
Abstract
The aim of the study was to examine the cardioprotective effect of morphine and Delta 2 opioid
Introduction
The stimulation of opioid receptors before ischemia
1–4
or at the reperfusion
5–13
has been shown to have protective effects against ischemia–reperfusion injury. Nevertheless, the effect of opioid receptors stimulation at the reperfusion period was investigated only in animal.
5–13
It has been shown that morphine, a non-specific agonist of opioid receptors, induced postconditioning (PostC), but at concentrations higher than that resulting from clinical use.
5,7,9,12,13
Many studies demonstrated that activation of delta opioid receptors mediated ischemic PostC in rat heart.
5,6
Delta-2 opioid
The mPTP appears to be a critical determinant of cell death in ischemia–reperfusion injury and the prevention of mPTP opening has been reported in ischemic PostC and in morphine-induced PostC. 5,7,17–19 Moreover, in isolated rat heart, a link between activation of delta opioid receptor and inhibition of mPTP in morphine-induced PostC has been suggested. 7 Shanmuganathan et al. 20 demonstrated that pharmacological inhibition of mPTP opening, at the onset of reperfusion, induced cardioprotection of isolated human right atrial trabeculae. However, in human myocardium, the link between morphine and DADLE-induced PostC and mPTP has never been investigated.
The aims of the present study were to examine: (1) the effect of administration of morphine and the DADLE during the first minutes of reoxygenation and (2) the involvement of the mPTP in morphine and DADLE -induced PostC in human atrial trabeculae model.
Material and methods
Patients demographic data, preoperative drug treatments, and preoperative left ventricular ejection fraction
The number in brackets after heart disease and drug abbreviation indicate the number of patients. Age and LVEF are expressed as mean ± SD
Atract, Atractyloside; AVR, aortic valve replacement; CABG, coronary artery bypass graft; DADLE,
Experimental conditions
As previously described, 21 one or two trabeculae were isolated from right atrial appendage, and placed vertically between an isometric force transducer (MLT0202; ADInstruments, Sydney, Australia) and maintained by clip in a 200 ml jacketed reservoir contained Tyrode's modified solution (120 mmol NaCl, 3.5 mmol KCl, 1.1 mmol MgCl2, 1.8 mmol NaH2PO4, 25.7 mmol NaHCO3, 2.0 mmol CaCl2, and 5.5 mmol glucose, pH 7.40). The Tyrode's modified solution was insufflated with 95% O2–5% CO2, resulting in a partial pressure of oxygen of 600 mmHg. A thermostatic water circulator (Polystat micropros; Bioblock, Illkirch, France) maintained the temperature of reservoir at 34°C. Trabecualae were field-stimulated by two platinum electrodes at 1 Hz with rectangular wave pulses of 5-ms duration 20% above threshold (CMS 95107; Bionic Instrument, Paris, France).
A period of equilibration (90 min) was respected, permitting that trabeculae develop their mechanical performance at the apex of the length active isometric tension curve (L max). The developed force was measured in continuous, digitized at a sampling frequency of 400 Hz and the data stored in a computer (PowerLab; ADInstruments).
At the end of experiment, the muscle cross-sectional area was calculated from its weight and length assuming a cylindrical shape and a density of 1. To avoid including sample suffering from core hypoxia, We excluded trabeculae with a cross-sectional area grater than 1.0 mm2, a force of contraction normalized per cross-sectional area (FoC) less than 5.0 mN/mm2, and a ratio of resting force/total force grater than 0.50 otherwise they were excluded a posteriori. 22
Experimental protocol
At the end of the equilibration period, the trabeculae were randomized into eight groups. In all groups, trabeculae were exposed to the hypoxia reoxygenation protocol, by insufflation with 95% N2–5% CO2 in the buffer for 30 min, followed by a 60 min oxygenated recovery period, as previously described by our group
21
(Figure 1).
Experimental protocol. In morphine group, morphine was administered at 0.5 μmol during the first 15 min of reoxygenation. In DADLE groups, DADLE were administered during the first 15 min of reoxygenation, at 10 nmol (DADLE 10 group), at 50 nmol (DADLE 50 group) and at 100 nmol (DADLE 100 group). In morphine + atract and DADLE + atract groups, morphine 0.5 μmol and DADLE 100 nmol were administered in the presence of atractyloside 50 μmol. Atract, atractyloside; DADLE, 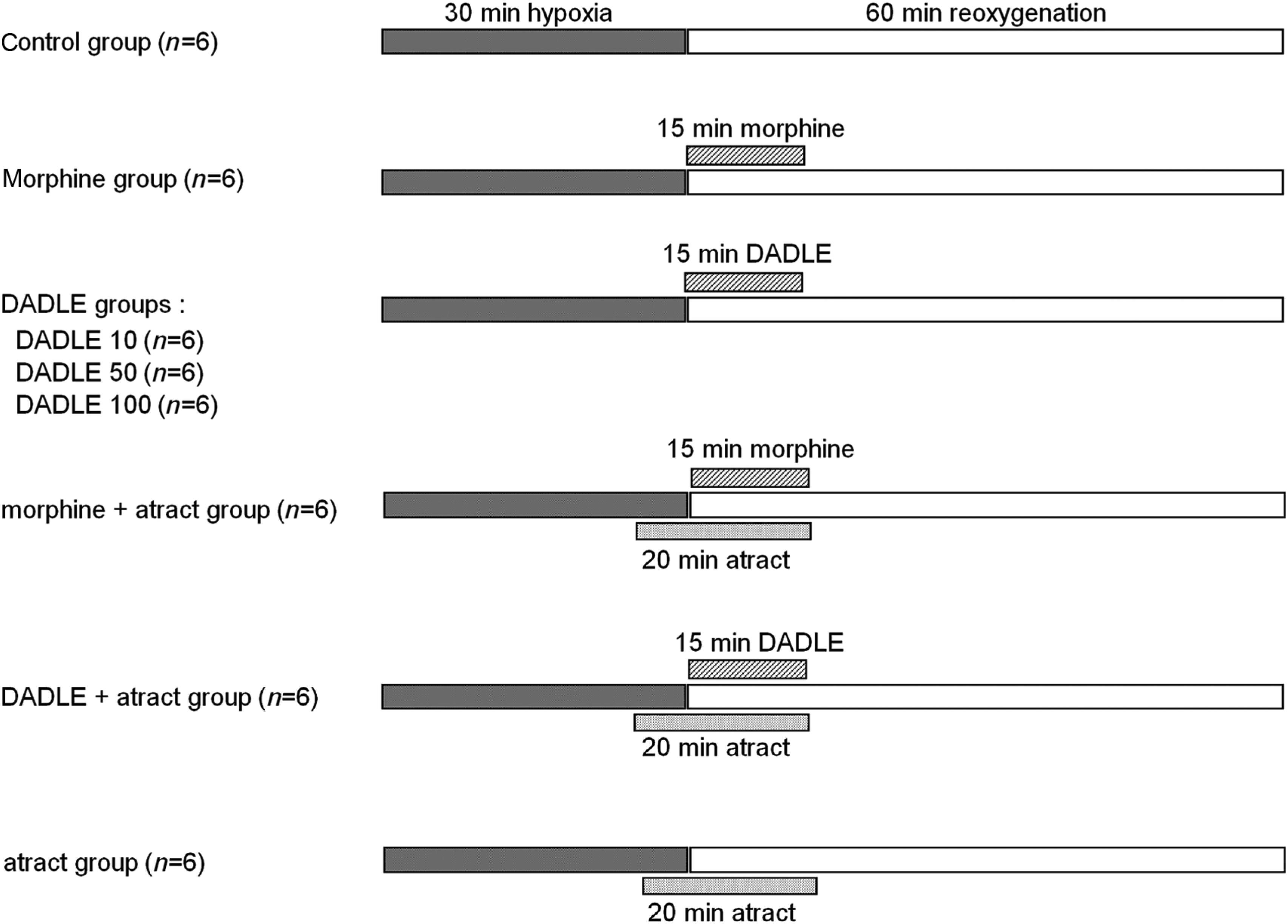
In the control group (control; n = 6), no other treatment were administered (Figure 1).
In treatment groups, morphine 0.5 μmol (morphine; n = 6), DADLE 10 nmol (DADLE 10; n = 6), DADLE 50 nmol (DADLE 50; n = 6), DADLE 100 nmol (DADLE 100; n = 6) were administered during the first 15 min of reoxygenation (Figure 1).
In another two groups, DADLE 100 nmol and morphine 0.5 μmol were respectively administered in the presence of atractyloside 50 μmol (Sigma Aldrich, Saint Quentin Fallavier, France), the mPTP opener (morphine + atract and DADLE + atract; n = 6 in each group). Atractyloside was administered five minutes before morphine or DADLE and throughout the administration of morphine or DADLE (Figure 1).
In an additional group atractyloside 50 μmol was administered alone five minutes before reoxygenation and during the 15 first minutes of reoxygenation (atract; n = 6; Figure 1).
The morphine dose, used in the present study, was based on clinical practice and are comparable to a blood concentration of patient that received high doses of morphine intravenously. 23 This DADLE range dose (nmol) has been used in the human myocardium in vitro, in a context of PC. 16 We have previously shown that atractyloside, used at a dose of 50 μmol, was sufficient to abolish cardioprotection without some effect in control conditions, in the same experimental model. 21
Statistical analysis
The endpoint of the study was the recovery of FoC at 60 min of reoxygenation (FoC60, expressed as percent of baseline value). Taken account the number of comparisons, the power analysis calculated a group size of n = 6 to detect a difference of 40% in FoC60 with a power of 0.8 at alpha-level of 0.05. Data are expressed as mean ± standard deviation (SD). Age, preoperative left ventricular ejection fraction (Table 1) and FoC60 are compared by an univariate analysis of variance with group factor as the independent variable. If P value was inferior to 0.05 a post hoc test (Bonferroni) was performed. Within-group data were analyzed over time using analysis of variance for repeated-measures and Bonferroni post hoc analysis with group factor and time (baseline, hypoxia 5, 10, 20, 30 min and reoxygenation 5, 10, 20, 30, 40, 50 and 60 min) as covariates. All P values were two-tailed, and a P value of less than 0.05 was required to reject the null hypothesis. Statview 5 software (Deltasoft, Meylan, France) was used for perform statistical analysis.
Results
Control values of main mechanical parameters of human right atrial trabeculae
Data are mean ± SD
L
max, maximal length at the apex of the length—active force curve; CSA, cross-sectional area; FoC, isometric force of contraction normalized per cross-sectional area; RF/TF, ratio of resting force on total force; atract, atractyloside; DADLE,
Effect of morphine and DADLE on hypoxia reoxygenation
In the control group, after 30 min of hypoxia and 60 min reoxygenation resulted in a partial recovery of FoC60 (53 ± 3% of baseline). As compared with control group, DADLE 10 (50 ± 9% of baseline; P = 0.60 versus control group) did not significantly modify FoC60 (Figure 2).
Recovery of force of contraction of isolated human right atrial trabeculae at the end of the 60-min reoxygenation period (FoC60). Recovery of force of contraction of isolated human right atrial trabeculae at the end of the 60-min reoxygenation period (FoC60) after the 30-min hypoxic challenge in groups exposed, during the first 15 min of reoxygenation, to morphine 0.5 μmol (Morphine; n = 6), DADLE 10 nmol (DADLE 10; n = 6), DADLE 50 nmol (DADLE 50; n = 6), DADLE 100 nmol (DADLE 100; n = 6), morphine 0.5 μmol in the presence of atractyloside 50 μmol (morphine + atract; n = 6) DADLE 100 nmol in the presence of atractyloside 50 μmol (DADLE + atract; n = 6) and atractyloside 50 μmol alone (atract; n = 6). Data are mean ± SD. *P < 0.001 versus control, DADLE 10, morphine + atract, DADLE + atract, atract groups. Atract, atractyloside; DADLE, 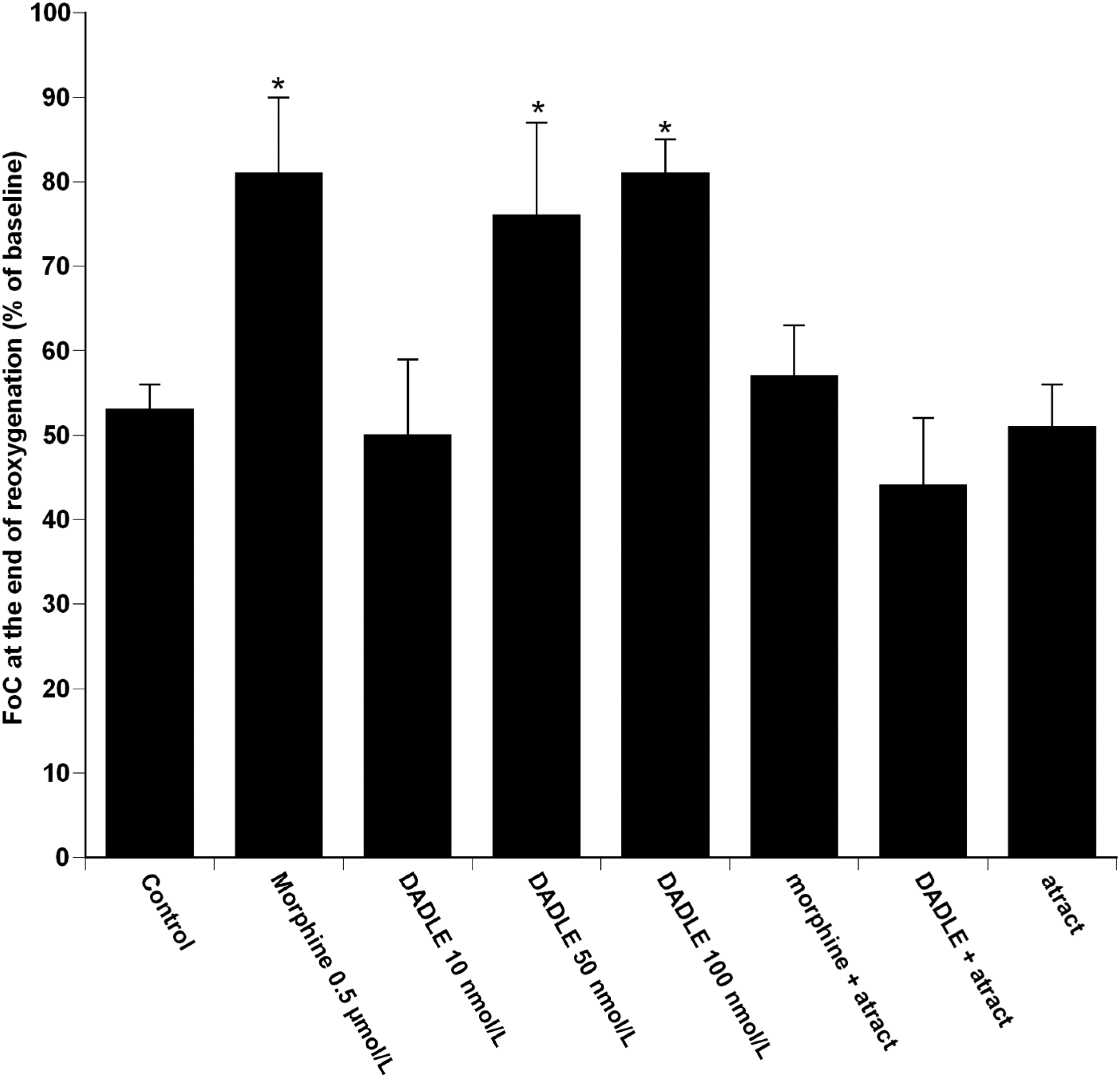
As compared with the control group, morphine (81 ± 9% of baseline; P < 0.001 versus control group), DADLE 50 (76 ± 11% of baseline; P < 0.001 versus control group), DADLE 100 (81 ± 4% of baseline; P < 0.001 versus control group) increased the FoC60. There was no difference in the FoC60 measured in the morphine, DADLE 50 and DADLE 100 groups (morphine group versus DADLE 50 group P = 0.29; morphine group versus DADLE 100 group P = 0.95 and DADLE 50 versus DADLE 100 P = 0.32) (Figure 2).
Effect of atractyloside on morphine and DADLE treatment
As shown in Figure 2, morphine-induced enhanced recovery of FoC60 (81 ± 9% of baseline) was also abolished in the presence of atractyloside (morphine + atract: 57 ± 6%; P < 0.001 versus morphine group). The DADLE 100 nmol-induced enhanced recovery of FoC60 (81 ± 4% of baseline) was abolished in the presence of atractyloside (DADLE + atract: 44 ± 7%; P < 0.001 versus DADLE 100 group; Figure 2).
Atractyloside alone has no significant effect on FoC60, as compared with the control group (FoC60: 51 ± 5% of baseline; P = 0.76 versus control group; Figure 2).
Discussion
The present study showed that: (1) administration of morphine and DADLE, during the first minutes of reoxygenation, induced pharmacological PostC of isolated human myocardium; (2) the inhibition of mPTP opening was involved in morphine and DADLE-induced myocardial PostC.
Morphine-induced postconditioning
Morphine is daily used in the management of pain during myocardial ischemia and in the postoperative period of cardiac surgery. Morphine is a non-selective opioid receptor agonist binding to all subtypes of opioid receptors (delta, mu, kappa), but with a higher affinity for mu receptors. This high affinity for mu receptors could be constitute a limitation, since, mu opioid receptors’ stimulation determined cardiovascular and respiratory adverse effects. 24 It has been shown, in vivo, that morphine administered at the reperfusion, in rat (0.3 mg/kg), and in rabbit (5 mg/kg), significantly reduced myocardial infarct size. 9,12 In isolated rat heart, subjected to 30 min of ischemia and two hours of reperfusion, administration of morphine in a range dose of 1–30 μmol in early period of reperfusion, reduced the infarct volume. 5,7,13 Nevertheless, the doses used in these studies are far from those measured in clinical practice. 23 In the present study, the morphine's concentration used are comparable to that measured in the serum of patients. 23 Importantly, the present results strongly suggest that 15 min administration of morphine 0.5 μmol at the onset of reoxygenation could induced postC of human myocardium in vitro. The beneficial effect of morphine-induced PostC was observed on the recovery of FoC at the end of the reoxygenation period.
Concentration relationship of DADLE postconditioning
DADLE may be a promising synthetic molecule capable to induce hypometabolism state such as hibernation induce trigger, to improve the preservation of solid organs (heart, brain, kidney, liver) 15 and, if administered before ischemia, to protect organs against ischemic–reperfusion injury. 25–27 DADLE is a selective delta opioid agonist, with an affinity nine-fold greater than that of morphine. It also binds to mu receptors with an affinity comparable to that of morphine. In the current study, 15 min administration of DADLE 50 and 100 nmol at the onset of reoxygenation enhanced the recovery of FoC60 as compared with control group suggesting that DADLE induced PostC of human myocardium, in vitro. Interestingly, the present results showed that the cardioprotective effects of DADLE (50 and 100 nmol) induced PostC was comparable to that of morphine-induced PostC. Our results suggested that a lower dose of DADLE could be necessary to induce protection seeing its high affinity for delta receptors. Moreover, opioid side-effects, determined in particularly by mu opioid receptors’ stimulation, are dose-dependent so, we can then assume that DADLE could have fewer side-effects as compared with a non-selective opioid receptor agonist, such as morphine. Importantly, DADLE has a favorable pharmacokinetic data for its short half-life because is quickly metabolized by endopeptidases and for this reason is free from late complication. 28 Bell et al. 16 showed that DADLE 10 nmol preconditioned human atrial trabeculae against hypoxia reoxygenation. In the present study, DADLE 10 nmol administered in the early reoxygenation period had no effect on the recovery of FoC60, suggesting that a higher concentration of DADLE could be required to trigger pharmacological PostC. Thus, in isolated rabbit hearts, the concentration of DADLE able to induce PC, failed to induce PostC. 29 Taken together, these results suggest that a higher concentration of DADLE could be required to trigger myocardial PostC as compared with the concentration required to trigger PC. We cannot rule out the hypothesis that increasing the dose of DADLE (from 10 to 50 nmol) results in activation of mu and kappa subtypes of opioid receptors in addition to the delta subtype. Thus, Zatta et al. 6 showed that both mu and delta opioid receptors were involved in ischemic PostC of rat heart. Moreover, Wong et al. 30 showed that delta and kappa opioid receptors mediate ischemic PostC and PostC by remifentanil, in rat in vivo.
Involvement of mitochondrial permeability transition pore
Mechanisms involved in morphine- and DADLE-induced cardioprotection are poorly documented. A growing body of evidences suggests that mitochondrion is a major component of cellular cardioprotective pathways. Although the role of mitochondrial adenosine triphosphate-sensitive potassium channels in DADLE-induced PC has been demonstrated. 16 It has been shown, in isolated rat heart, that inhibition of mPTP mediated morphine-induced PostC. 5,7 In addition, Kim et al. 7 suggested that this inhibition was dependent on the delta(1) opioid receptors in morphine-induced PostC. The key role of mPTP in cardioprotection in human myocardium has been established by Yellon's group, 20 showing that inhibition of mPTP by cyclosporine A administered at the onset of reoxygenation protects human myocardium against lethal hypoxia–reoxygenation injury, in vitro. This suggests that, in the human heart in vitro, the mPTP is a viable target for cardioprotection. 20 Nevertheless, its role in morphine and DADLE-induced cardioprotection of human heart has never been investigated. Our results showed that morphine and DADLE-induced PostC were abolished by mPTP opening (with atractyloside), at the onset of reoxygenation, suggesting that both morphine and DADLE administration in first minutes of reoxygenation prevents mPTP opening. The current study suggested that likely, in human myocardium in vitro, morphine and DADLE-induced PostC via the inhibition of mPTP in early reoxygenation period.
Several limits must be considered in the interpretation of the present results. First, the effects of anesthetic drugs, 3,31 diseases and treatments received by the patients, before obtaining atrial appendages cannot be ruled out. On the other hand, our study included a control group equally affected by all these potentially confounding factors, and representative of population, that could have benefits from this type of cardioprotection strategy. Second, studies in isolated human right atrial myocardium must be performed at 34°C to obtain a stable isometric contraction during several hours. However, hypothermia is routinely used in cardiac surgery and mild hypothermia is a protective strategy during cardiopulmonary resuscitation. 32 Third, actually no data are available on the clinical pharmacokinetics and pharmacodynamics of DADLE. Fourth, our data strongly suggest a key role for mPTP inhibition in morphine and DADLE-induced PostC. Nevertheless, it has been reported that atractyloside not only opens mPTP but also inhibits adenosine diphosphate transport by inhibition of adenine nucleotide translocase, therefore limiting oxidative phosphorylation. 33 As such, it would be difficult to differentiate the effects of atractyloside on mPTP opening versus loss of energy production as causative factors in attenuated protection. Our results also require qualification because the actions of morphine and DADLE with or without atractyloside pretreatment on mPTP channel activity in isolated mitochondria were not investigated. Fifth, the use of human right atrial trabeculae is easily accessible, relatively disease free and eliminates inter species differences. However, for ethical reason is not possible to obtain ventricular tissue. Bell et al. 16 have shown that atrium and ventricle have a similar copy number of δ and μ receptors, even if they have different structural and mechanical features.
In conclusion, administration of morphine and DADLE, in early reoxygenation, induced PostC of human myocardium in vitro, at least in part, through the inhibition of mPTP opening. Similar results have been reported in brain exposed to ischemia–reperfusion injury. 34 Because DADLE has a short half-life, it could be proposed as protective agent against ischemia–reperfusion injury. Otherwise, further studies will be required to examine if this PostC effect of DADLE could be proposed in clinical setting.
Footnotes
ACKNOWLEDGEMENTS
Financial support was provided solely from institutional and/or departmental sources.