurrent biophysical compensation for those in whom this threshold remains physiologically unattainable.
Footnotes
Acknowledgements
The authors express their gratitude to the clinicians and support staff of the Department of Orthopaedic Surgery at both the University Malaya Medical Centre and the University Malaya Specialist Centre for their sustained institutional support and essential assistance with participant recruitment throughout this investigation.
Institutional Review Board Statement
The investigation was conducted in strict accordance with the ethical principles of the Declaration of Helsinki. This prospective protocol received independent ethical approval for the University Malaya Medical Centre under MREC Ref: 20241023-14342, and for the University Malaya Specialist Centre under MREC Ref: 2025113-14583.
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Consent to Publish
The authors affirm that human research participants provided informed consent for publication of the data and figures included in this manuscript.
Author Contributions
T.H.Y.Q.: Conceptualization, Methodology, Investigation, Resources, Data curation, and Writing–original draft preparation; A.A.: Investigation, Data curation, and Project administration; X.W.L.: Investigation and Data curation; A.H.: Investigation and Data curation; E.M.Z.: Investigation and Data curation; T.K.: Conceptualization, Methodology, and Supervision; T.H.L.: Conceptualization, Methodology, Supervision, Project administration, and Funding acquisition; A.Y.F.W.: Software, Formal analysis, and Visualization; all authors: Writing–review & editing and final approval of the version to be published.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Universiti Malaya Bantuan Khas Penyelidikan - Early Career Research Grant (BKP-ECRG, Project No. BKP031-2025-ECRG) and the Universiti Malaya Specialist Centre C.A.R.E. Fund Research Grant (UMSC-RG, Project No. UMG004C-2025).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The datasets generated and analyzed during the current study are not publicly available due to institutional data protection policies and patient privacy regulations, but are available from the corresponding author upon reasonable request.
Use of Artificial Intelligence
In the preparation of this manuscript, the authors utilized ChatGPT (OpenAI) solely for grammatical refinement and language polishing. The authors have reviewed the output and assume full responsibility for the entire content.