
Abstract
The present article describes the prevalence and predictors of adverse mental health reactions in first responders, a population exposed to stress (rather than a population who are exposed). Mental health impairments in first responders exact considerable personal and public costs and are likely to negatively affect work performance, including providing care to trauma survivors. This article provides an update on first responders’ mental health and examines predictors of trauma-related psychopathology in this population. This information is of vital importance for the development and implementation of prevention and intervention strategies.
The present report describes the prevalence and predictors of adverse mental health reactions in first responders, a population who are exposed to stress, trauma, and adversity on a regular basis. First responder groups include rescue disaster workers, paramedics, medical personnel at accident and emergency departments, firefighters, military personnel, and others. As part of their job profiles, these groups fulfill different roles when attending to a critical incident. Paramedics and emergency medical personnel have to attend to the physical needs of injured victims of an event, whereas military personnel typically have to attend to issues of safety first. Common to all groups of first responders is that, following a traumatic event, they will be among the first present at trauma sites and often the very first to attend to the victims. A look at the literature, however, shows that the first responder group as a whole is much less studied than victims of the same events that they attend. Some first responder groups, such as military personnel, are better researched than others. Clearly, however, there is a larger body of literature on the mental health consequences of victims of traumatic events than of first responders. A recent search on MedLine using the keywords “trauma” and “victim” resulted in 969 hits, whereas a search on “trauma,” and “first responder” produced far fewer hits. Mental health impairments in first responders are associated with substantial personal and public costs and can adversely affect their service to victims and patients. This report provides an update on first responders’ mental health and reviews predictors of adverse mental health outcomes in this population. This information is of vital importance for the development and implementation of prevention and intervention strategies, which will be discussed in the final section of this article.
Adverse Mental Health Reactions in First Responders
First responders and disaster workers are routinely exposed to life-threatening and potentially traumatic situations, work with survivors and their families, and often recover the dead and injured. The most frequent trauma-related disorders are posttraumatic stress disorder (PTSD), major depressive disorder, and drug and alcohol-related disorders (e.g., Benedek, Fullerton, & Ursano, 2007; Breslau, Davis, Andreski, & Peterson, 1991; Fullerton, Ursano, & Wang, 2004; Kessler et al., 1995; Surtees et al., 1986).
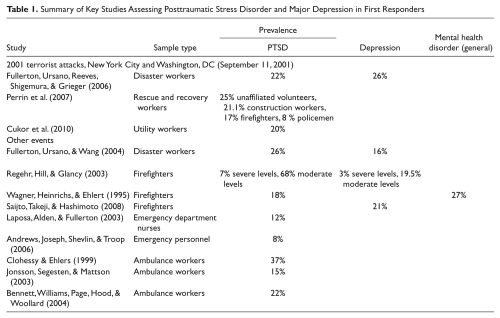
The terrorist attacks of September 11, 2001, are among the most recent and relevant traumatic events that affected an immense number of victims and first responders as well as many other populations. Disasters related to terrorism may have more severe mental health consequences compared to other large-scale disasters that do not involve the intentional perpetration of violence (North, 1995). Victims and first responders exposed to the latter are likely to experience a loss of one’s sense of safety and feelings of uncontrollability (Fullerton, Ursano, Reeves, Shigemura, & Grieger, 2006; Grieger, Fullerton, & Ursano, 2004; Silver, Holman, McIntosh, Poulin, & Gil-Rivas, 2002). A study conducted 2 weeks after the 9/11 terrorist attacks found PTSD scores above the cutoff for PTSD diagnosis and for depression, 22% and 26%, respectively, in a sample of disaster workers involved in responding to the attacks, including medical personnel, police, fire fighters, search and rescue, and other disaster-site workers (Fullerton et al., 2006). Another large-scale study including almost 30,000 rescue and recovery workers involved in rescue operations following 9/11 reported PTSD rates of 15% (Perrin et al., 2007). Interestingly, PTSD rates were highest among unaffiliated volunteers (25%), followed by construction workers (21.1%) and fire fighters (17%), suggesting that workers in occupations least likely to have had prior training in responding to disasters may be at greater PTSD risk. Considerably lower PTSD levels (8%) were found in policemen involved in the same event. Similarly, a group of canine search and human handler teams exposed to injured survivors or bodies after 9/11 also reported fairly low levels of psychological distress and few met criteria for a mental disorder (Alvarez & Hunt, 2005). Another recent study has been concerned with the mental health of utility workers, that is, nonrescue disaster relief workers who were deployed to the World Trade Center following the attacks (Cukor et al., 2010). Almost 20% of utility workers deployed to the site reported symptoms consistent with a PTSD diagnosis of full or subsyndromal PTSD. These rates of PTSD were comparable to those of professional first responders and rescue workers reported previously.
Studies conducted on populations of trauma-exposed disaster workers involved in events other than 9/11 paint a similar picture. These show heightened PTSD levels, as well as acute stress disorder, and increased health care utilization in disaster workers (Fullerton et al., 2004). More specifically, PTSD rates in a study of exposed disaster workers yielded rates of 26%, and of 17% at 7 and 13 months, respectively, postdisaster, whereas depression rates were at 16%, 7 and 13 months, respectively, postdisaster (Fullerton et al., 2004). Moreover, in this study, more of the exposed disaster workers, compared to nonexposed comparison participants, were seeking medical care for emotional problems following the event.
Firefighters are another group among whom PTSD levels have been reported to exist in the range of 11% to 32% (Fullerton, McCarroll, Ursano, & Wright, 1992; McCarroll, Fullerton, Ursano, & Hermsen, 1996; McFarlane, 2000; North et al., 2002; Ursano et al., 1995). An Australian study of firefighters reported 7% of firefighters with severe levels of PTSD symptom, with 68% indicating moderate-level PTSD symptoms. Three percent of the same sample participants had depression scores indicative of severe depression, and 19.5% suffered from moderate levels of depression (Regehr, Hill, & Glancy, 2000). In a sample of German firefighters, the PTSD rate was 18%, with 27% of this representative sample of recruited firefighters reporting at least one mental health disorder on the General Health Questionnaire (Wagner, Heinrichs, & Ehlert, 1995). A recent study from Japan reported 21% of depression in firefighters involved in firefighting, emergency services, and recue work related to various fire-related disasters, such as earthquakes, typhoons, or volcanic eruptions (Saijto, Takeji, & Hashimoto, 2008).
Finally, medical doctors and emergency personnel, specifically those working in accident and emergency settings, comprise another group of first responders frequently afflicted with mental health outcomes. Work-related stress and potentially traumatic events in the emergency department have previously been linked to depression and anxiety disorders, including PTSD. In a sample of emergency department nurses, for instance, Laposa, Alden, and Fullerton (2003) recorded the following most upsetting events: provision of care to a patient who is a relative or close friend and is dying or in serious condition, threatened physical assault of self, multiple trauma with massive bleeding or dismemberment, death of a child, providing care to a traumatized patient who resembles yourself or a family member in age or appearance, and caring for a severely burned patient. In their sample, 12% met full criteria for PTSD. Another study yielded a rate of 8% of current PTSD in a large sample of emergency personnel in the United Kingdom (Andrews, Joseph, Shevlin, & Troop, 2006).
Rates of mental health consequences may differ between emergency personnel serving as ambulance workers and those stationed in the actual emergency department, as work profiles differ and ambulance drivers may be closer to the actual trauma scene. Studies have indeed reported significant higher PTSD rates in on-the-scene rescue workers compared to in-hospital staff (e.g., Durham, McCammon, & Allison, 1985). In an earlier study involving ambulance workers, rates of PTSD prevalence have been reported to be up to 37% (Clohessy & Ehlers, 1999). Other studies documented considerably lower rate, such as a Swedish study involving ambulance workers, with 15% of the participants scoring above the cutoff for a probable PTSD diagnosis (Johnson, Segesten, & Mattson, 2003) and a similar study from the UK reporting PTSD prevalence of about 22% among its participants (Bennett, Williams, Page, Hood, & Woollard, 2004).
Table 1 presents an overview of rates of mental health consequences in groups of first responders. Taken together, prevalences of PTSD, depression, and other mental health problems in first responders range from 8% to 32% for PTSD, and somewhat lower reported depression prevalences, with the higher PTSD prevalence rates documented for those first responders who have not been specifically trained for disaster work (Dyregrov et al., 1996; Guo et al., 2004). Notably, these rates are considerably higher than those reported for national prevalence rates for the general population, which yield rates of 4% of PTSD, for instance, and 10% for depression in the US (Kessler et al., 2003, Kessler, Chin, Demler, Merikangas, & Walters, 2005).
Summary of Key Studies Assessing Posttraumatic Stress Disorder and Major Depression in First Responders
Predicting Adverse Mental Health Consequences and Resilience in First Responders
Why do some first responders develop psychiatric disorders whereas others appear to experience no lasting adverse mental health consequences? This section summarizes the literature for selected first responder groups. Candidate predictors can be divided into factors related to demographic background, pretrauma characteristics (e.g., prior mental illness, preexisting traits, pre- or post-trauma life events, perceived social support), characteristics relating to cognitive processing during the event itself, and aspects of postevent processing.
First, a number of independent factors have been shown to predict PTSD. With respect to demographic predictors, Fullerton and colleagues reported that younger and single responders were more likely to develop acute stress disorder after critical incidents (Fullerton et al., 2004). In police officers, Caucasian race, less previous trauma exposure, and less critical incident exposure during service were associated with lower PTSD symptoms prospectively (Liberman et al., 2002; Yuan et al., 2011). Predictors for PTSD in firefighters were prior psychiatric impairment, including symptoms of depression, psychosomatic complaints, substance abuse, and social dysfunction (Wagner, Heinrichs, & Ehlert, 1999). For New York City transit workers, who had experiences or witnessed a traumatic event prior to 9/11, depressive symptoms were significantly associated with witnessing September 11 tragedy (Tapp et al., 2005). Finally, Leck and colleagues (Leck, Difede, Patt, Giosan, & Szkodny, 2006) reported higher depression and PTSD scores following the 9/11 terrorist attacks in male disaster workers who had been exposed to childhood sexual abuse.
Experiences during the traumatic event were also significant risk factors for the development of mental health problems. Sustaining an injury, for instance, was the strongest risk factor for PTSD volunteers and other rescue and recovery workers involved in the World Trade Center disaster rescue (Perrin et al., 2007). The same study documented that evacuating from one of the towers, as well as dust cloud exposure, was a significant risk factor for PTSD, but in volunteer organizations only, highlighting once again that there are important differences among first responder subpopulations. Perceived safety during and after an adverse event has been shown to be lower in first responders with greater exposure, that is, those who worked in physical danger, or with dead bodies (Fullerton et al., 2006). Those who perceived less safety reported more symptoms of depression and peritraumatic dissociation, hence indicating that lowered perceptions of safety may have serious implications for work-related behavior and can affect long-term health and morale in first responders.
Other cognitive factors and beliefs during the trauma seem to play an important role. A greater sense of self-worth, beliefs of greater benevolence in the world, greater social support, and better social adjustment during academy training were all associated with lower PTSD symptoms prospectively (Yuan et al., 2011). In accord with these results, a recent study assessed the pretrauma tendency to catastrophize about negative events in firefighters, which was a risk factor for the development of PTSD symptoms later (Bryant & Guthrie, 2007).
Social support is among the most robust predictors for PTSD following different traumatic events (Brewin, Andrews, & Valentine, 2000; Ozer, Best, Lipsey, & Weiss, 2003). Studies have replicated the importance of social support as a protective factor against the development of PTSD in first responders, indicating that it may be a primary factor within the individual’s personal as well as organizational network, particularly when there is social support from superiors (Leffler & Dembert, 1998; Regehr et al., 2000; Weiss, Marmar, Metzler, & Ronfeldt, 1995). First responders who feel supported and valued may thus experience lower distress levels.
Finally, a number of work-related factors are thought to increase stress-related reactions following traumatic events and have been associated with depression or PTSD among first responders. Three sets of such factors have been shown to contribute to stress in emergency personnel: organizational characteristics, patient care, and the interpersonal environment. Prior studies have demonstrated that stress predisposes health care workers to clinical conditions, such as depression (e.g., Gallery, Whitely, Lonis, Anzinger, & Revicki, 1992; Revicki, Whitely, & Gallery, 1993). Relatively, shorter nap time was significantly related to depressive symptoms in firefighters, even after adjustment for a number of other variables, such as age, gender, job type, marital status, smoking, and others (Saijto et al., 2008). Longer job experience and number of stressful missions during the past month were also predictive of PTSD in firefighters (Wagner, Heinrichs, & Ehlert, 1999).
Interestingly, Marmar and colleagues tested several predictors of PTSD from the above candidate categories in a combined model and isolated five key variables that explained a considerable amount of PTSD variance in police officers: greater peritraumatic distress and dissociation, greater problem solving and coping, greater routine work, environment stress, and lower levels of social support (Marmar et al., 2007).
Implication for Prevention and Intervention Strategies in the First Responder Sector
Considering the prevalence of mental health consequences in first responders, developing prevention and intervention strategies is a vital objective. Yet there continues to be considerable controversy over which type of intervention should be offered at what time and to whom after exposure to traumatic events (Roberts, Kitchiner, Kenardy, & Bisson, 2009). Several experts (e.g., Bisson, Roberts, & Macho, 2003; Brewin, Scragg, Robertson, & Thompson, 2008) maintain that interventions should target those who are at highest risk of experiencing persistent psychological problems following exposure to potentially traumatic events. Consistent with this view are the data supporting the effectiveness of certain intensive treatments offered to trauma-exposed individuals in the general population who have been identified as high risk (e.g., people with acute stress disorder; Roberts, Kitchiner, Kenardy, & Bisson, 2010). In contrast, single and multisession early interventions directed at everybody exposed to trauma have been found to be relatively ineffective or even harmful (Roberts et al., 2009; Rose, Bisson, Churchill, & Wessely, 2002).
A number of implications for prevention and intervention strategies can be drawn from the results of the present review. Based on the predictor studies reviewed above, first responders identified as high risk groups due to risk factors such as a history of mental illness, being injured during rescue operations, or those who screen positive for symptoms of acute or posttraumatic stress disorder or other psychological disorders in the initial aftermath of the event would present important candidates for these interventions. Measuring postevent processing and appraisals may yield another set of target groups. For example, first responders who felt their own life was in danger during the event and that they had no control over it or those who catastrophize about negative events following a traumatic event may be particularly likely to benefit from short-term cognitive-behavioral interventions that help to modify maladaptive trauma-related appraisals and are adapted to the specific population.
Another approach would be to develop, test, and disseminate prevention programs. Such programs could promote resilience in first responders. However, in contrast to the extensive knowledge base of risk factors known to predict onset of PTSD, there are relatively limited empirical data on factors that may serve protective functions in this population, such as cancelling out the effects of certain risk factors or providing resources that independently lead to positive outcomes. Such information is vital for the development of evidence-based prevention programs targeted at first responders.
A number of prevention programs have been developed, many of which target factors that are generally thought to boost resilience rather than targeting specific risk factors in a given population. One example is the Battlemind program (Adler, Bliese, McGurk, Hoge, & Castro, 2009), a predeployment training program for soldiers. This program was designed to build soldier resiliency by developing self-confidence and mental toughness. The training focuses on general factors such as soldier strengths and aims to identify specific actions that soldiers and leaders can engage in to meet the challenges of combat. This study found that soldiers reporting high levels of combat exposure who participated in large group Battlemind training shortly after deployment exhibited lower levels of stigma and reported less posttraumatic stress at 4 months follow-up compared to soldiers who had received standard postdeployment stress education. Moreover, regardless of level of combat exposure, the intervention led to a decrease in depressive symptoms. However, the lack of a true control condition and the fact that training for the stress education comparison group was substantially shorter than training for the Battlemind intervention limit the conclusions one may draw from this study (Adler et al., 2009).
More specific trauma-informed, skill-based programs have been developed for families facing the impact of wartime deployments (Beardslee et al., 2011; Saltzman et al., 2011). However, most of these programs have not yet been formally evaluated and tested in randomized controlled trials. Moreover, programs for many of the above-reviewed first responder groups are still lacking. Well-designed research on risk factors, including multivariate longitudinal studies and randomized controlled trials of prevention programs that employ validated measures, will be crucial for developing a solid evidence base for designing future prevention programs with first responders.
Extant work on secondary trauma may provide an important theoretical framework for developing prevention and intervention programs for first responders. It has been proposed that the emotional impact of experiencing or witnessing traumatic events may be contagious in that those who treat trauma survivors may experience symptoms of secondary trauma (Figley, 1995) that are thought to be transmitted through the process of empathy (Pearlman & Mac Ian, 1995; Stamm, 1995). Several strategies at an organizational and individual level have been proposed to prevent or reduce the impact of vicarious trauma, such as changes in organizational culture, workload, group support, supervision, self-care, education, and modification of work environment (Bell, Kulkarni, & Dalton, 2003). The emphasis on organizational and systemic factors that may increase risk for secondary trauma among helpers in this literature contrasts with the almost exclusive focus on the individual that characterized early posttraumatic interventions implemented by psychologists (Hobfoll, Dunahoo, & Monnier, 1995) and that to some extent continues to pervade more recent interventions to promote resilience. Thus, the authors of a recent systematic review of psychosocial interventions designed to prevent stress-related symptoms and psychological disorders in law enforcement officers (Peñalba, McGuire, & Leite, 2008) noted that none of 10 randomized or quasi randomized controlled trials that qualified for inclusion targeted stressors related to the job context. The main intention of these psychosocial interventions was to improve police officers’ ability to cope with stressful events encountered at work. However, there is growing evidence that the conditions or circumstances within a specific organizational context may present a more potent source of occupational stress within the police force than the job content (Burke, 2000; Collins & Gibbs, 2003; Kirkcaldy, Cooper, & Ruffalo, 1995). This research suggests that organizational characteristics need to be addressed when tailoring prevention programs to specific first responder populations.
Systematic study of the preventative impact of these programs on first responders using longitudinal prospective design has the potential to greatly advance our understanding of risk and resilience in first responders and other populations working with trauma survivors. For example, literature on prevention of vicarious trauma emphasizes the importance of repeated assessment of individual vulnerability factors in tandem with organizational structures that emphasize continuous self-care and supervision as a crucial preventative measure. If implemented and formally measured on an ongoing basis, such interventions are likely to be superior to “one-fits-all” resilience interventions that are administered at a specific point in time. In addition, emphasis on ongoing assessment may provide a check on maladaptive perceptions of psychological risks associated with exposure to high-stress situations. For example, some people might overestimate their own coping ability or underestimate the level of distress they might experience in response to potentially traumatic events such as viewing mutilated bodies of children at an accident site. Discrepancies between perceptions of risk and coping ability may be particularly pronounced among volunteers receiving less extensive professional screening and preparation than professional first responders.
A key objective is to critically test novel prevention and intervention programs. Methodologically, Ehlers and Clark (see also Agorastos, Marmar, & Otte, 2011) made several recommendations for conducting RCTs on early intervention. These included the need to include a no-intervention control condition given the expectation that most trauma survivors appear to recover on their own and findings that recovery rates observed in different studies may depend on the selection criteria used to recruit participants. Another recommendation was the incorporation of follow-up assessments that would help identify potential negative effects of the intervention in the long term. Finally, they called for the importance of monitoring dropouts more closely given high attrition rates in early intervention studies (Ehlers & Clark, 2003).
Taken together, there are some serious limitations to translating the above-reviewed mental health prevalences and predictor findings into practice. First and foremost, predictors appear to be rather heterogeneous and sometimes inconsistent across studies. Subgroups within first responder populations, that is, trainee first responders versus volunteers, may display different pathways to psychopathology and were characterized by different predictors in one study (Perrin et al., 2006). Some studies have reported effects of exposure types, and these events may indeed differ between responder groups, that is, emergency medical setting versus firefighters.
It is important to note that information on predictor variables can be used in different ways. That is, sex, for instance, is a strong predictor for PTSD, but it can only be used to screen for potentially vulnerable individuals. Other variables, such as cognitive or emotional processing during the event, can be modified following trauma exposure and often after PTSD symptoms are present. However, prevention strategies could set out to train individuals in certain ways of responding to adversity. Moreover, other characteristics, for instance job-related characteristics, could be modified to change the situation and make the development of PTSD less likely. Disaster preparedness training and shift rotations to enable a shorter duration of service at the site may reduce PTSD among workers and volunteers in future disasters. Several studies highlighted higher PTSD prevalence in less trained first responder populations, such as untrained volunteers (e.g., Perrin et al., 2008). These results call for a better and specific training in these subgroups.
Conclusion
Results from the present review suggest that a considerable minority of first responders who respond to various events and disasters experience substantial psychological distress following such events, such as PTSD or depression. Longitudinal, well-designed research on risk and resilience factors and their relationship to mental health outcomes in first responders is needed to inform the development of prevention and intervention programs for this diverse population. Our review highlights the need for targeted prevention and intervention strategies that take into account heterogeneity in job profile and background characteristics of first responders to reduce the psychological burden associated with participation in rescue operations. We have highlighted current shortcomings as well as avenues and potential barriers to the development and dissemination of such efforts.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article from a Swiss National Science grant (Ambizione) to Birgit Kleim.