
Abstract
This trial evaluates whether transcutaneous gaseous carbon dioxide therapy (CO2 therapy) combined with standard of care (SOC) improves healing of hard-to-heal recurrent diabetic foot ulcers (DFUs) compared with SOC alone. A total of 30 participants with recurrent hard-to-heal DFUs were included and randomized 1:1 to an intervention (CO2 therapy plus SOC) or a control group (SOC only). The intervention consisted of 20 daily 50-minute CO2 therapy sessions over 4 weeks. After 4 weeks, 46.7% of ulcers in the intervention group were completely healed, versus 0% in the control group (p = 0.005). The intervention group showed a median area reduction of 85.7% (IQR 54.9–100) compared to 17.2% (IQR 0.88–33.5) in controls (p < 0.001), with significantly better Falanga wound-bed scores (p < 0.001). The intervention group demonstrated a significant relative increase in StO2 (29.6 ± 19.6%), whereas the control group exhibited a decrease (-2.2 ± 6.9%), resulting in a between-group difference of 31.8% (95% CI 20.5%–43.0%; p < 0.001). Pain intensity significantly decreased in the intervention group only (p = 0.002). This trial suggests that CO2 therapy in combination with SOC is superior to SOC alone in healing recurrent, hard-to-heal DFUs.
Introduction
Diabetic foot ulcers (DFUs) cause a substantial burden on public health.1,2 If unmanaged, DFUs represent a life threat for patients with DFU, with a five-year mortality rate up to 30%.3 Even upon complete ulcer healing, the risk of ulcer recurrence is high - approximately 40% within one year and 60% within five years.4
A particularly challenging subset is hard-to-heal DFUs, typically defined by a failure to achieve a 50% area reduction after four weeks of standard of care (SOC). The specific clinical problem of these DFUs is primarily characterized by a persistent, chronic inflammatory state that prevents the normal progression of wound repair.5 This state is attributable to several intrinsic factors, such as biochemical imbalance (between proinflammatory cytokines and their inhibitors, as well as proteases and their antiproteases), failure of matrix synthesis (due to continuous influx of inflammatory cells and sustained production of inflammatory mediators), cellular barriers due to ischemia, infection etc., but also extrinsic factors such as delayed clinical intervention and lack of universal adoption of the guidelines published by the International Working Group on the Diabetic Foot (IWGDF).5 Next, patient-specific factors such as non-adherence to treatment, mental health comorbidities, and socioeconomic barriers further complicate the wound healing.5 Finally, Meloni et al.6 report in their large cohort study that prevalence of purely neuropathic DFUs in patients with diabetes mellitus in Europe is decreasing, becoming less common than ischemic/neuro-ischemic ulcers. This epidemiological shift underscores the importance of addressing tissue hypoxia as one of the key barriers to healing.
Consequently, there is a critical clinical need for a safe, cost-effective, and non-invasive adjunctive therapy capable of clinically addressing the local tissue hypoxia. In this context, prior work7 in the field of DFUs indicates that repeated CO2 therapy can improve cutaneous microvascular function. Collectively, these findings support CO2 therapy as a promising adjunct treatment method for DFUs with the potential to mitigate local hypoxia and improve microcirculatory function, which are essential for sustained ulcer healing. Building on this rationale, our trial extends the evidence base by adding serial hyperspectral imaging (HSI) of superficial tissue oxygenation (StO2) as an objective physiologic response marker, demonstrating a progressive increase in oxygenation across the prespecified weekly trial visits during the 4-week period. The importance of implementing newer treatment technologies in healing hard-to heal DFUs is also recognized by IWGDF.8 Although the need to improve ulcer healing in patients with hard-to-heal DFUs is widely recognized, the overall quality of evidence from studies evaluating new treatments is, unfortunately, poor8.
Transcutaneous application of gaseous carbon dioxide (CO2) (hereinafter CO2 therapy) is a promising adjuvant treatment method for non-invasive management of DFUs due to its accelerated ulcer-healing rate9,10, improved microcirculatory function7, and reduced ulcer recurrence rates10, with no observable systemic or local adverse effects7,9–11.
The primary objective of this trial was to determine if combining CO2 therapy with SOC improves healing rates in patients with hard-to-heal, recurrent DFUs compared to those receiving SOC alone.
Materials and methods
This prospective, open-label, parallel-group, superiority, single-center randomized controlled trial (RCT) with allocation ratio of 1:1 was carried out (including recruitment) at the Department of Vascular Surgery, General hospital Novo mesto (Novo Mesto, Slovenia), between September 2024 and March 2025. The trial was conducted in accordance with the Declaration of Helsinki and approved by the National Medical Ethics Committee of the Republic of Slovenia (Approval ID: 0120- 316/2024-2711-3, date of approval: August 20, 2024). There were no modifications to the study design, pre-specified outcomes, or planned statistical analyses after trial commencement. The trial protocol, statistical analysis plan, de-identified participant data and statistical code are accessible via the corresponding author following a formal proposal. Patients and the public were not involved in the design, conduct or reporting of this trial. The trial reporting adheres to the CONSORT 2025 guidelines for reporting RCTs. Written informed consent was obtained from all participants. The sample size chosen was determined by feasibility considerations.
The primary hypothesis of this trial was: CO2 therapy, combined with SOC, is superior to SOC only in terms of ulcer healing in patients with recurrent, hard-to-heal DFUs (often accompanied by structural foot deformity and prior minor amputation).
The primary endpoint was the proportion of healed ulcers after 4 weeks; complete ulcer healing was defined as full epithelialization of the ulcer surface without exudate, and no requirement for dressings, confirmed at two consecutive visits. The secondary endpoints were (1) relative change of StO2 from baseline after 4 weeks
The inclusion criteria were (1) age 18 years or older, (2) confirmed diagnosis of recurrent hard-to-heal DFU, (3) the ability to understand the trial procedure and provide written informed consent, and (4) no comorbidities constituting contraindications to CO2 therapy (for the list of contraindications refer to the study by Ban Frangež et al.11). Exclusion criterion was clinically infected ulcer at baseline. A hard-to-heal ulcer was defined as an ulcer failing to show a 50% reduction in its area after 4 weeks of SOC. Note that formal power calculation was waived in favor of a feasibility-based recruitment strategy.
Patient baseline characteristics included sex/gender, age, body mass index (BMI), smoking status, ankle-brachial index (ABI), glycated hemoglobin (HbA1c), functional status, psychological symptoms, mobility status, and amputation history. ABI was measured using AngE™ Pro 8 ABI + (SOT Medical Systems, Maria Rain, Austria). Ulcer baseline characteristics included ulcer type (etiology), ulcer classification, ulcer area, and ulcer duration.
The values of characteristics were obtained from structured interviews, physical examinations, device-based measurements, blood testing, and medical records. HbA1c was analyzed in a certified hospital laboratory using standardized methods. An ulcer area was measured using the imitoMeasure app (imito AG, Zürich, Switzerland). Ulcer type was defined as neuropathic (in the presence of distal symmetrical polyneuropathy), ischemic (if ABI<0.90), or neuro-ischemic (if criteria for both, neuropathic and ischemic ulcer type were met). Ulcer classification used the SINBAD score and the Falanga wound bed score. Measurements of StO2 were carried out using the TIVITA® Tissue HSI system (Diaspective Vision GmbH, Am Salzhaff, Germany), with the center of the ulcer defined as the primary measurement site; the acclimatization period consisted of 15 minutes of supine rest in a room with ambient temperature of 22 °C. HSI was carried at weekly trial visits (after weeks 1, 2, 3 and 4); in the intervention group, measurements were carried out 30 min after completion of the 5th (week 1), 10th (week 2), 15th (week 3) and 20th (week 4) CO2 therapy, while in the control group the measurements were obtained at the same study time points, synchronized with the intervention schedule. The measurement site for StO2 was defined before the baseline measurement, and all subsequent measurements were performed at the same site. To ensure reproducibility across measurement sessions, a reference calibration was performed, and a fixed focal distance of 50 cm was maintained. Consistency was further ensured by automatic alignment of the regions of interest with a chosen anatomical landmark, i.e. the center of each participant’s ulcer.
Medical personnel continuously monitored participants for local reactions (irritation/edema) during CO2 therapies and observed for signs of distress. Systemic effects—including dizziness, headache, or palpitations—were patient-reported. Physical examination of ulcer site and patient reports were collected at each visit to identify any adverse events occurring between sessions.
After obtaining all baseline characteristics, participants were randomized to intervention and control groups in a 1:1 allocation ratio using a computer-generated randomization sequence (based on permuted block randomization method with a fixed block size of 4) in Microsoft Excel (Microsoft, Redmon, Washington, USA) prepared by an independent researcher not involved in treatment or outcome assessment. Allocation was concealed using sequentially numbered, opaque, sealed envelopes, opened only after completion of the baseline assessments. Electronic laboratory notebook platform was not used.
Intervention and control procedure
Participants in the intervention group received SOC alongside 20 sessions of CO2 therapy. These 50-minute sessions were administered once daily on weekdays (Monday–Friday) over a 4-week period. CO2 therapies were performed using the PVR system® medical device (Derma Art d.o.o. & PVR med d.o.o., Brežice, Slovenia). The participant's lower body was sealed in a single-use, biocompatible, medical-grade wrap. The wrap was filled with medical-grade CO2 to a 99.9% concentration for a 50-minute session. After 50 minutes, CO2 was pumped out and the wrap removed. Participants in the control group received only SOC without the administration of a placebo intervention. SOC included sharp debridement as clinically indicated at trial visits, local ulcer care with standardized dressings and scheduled changes three times per week (an amorphous hydrogel covered with a polyurethane foam secondary dressing), offloading using a half-shoe in the case of forefoot/hindfoot ulcers or a combination of an offloading shoe with a donut cushion/pad for midfoot ulcers, and infection screening at each trial visit (any infection developing during the trial was managed according to the local hospital’s protocols). SOC was provided consistently in both groups. To enhance adherence and minimize loss to follow-up, participants in both groups received reminder calls/SMS messages and, if necessary, transportation to and from the hospital. StO2 measurements were repeated after weeks 1, 2, 3, and 4. After week 4, ulcer healing was assessed, along with reassessment of ulcer area, ulcer classification (only in unhealed ulcers), StO2, and pain intensity.
Statistical analysis
Categorical variables are presented as counts and proportions. Continuous variables are summarized as mean ± standard deviation (SD) when normally distributed and as median (interquartile range (IQR)) when non-normally distributed. Normality was assessed using the Shapiro-Wilk test. Homogeneity of variances for between-group comparisons was evaluated using Levene’s test; when the equal-variance assumption was violated, the unequal-variance (Welch) t-test was applied.
Between-group comparisons of continuous variables were performed using the independent-samples t-test (or Welch t-test, as appropriate) for normally distributed data and the Mann-Whitney U test for non-normally distributed data. Within-group paired comparisons were performed using the paired-samples t-test or the Wilcoxon signed-rank test, as appropriate. For within-group repeated measurements across more than two time points, the Friedman test (ANOVA by ranks) was used. Categorical variables were compared using the chi-square test; Fisher’s exact test (two-sided) was used when expected cell counts were small (Fisher–Freeman–Halton exact test for r × c tables), with mid-p values reported where applicable.
All tests were two-sided, with statistical significance defined as p < 0.05. Analyses were conducted using IBM SPSS Statistics, version 21.0 (IBM Corp., Armonk, NY, USA).
Since complete baseline data were a prerequisite for enrolment, no data imputation method was required.
Results
A total of 33 patients with DFUs were enrolled in our RCT and screened. Three of these were not included in the trial after they declined to participate, having confirmed they would not be able to do so under the RCT's protocol. As a result, 30 patients were randomized in a 1:1 allocation ratio to the intervention (n = 15) and control (n = 15) groups, yielding group sizes of 15 each. The flow of participants through the RCT was documented according to protocol (Figure 1). All participants completed the trial as planned, with no losses to follow-up and no exclusions from the intention-to-treat analysis. Both study groups followed the protocol exactly as described.
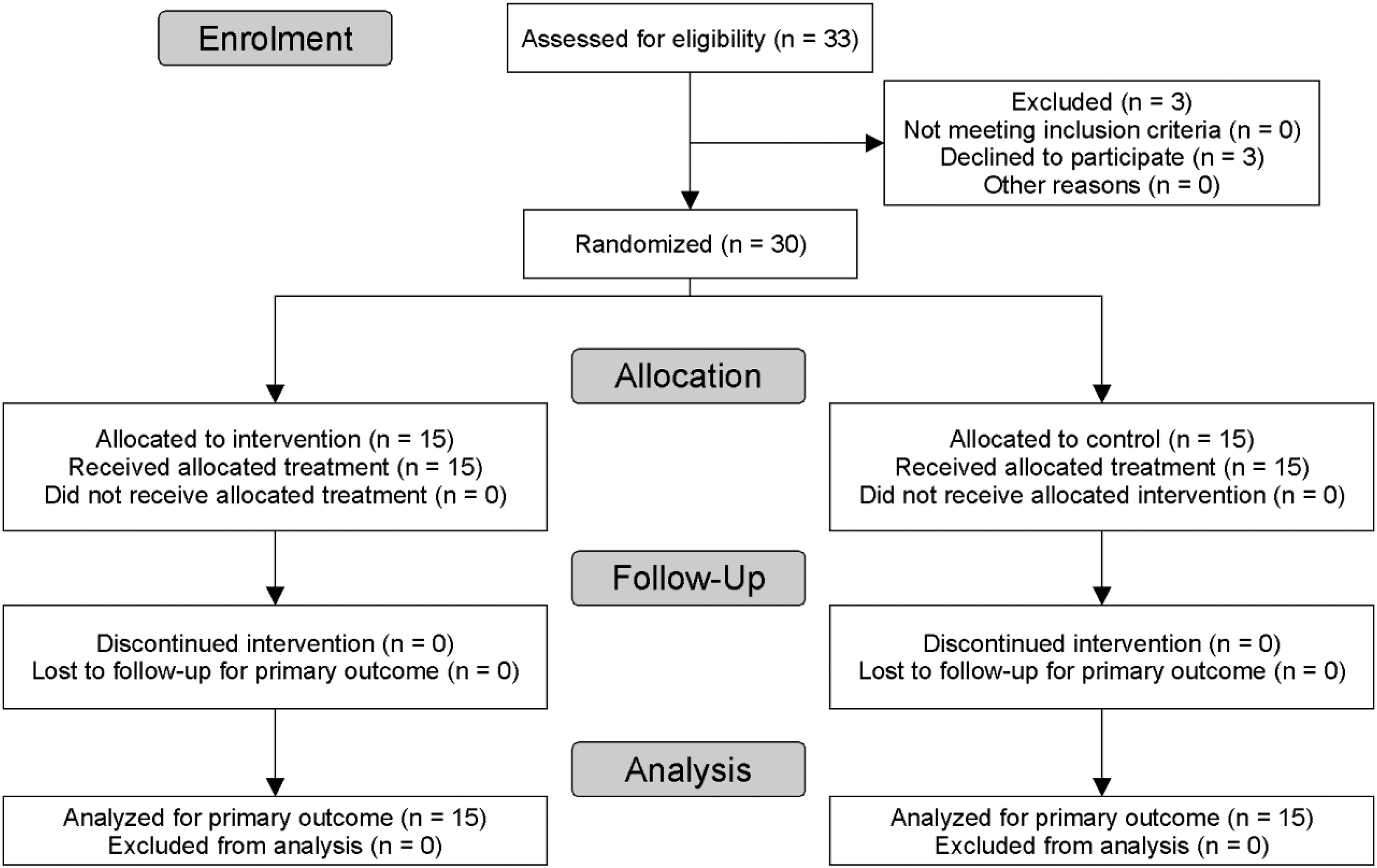
Flow diagram of the progress through the phases of our RCT of the intervention and study groups.
Table 1 presents baseline person and ulcer characteristics for participants in both groups.
Baseline person and ulcer characteristics of the control and intervention groups
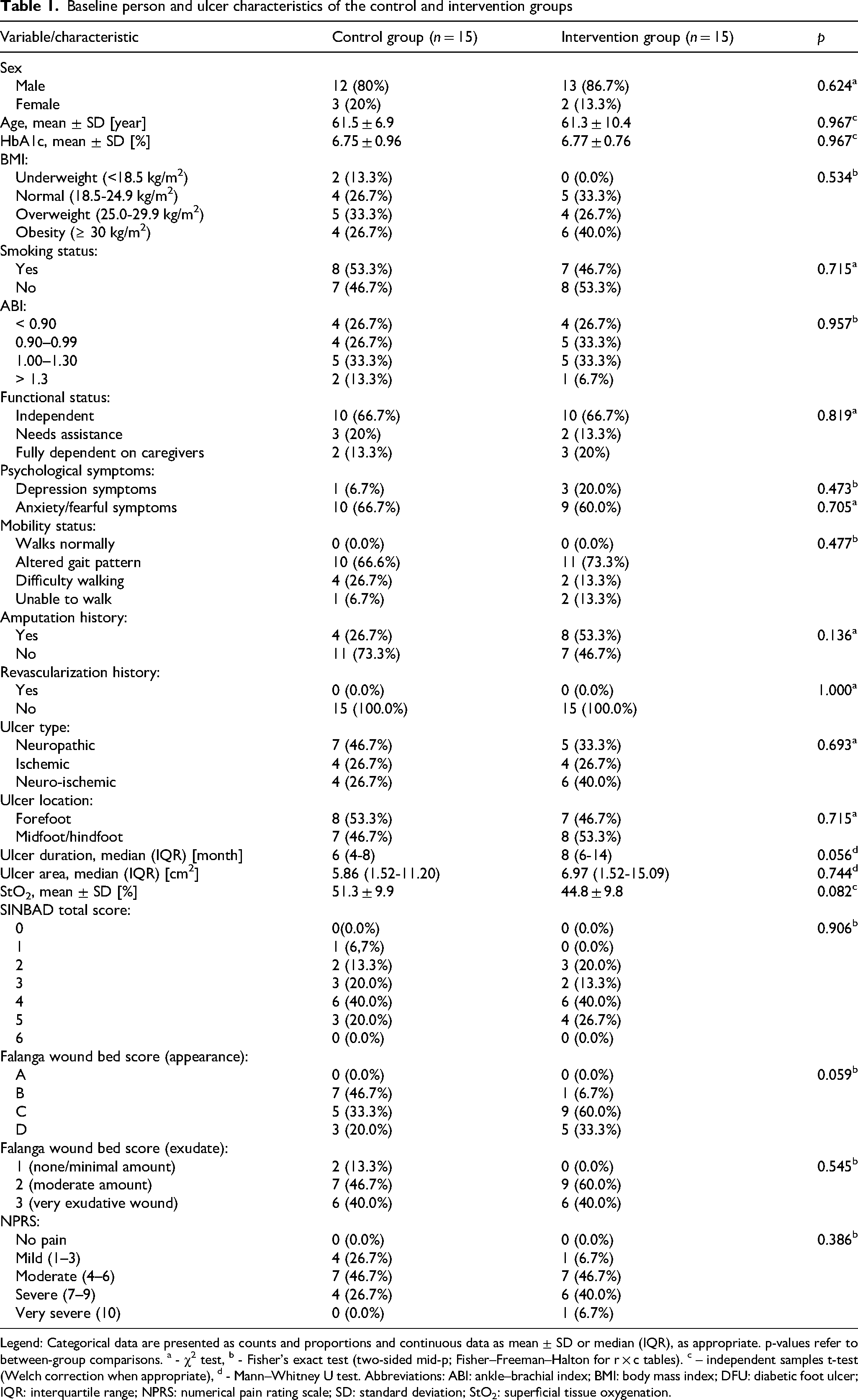
Legend: Categorical data are presented as counts and proportions and continuous data as mean ± SD or median (IQR), as appropriate. p-values refer to between-group comparisons. a - χ2 test, b - Fisher’s exact test (two-sided mid-p; Fisher–Freeman–Halton for r × c tables). c – independent samples t-test (Welch correction when appropriate), d - Mann–Whitney U test. Abbreviations: ABI: ankle–brachial index; BMI: body mass index; DFU: diabetic foot ulcer; IQR: interquartile range; NPRS: numerical pain rating scale; SD: standard deviation; StO2: superficial tissue oxygenation.
Age, HbA1c, and StO2 were normally distributed in both groups, whereas the distribution of all other variables was non-normal. At baseline, there were no statistically significant differences between the groups in any of the variables characterizing persons and ulcers. In addition, when it comes to the SINBAD score, there were no statistically significant differences between the scores for each category between the two groups. All previous amputations were classified as minor, occurring distal to the ankle (e.g., toe, ray, transmetatarsal, Lisfranc, or Chopart amputations).
Table 2 shows characteristics of the intervention and control groups after 4 weeks.
Ulcer characteristics and pain scores of the control and intervention groups after 4 weeks
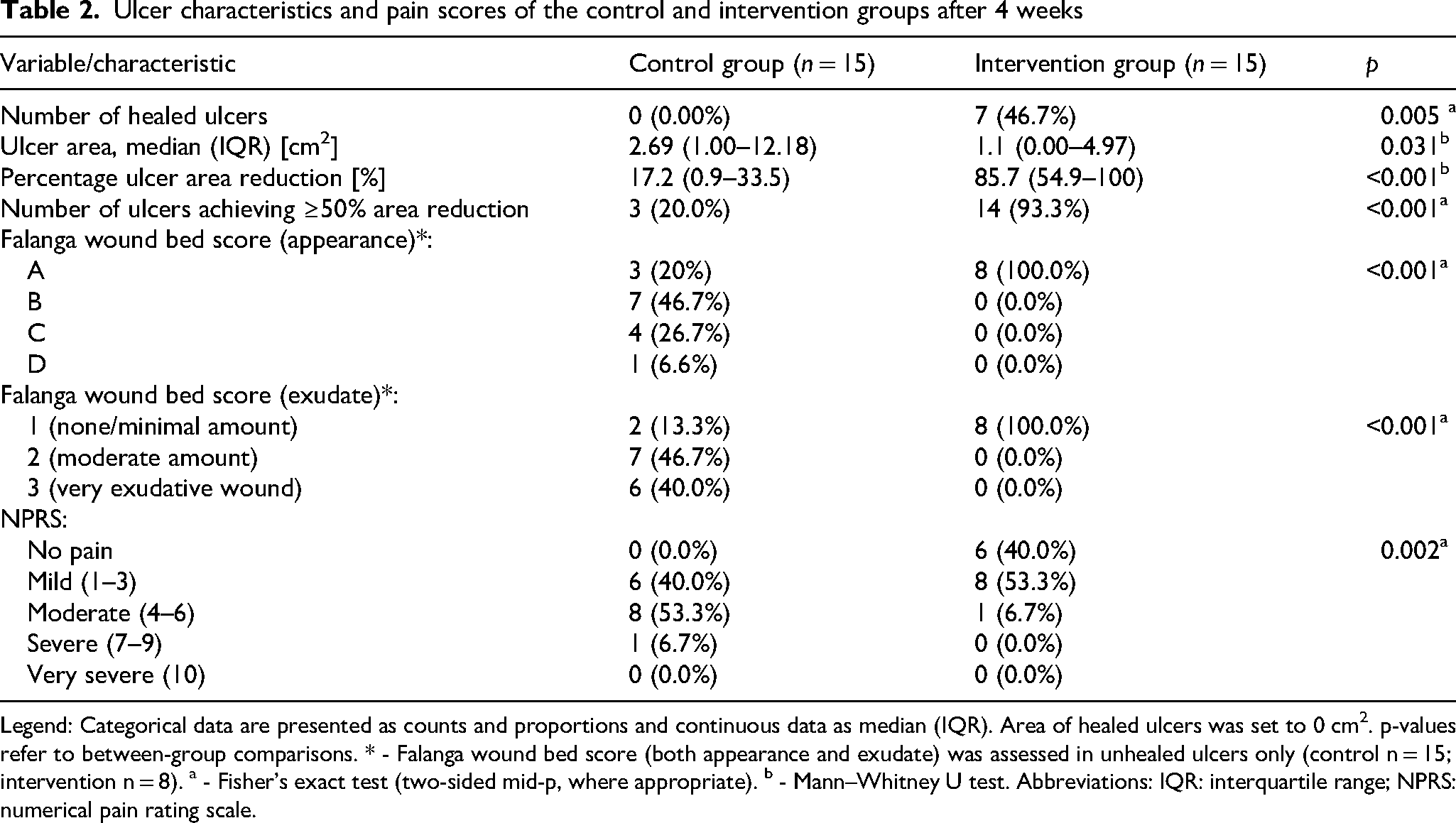
Legend: Categorical data are presented as counts and proportions and continuous data as median (IQR). Area of healed ulcers was set to 0 cm2. p-values refer to between-group comparisons. * - Falanga wound bed score (both appearance and exudate) was assessed in unhealed ulcers only (control n = 15; intervention n = 8). a - Fisher’s exact test (two-sided mid-p, where appropriate). b - Mann–Whitney U test. Abbreviations: IQR: interquartile range; NPRS: numerical pain rating scale.
In addition to these results, in 7 unhealed ulcers in the intervention group after 4 weeks, the ulcer area was reduced by more than 50%, i.e., 55.3% (52.3% - 76.9%). In the control group, only 3 such ulcers were observed. In addition, the ulcer area of one ulcer in the control group even increased. There was a statistically significant difference in the number of ulcers, with their area reduced by 50% or more, between the intervention and control groups (p < 0.001; Fisher’s exact test (two-sided; mid-p where applicable). Falanga wound bed scores were evaluated only in ulcers that remained open at week 4; therefore, between-group comparisons reflect differences among persistent wounds Lastly, the Wilcoxon signed rank test revealed a statistically significant difference in ulcer area before and after 4 weeks in control (p = 0.006) and treatment group (p = 0.012). To sum these results, CO2 therapy in combination with SOC is superior to SOC alone in terms of (1) proportion of healed ulcers after 4 weeks (primary endpoint), (2) percentage ulcer area reduction, (3) proportion of ulcers with ulcer area reduction of ≥50% and (4) formation of granulation tissue/reduction of exudate in ulcers after 4 weeks (all supportive endpoints), and (5) statistically significant change in pain intensity (second secondary endpoint).
Table 3 presents StO2 values measured after weeks 1, 2, 3, and 4, together with the between-group differences in StO2 (ΔΔStO2). The ΔΔStO2 values favored the intervention group at all post-baseline trial visits (p < 0.001).
Superficial tissue oxygenation StO2 measured with hyperspectral imaging: weekly values and between-group differences
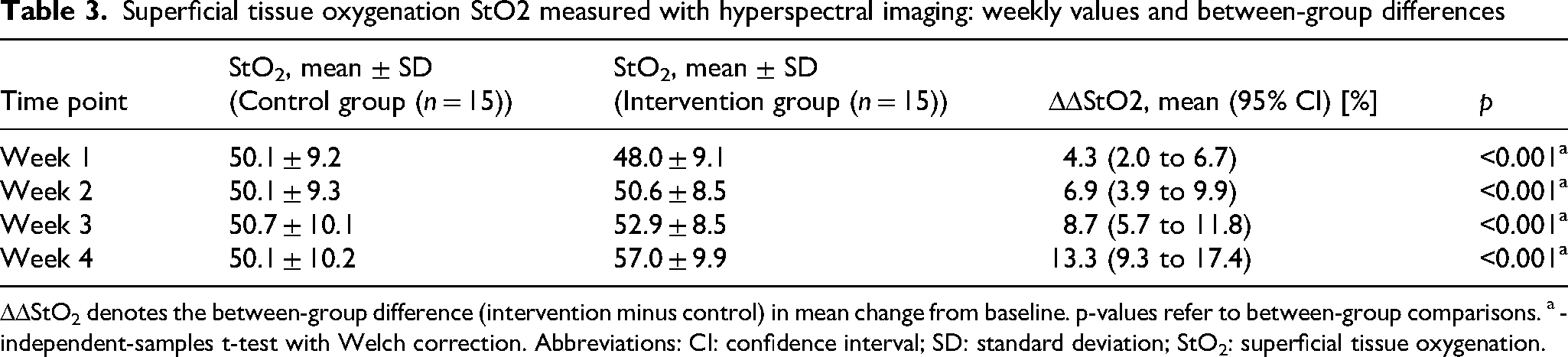
ΔΔStO2 denotes the between-group difference (intervention minus control) in mean change from baseline. p-values refer to between-group comparisons. a - independent-samples t-test with Welch correction. Abbreviations: CI: confidence interval; SD: standard deviation; StO2: superficial tissue oxygenation.
The %ΔStO2 values were calculated for both groups at weeks 1, 2, 3, and 4 (Figure 2). In the intervention group, %ΔStO2 increased progressively over time, whereas the change in the control group remained stable, resulting in a widening between-group separation throughout the trial. After 4 weeks, the relative change in StO2 from baseline was 29.6 ± 19.6% in the intervention group compared to -2.2 ± 6.9% in the control group (between-group difference was 31.8% (95% CI 20.5%–43.0%) (p < 0.001).
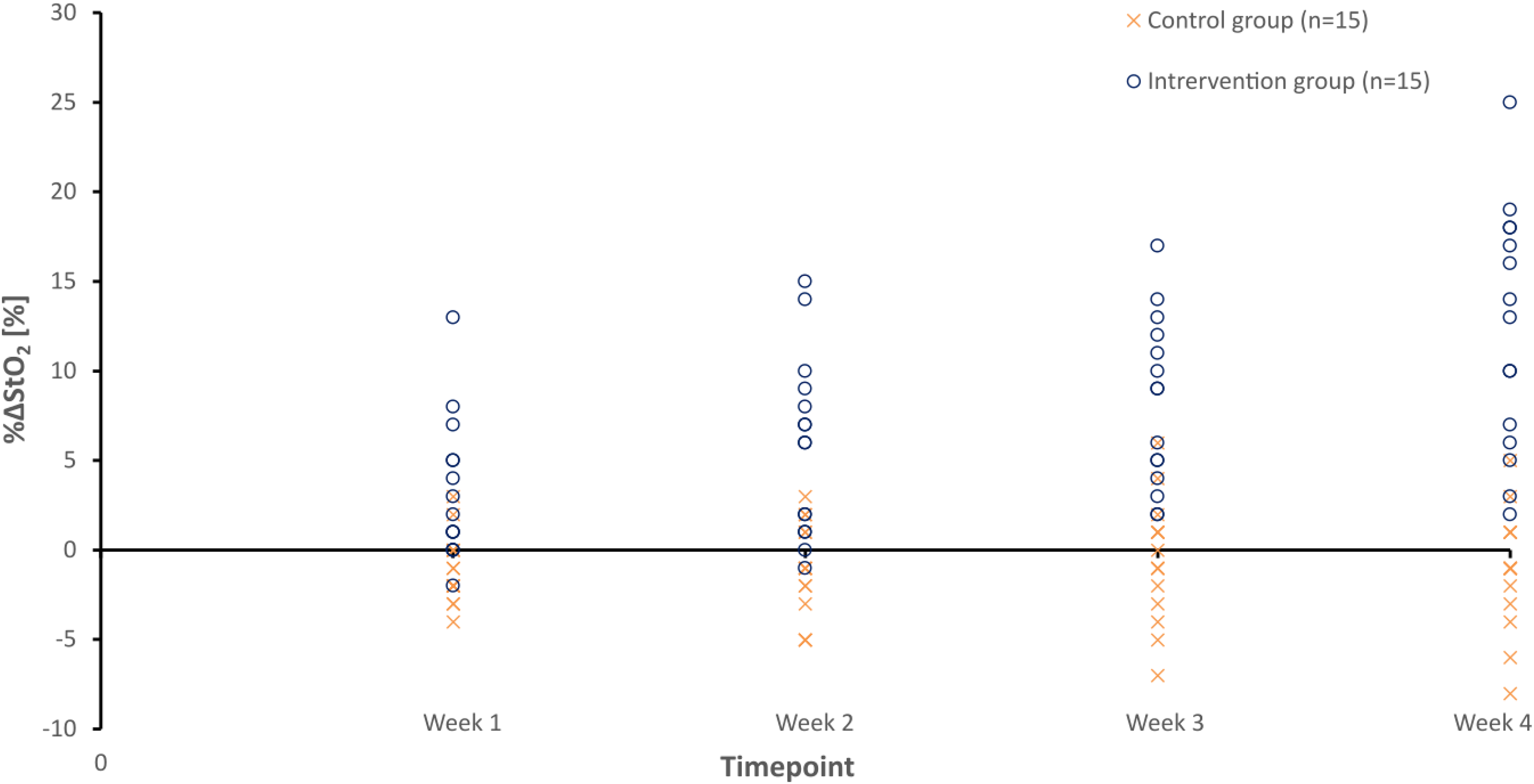
Relative change of superficial tissue oxygenation from baseline (%ΔStO2) over time. Individual measurements are shown as scatter points. The horizontal axis labels refer to synchronized weekly trial visits conducted after 1, 2, 3, and 4 weeks.
Finally, no adverse events were observed in either group, and no participants reported negative sensations or discomfort during the trial.
Discussion
Results of our RCT demonstrate that CO2 therapy, when added to SOC, can meaningfully improve outcomes in a high-risk subgroup of DFUs with recurrent, hard-to-heal ulcers. After 4 weeks, 46.7% (7 out of 15) of ulcers in the intervention group were completely healed compared with none (0 out of 15) in the control group (p = 0.005). Consistently, the intervention group achieved a markedly greater percentage ulcer area reduction (85.7% vs. 17.2%, p < 0.001) and a substantially higher proportion of ulcers reaching the clinically relevant ≥50% area-reduction threshold (93.3% vs. 20.0%, p < 0.001). Together, these results suggest that CO2 therapy may help overcome the stagnant healing trajectory characteristic of hard-to-heal DFUs. Importantly, baseline superficial tissue oxygenation tended to be lower in the intervention group, suggesting that the observed differences in healing were unlikely to be attributable to more favorable initial perfusion status. Compared to other trials studying the effect of CO2 on DFU healing9,10, the achieved proportion of healed ulcers in the intervention group is lower. This is most likely attributable to a deliberate inclusion of a particularly challenging subgroup, i.e., patients with recurrent, hard-to-heal DFUs, which makes the observed healing rate clinically meaningful, particularly given the fact that none of the ulcers in the control group healed after 4 weeks.
Beyond the observed proportion of healed ulcers in the intervention group, the proportion of achieving percentage area reduction of ≥50% and marked improvements in wound-bed appearance and exudate control in the intervention group suggest that CO2 therapy favorably modifies the local ulcer environment, promoting granulation and progression toward healing even when full epithelialization is not yet achieved.
A core barrier to DFU healing is local tissue hypoxia driven by impaired microcirculation. The significant improvement in StO2 serves as an objective physiological marker of the observed clinical response. Mechanistically, the observed improvement in tissue oxygenation is likely multifactorial and may involve complementary physiological pathways, including (1) enhanced oxygen unloading from hemoglobin associated with increased CO2 (Bohr effect; rightward shift of the oxyhemoglobin dissociation curve)12, (2) CO2-associated vasodilatory responses at the microcirculatory level, and (3) changes in endothelial (including NO-mediated) and neurogenic regulation of cutaneous blood flow7. These findings are consistent with prior clinical reports of improved wound outcomes following transcutaneous CO2 therapy9,10, supporting the clinical relevance of CO2-evoked improvements in local microcirculation. To properly interpret StO2 results, it is important to note there is a well-established physiological relationship exists between StO2 and transcutaneous oxygen pressure tcpO2, as both parameters are bound by the hemoglobin-oxygen dissociation curve, even though both parameters measure different physiological parameters. In undisturbed, resting chronic wounds, StO2 and tcpO2 correlate well.13 However, this correlation disappears when physiological stress is introduced (e.g., acute surgical trauma14). This divergence occurs because StO2 reacts dynamically to regional fluid and hemoglobin volume shifts, whereas tcpO2 captures forced capillary oxygen pressure under induced hyperemia.
CO2 therapy was also associated with a clinically meaningful reduction in pain. At week 4, 40.0% of participants in the intervention group reported being pain-free, compared with 0% in the control group (p = 0.002), while moderate-to-severe pain remained common in the control group (60.0%) but was uncommon in the intervention group (6.7%). Given the well-established impact of pain on quality of life in DFU patients15, this suggests an additional patient-centered benefit beyond ulcer healing.
Finally, no adverse effects were observed in the intervention group, supporting the feasibility and local safety profile of CO2 therapy, consistent with previous studies9–11.
This RCT is subject to several limitations. First, the small sample size (n = 30) reduces the statistical power (due to type II error) and limits the generalizability of the findings. Second, the feasibility-based recruitment without formal power calculation potentially may have precluded the detection of subtle, but clinically significant differences; thus, non-significant results should be interpreted with caution. Third, the open-label design (necessitated by the nature of the intervention) may have introduced performance or attention bias, which must be considered when interpreting the magnitude of the observed effects. Finally, due to the lack of a follow-up period, it is not possible to draw definitive conclusions regarding long-term sustained ulcer healing or ulcer recurrence rates. Nevertheless, this RCT provides exploratory efficacy data and mechanistic insight and lays the groundwork for future adequately powered multicentre studies with extended follow-up.
Conclusions
CO2 therapy in combination with SOC is superior to SOC alone in healing recurrent, hard-to-heal DFUs, including persistent ulcers at prior minor-amputation sites. It is associated with significant improvements in tissue oxygenation, reduced pain and consequent improvement of quality of life. CO2 therapy represents a promising non-invasive adjuvant to standard care for hard-to-heal DFUs.
Footnotes
Acknowledgments
The authors have no acknowledgments to declare.
Author Contributions
M.P.: Investigation, Formal Analysis, Writing – original draft; B.A.: Data Curation, Formal Analysis, Investigation, Visualization, Writing – original draft; J.L.L.-M.: Writing – Formal Analysis, Review & Editing; M.B.: Writing – Formal Analysis, Review & Editing; N.P.: Writing – Formal Analysis, Review & Editing; I.F.: Conceptualization, Methodology, Project administration, Supervision, Writing – original draft
Ethical Considerations
The trial was conducted in accordance with the Declaration of Helsinki and approved by the National Medical Ethics Committee of the Republic of Slovenia (Approval ID: 0120-316/2024-2711-3, date of approval: August 20, 2024).
Consent to participate
Written informed consent was obtained from all individual participants included in the study.
Consent for Publication
Not applicable.
Funding Statement
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interest
Miloš Potkonjak no conflicts of interest to declare. Bernardka Ančimer no conflicts of interest to declare. José Luis Lázaro-Martínez no conflicts of interest to declare. Marianne Brodmann no conflicts of interest to declare. Nikolaos Papanas has been an advisory board member of Astra-Zeneca, Bayer, Boehringer Ingelheim, Menarini, MSD, Novo Nordisk, Pfizer, Takeda and TrigoCare International; has participated in sponsored studies by Astra-Zeneca, Eli-Lilly, GSK, MSD, Novo Nordisk, Novartis and Sanofi-Aventis; has received honoraria as a speaker for Astra-Zeneca, Bayer, Boehringer Ingelheim, Eli-Lilly, Elpen, Menarini, MSD, Mylan, Novo Nordisk, Pfizer, Sanofi-Aventis and Vianex; and has attended conferences sponsored by TrigoCare International, Astra-Zeneca, Boehringer Ingelheim, Eli-Lilly, Galenica, Menarini, Novo Nordisk, Pfizer and Sanofi-Aventis. Igor Frangež no conflicts of interest to declare.
Data Availability