
Abstract
The purpose of this pilot study was to examine the feasibility and acceptability of Reiki therapy for cancer survivors with moderate-to-severe symptom clusters. Adult patients with a neoplasm diagnosis, not currently undergoing active treatment, and reporting a fatigue score of ≥ 4 and two other symptoms were eligible to participate. The intervention was six 30-45-minute Reiki sessions within 6-8 weeks. The Edmonton Symptom Assessment System (ESAS-9) was completed pre- and post-Reiki session. Quality of life (PROMIS-29) measures were completed at baseline and 8 weeks after the first Reiki session. As a pilot feasibility study, recruitment, retention, attendance, data completeness, and acceptability were the focus. Descriptive statistics were generated for ESAS and PROMIS data, but no hypothesis testing was done. Twenty-three patients were pre-screened and ten were eligible, enrolled in the study, and completed baseline measures. Nine signed up for Reiki and six of those participants completed the intervention and follow-up measures (67%). All participants were female and non-Hispanic, 70% were White, 20% were African American/Black, and 10% were multiracial. Participants attended an average of 5.5 Reiki sessions. Outcome data completeness was 100%. Numerical improvements in all symptom scores and quality of life domains after Reiki were observed. Participants were overall satisfied with the Reiki. This pilot study of Reiki for cancer survivors demonstrated satisfactory feasibility. Highly preliminary assessment of outcome measures revealed sensitivity to change following Reiki. This study provides support to proceed with more research; however, modifications are needed before conducting a fully powered randomized controlled trial.
Introduction
Cancer and its treatment often produce a wide range of distressing physical and psychological symptoms, including fatigue, pain, sleep disturbance, anxiety, and decreased sense of wellbeing that often persist following active treatment. 1 There are an estimated 18.6 million cancer survivors in the United States, approximately 1 in 18 Americans, and this number is expected to grow in the coming years. 2 Despite advances in pharmacological management, symptom burden remains high among cancer survivors, and some symptoms, such as fatigue and anxiety, are often challenging to treat with standard therapies alone. 3 Fatigue is one of the most common symptoms experienced by both patients undergoing active cancer treatment and cancer survivors who have completed treatment, disrupting their quality of life.4-7 Additionally, polypharmacy, treatment side effects, and individual variability in response further complicate symptom management.8,9 As a result, there is growing interest in the use of nonpharmacological interventions to complement conventional care and support quality of life throughout the cancer continuum. Organizations including the Society for Integrative Oncology, 10 Society of Clinical Oncology, and the National Comprehensive Cancer Network11-13 endorse nonpharmacologic, complementary therapies to address cancer patients’ symptoms including cancer-related fatigue.14,15
Reiki is a gentle, non-invasive, integrative, biofield therapy originating in Japan that has demonstrated the ability to improve health-related symptoms in a variety of patient populations.16-22 Biofields are energy and/or information fields that surround living organisms and play a role in maintaining physiological and psychological homeostasis, thus having the potential to influence overall health. 23 Reiki involves a trained practitioner placing their hands lightly on or a few inches above the body of a receiver to elicit the relaxation response,23,24 thus stimulating the parasympathetic nervous system and leading to relaxation, decreased heart rate and blood pressure,25,26 and increased heart rate variability. 27 This physiological shift could explain some of Reiki’s observed effects on symptom relief, particularly in conditions associated with autonomic dysregulation and chronic stress.
Reiki is offered in many hospital and clinical settings in the U.S. as part of whole-person care, including in most top hospitals, 28 such as Cleveland Clinic, Mayo Clinic, and Johns Hopkins. In oncology patients, Reiki has been shown to improve symptom clusters 29 including fatigue30-35 and anxiety,32,34-37 but also pain,30-32,34,36,38 sleep quality, 36 stress, 31 and overall wellbeing/quality of life.32,33,36,38 However, no study to date has evaluated Reiki as a standalone therapy for cancer survivors no longer in active treatment.
This single-arm feasibility study aimed to build on our previous results showing benefits in fatigue, anxiety, pain, nausea and wellbeing in cancer patients receiving infusions. 32 The purpose of the current study was to explore the feasibility and acceptability of 6–8 weeks of a single arm trial of Reiki therapy for adult patients with fatigue at the University Hospitals Connor Whole Health (UHCWH) Integrative Oncology Clinic in Ohio. As this is the first study to date where outpatients received Reiki without receiving other treatments such as chemotherapy or radiation, evaluating feasibility is important. The results from this study will inform future, larger-scale trials and contribute to the growing body of evidence supporting integrative therapies in oncology care.
Methods
Study Design and Setting
This was a single-arm feasibility study conducted at University Hospitals Connor Whole Health (UHCWH) Integrative Oncology Clinic in Cleveland, Ohio. The study aimed to evaluate the feasibility and acceptability of Reiki therapy for managing moderate to severe cancer-related symptoms and to explore symptom changes over time. The study was conducted from July 2024 to August 2025. Reporting guidelines used were the CONSORT extension for pilot and feasibility studies, recommended for the current study type. 39
Participants
Eligible participants were adults aged 18–89 with a confirmed neoplasm diagnosis (ICD-10 C00–D49), receiving care at the UHCWH Integrative Oncology Clinic. Participants were required to report at least three symptoms rated ≥4/10 on the Edmonton Symptom Assessment System (ESAS), 40 including fatigue and at least two other symptoms from the 9-item ESAS questionnaire. Additional eligibility criteria included English fluency, ability to provide informed consent, and access to email and a digital device with internet capability. Key exclusion criteria included significant uncorrected cognitive or visual impairments, active psychosis, pregnancy, metastatic disease, recent Reiki exposure (within 3 months), and receipt of chemotherapy, immunotherapy, or radiation within the past 3 months (except for tamoxifen or aromatase inhibitors). Participants with metastatic disease were excluded because of their greater likelihood of rapidly changing symptoms, more intensive treatment side effects, and overall clinical instability.
Due to the exploratory nature of the study, no sample size planning was done but for pragmatic reasons, a target size of 10-20 participants was selected as a realistic number for a single-center, single-provider study with only one day of Reiki sessions per week.
Participants were recruited via provider referral by the Integrative Oncologist (SR). Eligibility was confirmed by research assistants (SC, JC) through chart review and a virtual (via Zoom) or in-person screening process. Once eligibility was confirmed, informed consent and baseline data collection was obtained using the secure online data capture software REDCap. 41 There was no compensation for completion of surveys, but participants did not have to pay for the Reiki sessions as they were covered by philanthropic funds.
Reiki Intervention
Participants received six individual Reiki therapy sessions over a maximum of eight weeks. The initial session lasted 45 minutes; the subsequent five sessions were 30-45 minutes each. All sessions were delivered in person by a certified Reiki Master integrated into the oncology clinic’s symptom management team. The Reiki Master (KF) was trained in Usui Reiki Ryoho with 22 years of experience, including 18 years of experience providing Reiki to patients in the hospital setting. She was also a holistic nurse and already a paid part of the integrative health team prior to this study.
The Reiki was administered in a quiet setting in a room at the symptom management clinic. The participant was lying down fully clothed in the supine position on a massage/treatment bed with their eyes closed, and the practitioner was either standing or seated next to them during the session. During the 30-45 min session, the practitioner (1) set their intention for the session (for the patient’s highest greatest well-being, health, and healing); (2) invited the recipient to set their intention for the session, if they chose; and (3) used routine Reiki hand placements with the option to deviate for an individualized treatment. The Reiki sessions included both touch and non-touch positions, such as for sensitive areas of the body (e.g., chest, pelvis). The Reiki was administered hands-on for the following positions: head: frontal, temporal, occipital, posterior neck, anterior and posterior shoulders, hands, mid-back, lower back, lateral hips, ankles, dorsal and planter surfaces of feet. The Reiki was administered hands off/hovering for the following positions: anterior chest, abdomen, pelvic region or anterior neck and chest. During the session the Reiki practitioner provided relaxing music from the Spotify Spa channel. Following the session, patients were invited to discuss their experience with Reiki.
Fidelity to the protocol, including session duration, whether hands were on, off, or both, and whether music was played during the session was recorded by the Reiki practitioner in the electronic health record (EHR).
Data Collection and Measures
Participant characteristics. At enrollment, participants completed a demographic survey capturing age, gender, race, and ethnicity. Additional clinical data, including tumor location, cancer stage, and Eastern Cooperative Oncology Group (ECOG) status (6-point scale from 0 - fully active to 5 – deceased) 42 were extracted from the EHR. Participants were asked if they had ever received Reiki (yes, no, I don’t know).
Expectancy. At baseline, before having any Reiki sessions, they also completed an expectancy survey with the questions: “At this point, how much do you really feel that the Reiki treatment will help you to reduce your cancer-related symptoms?” (rated from 1 = not at all, to 9 = very much) and “By the end of six weeks of Reiki treatment, how much improvement in your cancer-related symptoms do you really feel will occur?” (rated from 0-100%).
Feasibility
There are no universally recommended benchmarks for meeting feasibility due to extensive variability across studies. However, we set the criteria for meeting feasibility to proceed to a fully powered RCT based on discussions with the research team.
Recruitment. Screening rate (# agreeing to be screened/# approached) and recruitment rate (# enrolled/# eligible) were assessed. Criteria for a successful screening rate was set to ≥ 35% and recruitment rate was set to ≥ 50%.
Attendance. Participant attendance was recorded via EHR documentation and REDCap forms. We considered individual attendance to be acceptable if a given participant attends 4 of 6 sessions in 8 weeks.
Data completeness. We tracked completeness of ESAS and PROMIS-29 data collection, and patterns and proportions of missing data at each time point. Success of data completeness was be determined by ≥ 90% completion of all items of all outcome measures at each time point (e.g., at least 26/29 items from PROMIS-29 completed at baseline).
Retention. Successful retention criterion was set to ≥ 70% (# of participants that completed the final survey time point/# of participants receiving intervention).
Acceptability. Participants also rated their satisfaction with the Reiki experience eight weeks after the first Reiki session using a single-item scale from 0 (“not at all satisfied”) to 10 (“completely satisfied”) and were able to provide written feedback about the Reiki if desired. Acceptability was considered satisfactory at a mean of ≥ 7.
Cancer-related symptoms. Symptoms were assessed using the Edmonton Symptom Assessment System (ESAS) 9 item version 40 before and after each Reiki session. The ESAS-9 evaluates the intensity of nine cancer-related symptoms (pain, tiredness/fatigue, drowsiness, nausea, lack of appetite, shortness of breath, depression, anxiety, wellbeing) on a 0–10 numeric scale. A total ESAS score is calculated by summing the 9 scores. For each symptom, a score of 0 indicates no symptom, 1–3 is mild; 4–6 is moderate; and 7–10 indicates severe symptomatology. Clinically meaningful improvement is a reduction of at least 1 point for any symptom and 3 points or more for the total score. 42 We were particularly interested in the fatigue score as the study population had to have a baseline fatigue score of ≥ 4.
Quality of life. The Patient-Reported Outcomes Measurement Information System (PROMIS-29) 43 instrument was administered at baseline/enrollment and eight weeks after the first Reiki session via personal smartphone or electronic device. PROMIS-29 measures quality of life across seven domains such as physical function, pain, fatigue, sleep disturbance, depression, anxiety, and social participation on a 5-point Likert scale. There is also a pain intensity item rated from none (0) to worst possible (10). The seven sub-scales of the PROMIS-29 are normalized to T-scores, with mean = 50 and SD = 10. A score of 50 reflects the U.S. adult population average for each PROMIS scale 43 and an improvement of between 2-6 points indicates a minimal important difference/change. 44 For symptoms of anxiety, depression, fatigue, sleep disturbance and pain interference, higher T-scores mean worse health. For the functional domains of physical function and social participation, higher T-scores mean better health. 45
Data Analysis
Descriptive statistics were used to evaluate feasibility metrics, including recruitment, retention, attendance, data completeness, acceptability (participant satisfaction) of the intervention. Patient-reported outcomes were summarized using means, standard deviations, counts, and percentages. No formal hypothesis testing was conducted, consistent with the exploratory nature of feasibility studies.
Ethical Considerations
The study received approval from the University Hospitals Institutional Review Board (STUDY20240067, Case3Z24). All participants provided written informed consent prior to enrollment. Risks to participants were minimal, limited to potential discomfort during Reiki sessions or distress from symptom questionnaires. Participants were allowed to withdraw at any time without penalty. Confidentiality was maintained through secure data handling in REDCap, Velos, and OnCore systems. Safety protocols included alerting the clinical care team for any participant reporting ESAS depression scores ≥7 or PROMIS depression t-scores ≥ 70.
Results
Feasibility
Recruitment. During the one-year study period (July 2024 – August 2025), twenty-three patients were pre-screened and of those, n = 3 were ineligible (n = 2 active treatment, n = 1 metastatic disease); an 87% screening rate, exceeding the screening criteria of ≥ 35%. The remaining 20 patients were approached for participation. Of those, n = 10 were eligible, enrolled in the study, and completed baseline measures (n = 6 no response; n = 2 did not meet ESAS criteria; and n = 2 were not interested), generating a 56% recruitment rate (10 enrolled/18 eligible), meeting the criteria of ≥ 50%. Of those who were eligible and agreed to participate, 1 participant delayed scheduling the Reiki to beyond the study time frame, leaving n = 9 that enrolled and began the Reiki intervention. Six participants (67%) completed the intervention and follow-up measures. Two participants stopped scheduling Reiki sessions, and one withdrew from the study due to pre-existing symptoms (see CONSORT Figure 1). CONSORT participant flow diagram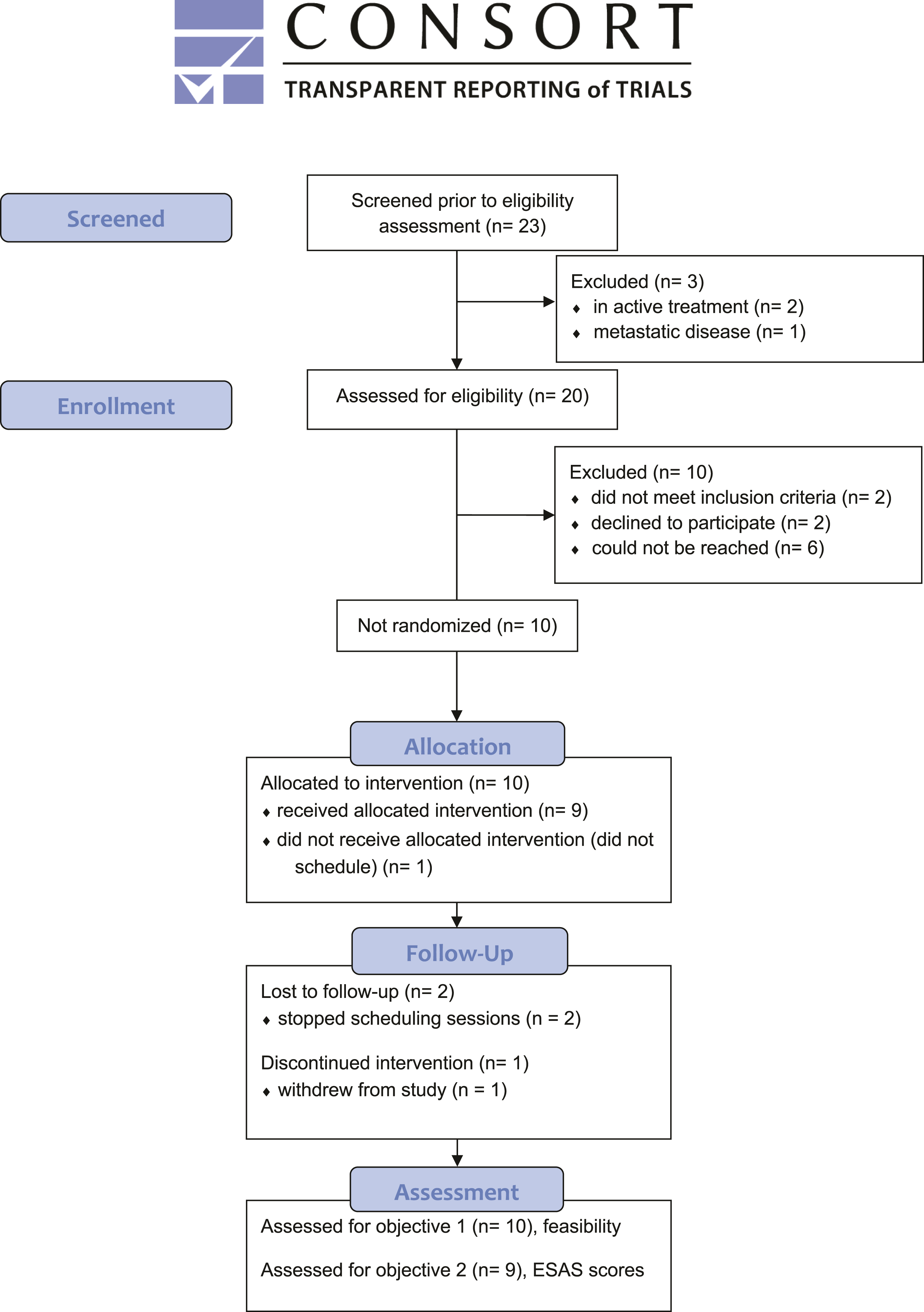
Participants’ Demographics and Characteristics at Baseline
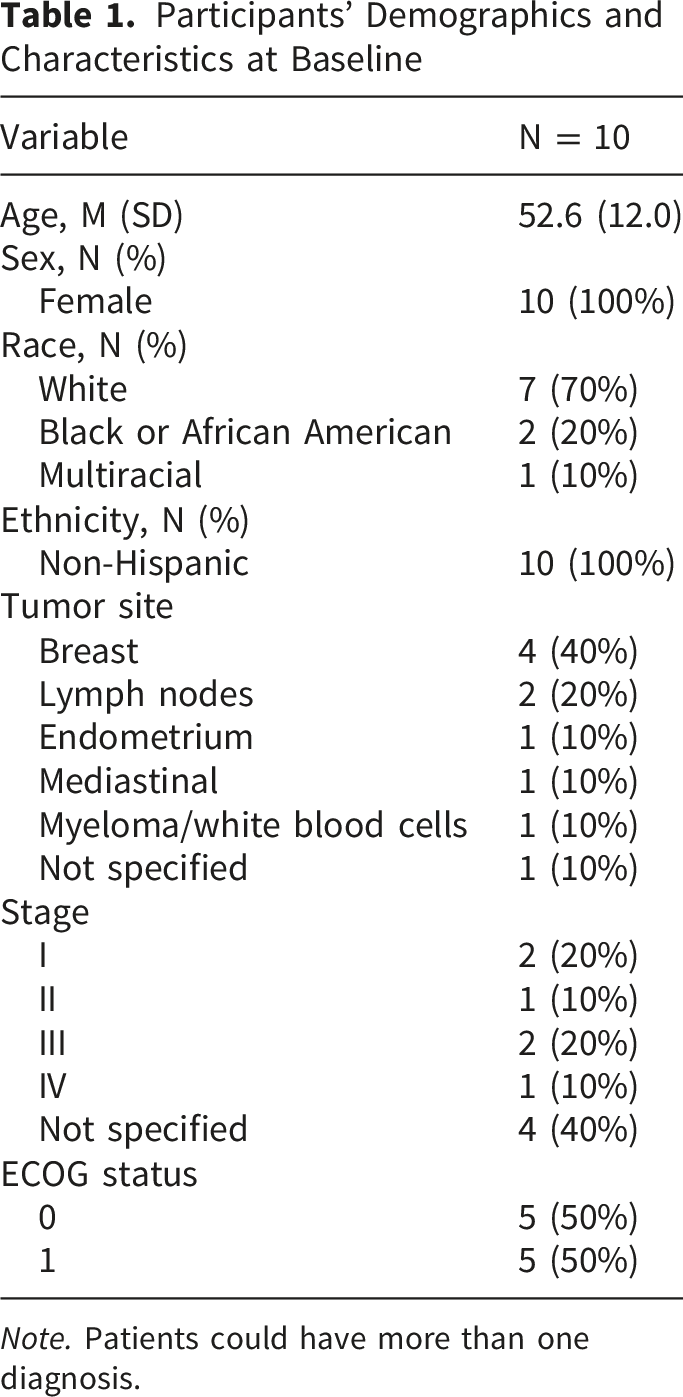
Note. Patients could have more than one diagnosis.
Expectancy. To the question, “At this point, how much do you really feel that the Reiki treatment will help you to reduce your cancer-related symptoms?” participants had a mean rating of 6.44 (SD = 1.74). For the question, “By the end of six weeks of Reiki treatment, how much improvement in your cancer-related symptoms do you really feel will occur?” participants had a mean rating of 75.5% (SD = 13.79), indicating moderate expectancy.
Attendance. Overall, participants attended an average of 5.5 out of 6 Reiki sessions (range 3-6). Six of the 9 participants (67%) completed all 6 Reiki sessions, meeting the attendance criteria of at least 4 Reiki sessions within 8 weeks.
Data completeness. There was no missing data for the outcome measures (ESAS and PROMIS-29), indicating a 100% data completion rate.
Retention. All participants completed all ESAS measures before and after each Reiki session (100% complete). Of the 9 participants that received the Reiki intervention, 6 completed the follow-up PROMIS measures (67% retention), falling 3% short of criteria.
Acceptability. Participants’ mean satisfaction with the Reiki intervention was 8.2 out of 10 and ranged from 5-10. Three participants provided additional comments about the Reiki, which were the following: “Better outcomes than I thought I would receive. This made a world of difference for my energy and stress levels.” “Very relaxing and peaceful, soothing.” “After each session, I felt relaxed, refreshed and less anxious. It took a few sessions to figure out the best way for me to receive Reiki, and once I did, it was so invaluable. I also feel that it was a cumulative feeling of wellbeing overall.”
Out of the six participants that completed all six Reiki sessions, four continued scheduling Reiki sessions after the study as integrative oncology patients.
Fidelity. The Reiki protocol was adhered to, with all sessions lasting between 30-45 minutes, both hands on and hands off positions were used, and meditation music was played during all sessions.
Preliminary Assessment of Outcomes
Due to this being a feasibility study, there was no power calculation performed, and the small sample size did not permit data analysis to detect statistical differences. However, we present descriptive statistics of means and standard deviations (SDs) at each time point to indicate potential symptom improvements for future fully powered research.
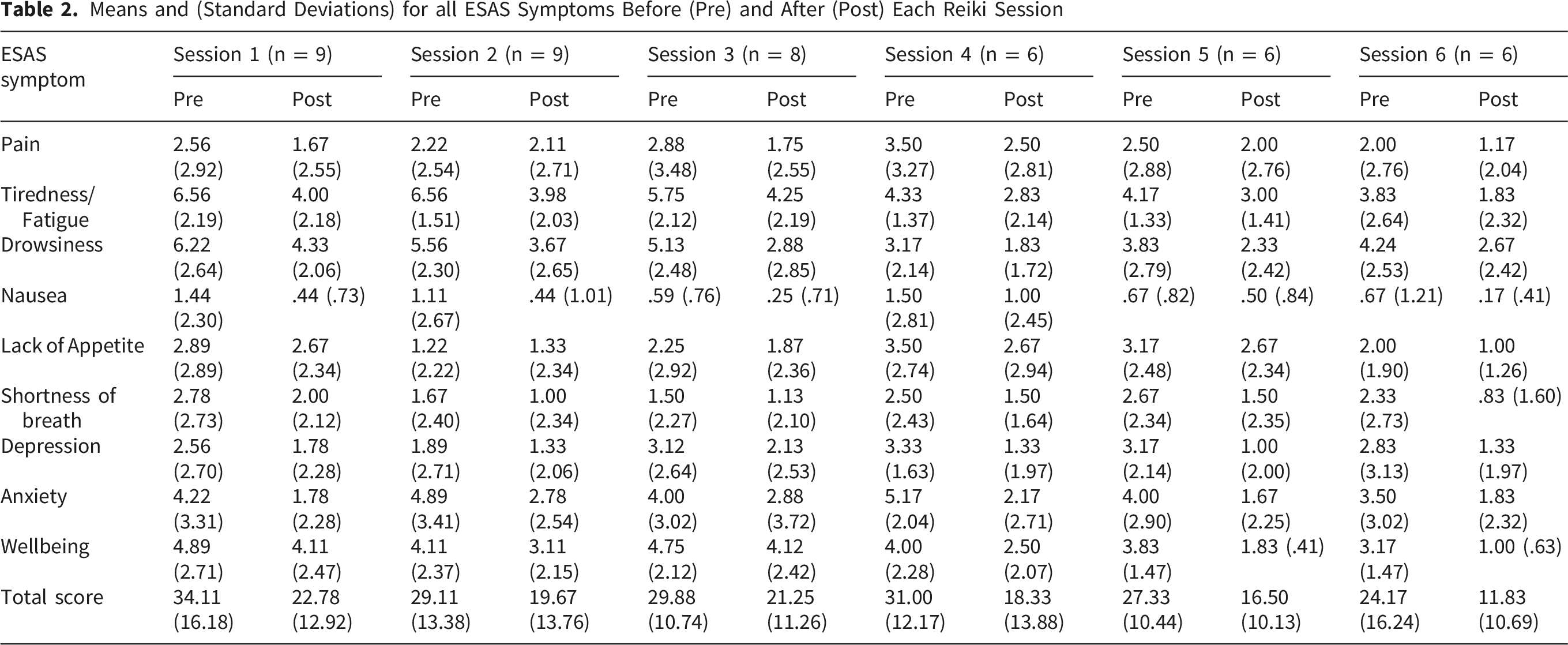
Cancer-related symptoms. Figure 2 displays the means and SDs of the total ESAS score (A) and the means and SDs of the fatigue scores (B) before and after each of the 6 Reiki sessions. Table 2 displays the means and SDs for all ESAS symptoms before (pre) and after (post) each of the 6 Reiki sessions. Each symptom showed numerical improvement, but statistical testing was not done. Means and standard errors of the total ESAS score (A) and the fatigue score (B) before and after each of the six Reiki sessions Means and (Standard Deviations) for all ESAS Symptoms Before (Pre) and After (Post) Each Reiki Session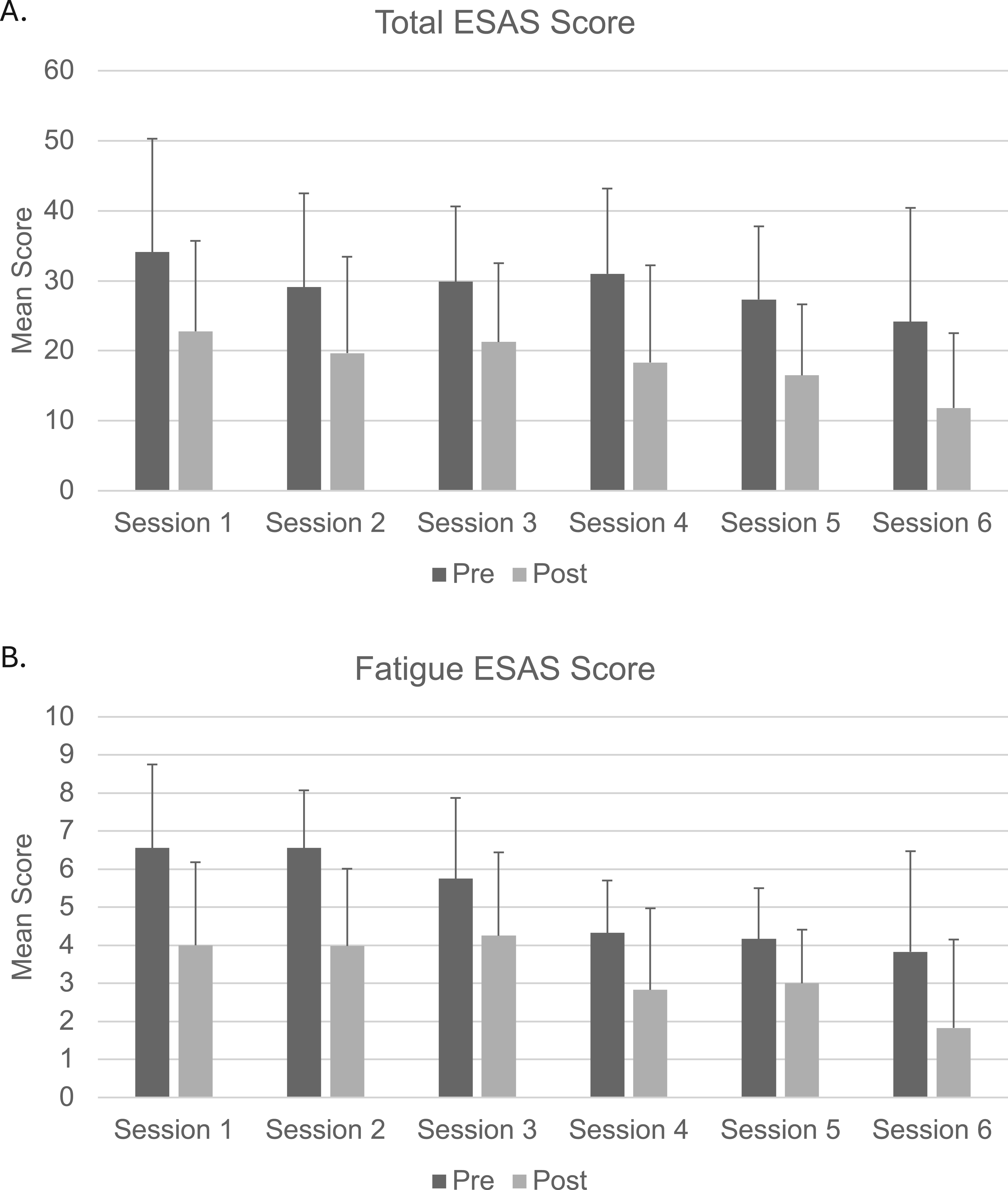
Means and Standard Deviations (SD) of Adjusted Mean T Scores and Change Scores (

Adverse Events
Two participants reported ESAS depression scores ≥7 or PROMIS depression t-scores ≥ 70 and their clinical care team was contacted. Study coordinator received an EHR notification that one participant was seen in the ED after being in a motor vehicle accident with complaints of neck pain. They remained in the study. These adverse events were deemed unrelated to receiving Reiki and there were no adverse events during the Reiki sessions.
Discussion
This feasibility study was the first evaluation of a standalone multi-week program of Reiki therapy for oncology outpatients. This study demonstrated that oncology patients could be recruited to participate in a Reiki intervention and complete outcome measures. While the retention rate was 67%, short of meeting the criteria of 70%, data completion was at 100%. Overall attendance was suitable (5.5/6 sessions) and 67% of patients met attendance criteria (4 out of 6 sessions). Overall, participants were satisfied with the Reiki intervention, indicating acceptability. Outcome measures, ESAS and PROMIS-29, were sensitive to change for every domain, indicating their appropriateness for this type of intervention.
Despite some of the successes of this evaluation, there are several areas for improvement needed before moving forward toward a fully powered randomized controlled trial. First, given that half of the tentatively eligible patients that did not enroll in the study were unreachable by phone, contacting patients through text or email, or medical message through the EHR might have resulted in a better recruitment. Second, the retention rate did not quite meet criteria (by 3%), therefore, following up with participants by contacting them to complete the outcome measures via phone and/or email and/or medical messaging in the EHR, or providing remuneration for completing the follow-up measures is recommended to increase retention. Third, there was a slight bottleneck in terms of scheduling the sessions, whereby there was only one day a week that the Reiki practitioner administered the sessions. More time available for the Reiki practitioner might have improved pace of recruitment.
Fourth, of the five men that were referred by the oncologist (SR) for study participation, two expressed not being interested, two did not respond when contacted, and one was ineligible on the ESAS. However, one study of men with prostate cancer succeeding in enrolling males for a study of Reiki or relaxation therapy (84% enrollment rate). 46 However, in that study, the Reiki was given when patients were already coming to the hospital that day for radiation therapy. Therefore, strategies to improve male enrollment will be incorporated into future studies of standalone Reiki therapy, including modifying the messaging around Reiki to include more clinical and scientific language and a brief discussion of its evidence base to increase buy-in. Fifth, participants often had variable times between their enrollment and being scheduled for Reiki, making the time between baseline and follow-up assessment for the PROMIS-29 measure different across participants. Therefore, completion of the PROMIS-29 measure right before their first Reiki session would be a more appropriate timepoint for future studies.
Although we were unable to test for statistically significant changes in outcome measures, we observed numerical improvements in all ESAS symptoms and PROMIS-29 domains following Reiki intervention. Participants had to have baseline levels of ≥ 4 for fatigue/tiredness (baseline M = 6.17, SD = 2.44) and at least two other symptoms on the ESAS to meet inclusion criteria. As mentioned previously, other studies have reported improvements in fatigue in oncology patients following Reiki therapy.30-35 Two of these studies used the ESAS32,34 but no study had used the PROMIS measure, making this a novel assessment for this population and intervention. Further, no study had tested Reiki therapy as part of an integrative oncology treatment plan for symptom management in outpatients.
In addition to fatigue, two other symptoms that were rated high were drowsiness (related to fatigue) and anxiety, both of which showed numeric improvement following Reiki. Anxiety is another symptom that has shown improvement following Reiki in patients with cancer31,32,36 and many other populations. 17 Despite no statistical testing, given that the ESAS and PROMIS were both sensitive to change in a positive direction following the Reiki intervention, we determine these measures to be appropriate for future studies.
As a pilot feasibility study, there were several limitations that require discussion. First, as is often the case with feasibility studies, no power calculation was performed and with the small sample size, we were not statistically powered to detect differences before and after the Reiki. Hence, no conclusions can be drawn regarding changes in the outcome measures and further research with a larger sample size is needed. Second, there was no control group, meaning we cannot determine the feasibility of including a passive or active control group or the randomization process itself until we conduct a future feasibility RCT. Further, in assessing numerical changes over time, we cannot account for nonspecific effects of the Reiki intervention such as the benefit of support and touch, or the Hawthorne effect, 47 or natural changes over time for those receiving the Reiki intervention. Additionally, controlling for expectancy effects will be explore in future studies that test effectiveness or efficacy.
Third, there were issues with pace of recruitment and scheduling that will require adjustments to subsequent studies, including greater time allocation for the Reiki practitioner and multiple means of patient recruitment, including self-referral and contacting interested patients via text and email as well. Fourth, as a single arm study there is a chance of selection bias, as participants self-selected into the Reiki intervention. Indeed, participants reported moderate to high levels of expectation for Reiki’s benefits, which could enhance placebo effects. However, a previous study reported that participants’ expectancy did not predict improvements in wellbeing following Reiki. 48 Future work with a larger sample will test whether expectancy influences symptom changes. Fifth, these results are not generalizable to other demographics outside of those commonly observed in integrative health studies, that is, White, middle aged, females.49,50
Conclusions
Overall, the study demonstrated that it was feasible and acceptable to conduct a Reiki intervention with oncology patients in an integrative oncology symptom management clinic. However, modifications are suggested before proceeding to a fully powered trial, including strategies to broaden recruitment and increase retention. The current study had a small sample size and was not powered to detect statistical significance. A highly preliminary assessment of outcome measures revealed numerical improvements in participants’ pain, drowsiness, fatigue/tiredness, nausea, appetite, shortness of breath, depression, anxiety, overall wellbeing, and total ESAS symptom score after each Reiki session. However, the observed sensitivity to change indicates that it is appropriate to use these outcome measures in a subsequent study. Future work will take the lessons learned during this feasibility study into the design and execution of a fully powered RCT to test efficacy.
Footnotes
Acknowledgments
We would like to thank study coordinators Hayley Sluka, BSN, RN; Kathryn DiFrancesco, BA, ACRP-CP; Katrina Godin, MS; and Jessica Surdam, MPH; and Sam Rodgers-Melnick, PhD for his study design recommendations.
Ethical Considerations
The study received approval from the University Hospitals Institutional Review Board (STUDY20240067, Case3Z24). All participants provided written informed consent prior to enrollment. Risks to participants were minimal, limited to potential discomfort during Reiki sessions or distress from symptom questionnaires. Participants were allowed to withdraw at any time without penalty. Confidentiality was maintained through secure data handling in REDCap, Velos, and OnCore systems. Safety protocols included alerting the clinical care team for any participant reporting ESAS depression scores ≥7 or PROMIS depression t-scores ≥ 70.
Consent to Participate
All participants provided written informed consent via the secure online data capture software REDCap.
Author Contributions
NLD assisted in study design, analyzed the data, and wrote the manuscript. SC and JC recruited participants, extracted EHR data, and wrote the manuscript. KF assisted in the study design, performed the Reiki intervention, collected outcome data, and edited the manuscript. SR assisted in the study design and recruitment and JAD in the study design. All authors reviewed, edited, and approved of the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was generously funded by the Elizabeth Severance Prentiss foundation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Trial Registration
NCT06354049.