
Abstract
The effects of carvacrol on tracheal responsiveness (TR) to methacholine and ovalbumin (OA), serum nitric oxide (NO) concentration, total and differential white blood cells (WBC) in blood of sensitized guinea pigs were examined. Five groups of guinea pigs sensitized to OA were given drinking water alone (group S), drinking water containing three concentrations of carvacrol (40, 80 and 160 μg/mL) and dexamethasone (50 μg/mL). TR to methacholine and OA, serum NO concentration, total and differential WBC in blood of sensitized and control guinea pigs were measured (n = 6, for each group). TR to methacholine and OA, serum level of NO and nitrite, total WBC, eosinophil and neutrophil counts were increased but lymphocyte decreased in group S compared with control group (P < 0.01 for NO and nitrite and P < 0.001 for other cases). Treatment of S animals with dexamethasone and two higher concentrations of carvacrol significantly improved all measured parameters except TR to OA in treated group with dexamethasone (P < 0.05 to P < 0.001). Treatment of S animals with low concentration of carvacrol also improved TR to methacholine and OA, total WBC count and nitrite level (P < 0.05 to P < 0.001). The effects of two higher concentrations of carvacrol on TR, NO and nitrite and the effects of its highest concentration on total and differential WBC count were significantly higher than those of dexamethasone (P < 0.05 to P < 0.001). In addition, the effects of highest concentration of carvacrol on all parameters and its medium concentration on some parameters were significantly higher than its low concentration (P < 0.05 to P < 0.001). These results showed a preventive effect of carvacrol on tracheal responsiveness, serum level of NO and nitrite, total and differential WBC in the blood of sensitized guinea pigs which was equal or even more potent than dexamethasone at used concentrations.
Introduction
One constituent of several medicinal plants including Zataria multiflora Boiss is carvacrol or cymophenol, C6H3CH3(OH)(C3H7). 1 For all plants containing carvacrol therapeutic effects on respiratory disease were described.1–3
Different pharmacological effects were shown for carva-crol including antibacterial4–7 and anticandidacies. 8 The effect of carvacrol on DNA bindinding,9,10 genotoxicity, 11 chromatid exchanges, 12 gene expression in Bacillus cereus 13 anticancer 14 and apoptosis 15 were also observed. The anti-inflammatory16–18 and antioxidant19,20 effects of carvacrol were also demonstrated.
All plants containing carvacrol showed relaxant effect on smooth muscles of different organs including trachea.21–26 It was also documented that the relaxant effect of Carum copticum on tracheal smooth muscle is mainly due to its fraction 2, which is suggested to be carvacrol. 27 The relaxant effect of carvacrol on tracheal chains was also observed. 28 The hypotensive effects of carvacrol on the blood pressure of normotensive rats was also shown which could be due to it relaxant effect on blood vesicles. 29 Inhibitory effects of carvacrol on 7,12-dimethylbenz(α)anthracene-induced pulmonary tumorigenesis in rats was also shown. 30
The main characteristic feature of asthma is airway hyper responsiveness (AHR) to many stimuli 31 which is due to inflammatory disorder of the airway. 32 Various inflammatory cells, including eosinophils are involved in the patho-genesis of airway inflammation in asthma. 33 Reactive oxygen species secreted by inflammatory cells can modulate contractility of airway smooth muscle. 34
Nitric oxide produced by endothelial nitric oxide syn-thase can induce plasma extravasation and lung edema. High concentrations of inducible NOS (iNOS)-derived NO can increase vascular permeability, mucus hypersecretion, inflammatory cell infiltration, epithelial cell damage and perpetuation of the Th2-mediated inflammatory response in the airways to contribute in asthma physiopathology.35,36 Previous studies have noted increased nitrite, nitrate and nitrotyrosine concentrations in the exhaled breath condensate of asthmatic children 37 and in the epithelial lining fluid (ELF) of adults with mild-to-moderate and severe asthma. 38 Inducible NOS is inhibited by glucocorticoids, but selective inhibitors of this enzyme may have therapeutic potential in asthma.35,39
With regard to existence of airway inflammation in asthma and due to anti-inflammatory property of carvacrol, in the present study the protective effect of oral carvacrol on tracheal responsiveness, serum NO concentration and WBC count in blood of sensitized guinea pigs was examined.
Material and methods
Animal sensitization and animal groups
Animals were sensitized to OA according the method described previously.40-42 Briefly, guinea pigs were sensitized to intraperitoneally injection of 10 mg OA (Sigma Chemical Ltd, Dorset, UK) and 100 mg Al(OH)3 dissolved in 1 mL saline in day one and 2 mg OA and 100 mg Al(OH)3 dissolved in 1 mL saline as a booster dose in day 7. Sensitized animals were exposed to an aerosol of 4% OA from day 14, for 18 ± 1 d, five min daily (Figure 1). The dimensions of closed chamber used for aerosol admonition were 30 × 20 × 20 cm. Control animals were treated similarly but saline was used instead of OA solution. The study was approved by the ethical committee of the Mashhad University of Medical Sciences.
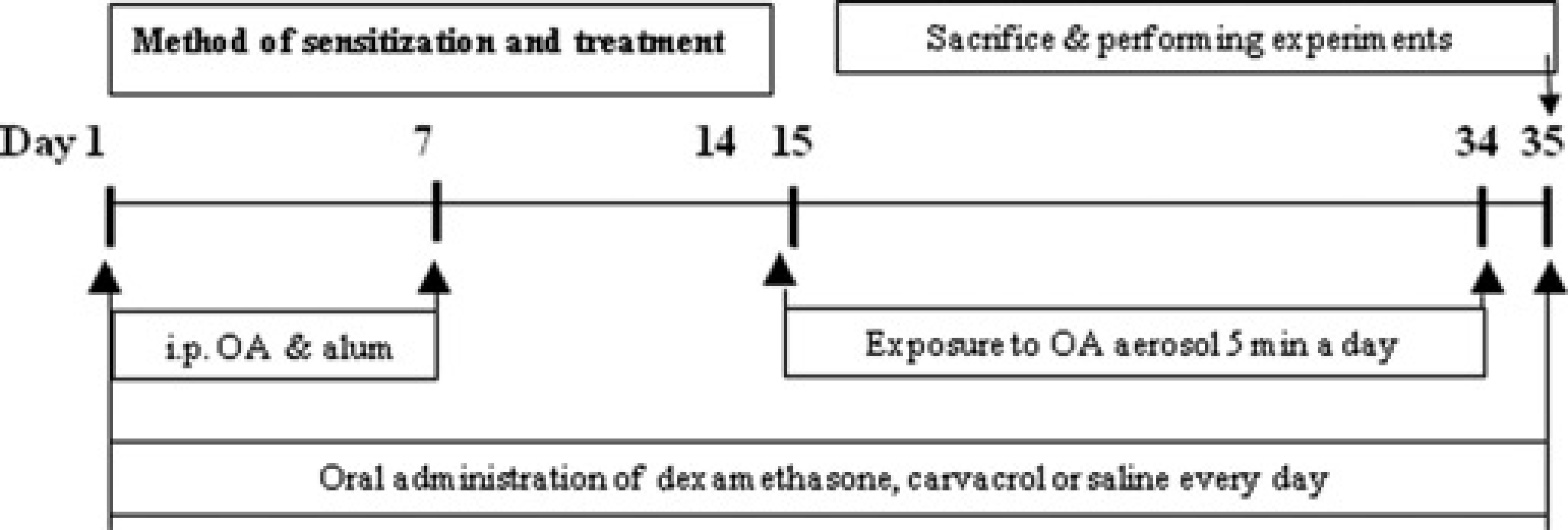
Method of sensitization and administration of cavacrol, dexametha-sone or saline during sensitization period (for each group, n = 6)
The study was performed in control animals (group C, which were given drinking water alone) and five groups of sensitized animals which were given drinking water alone (group S, an animal model of asthma) or drinking water containing treatment agents during sensitization period, from the beginning of OA injection to the end of administration of aerosolized OA (for 35 d), (Figure 1) as follows (n = 6 for each group);
50 μg/mL dexamethasone (group S
40 μg/mL carvacrol (group S
80 μg/mL carvacrol (group S + C2)
160 μg/mL carvacrol (group S + C3)
The volume of drinking water consumed by animals was checked regularly throughout the study period which was 100 to 150 mL in each guinea pig/day. There was not significant difference between animals of different groups in this regard.
Tissue preparation
Guinea pigs were sacrificed by a blow on the neck at the end of sensitization period which was the end of treatment in treated groups (day 35), and trachea was removed. One tra-cheal chain was prepared in each animal by cutting trachea into 10 rings (each containing 2–3 cartilaginous rings), cutting cartilage opposite the trachealis muscle and sutured together to form a tracheal chain according previous studied.42,43
Tissue was then suspended in a 10 mL organ bath (Schuler organ bath type 809, March-Hugstetten, Germany) containing Krebs–Henseliet solution of the following composition (mmol/L): NaCl 120, NaHCO3 25, MgSO4 0.5, KH2PO4 1.2, KCl 4.72, CaCl2 2.5 and dextrose 11. The Krebs solution was gassed with 95% O2 and 5% CO2 and maintained at 37°C. Tissue was suspended under isotonic tension of 1 g and allowed to equilibrate for at least one hour while it was washed with Krebs solution every 15 min.
Responses were measured using vernier control type 850 N sensor with sensitivity range: 0–20 g and resolution: 0.2 mm/turn (Hugo-Sachs Elektronik, Germany) and amplified with amplifier (ML/118 quadribridge amp, March-Hugstetten, Germany) and recorded on powerlab (ML-750, 4 channel recorder).
Assessment of tracheal response to methacholine
A cumulative log concentration–response curves of methacholine hydrochloride (Sigma Chemical Ltd, UK)-induced contraction of tracheal chain was obtained in each experiment as previously described. 42 Consecutive concentrations (including 10−7 to 10−5 mmol/L, dissolved in saline) were added every three minutes. The contraction due to each concentration was recorded at the end of three minutes. A concentration–response curve of methacholine was performed in tracheal chain of each studied animal by plotting the percentage of contraction of the tracheal smooth muscle due to each concentration of methacholine (in proportion to the maximum contraction obtained by its final concentration) against log concentration of methacho-line. The effect reached a plateau in all experiments.
From concentration–response curve in each experiment, the effective concentration of methacholine, causing 50% of maximum response (EC50) was determined using 50% of maximum response in Y-axis and measuring the dose of methacholine causing this response in X-axis. Contractility response to 10 μmol/L methacholine as the magnitude of contraction was also measured.
Measurement of tracheal response to OA
Tracheal response to 0.1% solution of OA (adding 0.25 mL of 4% OA solution to the 10 mL organ bath) was measured according to the previously described method. 42 After 15 min, tracheal smooth muscle contraction was measured and expressed as the proportion (in percentage) of contraction obtained by 100 (μmol/L methacholine. Contractility response to OA was also determined as maximum contractility response of tracheal smooth muscle to 0.1% solution of OA. The measurement of tracheal response to methacholine and OA was performed in random order.
Measurement of serum nitric oxide
A total of 5 mL peripheral blood was obtained immediately after sacrificing the animals and placed at room temperature for one hour. The samples were then centrifuged at 3500 × g at 4°C for 10 min. The supernatant was collected and immediately stored at 70°C until analysis. Serum NO concentration were determined by Nitric Oxide Calorimetric Assay kit (nitric oxide colorimetric assay kit k262-200, BioVision Research Products, Mountain View, USA) according to the manufacturer's instructions. Nitrate in the samples and standards were converted to nitrite by nitrate reductase and Griess reagent was added in the each well plate. Absorbance was determined at 540 nm. The concentration of total NO (nitrite
White blood cells count
After sacrificing and exposing the animals chest, 2 mL blood sample was taken by cardiac puncture and collected into test tube containing anticoagulant ethylendiaminetetraacetic acid. 42 Total white blood cell (WBC) was counted in duplicate in blood sample stained with Turk solution (1:10 dilution) using a hemocytometer (in a Burker chamber). The compositions of Turk solution were included; 1 mL of glacial acetic acid, 1 mL of Gentiac Vialet solution 1% and 100 mL distilled water.
Differential cell counts were done on thin slide, prepared with smearing blood sample, using Wright-Giemsa's stain. According to staining and morphological criteria, differential cell analysis was carried out under a light microscope by counting 100 cells, and the percentage of each cell type was calculated.
Statistical analysis
The data were quoted as mean ± SEM. According to the Kolmogorov–Smirnov test these data had normal distribution. The data of sensitized group were compared with control guinea pigs using unpaired ‘t’ test. The data of treated groups were also compared with sensitized guinea pigs using unpaired ‘t’ test. The data of three groups of animals treated with carvacrol were compared using unpaired one way analysis of varience with Tuky Kermar post hoc test. Significance was accepted at P < 0.05.
Results
Tracheal response to methacholine
Left ward shift in concentration response curve to metha-choline of group S compared with that of group C was observed but, the curves of treated groups with dexametha-sone and all concentrations of carvacrol were shifted to right compared with group S (Figure 2).
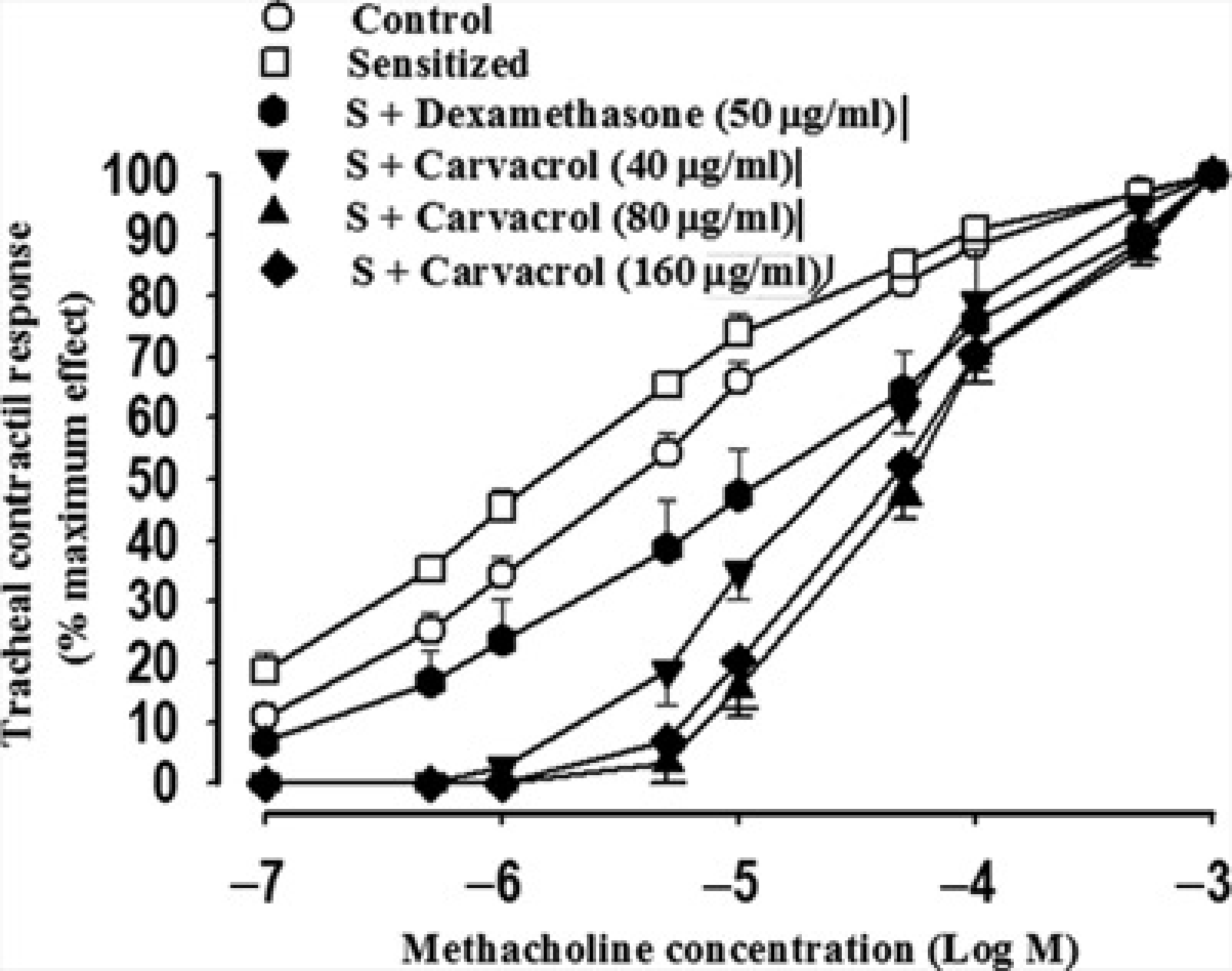
Cumulative log concentration-response curves of methacholine induced contraction of isolated trachea in control (C), sensitized (S), S treated with dexamethasone and three concentrations of carvavcrol (S + Carvacrol) guinea pigs (for each group, n = 6)
The mean value of EC50 methacoline in group S was significantly lower but contractility response to methacholine was non-significantly higher than group C (P < 0.001, Figure 3a). However, the mean value of EC50 in treated groups with all three concentrations of carvacrol and dexamethasone were significantly improved compared with the group S (P < 0.001 for all cases, Figure 3a). Contractility response to methacholine was also significantly decreased in treated groups with all three concentrations of carvacrol and dexamethasone (P < 0.05 to P < 0.001, Figure 3b).
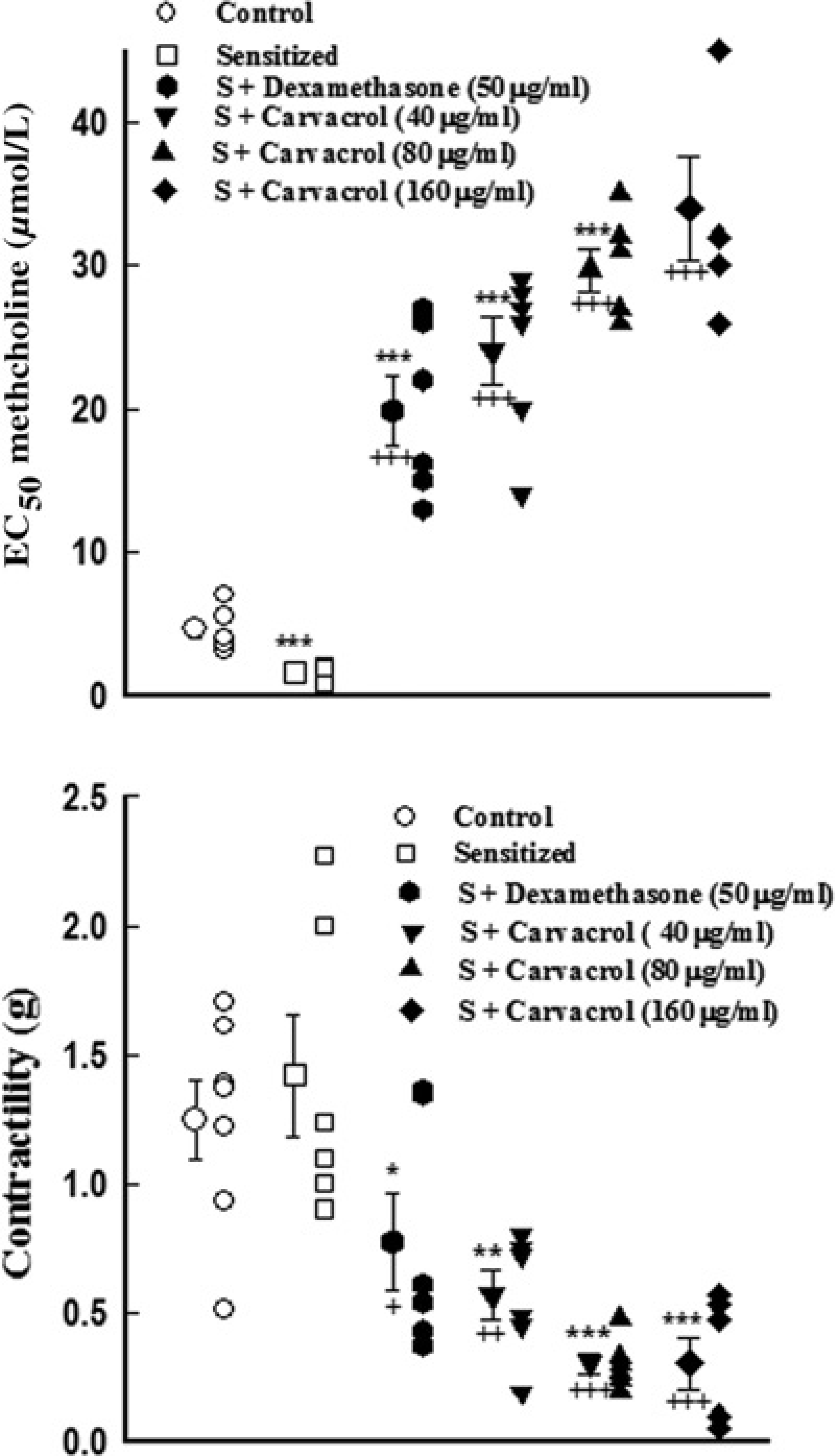
Individual values and mean ±
Tracheal response to ovalbumin
Tracheal response and maximum contractility response to OA in group S were significantly higher than group C (P < 0.001 and P < 0.01 respectively, Figure 4). Tracheal response to OA in treatment groups with all three concentrations of carvacrol were significantly improved compared with group S (P < 0.05 to P < 0.001, Figure 4a). Maximum contractility response to OA in treatment groups with two higher concentrations of carvacrol was also significantly lower than in group S (P < 0.05 and P < 0.01 for medium and high concentrations, Figure 4b).
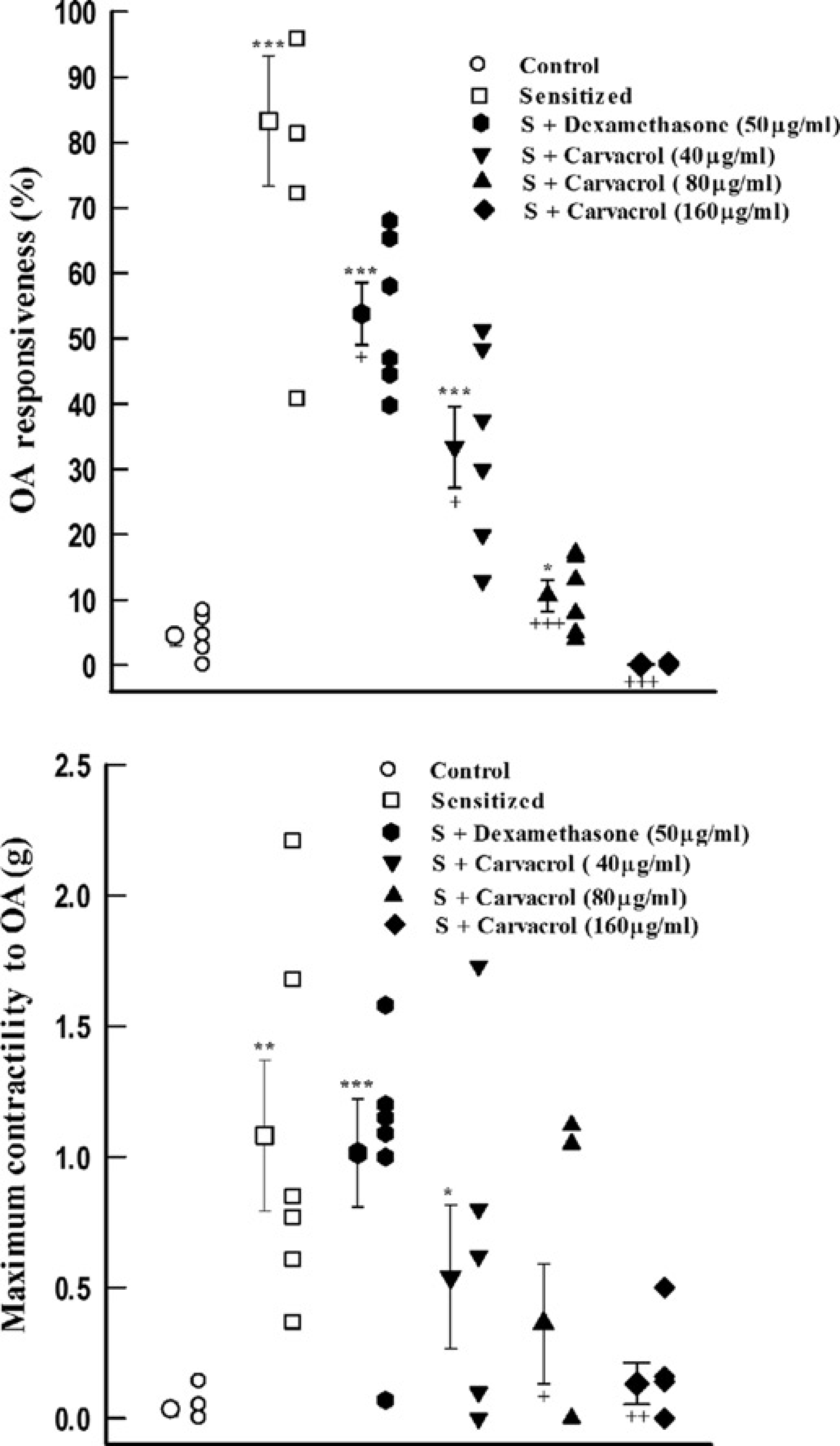
Individual values and mean ±
Serum NO and nitrite concentration
Serum concentration of NO and nitrite in group S were significantly higher than those of group C (P < 0.01 for both cases, Figure 5). Treatment of S animals with two higher concentrations of carvacrol (80 and 160 μg/mL) lead to significant reduction in serum concentration of NO and nitrite (P < 0.001 for all cases, Figure 5). Treatment with dexamethasone also caused significant reduction in serum concentration of NO and nitrite (P < 0.01 for NO and P < 0.05 for nitrite concentration, Figure 5).
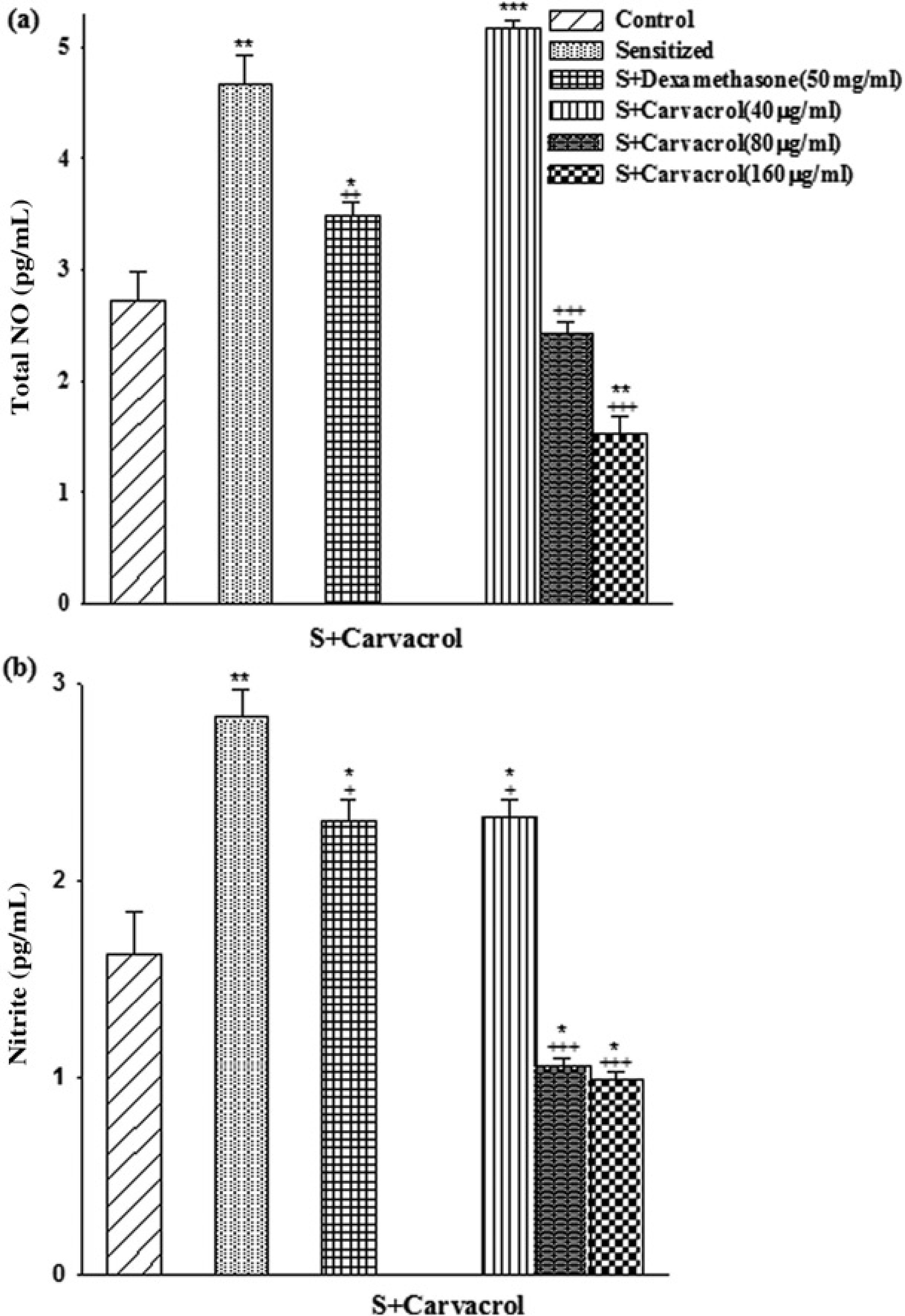
The levels of serum
Total and differential WBC counts
Total WBC, eosinophil and nutrophil counts were significantly higher but lymphocyte count was lower in group S compared with hose of group C (P < 0.001 for all, Figure 6). Treatment of S animals with two higher concentrations of carvacrol (80 and 160 μg/mL) and dexa-methazone caused significant improvement total WBC, eosinophil, nutrophil and lymphocyte counts (P < 0.05 to P < 0.00, Figure 6). However, treatment with only highest concentrations of carvacrol significantly reduced monocyte count (P < 0.001, Figure 6).
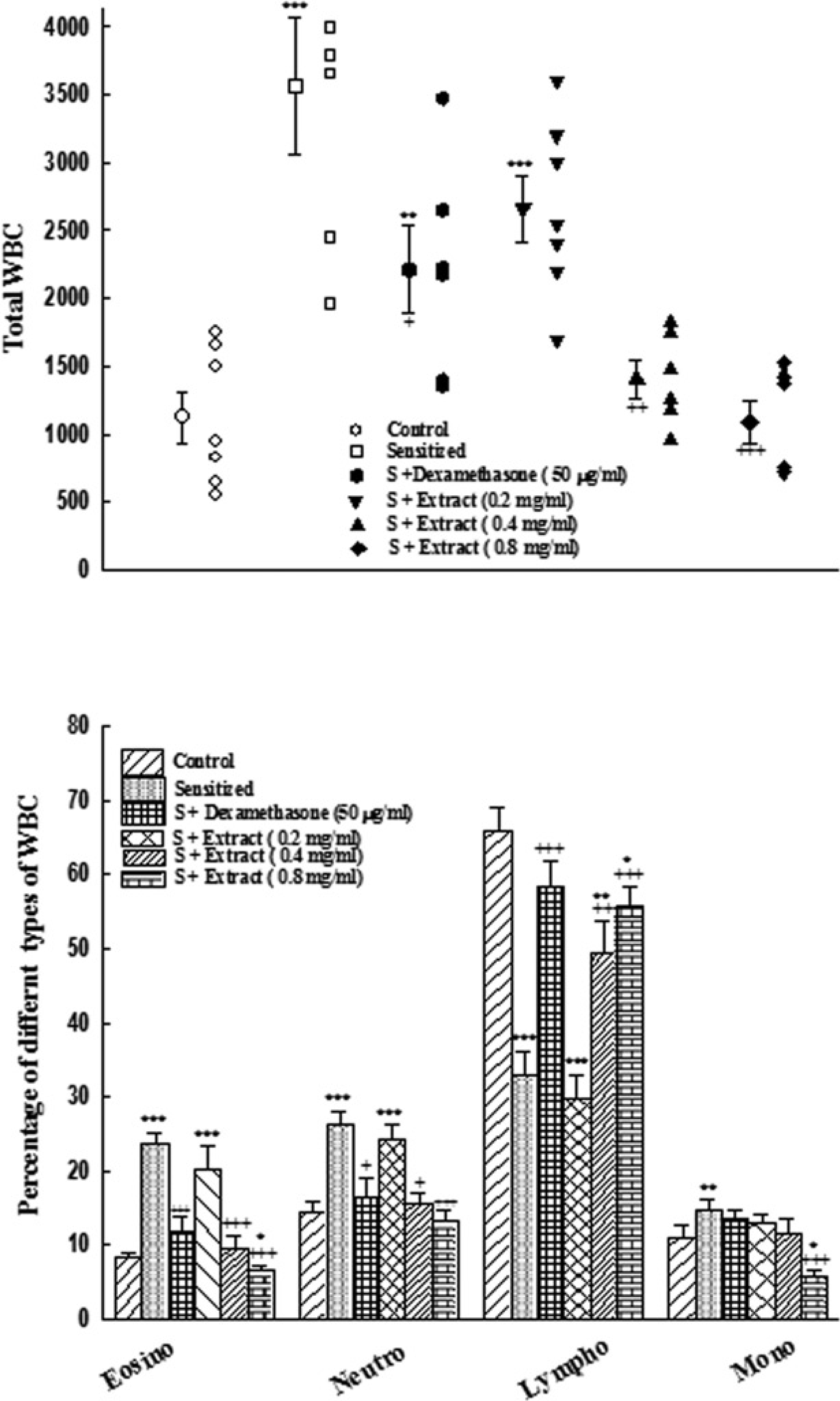
Individual values and mean ±
Differences between the effect of dexamethasone and carvacrol
The effects of two higher concentrations of carvacrol (80 and 160 μg/mL) on TR and contractility to methacholine, TR to OA, serum concentration of NO and nitrite concentration, total and differential WBC counts except monocytes were significantly higher than the effect of dexamethasone (P < 0.05–0.001, Table 1–3). The effects of low concentration of carvacrol (40 μg/mL) on eosinophil, nutrophil and lymphocyte were significantly lower than dexametha-sone (P < 0.05 for all cases, Table 3).
Values of tracheal response to methacholine (EC50) and Ovalbumin in control guinea pigs (C), sensitized animals (S), S treated with three concentrations of carvacrol (S + C1, S + C2 and S + C3) and dexaethasone (S + D), (for each group, n = 6)
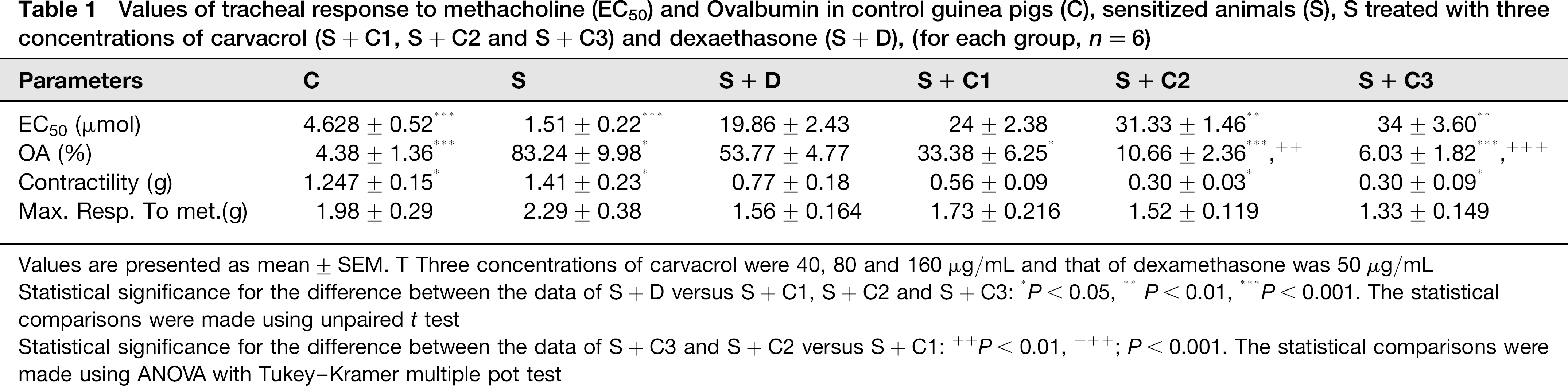
Values are presented as mean ± SEM. T Three concentrations of carvacrol were 40, 80 and 160 μg/mL and that of dexamethasone was 50 μg/mL Statistical significance for the difference between the data of S + D versus S + C1, S + C2 and S + C3:
P < 0.05,
P < 0.01,
P < 0.001. The statistical comparisons were made using unpaired t test
Statistical significance for the difference between the data of S + C3 and S + C2 versus S + C1:
P < 0.01,
; P < 0.001. The statistical comparisons were made using ANOVA with Tukey-Kramer multiple pot test
Values of serum NO2 + NO3 and NO3 concentration (pg/mL) of control guinea pigs (C), sensitized animals (S), S treated with three concentrations of carvacrol (S + C1, S + C2 and S + C3) and dexamethasone (S + D), (for each group, n = 6)
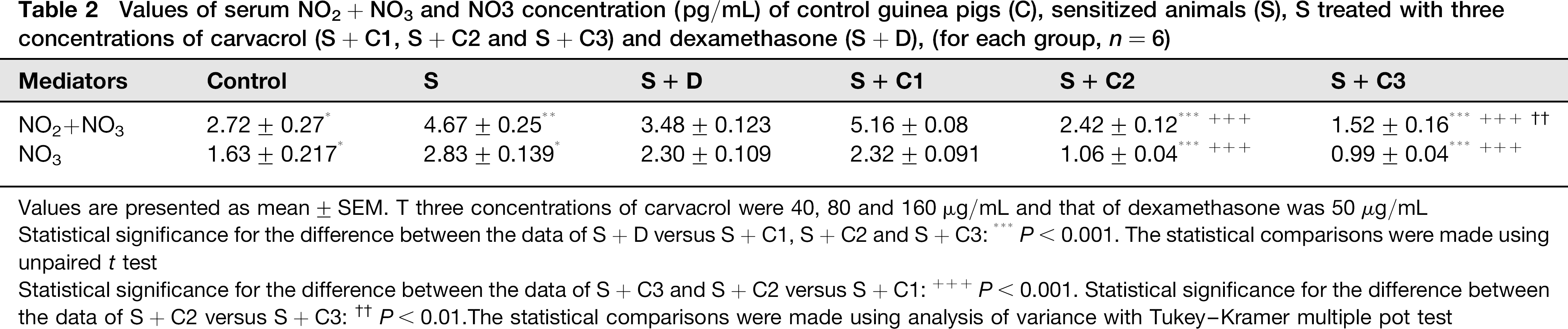
Values are presented as mean ± SEM. T three concentrations of carvacrol were 40, 80 and 160 μg/mL and that of dexamethasone was 50 μg/mL Statistical significance for the difference between the data of S + D versus S + C1, S + C2 and S + C3:
P < 0.001. The statistical comparisons were made using unpaired t test
Statistical significance for the difference between the data of S + C3 and S + C2 versus S + C1:
P < 0.001. Statistical significance for the difference between the data of S + C2 versus S + C3:
P < 0.01 The statistical comparisons were made using analysis of variance with Tukey-Kramer multiple pot test
Values of blood total and differential WBC count in control guinea pigs (C), sensitized animals (S), S treated with three concentrations of carvacrol (S + C1, S + C2 and S + C3) and dexamethasone (S + D), (for each group, n + 6)
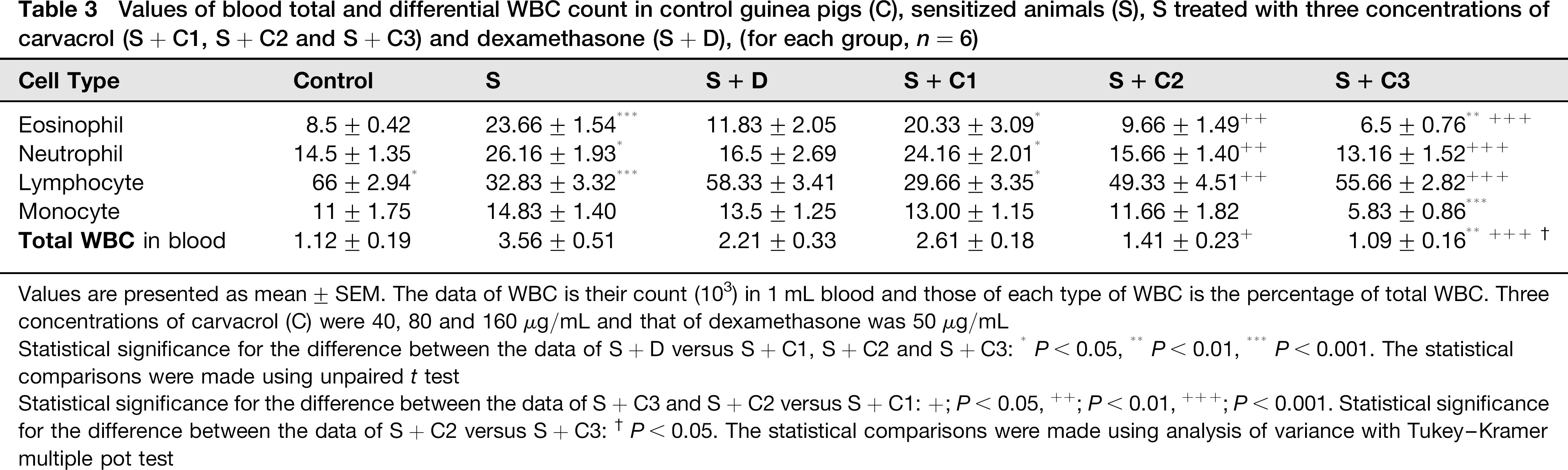
Values are presented as mean ± SEM. The data of WBC is their count (103) in 1 mL blood and those of each type of WBC is the percentage of total WBC. Three concentrations of carvacrol (C) were 40, 80 and 160 μg/mL and that of dexamethasone was 50 μg/mL
Statistical significance for the difference between the data of S + D versus S + C1, S + C2 and S + C3:
P < 0.05,
P < 0.01,
P < 0.001. The statistical comparisons were made using unpaired t test
Statistical significance for the difference between the data of S + C3 and S + C2 versus S + C1: +; P < 0.05,
P < 0.01,
; P < 0.001. Statistical significance for the difference between the data of S + C2 versus S + C3:
P < 0.05. The statistical comparisons were made using analysis of variance with Tukey-Kramer multiple pot test
Differences between three concentrations of carvacrol
The effects of two higher concentrations of carvacrol (80 and 160 μg/mL) on TR to methacholine and OA, serum concentration of NO and nitrite, eosinophil, nutrophil and total WBC counts were significantly higher than the effects of its low concentration (P < 0.05–P < 0.001, Table 1–3).
Discussion
In the present study the effect of carvacrol, the constituent of different medicinal plants including Z. multiflora and Tymus volgaris on tracheal responsiveness, serum NO concentration, total and differential WBC count in blood of sensitized guinea pigs was examined.
Dexamethasone and all concentrations of carvacrol showed concentration-dependent protective effect on increased tracheal responsiveness to methacholine and OA as well as total WBC count in sensitized guinea pigs. Treatment of sensitized animals with two higher concentrations of carvacrol and dexamethasone also caused significant improvements in serum concentration of NO and ntrite as well as eosinophil, nutophil and lymphocyte counts. Monocyte count also decreased in treated sensitized animals with highest concentration of carvacrol.
The main pathological feature of asthma is airway inflammation and prophylactic drugs used in the treatment of this disease should reduce airway inflammation. The preventive effect of carvacrol, one of the main constituent of Z. multiflora, on tracheal responsiveness is perhaps due to its suppressing effect on the airway inflammation in sensitized animals.
In sensitized animals treated with carvacrol the serum concentration of total NO and nitrite were also decreased which may suggest its antioxidant effect. Increased nitrite, nitrate and nitrotyrosine concentrations in the exhaled breath condensate of asthmatic children 37 and in the epithelial lining fluid (ELF) of adults 39 indicate the role of this agents in pathophysiology of asthma. Inhibition of iNOS by glucocorticoids, and selective inhibitors of this enzyme in asthma 35,39 support the anti-inflammatory effect of carvacrol observed in the present study.
Treatment of sensitized animals with carvacrol also leads to reduction of total and differential WBC count except lymphocyte percent which increased in treatment groups. These results are further evidence indicating antiinflammatory effect of carvacrol. Our previous study also showed an improvement of total and differential WBC count in sensitized guinea pigs treated with an antiinflammatory drug 42 which support the results of the present study. The decreased percentage of lymphocytes in sensitized animals was improved in treated groups with dexamethasone and carvacrol similarly. However, the absolute lymphocyte count was increased in group S compared with group C (33% × 3560 = 1175 compared with 66% × 1120 = 739). However, absolute lymphocyte count was not changed in treated animals with dexamethasone (58% × 2210 = 1282) but treatment with carvacrol lead to concentration-response curve reduction in lymphocyte count (30% × 2610 = 7830, 49% × 1410 = 690 and 56 × 1090 = 610 for low, medium and high concentrations respectively).
The anti-inflammatory16–18 and antioxidant19,20 effects of carvacrol were demonstrated which support the observed effect of carvacrol on sensitized guinea pigs in the present study. Carvacrol also showed inhibitory effect on histamine (H1) receptor seen in our previous study 44 which can contribute to its anti-inflammatory effect and could support the results of the present study. The decreasing effect of car-vacrol on thromboxane A2 production in platelets was shown. 45 Carvacrol also prevents lipid peroxidation, hepatic cell damage, and protects the antioxidant system in DEN-induced hepatocellular carcinogenesis. 46 Significantly decrease in tumor necrosis factor-alpha concentration in pleural lavage, suppressing the recruitment of leukocytes and significant reduce in LPS-induced nitrite production in vitro was also shown for carvacrol. 47 The two later studies46,47 support the finding of present study.
The results of this study showed that treatment of sensitized animal with carvacrol lead to reduction of concentration of total NO and nitrite which may lead to reduction of lung inflammation in sensitized animals, which in turn caused decrease of tracheal responsiveness. In fact, reduction of total and differential WBC counts in sensitized animals treated with carvacrol, support its effect on inflammation. The inhibitory effect of carvacrol on histamine (H1) receptors 44 may also contribute on its effect on inflammation. However, to clarify the exact mechanism(s) of carvacrol its effect on other inflammatory pathway as well as on histological changes of the lung in sensitized animals should be evaluated in further studies.
The results also showed that the effects of lower concentration of carvacrol on all measured parameters were lower than its two higher concentrations. These results showed concentration dependent preventive effect of carvacrol on sensitized animals and could be regarded as further evidence of specific anti-inflammatory effect of this substance.
Although, the preventive effect of low concentration of carvacrol observed in the present study on sensitized animals was lower than that of dexamethasone, the effects of its two higher concentrations were higher than dexamethasone. These findings also confirmed anti-inflammatory effect of carvacrol in sensitized guinea pigs which was comparable or even greater than the effect of dexamethasone.
Our previous study showed a potent relaxant effect of the extract of other plant containing carvacrol (T. volgaris) 24 and carvacrol itself 28 on tracheal smooth muscle, stimulatory effect of the plant on ß2-adrnoceptors 48 and the inhibitory effect of the plant and carvacrol on histamine (H1) receptors. 44 In addition the inhibitory effect of crvacrol 49 and the extract of Z. multiflora 50 on muscrinic receptors of tracheal smooth muscel were also documented.
The results of the present study showed the improvement in tracheal responsiveness, serum concentration of total NO and nitrite as well as total and differential WBC count in sensitized guinea pigs treated with carvacrol. Based on the results of the present study together with other studies indicating anti-inflammatory and antioxidant effect for carva-crol and its relaxant effect on tracheal smooth muscle, this agent could have a therapeutic effect on inflammatory diseases such as asthma by causing both bronchodilation and reduction effect on lung inflammation. However further studies needed to evaluate the effect of carvacrol on asthmatic patients.
Conclusion
In conclusion, the results of this study showed a preventive effect of carvacrol on tracheal responsiveness, serum level of NO and nitrite, total and differential WBC in the blood of sensitized guinea pigs which was equal or even more potent than dexamethasone at used concentrations. These results indicate could be valuable in treatment of inflammatory diseases such as asthma.
Footnotes
Acknowledgements
This study was financially supported by Research Department of Mashhad University of Medical Sciences. This paper is the results of a part of PhD. thesis.