
Abstract
Few studies describe the training of student therapists in prolonged exposure (PE), an evidence-based psychotherapeutic approach to the treatment of trauma. Using a case study, this article describes training and supervision of a master-level graduate student in the implementation of PE with a research participant who had depression and posttraumatic stress disorder (PTSD) due to traumatic stress exposure. The participant’s symptom severity of depression and PTSD decreased from pretreatment to posttreatment, and symptom gains were maintained at the 3-month follow-up assessment. Implications for the training and supervision of students in the mental health professions are discussed.
Research indicates that many therapists who treat traumatized individuals are not readily inclined to adopt empirically supported treatments (ESTs), including prolonged exposure (PE) therapy, a trauma focused therapy with a strong evidence base (Cahill, Foa, Hembree, Marshall, & Nacash, 2006; Cook, Schnurr, & Foa, 2004). Moreover, few studies have investigated whether therapist trainees may be suitable to learn and effectively treat traumatized individuals with PE. This is particularly important considering students often embrace the techniques taught to them during their clinical training and incorporate those techniques in future clinical practice (Seligman, 1998). The process by which therapist trainees learn and apply PE remains unclear. Moreover, research that describes the training and supervision of therapist trainees in implementation of PE is lacking. Using a case study, the purpose of this article is to illustrate the training, supervision, and learning of a therapist trainee who implemented PE with a client who had a history of multiple traumas.
In 2000, Foa, Keane, and Friedman published guidelines summarizing state of the art treatment of posttraumatic stress disorder (PTSD) and other traumatic stress reactions with the purpose of informing mental health clinicians about recommended care of traumatized individuals. Based on a review of both clinical and research findings, the guidelines indicated that PE was a treatment of choice for PTSD. PE includes both imaginal and in vivo confrontation with traumatic memories and situations that serve as trauma reminders and are often avoided (Cook et al., 2004). PE consists of four major components: (a) education about the nature of trauma and trauma reactions; (b) controlled breathing training; (c) imaginal exposure (IE) to the traumatic event; and (d) in vivo exposure to trauma reminders that have been avoided (Foa & Rothbaum, 1998).
To date, there is little evidence indicating that therapist trainees use PE (Becker, Zayfert, & Anderson, 2004; Fontana, Rosenheck, Spencer, & Gray, 2002; Rosen et al., 2004). Much has been written about the barriers to using best practice guidelines, and some explanations include negative attitudes that providers have toward evidence-based practice (EBP) and “manualized” treatments; lack of acceptability of the treatment to providers; inadequate time or financial support provided for initial training; inadequate infrastructure (supervision, consultation, money to adapt materials, etc.) to support adaptation of EBP for community settings or complexity of cases (Aarons & Palinkas, 2007; Glasgow, Lichtenstein, & Marcus, 2003; Schoenwald & Hoagwood, 2001).
Some research suggests that inadequate training is the single largest factor associated with failure to use PE (Becker et al., 2004; Cahill et al., 2006). However, few studies describe the training needed for master-level graduate student clinicians, also called therapist trainees, to effectively use the recommendations of the guidelines. Moreover, to our knowledge, no study to date has described the training and supervision of a therapist trainee in the implementation of PE. This is particularly important considering master-level mental health professionals often have the most regular mental health client contact compared with other mental health professionals (Ruby, 2004). Moreover, master-level mental health professionals are often core mental health providers in both rural and urban areas (Morris, 2009). Consequently, there is good cause to believe that master-level graduate students are often the future community practitioners treating trauma and PTSD in individuals who seek assistance for traumatic stress. Successful efforts at bridging the gap between research on PE for PTSD and its utilization in real-world practice requires studies specifying the teaching and supervision of PE to this group of therapist trainees.
A pilot study was conducted to test the effectiveness of PE versus present centered therapy (PCT) in clientele presenting to an urban community mental health center staffed by master-level graduate students. The full results of this study have not yet been reported, and the current study reports on the first client in the study who was randomized to the PE condition. The current report focuses on the work of the first therapist trainee who conducted PE with a client and describes the teaching, case description, therapeutic outcome, and reflections of the therapist trainee.
A Model for Teaching PE
The proposed model of training clinicians in PE takes into account recommendations set forth by Cook and colleagues (2004) and Cahill and colleagues (2006). The supervisor in this study had received training and supervision in PE by experts in PE. The supervisor trained three master-level graduate students who were research assistants in an IRB-approved treatment study. The therapist trainees who received training in PE had the following characteristics: completion of at least 1 year of coursework toward their master’s degree in counseling, marriage and family therapy (MFT) emphasis; completion of a course in psychological trauma treatment; interest in psychological trauma treatment.
The therapist trainees were trained using a structured approach. First, the supervisor had the therapist trainees read a PE training manual based on the training manual from Foa, Hembree, and Rothbaum (2007). Next, concepts in the training manual were discussed in three 2-hour training sessions. The following concepts were discussed: questions and concerns regarding the treatment manual; the rationale for PE; education regarding what to expect before, during, and after PE; specific education regarding how to implement both IE and in vivo exposure. After reading the treatment manual and completion of three initial training sessions, the therapist trainees were required to observe the supervisor implement 10 sessions of PE with a client weekly for 90-minute sessions for a total of 10 weeks. This was the length of time for treatment according to the research protocol. In this manner, the therapist trainees could see the entire process of therapy demonstrated to them by a senior clinician experienced in the implementation of PE. This method of training is based on recommendations from previous research, which has indicated demonstrations are often more helpful than both lectures and role-plays in the training of PE (Amsel, Neria, Suh, & Marshall, 2005; Cahill et al., 2006).
Therapy was conducted in a university-based community clinic, which is ideal for translation of PE to community clinical practice in several ways. The clinic was set up like a community agency and received referrals from the community at large. The university-based community clinic had therapy rooms with two-way mirrors, which allowed the therapist trainees to easily observe and listen to the supervisor demonstrate PE with an actual client. Over the course of the 10-week demonstration and immediately after the completion of each 90-minute therapy session, the supervisor met with the therapist trainees for supervision. Supervision consisted of a thorough review of the contents of the observed therapy session and an opportunity to ask and answer questions. After observing the supervisor conduct PE for an entire 10-week process with at least one research client, attendance at all training and supervision sessions, and adequate demonstration of knowledge about PE (based on familiarity with the treatment manual), the therapist trainees were considered ready to begin PE with their own client.
The next part of training included direct observation of the therapist trainees by the supervisor. Using a two-way mirror, the supervisor observed the therapist trainees conduct PE for each 90-minute therapy session during the 10 weeks of treatment to ensure adherence to the treatment manual and provide them live supervision. In addition, the therapist trainees received 1 hour of individual supervision per week. The supervision sessions focused on treatment integrity, adherence to the treatment manual, specific issues related to implementation of PE with the clients, client issues, therapist concerns, and other questions and concerns as appropriate.
Method
Participant
The participant was a 75-year-old woman referred to treatment by her daughter who was concerned about the participant’s emotional health following a recent life-threatening accident. As is typical for referrals to the university-based community clinic, the participant went through an intake evaluation to understand her symptoms and needs in regard to therapy. During the intake the participant revealed a history of multiple traumas that she had experienced throughout her life. These included witnessing and experiencing domestic violence (DV) as a child, which she reported as the most distressing trauma; witnessing and experiencing her mother become sick and die from cancer when she was a teenager; losing her younger sister to suicide, living through a civil war in her early 20s where her life was threatened as a result of constant bombings and nearby shootings; observing her husband get sick and die from cancer; and her most recent trauma, a life-threatening accident.
Procedure
The participant initially completed a phone screening to determine if she met inclusion and exclusion criteria for the treatment study. Inclusion criteria included English speaking; above 18 years of age; experienced, witnessed, or were confronted with any lifetime traumatic event that involved actual or threatened death or serious injury or threat to the physical integrity of others to which the individual responded with intense fear, helplessness, or horror (Diagnostic and Statistical Manual of Mental Disorders-IV [DSM-IV] Criterion A1 and A2 of PTSD; American Psychiatric Association [APA], 1994). Exclusion criteria included suicidal or homicidal ideation for at least 1 year prior to the screening interview; substance abuse or dependence in the 1 year prior to the screening interview; psychosis; or personality disorder diagnosis. The participant was deemed eligible for the study by meeting inclusion and exclusion criteria and was provided information about the treatment study.
After informed consent was obtained, the therapist trainee conducted a pretreatment intake evaluation, and the supervisor reviewed this evaluation. Based on a review of the presenting issues and clinical history, it was determined that the participant met DSM-IV criteria for PTSD and major depressive disorder (MDD). Although the participant identified experiencing a life-threatening accident a few months prior to the intake interview, she identified the DV that she witnessed and experienced during childhood as her index trauma. Specific symptoms related to the index trauma included flashbacks of the event; nightmares about the event; intense distress when confronted with information about others who have experienced DV; avoidance of discussions about her childhood with her brother; avoidance of television shows that include references to DV; feeling detached from others, particularly her family; difficulty falling asleep; irritability; difficulty concentrating; and hypervigilence. In addition, the participant reported symptoms related to a major depressive disorder including depressed mood and loss of interest in previously pleasurable activities for at least 1 month prior to the intake evaluation; insomnia; loss of energy; feeling guilty about being a burden on her daughter; and diminished ability to concentrate. The participant reported that her symptoms began after her most recent trauma, her life-threatening accident. The therapist trainee completed the initial pretreatment evaluation and her two subsequent evaluations (i.e., post 10 sessions of PE and at 3-month follow-up after completion of PE) using the instruments listed below. The participant received therapy sessions at no cost for her participation in the research study.
Clinical Measurement Instruments
The PTSD Checklist–Civilian version (PCL-C; Weathers, Litz, Herman, Huska, & Keane, 1993) is a 17-item self-report PTSD symptom scale. Respondents rated the extent they were bothered by each symptom (1 = not at all to 5 = extremely). Items were summed to yield a total score that serves as a measure of PTSD symptom severity.
The Brief Symptom Inventory-18 (BSI-18; Derogatis, 1992) is a self-report measure of psychological distress. Respondents reported how much each symptom or problem bothered them during the past 2 weeks (0 = not at all to 4 = extremely). The BSI–Depression subscale score was computed by taking the average of the responses to the individual symptoms. Raw scores were converted to T-scores using normative data from community samples.
The Generalized Anxiety Disorder-7 (GAD-7; Spitzer, Kroenke, Williams, & Löwe, 2006) is a 7-item screening measure of GAD (0 = not at all to 3 = nearly every day). Items were summed to yield a total score that serves as a measure of GAD symptom severity.
Treatment
According to the research protocol, treatment was delivered in ten 90-minute individual sessions conducted once weekly over 10 weeks. Session 1 focused on establishing the therapeutic alliance, completing the trauma interview (which identified the various traumas the client experienced throughout her life), discussing the overall rationale for PE, discussing common reactions to trauma, and breathing retraining. Breathing retraining was assigned for homework after Session 1.
Session 2 focused on identification of the index trauma, which was defined as the most distressing trauma memory, use of the subjective unit of distress (SUDS) scale to gauge the level of anxiety the client feels, and construction of the in vivo hierarchy. The participant identified the DV, specifically the physical and emotional abuse that she, her mother, and her siblings experienced by her father, as the index trauma during the trauma interview. She reported not being able to save her mother from the abuse, her illness, and death as associated with the DV. The participant expressed some difficulty separating the DV from observing her mother’s sickness and death due to cancer, as she believed that the DV caused her mother to get cancer and die. The DV was chosen as the focus of IE in accordance with recommendations from the PE manual developed by Foa et al. (2007).
The participant was provided education about PE including what to expect during both IE and in vivo exposure. The participant was informed that the trauma she identified as being most distressing would be the focus of IE and that she would be asked to recount the memory of her experience with DV. The participant was also provided information and education regarding the therapeutic environment as a safe place to recount the memory. The therapist addressed concerns regarding treatment at the end of each session and checked in with the participant as a means of facilitating communication regards concerns about treatment. Breathing retraining was also assigned as homework for Session 2.
Session 3 was devoted to the collaborative development of the in vivo hierarchy. SUDS ratings ranging from 0 to 10 were elicited from the participant for each avoided and anxiety-provoking event, with 0 being no anxiety, and 10 being the highest level of anxiety. The participant reported that she avoided watching the news on television (SUDS = 8), particularly if there was a story involving DV. She stated she avoided reading the newspaper for similar reasons (SUDS = 7). The participant also reported that she avoided speaking about her childhood and specifically her father (SUDS = 10). The participant was given homework to engage in reading the newspaper, an activity she had been avoiding. Beginning in this session and continuing to the end of treatment, the participant was instructed to rate her SUDS before, during, and after she finished the in vivo exposure homework.
The client engaged in IE focused on the index trauma during Sessions 4 through 9. Each 90-minute treatment session was divided as follows: presentation of the agenda for the session, review of homework, IE, processing the memory, assignment of homework for the following week. Homework consisted of listening to tapes of her IE, engaging in vivo exposure, breathing exercises, and completion of SUDS scale before, during, and after the exposures.
During Session 6, continued IE to the memory of the participant’s DV was planned; however, the client’s presentation of a crisis called for the therapist to focus on the crisis. The participant stated that she experienced a great deal of distress during the week due to the anniversary of her husband’s death that was approaching. Given that her husband’s cancer and death was reported as one of her traumas during the trauma interview, the therapist trainee judged it was appropriate to allow the participant to process her thoughts and memories in regard to her husband’s death and the upcoming anniversary of his death. Although SUDS ratings were not obtained, the participant engaged in IE regarding this memory as she was prompted to recount and relive her most distressing memory in relation to her husband’s illness and death. The session served as both a crisis intervention and an IE exercise. The participant ended the session by expressing that she felt good about having been given the chance to talk about her husband, and she felt at ease and better prepared for the anniversary of his death. The participant’s next item on the in vivo hierarchy, watching the news on television without changing the channel, was discussed and assigned for homework. In addition, the client was instructed to listen to the tape from the session for homework. Supervision following this session included how the therapist trainee deviated from the PE manual and protocol.
Beginning in Session 7, the participant collaboratively agreed to focus on the most currently distressing part of her index trauma, also called the hot spot (Foa et al., 2007). The participant recalled and relived the DV, and the memories of the DV were closely intertwined with memories of the illness and death of participant’s mother. The participant described details associated with witnessing her father’s abuse toward her mother, including during her illness and the last day of her life. Although the initial SUDS ratings for this memory were a “10,” following exposure to the memories, the participant’s SUDS dropped to a “2” as she expressed feeling similar to the feeling after a storm has passed. During the processing, the participant stated that she realized having bottled all of these thoughts and emotions for as long as she had, she did not allow herself the opportunity to process and deal with the lingering emotions associated with the impact of the DV and losing her mother, the only person she felt safe with. The participant also discussed attempting the last item on her in vivo hierarchy, having a discussion with her younger brother about their childhood, which was a subject that she had avoided for over 60 years.
Session 9 continued with exposure to the most distressing part of the DV; however, due to the participant’s strong desire to share her newfound insight with the therapist, the traditional structure of PE was compromised. The participant revealed having had an enlightening and life-altering experience in a dream prior to Session 9. She reported that in her dream she had returned to South America to her childhood home for the first time since her mother’s death. She stated that during the visit, she was able to walk around the house. The client reminisced about some of her memories in the house, particularly the abuse her family experienced, including her mother’s illness and death, without any feelings of anxiety or distress. She then walked out of the house, closed and locked the doors, and walked away with a feeling of relief and lightness, as if a heavy load was just lifted off of her shoulders. The participant reported waking up from the dream with a similar feeling. She expressed that for the first time she was able to feel a sense of relief by having finally accepted the traumatic events of her childhood. The rest of session nine focused on processing her acceptance. No SUDS rating was obtained during Session 9, partially due to the participant’s desire to process with the therapist trainee immediately on entering therapy and partially because the therapist trainee did not interrupt the client to gather the SUDS level. The participant was given the audiotape of the session to listen to for homework. The deviation from the PE manual and protocol were discussed during supervision.
Session 10, the termination session, included a review of homework, discussion of the agenda for the session, IE, a review of progress, and saying goodbye. The participant continued IE focused on the traumatic memory identified in previous sessions. The therapist and participant reviewed the participant’s progress since the first session, discussed the coping skills developed, discussed applications to real life, and discussed relapse prevention. No SUDS rating was obtained during Session 10.
Results
The participant’s symptom severity decreased from pretreatment to posttreatment on measure of depression, PTSD, and GAD (see Table 1). These treatment gains were maintained through the final assessment, conducted at 3-month posttreatment. The participant’s scores on the PCL-C, decreased from 58 at pretreatment, to 28 at posttreatment, and finally to 25 at 3-month follow-up. As a positive screen for PTSD is a PCL-C score of 50 or more (Hoge et al., 2004), this participant no longer met screen positive criteria for PTSD immediately after treatment or at 3-month follow-up. Her BSI–Depression subscale T-score also decreased from 70 at pretreatment to 45 at posttreatment, and it stayed at 45 at 3-month follow-up. BSI T-scores of 63 or greater are indicative of clinical “caseness” (Derogatis, 1992; Zabora et al., 2001); therefore, the participant no longer met caseness criteria for depression at posttreatment or at 3-month follow-up. The participant’s score on the GAD-7 decreased from 8 at pretreatment (a positive screen for GAD is 10 or higher [Spitzer et al., 2006]) to 2 at posttreatment, and then it increased to 6 at follow-up. The participant did not meet positive screen criteria for GAD at any time point. The participant’s SUDS ratings during the in-session IE exercises indicated a decrease in peak SUDS ratings after each IE exercise (see Figure 1). This reflected decreased anxiety and habituation over time with PE.
Change in Symptom Severity of Depression, PTSD, and GAD From Pretreatment to Posttreatment to 3-Month Follow-Up
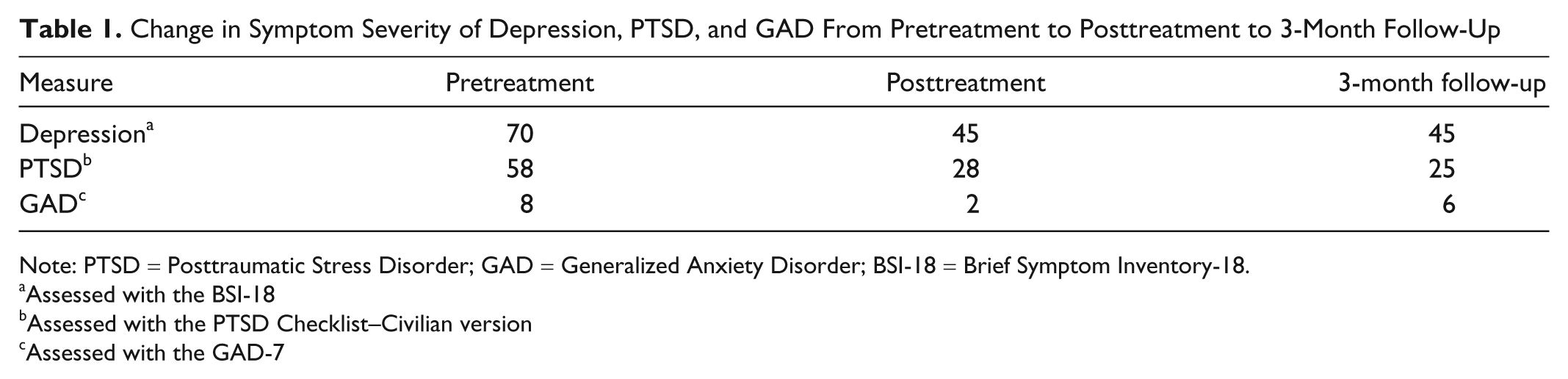
Note: PTSD = Posttraumatic Stress Disorder; GAD = Generalized Anxiety Disorder; BSI-18 = Brief Symptom Inventory-18.
Assessed with the BSI-18
Assessed with the PTSD Checklist–Civilian version
Assessed with the GAD-7
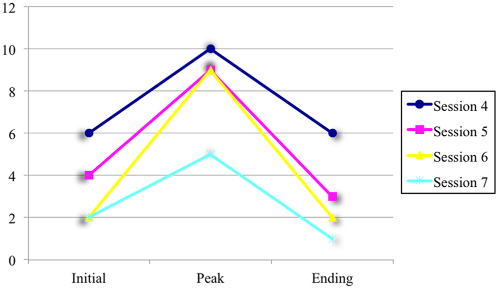
SUDS ratings during imaginal exposure exercises
Discussion
PE treatment by a master-level therapist trainee resulted in a substantial drop in self-reported symptoms of PTSD and depression at posttreatment and 3-month follow-up. The preliminary results from this case study are encouraging and warrant further investigation of training master-level graduate students pursuing careers in mental health, including graduate students in social work, psychology, and counseling, in the implementation of PE.
The participant in our case study demonstrated high engagement and habituation over time. In accordance with past studies, the combination of high engagement and habituation over the course of treatment was associated with a successful treatment outcome (Jaycox, Foa, & Morral, 1998). The participant learned that remembering and recounting her trauma memories were not dangerous and that her anxiety, which she carried for nearly 60 years, decreased.
The presented teaching model and case study provide an example of a method to disseminate PE to therapist trainees who express an interest in learning and using this EST. The model of training and supervision was based on direct recommendations from experts in the trauma field. For example, the treatment manual developed by Foa and colleagues (2007) was used as the foundation for training. The supervisor’s approach in supervision was affirming and bidirectional instead of hierarchical. It has been suggested that this method of supervision may assist in bridging the research practice gap (Addis, 2002), and it seemed true for this case. The supervisor addressed concerns about how to implement both in vivo and IE from the manual by live demonstration and open dialogue with the therapist trainee. This method allowed the therapist trainee to understand how the manualized intervention could be translated for clinical use in a community clinic setting. This supervision approach was particularly helpful when the therapist trainee deviated from the PE protocol. When this occurred, it was discussed in supervision, and the therapist trainees learned that deviations from the PE protocol were inappropriate, particularly for new, inexperienced therapists. Another important outcome of this case was the positive attitude of the therapist trainee after directly experiencing the positive results of the PE intervention. This is evident in the following clinical reflection by the therapist trainee in this case:
As an MFT trainee, I had limited knowledge and experience with PE. Given what I knew about the structure of Exposure Therapy (ET), and its tendency to bring clients to an extremely high-distressful state, I began the program with some hesitations regarding my competency to conduct this type of therapy. My hesitations were turned into insecurities following the intake session with the participant, as I was overwhelmed with the numerous traumatic experiences the participant presented with. I was immediately unsure which trauma to focus on, how to determine which was most important, and how to help her process all of these memories in a short 10-week psychotherapy program. However, with the constant supervision, assistance, and guidance of my supervisor, I was able to break it all down, and move forward one session at a time. Having now conducted PE with several other clients, there is one aspect I have found to be key to conducting successful PE. Given the high levels of distress the clients will likely face during the fist few exposure exercises, or even as early on as the trauma interview for some, it is absolutely crucial to discuss in great length the nature and rationale for PE. Clients must be warned about not only the high levels of distress they may experience during a session but also the distress they are likely to feel after the sessions. It must be explained that this is a normal, and even necessary part of therapy, and that they should not be alarmed or discouraged, as the high levels of distress are likely to reduce over time as they continue the program. With this participant, in particular, I found it useful to compare this process to the physical therapy she was receiving at the time for her injuries. I explained to her that the process is similar to physical therapy in that the initial sessions can be extremely painful and uncomfortable, and leave you going home feeling worse and in more pain than prior to the session. However, the pain is a necessary part of strengthening your muscles. Once you continue the sessions, and continue doing the exercises at home, your muscles will gradually build the strength necessary to complete the same exercises without any pain whatsoever. Similarly, in this program the “emotional muscles” need to be strengthened, and though sore and painful at first, they will end up much stronger and capable of handling bigger and more difficult obstacles. This example was helpful for the participant, as on numerous occasions throughout the therapeutic process, she was able to refer back to the example and remind herself that she is working on her “emotional muscles.”
There are numerous limitations to the generalizability of this teaching and training model as well as the results obtained in this case study. The teaching model may be labor intensive on the part of the supervisor, which may not be appropriate in some training settings. The therapist trainee made modifications to the PE protocol with this case study, such as not gathering SUDS ratings in Sessions 6, 9, and 10, attending to a crisis situation in Session 6, and taking a longer time to complete the trauma interview than is suggested in the training manual by Foa and colleagues (2007). In addition, the participant was only assessed at three time points and not after every other session. As this was the first case randomized to PE in the research project, all of the deviations in the protocol were discussed during supervision sessions so that the therapist trainees could learn to use the manual effectively. These modifications did not seem to negatively affect the treatment outcome as was evidenced by the drop in BSI and PCL-C scores at posttreatment and follow-up. Future research should further assess the relative impact of modifications to the treatment manual protocol.
Summary and Conclusions
In conclusion, specific recommendations for training graduate students in the mental health professions in PE for traumatic distress include: make strong efforts to provide supervised clinical experience for treatments that have been empirically validated; make treatment manuals available to graduate students; and provide ongoing consultation and supervision to graduate students as they learn how to implement PE. Although the limitations of a case study are numerous, the results of this report are promising as they indicate that background and level of experience of the clinician may not be crucial factors when deciding who may benefit from training in PE. However, further research is needed to determine the exact role of the clinician’s level of experience in relation to PE outcomes. This case study may suggest that clinicians with little experience are capable of successfully conducting PE when provided with appropriate training and supervision. We consider it a positive finding for clients, practitioners, and clinical researchers that relatively inexperienced graduate students can learn efficient treatment quickly and effectively when given appropriate supervision. Future research may investigate whether these results are replicable in other university clinics.
There is a clear need for more clinicians to be trained in PE for trauma related distress, particularly clinicians who will be working with trauma survivors in community-based settings. Given that master-level clinicians are often at the forefront of providing mental health services to the community, efforts should be made to improve training and supervision of this group of clinicians. Although the dissemination model presented may seem labor intensive on the part of the supervisor, it is important to note that university supervisors, particularly those who teach practica and fieldwork courses, routinely provide extensive training and supervision to students as part of their role in graduate student clinical training. Universities may be an ideal setting to provide the intensive training and ongoing supervision necessary to effectively learn PE, and future research should investigate the merit of providing training and supervision in PE as part of an overall graduate-level clinical training program. One promising aspect of the training model in this study is that it assisted the graduate student clinician to develop both the skills and confidence necessary to promote continued use of PE. Additional research is necessary to clarify whether therapist trainees are an appropriate group to train in PE.
Footnotes
Acknowledgements
The authors acknowledge the assistance of Dr. Kristin Powers and staff, Chelsea Edgecumbe, and Brian Dunphey.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a California State University, Long Beach Mini-Grant.