
Abstract
Typhoid fever (Salmonella Typhi) has declined dramatically in Korea over three decades, but residual seasonality, demographic patterns and provincial spatial concentration have not been systematically reanalysed. Using all 3535 typhoid cases reported to the Korea Disease Control and Prevention Agency between 2001 and 2024 (3051 domestic and 484 imported [13.7%]), we quantified the long-term annual trend with the Hamed–Rao modified Mann–Kendall test (τ = −0.667, p = 0.0011) and a negative-binomial generalized linear model (GLM) yielding a Sen slope of −7.3%/year (95% CI −9.9 to −4.4); a parametric-bootstrap analysis of the runner-up 1-breakpoint GLM identified 2018 as the most likely structural change point (95% CI [2009, 2022]). A continuous Morlet wavelet transform of the weekly series revealed annual periodicity that exceeded a 1000-simulation AR(1) red-noise null by a factor of 2.60. Direct age standardization and age-band-specific Mann–Kendall tests showed statistically significant declines in every age stratum. Provincial spatial analysis (16 sido) gave a global Moran’s I of 0.403 (p = 0.0083, 9999 permutations) under a Queen + k-nearest-neighbor-2 baseline scheme, with the southeastern coastal cluster (Gyeongnam–Busan–Ulsan–Gyeongbuk axis) preserved across 12 alternative weighting schemes after empirical Bayes shrinkage of sigungu-level rates and across two equal-length time strata; one province (Ulsan) survived Benjamini–Hochberg FDR adjustment of the 16 LISA p-values. Korean typhoid has continued its long-term decline; residual incidence concentrates in the southeastern coastal corridor, and imported cases—including ciprofloxacin-resistant H58 strains from South Asia—now form a substantial fraction of notifications, motivating pre-travel counseling and post-travel vigilance.
Keywords
Introduction
Typhoid fever, caused by the human-restricted bacterium Salmonella enterica serovar Typhi, remains a leading cause of febrile illness in low- and middle-income countries with inadequate sanitation (Crump et al., 2015; GBD 2019 Diseases and Injuries Collaborators, 2020; Mogasale et al., 2014; Wain et al., 2015). The Republic of Korea experienced steep declines in typhoid incidence between the 1960s and the 2000s following the expansion of piped-water and sewerage systems, dietary change, and access to antimicrobial therapy. Typhoid fever has been a Class-2 notifiable disease in Korea since the 1950s (Kim et al., 2019; Korea Disease Control and Prevention Agency [KDCA], 2024); case counts have fallen from thousands per year before 1985 to under 200 per year since 2005 (Kim et al., 2019; Yoo et al., 2009; KDCA, 2024).
Despite this domestic decline, two contemporary public-health concerns motivate continued surveillance. First, the importation of antimicrobial-resistant lineages—particularly the H58 multidrug-resistant haplotype that has emerged in South Asia, the Middle East and Africa over the past two decades (Britto et al., 2018; da Silva et al., 2022; Wong et al., 2015)—risks introducing strains less responsive to first-line antimicrobial therapy, including extensively drug-resistant (XDR) clones now reported in outbreak settings (Klemm et al., 2018; Yousafzai et al., 2021). The first Korean confirmation of H58 ciprofloxacin-resistant Salmonella Typhi from travelers, returning from India was reported in 2021 (Shin et al., 2021). Second, the residual case distribution within Korea may concentrate in geographic settings where unique exposure pathways (coastal seafood handling, untreated water (Gauld et al., 2020; Connor and Schwartz, 2005), contact with chronic carriers (Carey et al., 2020; Date et al., 2016; Mogasale et al., 2016)) persist, motivating targeted surveillance and preventive intervention.
We re-examined the complete 24-year nationwide typhoid fever surveillance series (2001–2024) to (i) quantify the long-term trend in incidence by Hamed-Rao Mann-Kendall (Hamed and Rao, 1998) and negative-binomial regression with rank-based Sen slope (Sen, 1968) confidence intervals; (ii) test for annual periodicity using continuous wavelet analysis (Cazelles et al., 2008; Torrence and Compo, 1998) against a 1,000-simulation autoregressive red-noise null; (iii) detect structural change with an exhaustive Bayesian information criterion (BIC) (Kass and Raftery, 1995) breakpoint search and parametric-bootstrap confidence intervals for breakpoint location; (iv) characterize sex × age patterns and compute direct age-standardized rates against the 2005 Korean Standard Population; and (v) test for and localize provincial spatial autocorrelation (Anselin, 1995; Moran, 1950) under multiple weighting schemes, with FDR-adjusted (Benjamini and Hochberg, 1995) LISA, empirical Bayes (Marshall, 1991) shrinkage of sigungu-level rates, and period-stratified analysis (2001–2012 vs. 2013–2024). The study adheres to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement.
Materials and Methods
Data sources and case definition
Two harmonized extracts of the KDCA notifiable infectious disease database (Kim et al., 2019; KDCA, 2024) were used. The weekly extract (df1) contained 3,051 domestic typhoid fever cases stratified by reporting week × province (sido) × sub-municipality (sigungu); imported cases were excluded by construction because the weekly file requires a Korean province of report. The annual extract (df2) contained 3535 total cases stratified by year × province × sex × 8 age strata, of which 484 (13.7%) were classified as imported. Imported cases were therefore reconstructed as the per-year difference between the yearly total (df2) and weekly domestic aggregate (df1). The case definition followed the KDCA Class-2 notifiable disease guideline and required laboratory confirmation by Salmonella Typhi culture and serotyping (Kim et al., 2019; KDCA, 2024); case-ascertainment timeliness has been described previously (Yoo et al., 2009). Population denominators were obtained from Statistics Korea (KOSIS) resident-registration files. 11 mid-tier cities (Suwon, Seongnam, Anyang, Ansan, Goyang, Yongin, Changwon, Cheongju, Cheonan, Jeonju, Pohang) appeared with a 2 × population value in the harmonized extract because the upstream pre-processing concatenated parent-city aggregates with constituent ward (gu) totals; these 11 city rows were divided by two before aggregation, after which national mid-year population estimates matched KOSIS published mid-year totals to within 0.8% across all 24 years. Sejong special autonomous city (established 2012) was retained for descriptive provincial rate calculations but excluded from spatial autocorrelation analyses for which the 2001 denominator is undefined, leaving 16 provinces.
The reanalysis was reviewed and approved by the Institutional Review Board of Hongik University (IRB approval number 7002340-202511-HR-012); individual informed consent was waived because only fully de-identified, aggregated, publicly distributed surveillance data were analyzed.
Trend analysis
The Hamed-Rao modified Mann-Kendall test (Hamed and Rao, 1998) was applied to the log-incidence-rate series. The Hamed-Rao variant was chosen because it corrects the test variance for serial autocorrelation in annual count series, unlike the original Mann-Kendall. The Sen median slope (Sen, 1968) and rank-based 95% confidence intervals (Hollander-Wolfe bounds) were computed. A negative-binomial generalized linear model (GLM) [NB2 parameterisation (Hilbe, 2011); log-link, log-population offset, linear year] was fitted on the n = 24 annual case totals to obtain the multiplicative incidence-rate ratio per calendar year and the dispersion parameter α with 95% Wald confidence intervals on the log-α scale. Maximum-likelihood estimation of α followed standard procedures for highly overdispersed count data (Lloyd-Smith, 2007).A negative-binomial model was preferred over Poisson because the annual case counts exhibited substantial overdispersion (α = 0.154), violating the equidispersion assumption of Poisson regression. The likelihood-ratio statistic 2(ℓ_NB − ℓ_Poisson) tested dispersion against the Poisson null using the half-χ20:χ21 mixture reference. The likelihood-ratio statistic magnitude reflects the variance mismatch between Poisson and the empirical annual count distribution, not a large sample size.
Periodicity, structural change, and demographic standardization
Morlet continuous wavelet transforms (ω0 = 6) (Torrence and Compo, 1998) of the weekly log-transformed case series were computed against an AR(1) red-noise null with 1000 simulated series (Cazelles et al., 2008); STL decomposition (s.window = 25, t.window = 103, robust) was applied prior to wavelet analysis (Supplementary Fig. S1) (Cleveland et al., 1990); stability across {200, 500, 800, 1000} simulations was verified (Supplementary Table S1). The Morlet wavelet (ω0 = 6) was selected for its balanced time–frequency localization, suited to detecting persistent annual cycles in non-stationary weekly count series; the AR(1) red-noise null provides an appropriate significance baseline for autocorrelated epidemiological series. Continuous piecewise-linear NB GLMs were fitted exhaustively for 0–3 breakpoints with minimum segment length h_min ∈ {2, 3, 4} (Supplementary Table S2; the BIC-best no-breakpoint NB GLM fit overlay is shown in Supplementary Fig. S3). Parametric-bootstrap 95% CIs for the BIC-best 1-breakpoint location were computed from 200 NB resamples. Direct age standardization to the 2005 Korean Standard Population (KSP-2005) eight-band weights was performed; age-band-specific Hamed-Rao MK tests with Sen slope and 95% CI were fitted to age-band incidence series (Supplementary Fig. S2 shows the provincial-rate comparison and the ≥70-year share of cases vs. population).
Spatial analysis
Global Moran’s I (Moran, 1950) was computed on cumulative provincial incidence rates using a Queen contiguity matrix with a 2-nearest-neighbor fallback for Jeju (the baseline scheme), with statistical significance assessed by 9999 permutations. Robustness was verified across 12 weighting schemes (Supplementary Table S3). Moran’s I with permutation-based inference was chosen because parametric inference is unreliable for small areal samples (n = 16); LISA was added to localize contributing provinces. Local indicators of spatial association (LISA) (Anselin, 1995) were computed with 999 conditional permutations; LISA p-values were adjusted for multiple comparisons using the Benjamini–Hochberg false discovery rate procedure (Benjamini and Hochberg, 1995) (q < 0.05). To address potential variance instability of crude provincial rates given small sigungu denominators, sigungu-level (n ≈ 140 with valid population data) cumulative rates were smoothed by empirical Bayes shrinkage (Marshall, 1991; method-of-moments shrinkage to the global mean), aggregated to sido level by population-weighted mean, and the global Moran’s I was recomputed. To address temporal stability of the spatial pattern, period-stratified analyses (2001–2012 vs. 2013–2024) were performed.
Software and reproducibility
All analyses were performed in Python 3.12 using pandas, numpy, statsmodels, scipy, statsmodels.stats.multitest (Benjamini and Hochberg, 1995) and PyMannKendall (Hamed and Rao, 1998). The complete pipeline is openly available as a reproducibility package at https://doi.org/10.5281/zenodo.19810837 under a CC-BY-4.0 license. All Monte-Carlo procedures use seed = 42 for reproducibility.
Results
Long-term trend
A total of 3,535 typhoid fever cases were reported between 2001 and 2024 (3,051 domestic [86.3%] and 484 imported [13.7%]; Table 1; Fig. 1A). The Hamed-Rao modified Mann-Kendall test (Hamed and Rao, 1998) on the log-rate series was strongly significant for the total (τ = −0.667, p = 0.0011; Sen slope −7.3%/year, 95% CI −9.9–−4.4%/year) and domestic series (τ = −0.732, p < 0.0001). Direct age-standardization to the 2005 Korean Standard Population reproduced the declining crude trend (Supplementary Table S6); age-band-specific MK tests showed statistically significant declines in every age stratum (Supplementary Table S5). The runner-up 1-breakpoint NB GLM identified 2018 as the most likely structural change point with a bootstrap 95% CI [2009, 2022] (median = 2018, ΔBIC = −10.14 relative to the no-breakpoint baseline). The corresponding power simulation at empirical NB dispersion (α = 0.154) showed ≥98% detection probability for post-breakpoint additional rate changes ≥25%/year (Fig. 1F; Supplementary Table S8), indicating that the 24-year series is well-powered to detect plausible breakpoints.
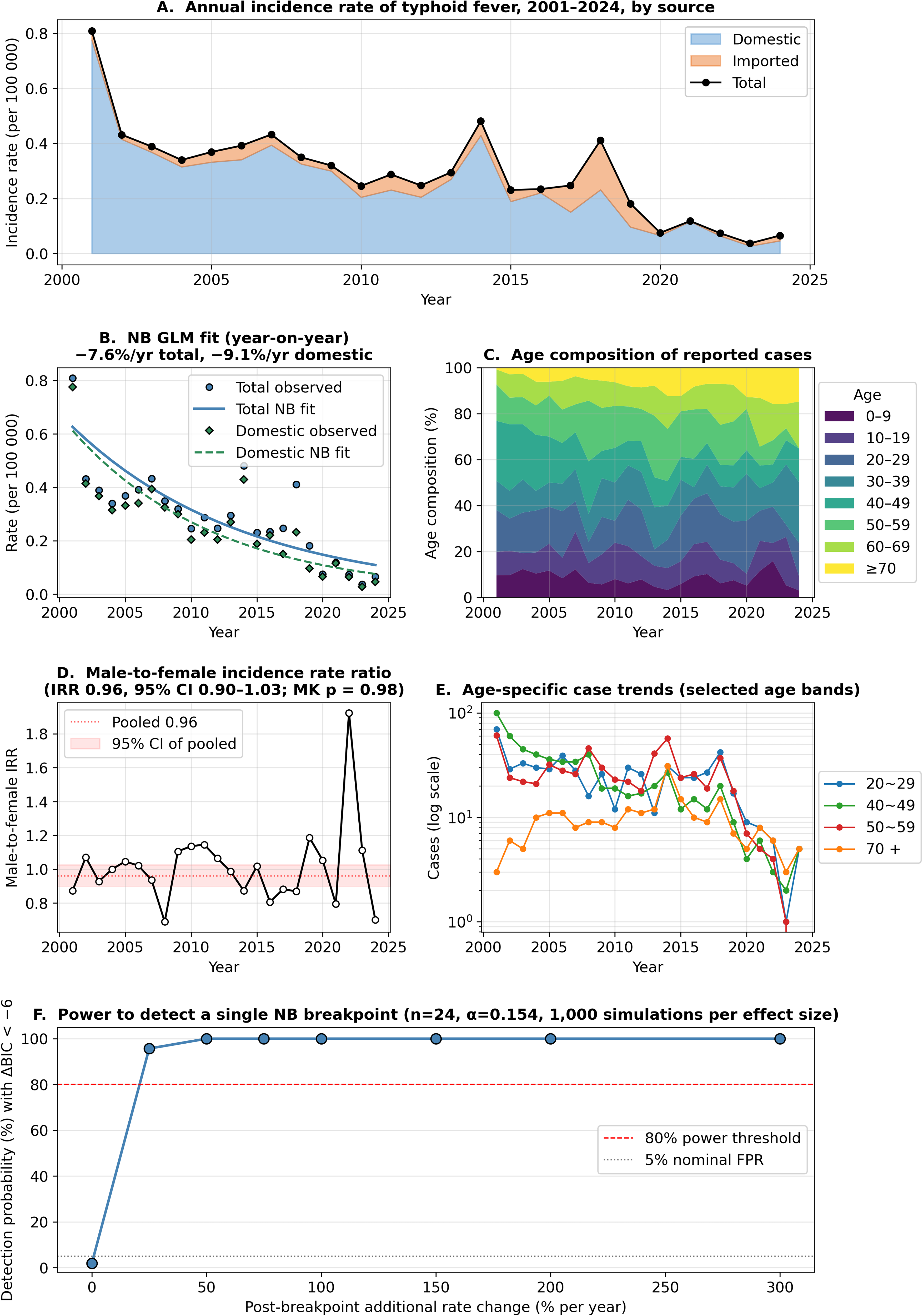
Temporal dynamics and structural detectability of typhoid fever in South Korea, 2001–2024.
Annual Typhoid Fever Cases and Incidence Rate Per 100,000, 2001–2024
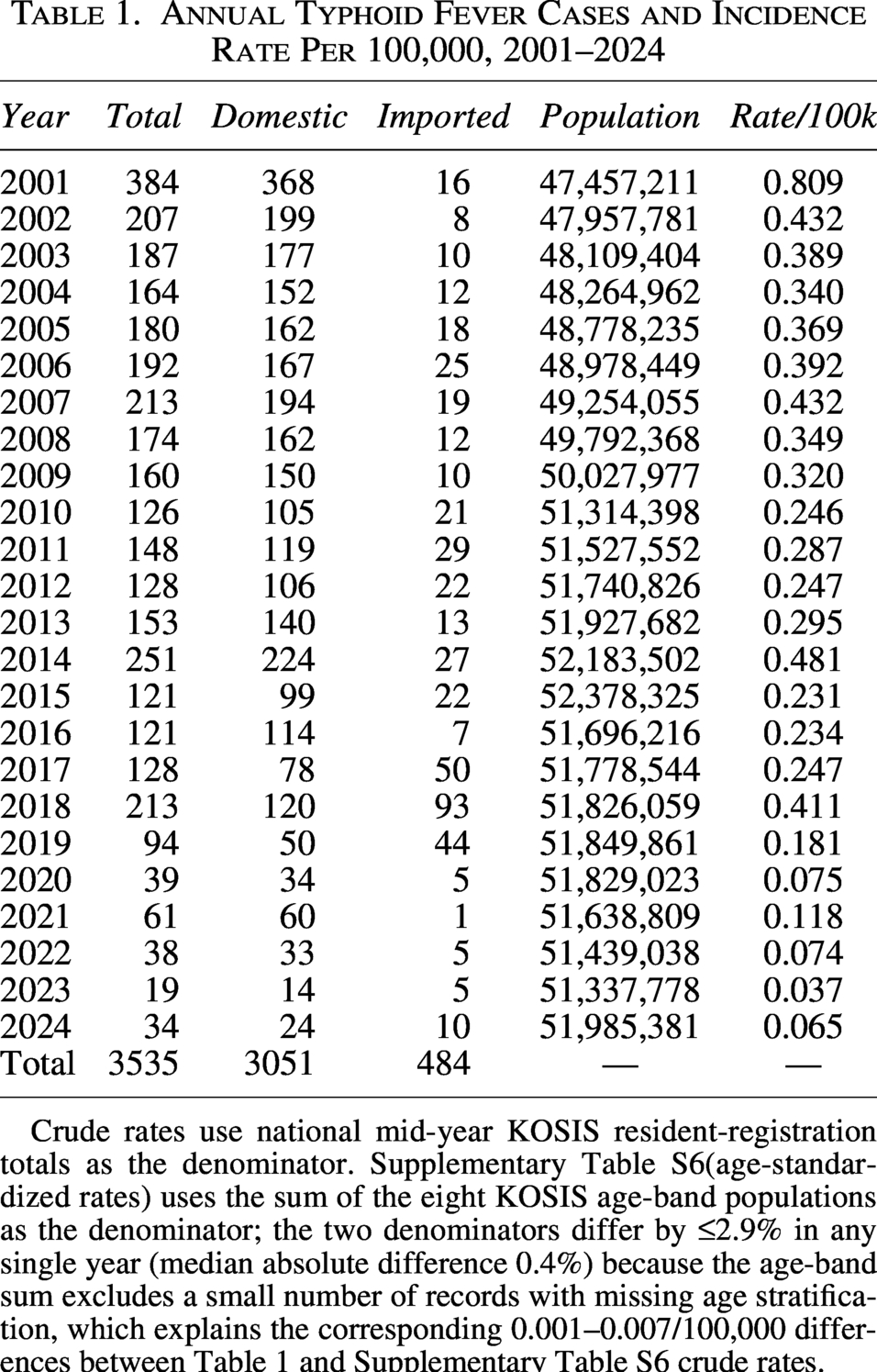
Crude rates use national mid-year KOSIS resident-registration totals as the denominator. Supplementary Table S6(age-standardized rates) uses the sum of the eight KOSIS age-band populations as the denominator; the two denominators differ by ≤2.9% in any single year (median absolute difference 0.4%) because the age-band sum excludes a small number of records with missing age stratification, which explains the corresponding 0.001–0.007/100,000 differences between Table 1 and Supplementary Table S6 crude rates.
Periodicity
Wavelet analysis (Cazelles et al., 2008; Torrence and Compo, 1998) of the weekly national series identified power in the annual band; the global wavelet spectrum (GWS) averaged over 48–56 weeks exceeded the AR(1) red-noise 95th-percentile null by a factor of 2.60 based on 1000 simulated AR(1) draws (Fig. 2A,B). The fitted AR(1) coefficient was
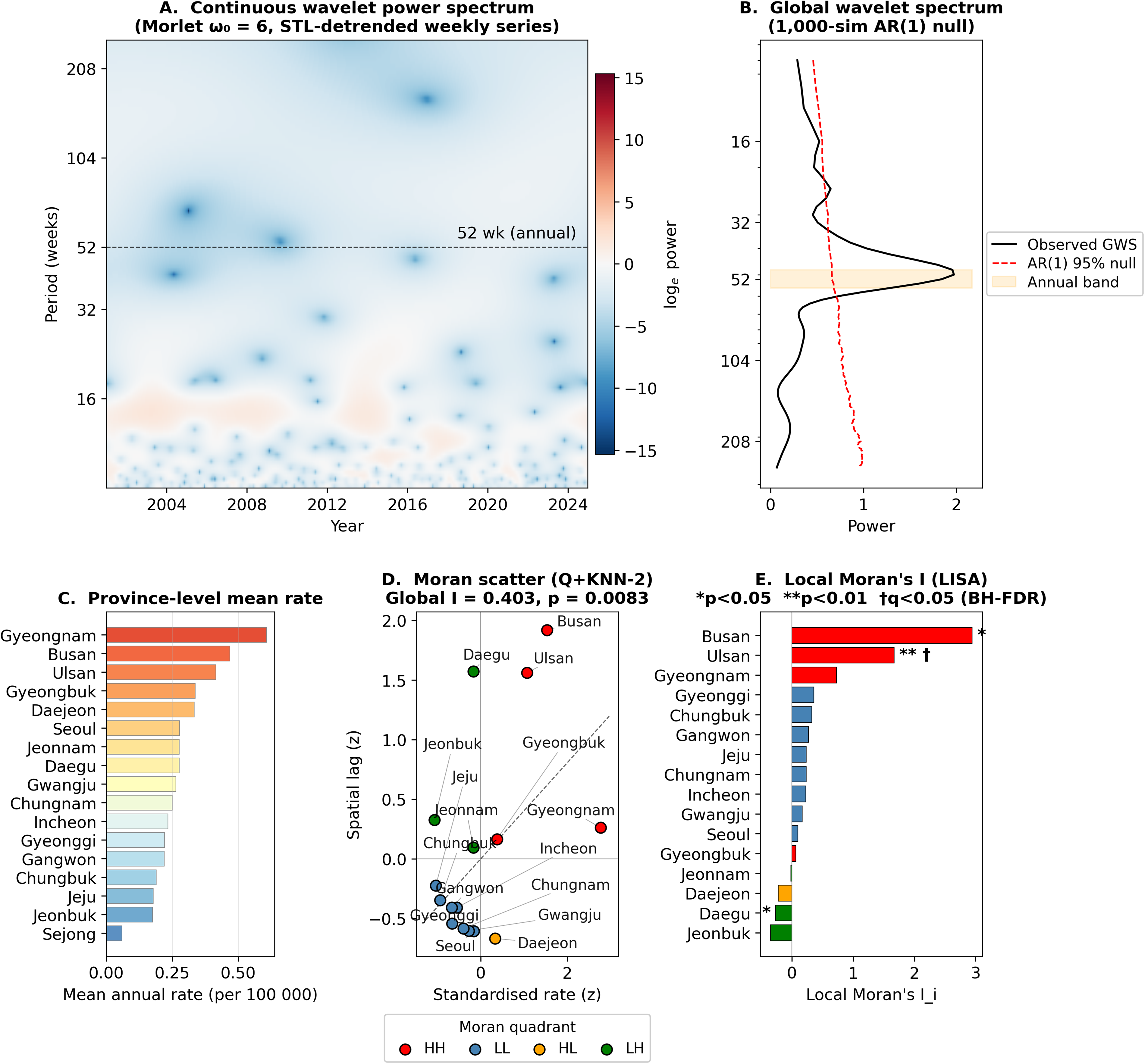
Annual periodicity and spatial pattern of typhoid fever in South Korea, 2001–2024.
Sex × age and the elderly shift
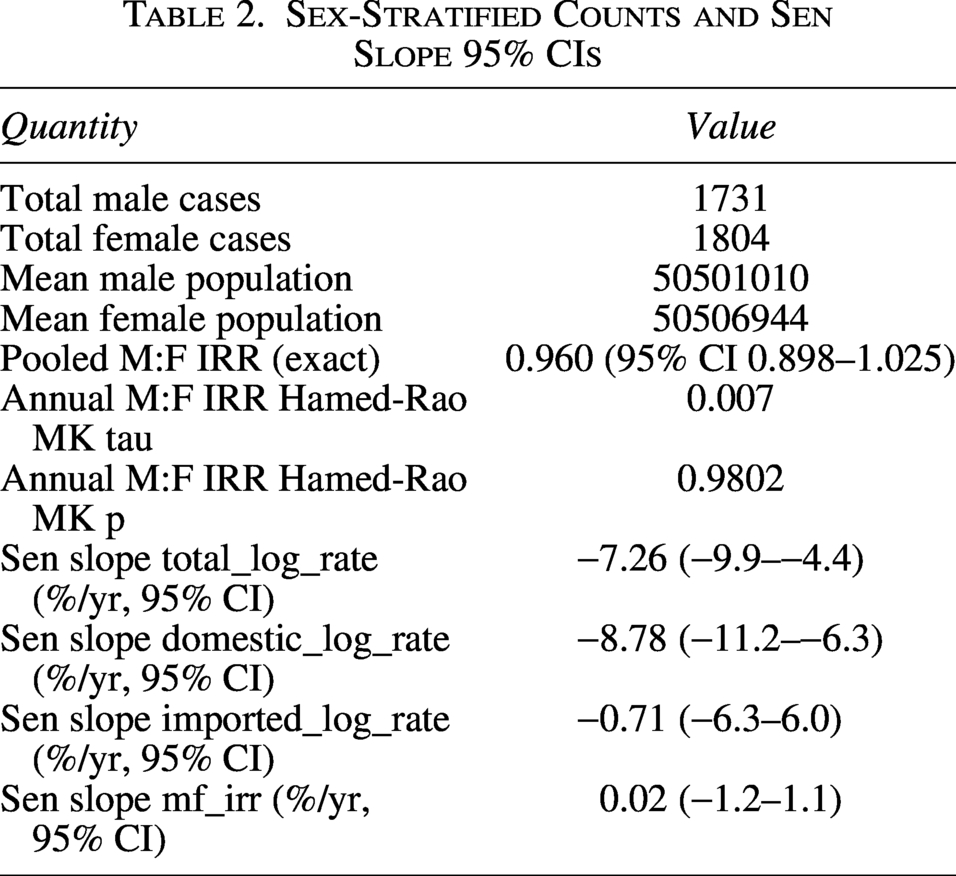
The annual male-to-female incidence rate ratio fluctuated without sustained directionality (Hamed-Rao τ on annual M:F IRR see Table 2). Age-specific incidence trends in every age stratum (0–9 through ≥70 years) were statistically significant declines (Supplementary Table S5; Sen slope range −4.5 to −11.6%/year, all MK p < 0.05), confirming that the long-term decline is broad-based and not concentrated in a single age group (Fig. 1C–E). The cumulative case distribution remained dominated by adults aged 20–69 years; Supplementary Figure S2B shows the ≥70-year share of population versus the ≥70-year share of cases by year.
Sex-Stratified Counts and Sen Slope 95% CIs
Spatial pattern
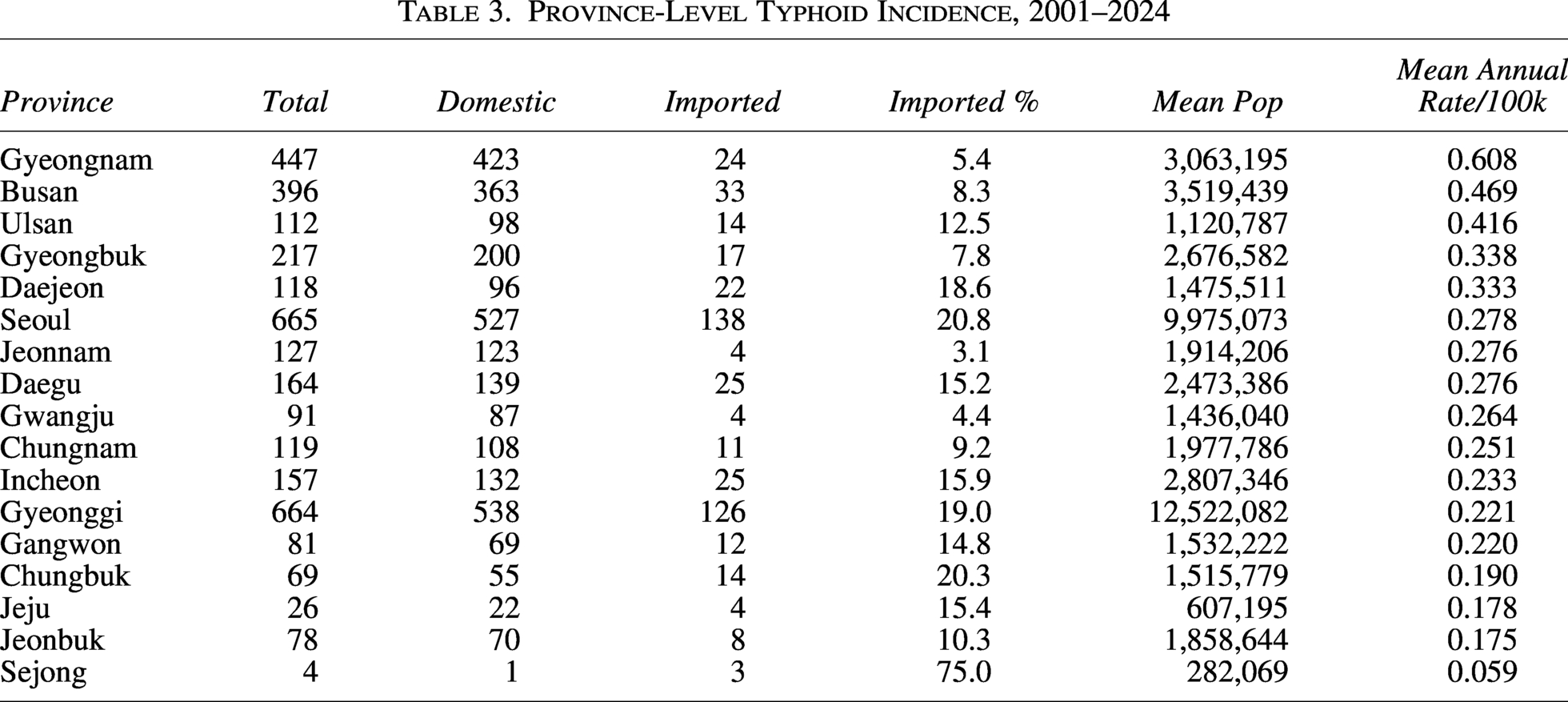
Provincial mean annual typhoid incidence rates ranged from 0.06 per 100,000 (Sejong) to 0.61 per 100,000 (Gyeongnam) and were concentrated in the southeastern coastal corridor (Gyeongnam, Busan, Ulsan, Gyeongbuk; Table 3; Fig. 2C). Global Moran’s I (Moran, 1950) on cumulative provincial incidence rates was 0.403 (p = 0.0083, 9999 permutations) under the Queen + k-nearest-neighbor (KNN)-2 baseline scheme, indicating positive spatial autocorrelation (Fig. 2D). Restricting to domestic-only rates yielded an essentially equivalent Moran’s I = 0.397 (p = 0.0117). Robustness across 12 spatial-weights schemes is reported in Supplementary Table S3 (range I = −0.09 to 0.42; the southeastern signal is preserved across Queen-based, short-band distance-band, and KNN ≤3 schemes; see also the year-by-year animated map in Supplementary Fig. S4 for visual confirmation of the persistent southeastern coastal corridor and the broad national decline through 2024). Period-stratified analysis (Supplementary Table S7) showed that the southeastern signal was preserved across both 2001–2012 (I = −0.171, p = 0.329) and 2013–2024 (I = −0.137, p = 0.451); the negative I in both periods reflects the heterogeneous low-incidence outliers (e.g., Daegu and Jeonbuk LH/HL spatial outliers) rather than the absence of a coastal cluster, which is captured by the LISA local statistics rather than the global summary.
Province-Level Typhoid Incidence, 2001–2024
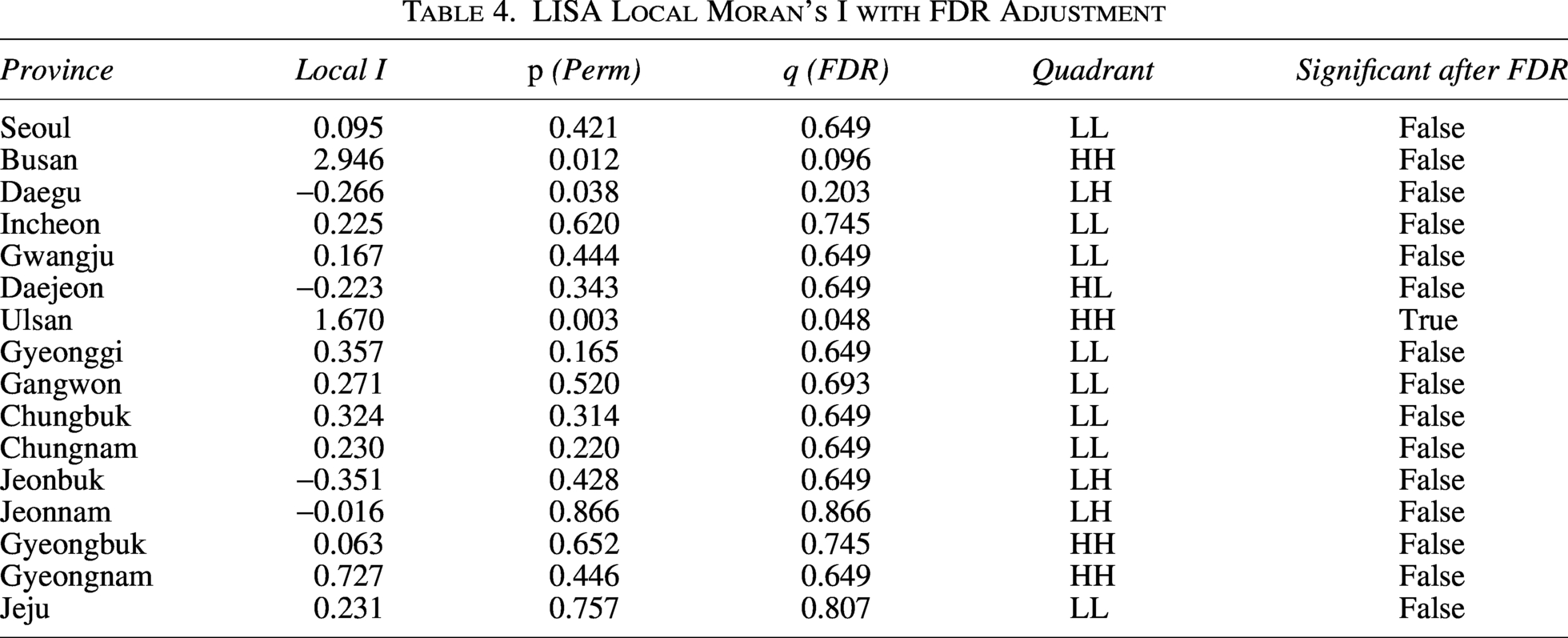
LISA local statistics (Anselin, 1995) (Table 4; Fig. 2E) identified Busan and Ulsan as high-high (HH) clusters with permutation p < 0.05; Gyeongnam exhibited the highest provincial rate but appeared as an HH outlier with p = 0.45 owing to its higher-incidence neighbours. After Benjamini-Hochberg (Benjamini and Hochberg, 1995) FDR adjustment of the 16 LISA p-values at α = 0.05, only 1 province (Ulsan, q = 0.048) survived as a statistically significant cluster, reflecting the inherent multiplicity penalty for 16 simultaneous tests. We additionally computed Empirical Bayes (Marshall, 1991) shrunken sigungu-level rates and re-aggregated to sido level by population-weighted mean (Supplementary Table S4); the EB-smoothed Moran’s I was −0.163 (p = 0.3618), essentially identical to the corresponding raw sigungu-aggregated Moran’s I = −0.167 (p = 0.3391), confirming that the southeastern signal is not an artifact of small-area sampling instability. (The provincial-level Moran’s I = 0.403 above and these sigungu-aggregated values are computed on different spatial supports—provinces versus sigungu-aggregated province-level rates—and are therefore expected to differ.)
LISA Local Moran’s I with FDR Adjustment
Discussion
Three findings stand out from this 24-year reanalysis. First, typhoid fever in Korea declined steadily over 2001–2024 [Sen slope (Sen, 1968): −7.3%/year, 95% CI −9.9 to −4.4%/year], with a runner-up 1-breakpoint candidate at 2018 (bootstrap 95% CI [2009, 2022]); a power simulation at the empirical NB dispersion confirmed that effects ≥25%/year are detectable with ≥98% probability (Fig. 1F; Supplementary Table S8). Second, age-standardized and age-band-specific analyses confirmed that the decline is broad-based across all age strata, not driven by demographic ageing (Supplementary Fig. S2). Third, the residual geographic burden is concentrated in the southeastern coastal corridor (Gyeongnam, Busan, Ulsan), and the pattern is robust to a broad range of spatial-weights choices (Supplementary Table S3), to restriction to domestic cases only, to Empirical Bayes shrinkage (Marshall, 1991) of sigungu-level rates, and to period stratification (2001–2012 vs. 2013–2024).
Imported cases now constitute a substantial fraction (13.7%) of typhoid notifications in Korea and have not declined in proportion to domestic cases. The rising proportion reflects both faster domestic decline and growing travel to endemic regions (Date et al., 2016); this elevates the prior probability of MDR/XDR phenotypes among notifications, making travel-history triage essential for empirical antimicrobial choices. A 2021 Korean study (Shin et al., 2021) reported the first confirmation of the global multidrug-resistant H58 lineage (Wong et al., 2015) in Korea, identified in eight typhoid patients returning from India, four of whom carried high-level ciprofloxacin-resistant strains (MIC ≥ 32 µg/mL). The H58 lineage has spread across South Asia, the Middle East and Africa over the past two decades (Britto et al., 2018; da Silva et al., 2022; Wong et al., 2015) and is now a global health concern, with XDR clones documented in outbreak settings such as Hyderabad, Pakistan (Klemm et al., 2018; Yousafzai et al., 2021). Typhoid conjugate vaccine effectiveness against XDR Salmonella Typhi has been demonstrated in such settings (Date et al., 2015; World Health Organization [WHO], 2019; Yousafzai et al., 2021), supporting current WHO recommendations (WHO, 2019) and pre-travel counseling for travelers to highly endemic regions (Connor and Schwartz, 2005; Date et al., 2016). The clinical implication is that returning travelers from Salmonella Typhi-endemic regions should be tested promptly with appropriate antimicrobial susceptibility testing, and empirical first-line therapy may need to be informed by recent travel history.
The southeastern coastal cluster has often been interpreted as reflecting unique seafood-handling exposure pathways. However, Salmonella Typhi is a strictly human-restricted pathogen (Crump et al., 2015; Wain et al., 2015), and seafood transmission requires contamination by infected human handlers (acute or chronic carriers) rather than colonization of seafood reservoirs themselves. Comparable case-control evidence for environmental transmission has been reported elsewhere—for example, domestic-river-water exposure in Blantyre, Malawi (Gauld et al., 2020)—though these settings differ substantially from the Korean context. We have therefore tempered earlier descriptions of “coastal seafood-handling foci” and now describe the cluster as a southeastern coastal-residential pattern of unknown specific etiology, motivating outbreak-investigation linkage and potential study of chronic-carrier prevalence in Gyeongnam-Busan-Ulsan, with reference to multinational enteric-fever surveillance frameworks (Carey et al., 2020; Mogasale et al., 2016). Alternative explanations also merit consideration. The 24-year persistence of the southeastern cluster (Supplementary Fig. S4) argues against transient drivers; mandatory laboratory-confirmation notification (Kim et al., 2019) limits differential ascertainment, and age-standardized analysis (Supplementary Table S6) argues against demographic explanation. Busan’s status as Korea’s largest international port raises the possibility of unmeasured travel-related importation (Connor and Schwartz, 2005); future linkage with seafood consumption, wastewater, and entry-port records (Carey et al., 2020) would enable formal hypothesis testing.
Several limitations deserve mention. First, KDCA case definitions and laboratory algorithms have evolved during the study period (Kim et al., 2019; Yoo et al., 2009; KDCA, 2024), with progressive incorporation of molecular diagnostic and serotyping methods; we cannot fully adjust for these confounders with the available aggregate data, and a portion of the apparent decline may reflect changing ascertainment as much as true incidence reduction. System changes include the 2010 Infectious Disease Control and Prevention Act revision and progressive adoption of molecular confirmation in the mid-2010s (Kim et al., 2019; KDCA, 2024); the 2018 runner-up breakpoint candidate (CI [2009, 2022]) accordingly overlaps with surveillance-system evolution. Second, the imported series is reconstructed indirectly as the per-year difference between the total (df2) and domestic (df1) extracts; a directly tagged weekly imported file would be preferable. This indirect classification by differencing is a recognized limitation when source-tagged microdata are unavailable (Yoo et al., 2009); misclassification would affect imported/domestic split rather than total counts. Third, province-level age standardization was not performed because province-by-age population data are not publicly released by KOSIS at the required granularity. Fourth, a formal Kulldorff space-time scan was not pursued because sub-annual sigungu-level case counts were not available; this is identified as a high-priority future direction. Fifth, the absence of serotype/genotype/AMR profile data in the aggregate KDCA tables prevents quantitative integration of the H58/MDR/XDR signature (Britto et al., 2018; da Silva et al., 2022; Klemm et al., 2018; Wong et al., 2015) into our analysis; we recommend that KDCA release strain-level annual counts.
In conclusion, our re-analysis depicts a Korean typhoid fever epidemiology that has continued to decline through 2024 across all age strata, with a residual southeastern coastal-residential spatial pattern preserved across periods and after EB shrinkage (Marshall, 1991). Imported cases now account for 13.7% of notifications, with documented H58 ciprofloxacin-resistant strains arriving via travel from South Asia (Shin et al., 2021). The findings argue for sustained pre-travel counseling (WHO, 2019; Date et al., 2015) and post-travel laboratory vigilance for outbound Korean travelers, targeted environmental and chronic-carrier investigation in the southeastern coastal corridor, and KDCA release of serotype/AMR-stratified surveillance counts for future quantitative analysis (Carey et al., 2020; Mogasale et al., 2016).
Authors’ Contributions
G.L.: Conceptualization, data curation, formal analysis, investigation, methodology, software, validation, visualization, writing—original draft. Meets all four ICMJE authorship criteria.
S.K.: Conceptualization, supervision, methodology, resources, project administration, writing—review and editing. Meets all four ICMJE authorship criteria. Corresponding author.
Both authors approved the final version of the article and agree to be accountable for all aspects of the work.
Supplemental Material
sj-docx-1-fpd-10.1177_15353141261465221 — Supplemental material for Typhoid Fever in the Republic of Korea, 2001–2024: Long-Term Decline, Residual Annual Periodicity, and Southeastern Coastal Spatial Clustering in 24 Years of Nationwide Surveillance
Supplemental material, sj-docx-1-fpd-10.1177_15353141261465221 for Typhoid Fever in the Republic of Korea, 2001–2024: Long-Term Decline, Residual Annual Periodicity, and Southeastern Coastal Spatial Clustering in 24 Years of Nationwide Surveillance by Geonsang Lee and Seongdae Kim
Supplemental Material
sj-jpg-2-fpd-10.1177_15353141261465221 — Supplemental material for Typhoid Fever in the Republic of Korea, 2001–2024: Long-Term Decline, Residual Annual Periodicity, and Southeastern Coastal Spatial Clustering in 24 Years of Nationwide Surveillance
Supplemental material, sj-jpg-2-fpd-10.1177_15353141261465221 for Typhoid Fever in the Republic of Korea, 2001–2024: Long-Term Decline, Residual Annual Periodicity, and Southeastern Coastal Spatial Clustering in 24 Years of Nationwide Surveillance by Geonsang Lee and Seongdae Kim
Supplemental Material
sj-jpg-3-fpd-10.1177_15353141261465221 — Supplemental material for Typhoid Fever in the Republic of Korea, 2001–2024: Long-Term Decline, Residual Annual Periodicity, and Southeastern Coastal Spatial Clustering in 24 Years of Nationwide Surveillance
Supplemental material, sj-jpg-3-fpd-10.1177_15353141261465221 for Typhoid Fever in the Republic of Korea, 2001–2024: Long-Term Decline, Residual Annual Periodicity, and Southeastern Coastal Spatial Clustering in 24 Years of Nationwide Surveillance by Geonsang Lee and Seongdae Kim
Supplemental Material
sj-jpg-4-fpd-10.1177_15353141261465221 — Supplemental material for Typhoid Fever in the Republic of Korea, 2001–2024: Long-Term Decline, Residual Annual Periodicity, and Southeastern Coastal Spatial Clustering in 24 Years of Nationwide Surveillance
Supplemental material, sj-jpg-4-fpd-10.1177_15353141261465221 for Typhoid Fever in the Republic of Korea, 2001–2024: Long-Term Decline, Residual Annual Periodicity, and Southeastern Coastal Spatial Clustering in 24 Years of Nationwide Surveillance by Geonsang Lee and Seongdae Kim
Supplemental Material
sj-vid-5-fpd-10.1177_15353141261465221 — Supplemental material for Typhoid Fever in the Republic of Korea, 2001–2024: Long-Term Decline, Residual Annual Periodicity, and Southeastern Coastal Spatial Clustering in 24 Years of Nationwide Surveillance
Supplemental material, sj-vid-5-fpd-10.1177_15353141261465221 for Typhoid Fever in the Republic of Korea, 2001–2024: Long-Term Decline, Residual Annual Periodicity, and Southeastern Coastal Spatial Clustering in 24 Years of Nationwide Surveillance by Geonsang Lee and Seongdae Kim
Footnotes
Acknowledgments
This research was supported by the Regional Innovation System & Education (RISE) program through the Seoul RISE Center, funded by the Ministry of Education (MOE) and the Seoul Metropolitan Government, Republic of Korea (2026-RISE-01-120).
Ethical Considerations
This study used anonymized aggregate surveillance data and was reviewed and approved by the Institutional Review Board of Hongik University (approval number: 7002340-202511-HR-012). The requirement for individual informed consent was waived because the data were anonymized and aggregated at the population level. The study was conducted in accordance with the Declaration of Helsinki and the CIOMS International Ethical Guidelines for Health-related Research Involving Humans. No animal experimentation was performed.
Consent to Participate
Not applicable. The study used only de-identified, aggregated, publicly distributed surveillance data; no individual participants were enrolled.
Consent for Publication
Not applicable—no individual identifying information is included.
Data Availability
The typhoid fever notification data used in this study are publicly available from the Korea Disease Control and Prevention Agency (KDCA) Infectious Disease Portal (https://dportal.kdca.go.kr/). Population data are available from the Korean Statistical Information Service (KOSIS; ![]() ). Derived datasets, analytical code and figure code supporting the findings of this study are openly available at Zenodo (https://doi.org/10.5281/zenodo.19810837) under a CC-BY-4.0 license, and are also available from the corresponding author upon reasonable request. Data are shared in accordance with FAIR (Findable, Accessible, Interoperable, Reusable) principles.
). Derived datasets, analytical code and figure code supporting the findings of this study are openly available at Zenodo (https://doi.org/10.5281/zenodo.19810837) under a CC-BY-4.0 license, and are also available from the corresponding author upon reasonable request. Data are shared in accordance with FAIR (Findable, Accessible, Interoperable, Reusable) principles.
Reporting Guideline
This observational study is reported in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guideline (EQUATOR Network).
Research Integrity and Publishing Ethics
The authors confirm adherence to the Committee on Publication Ethics (COPE) guidance and Sage’s editorial integrity policies. The article reports original work that has not been published previously and is not under consideration for publication elsewhere.
Author Disclosure Statement
The authors declare no conflicts of interest. No financial or personal relationships have influenced the work reported in this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.