
Abstract
This study was carried out to assess the protective bone-sparing effect of carnitine with anti-inflammatory properties on chronic inflammation-induced bone loss in ovariectomised (OVX) rats. A total of 64 rats were divided into eight groups. Sixteen rats were sham-operated (SH) while the others were ovariectomised (OVX). (1) SH, (2) sham + inflammation (SHinf), (3) OVX, (4) ovariectomy + inflammation (OVXinf), (5) OVX + CAR1, (6) OVX + CAR2, (7) OVXinf + CAR1, (8) OVXinf + CAR2. After the ovariectomy surgery, all the groups (3, 4, 5, 6, 7, and 8) were allowed to recover for two months. Sixty days after the OVX, inflammation was induced by subcutaneous injections of talc in groups 2, 4, 7, and 8. Group 5 and 7 were given 50 mg/kg CAR; Group 6 and 8 were given 100 mg/kg CAR from the 60th to the 80th day. Serum levels of TNF-α, IL-1, IL-6, OP, and OC were assessed to determine inflammation and to evaluate osteoblastic activity. Bone mineral density (BMD) was assessed by dual energy X-ray absorptiometry in femur bones of rats. Carnitine administration was able to restore BMD up to values measured in both the OVX and the SH animals. The serum levels of TNF-α, IL-1β, and IL-6 were increased significantly in the OVXinf rats compared with the SH group. In OVX rats, inflammation which is evaluated by serum cytokine levels exacerbated this bone loss, as supported by values of BMD of the total femur. The two different doses of carnitine reduced bone loss and improved inflammatory biomarkers.
Introduction
The incidence of osteoporosis continues to increase in postmenopausal women and it is thought that there are over 200 million people with osteoporosis in the world. 1 Osteoporosis is characterized by a reduction in bone mass and it causes increased bone fragility and susceptibility to fractures. 2 Fractures due to osteoporosis affect about 40% of women and 13% of men in their lifetime. 3 Osteoporosis is a multifactorial disease and the pathophysiology is complex. 4 Many experimental studies are beginning to understand the pathogenesis of this condition and to develop new types of treatment.5,6 The main cause is aging-induced estrogen loss, although many factors other than sex hormones play a role in the development of osteoporosis.7,8 The relationship between estrogen and inflammatory cytokines was demonstrated by Compston. 9 The estrogen decreases bone resorption directly by inhibiting osteoclasts and indirectly by suppressing osteoblastic production of various proresorptive paracrine factors such as IL-1β, IL-6, and TNF-α.10,11 It may also inhibit the inflammatory reaction by decreasing the expression of specific markers. Thus, estrogen reduces the degree of inflammation and tissue damage.12–15 Estrogen replacement therapy (ERT) is highly effective in the prevention and treatment of osteoporosis in postmenopausal women. However, the use of ERT is associated with increases in the risks of breast cancer, cardiovascular disease, and stroke.16–18 Therefore, in recent years, the alternative and complementary medicines have been popular subjects of osteoporosis research.19–22 The similarities in pathophysiologic responses between the human and rat skeleton have made the rat a valuable model in osteoporosis research. Therefore, OVX rat is a useful model for osteoporosis since the progressive loss of bone matrix is similar to that in postmenopausal women with osteoporosis. 23 The inflammatory process, which mimics the inflammatory and oxidative status that occur with aging, is induced by administering subcutaneous magnesium silicate. 24 The inflammatory and oxidative status decrease energy production in mitochondria and increase acyl CoA in cell. Carnitine reacts with acyl group that accumulated in anoxic cells and it carries out of cell and reacts with acyl group and shuttles accumulated acyl groups out of the mitochondria. 25 Carnitine is an essential substance for energy metabolism. Main function of carnitine is to transport long-chain fatty acids for β-oxidation in the mitochondria. 26 As fatty acid oxidation provides an important part of energy for bone cells, carnitine may directly improve the metabolism of osteoblasts. 27 The positive effects of carnitine on osteoblasts have been shown in previous studies.28–30 In addition, L-carnitine is capable of restoring the age-related changes in the functions of inflammatory cells. Moreover, L-carnitine may play a protective role in the tissue destruction in inflammation by decreasing the superoxide anion production. 31
We hypothesized that carnitine has protective effect on bone metabolism in OVX model of osteoporosis and we performed this study to investigate the possible protective effect of carnitine on bone metabolism in an experimental OVX model of osteoporosis in which inflammation was induced by subcutaneous magnesium silicate to mimic the inflammation that occurs with aging.
Material and method
Chemicals
All agents and chemicals were of analytical grade and purchased from commercial suppliers. Talc powder (magnesium silicate) was purchased from Sigma (243604, Sigma Aldrich). This study was performed in the Pharmacology Laboratory at Ataturk University, Faculty of Medicine, and Department of Pharmacology.
Animals
A total of 64 female Wistar rats (6-month-old) weighing 220–250 g were maintained in individual cages in a temperature-controlled room (21℃) with a 12 h light/12 h dark cycle. The animal care and experimental protocols were approved by Experimental Animal Ethics Committee of the Ataturk University and were conducted in accordance with current legislation on animal experiments.
Experimental groups
After two weeks of adaptation period, 16 rats were sham-operated (SH, controls), while the 48 others underwent ovariectomy (OVX) under anesthesia with a thiopental sodium injection 20 mg/kg, intraperitoneally. After the OVX, the rats were given 25 mg/kg metamizol sodium as an analgesic for two days.
Experimental design
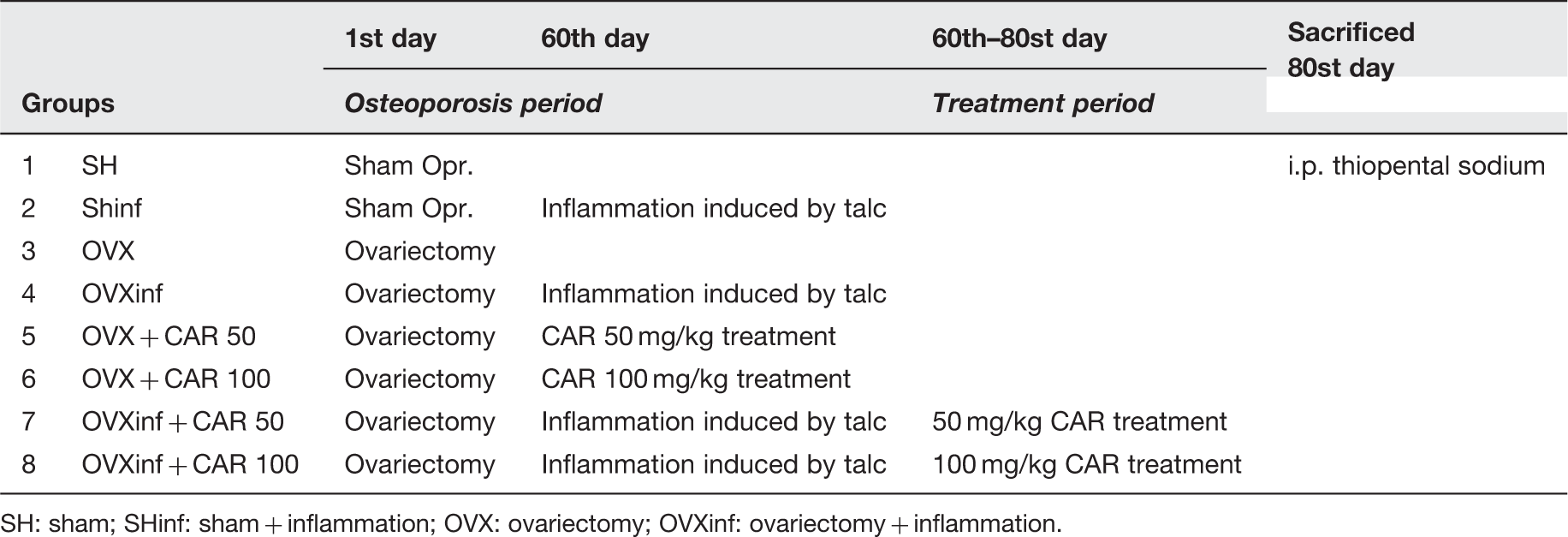
SH: sham; SHinf: sham + inflammation; OVX: ovariectomy; OVXinf: ovariectomy + inflammation.
Dual-energy X-ray absorptiometry (DEXA) estimations
The femur bones of the rats were evaluated in vitro after surgically removed. The bone mineral density (BMD) were analyzed by the dual-energy X-ray absorptiometry (DEXA) method using Discovery Wi (Hologic Inc., Bedford, MA, USA) equipped with appropriate software for bone assessment in small animals. The same researcher performed each measurement, and all analyses were done using the same region of interest (ROI) window size.
Markers for osteoblastic activity and markers of inflammation
Sera from the all the animal groups were separated and stored at −80℃ until they were thawed for the assay. IL-1β, IL-6, TNF-α, OP, and OC from each sample were measured with ELISA kits; eBioscience-bms630 (San Diego, CA, USA), Invitrogen- KRC0061 (Grand Island, USA), eBioscience-bms622 (San Diego, CA, U.S.A.), USCNK-E90899RA (Houston, USA), and USCNK-E90471RA (Houston, USA), respectively. The concentrations of OP and OC were measured with kits specifically designed for rats’ cytokines, and all measurements were performed according to the manufacturer’s instructions.
Statistical methods
To test for any difference among the groups, a one-way analysis of variance test (ANOVA) was conducted. Differences among the groups were obtained using the Duncan’s multiple range test option and were considered significant at P < 0.05. Correlation study was also examined in SPSS as bivariate Pearson correlation and P < 0.05 were considered significant. All data were expressed as mean ± standard deviation (SD) in each group.
Results
BMD
Femoral BMD (g/cm2) in the OVX group was markedly lower than in the sham-operated group (0.220 ± 0.01 and 0.250 ± 0.01, respectively; Figure 1). Inflammation exacerbated this osteoporosis in the OVX inf groups (0.206 ± 0.01), whereas the sham groups showed no effect (SHinf: 0.246 ± 0.01). Different doses of carnitine was able to restore BMD, up to values measured in both the OVX and the SH animals. Comparing the results for each therapy, the higher dose (100 mg/kg) of carnitine showed a greater increase than the lower dose of (50 mg/kg) carnitine. Both doses of carnitine were shown to decrease bone loss due to OVX and inflammation via talc aggravated.
Bone mineral density (BMD) values for all experimental groups. The means in the same column by the same letter are not significantly different, and the means in the same column by different letters demonstrate significant differences between the groups according to the Duncan test (α = 0.05). The results are the means ± SD. All statistical comparisons were performed within the same column. In the above table, the letter for the BMD level in the Shinf and OVX + CAR50, OVX + CAR100 and OVXinf + CAR100 is the same: “c,d”. This demonstrates that the values in these lines are not statistically different from each other. However, the lines with the letter “a” are statistically significant from the lines with the letters “b”, “c” and “d”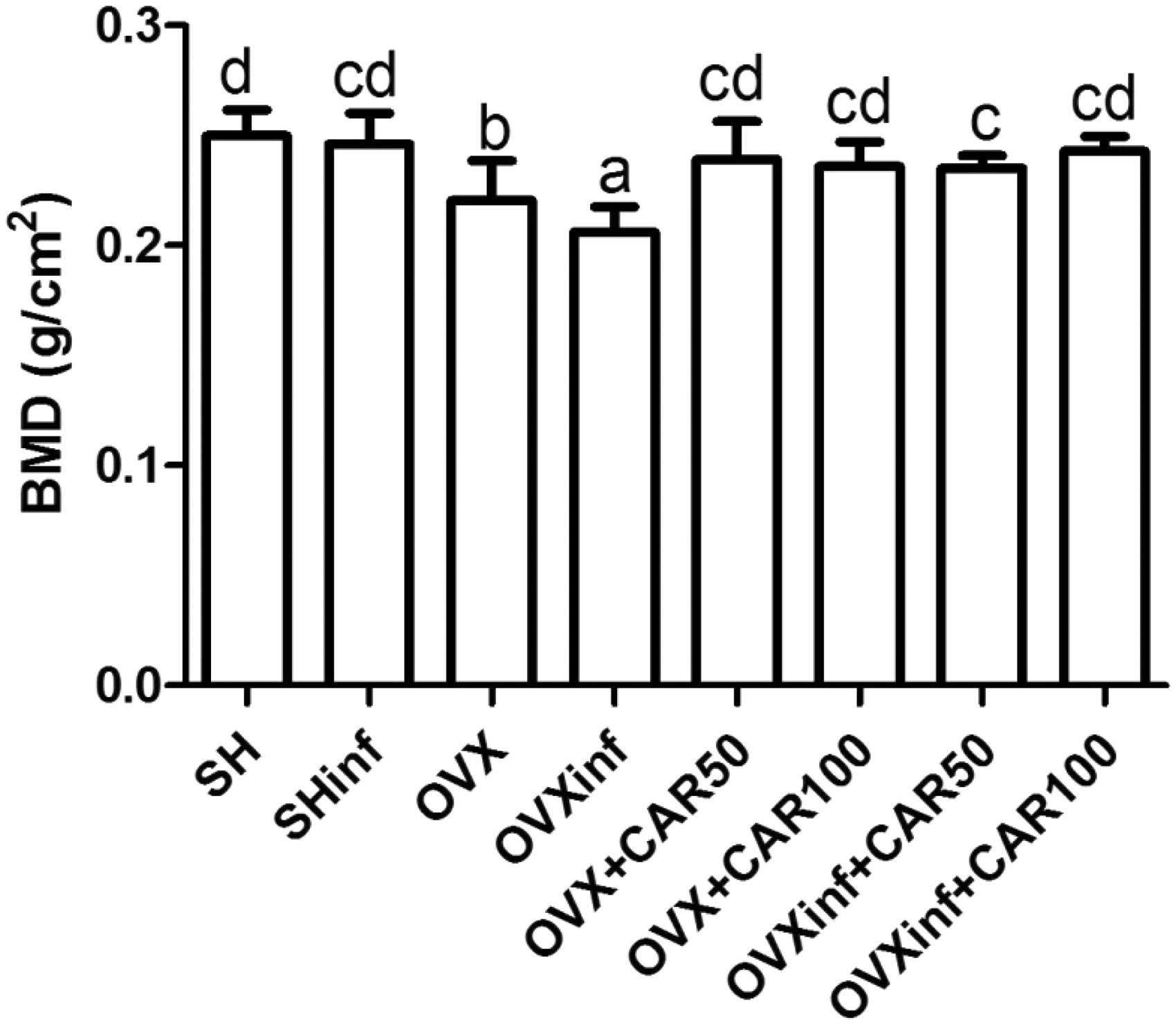
Bone turnover
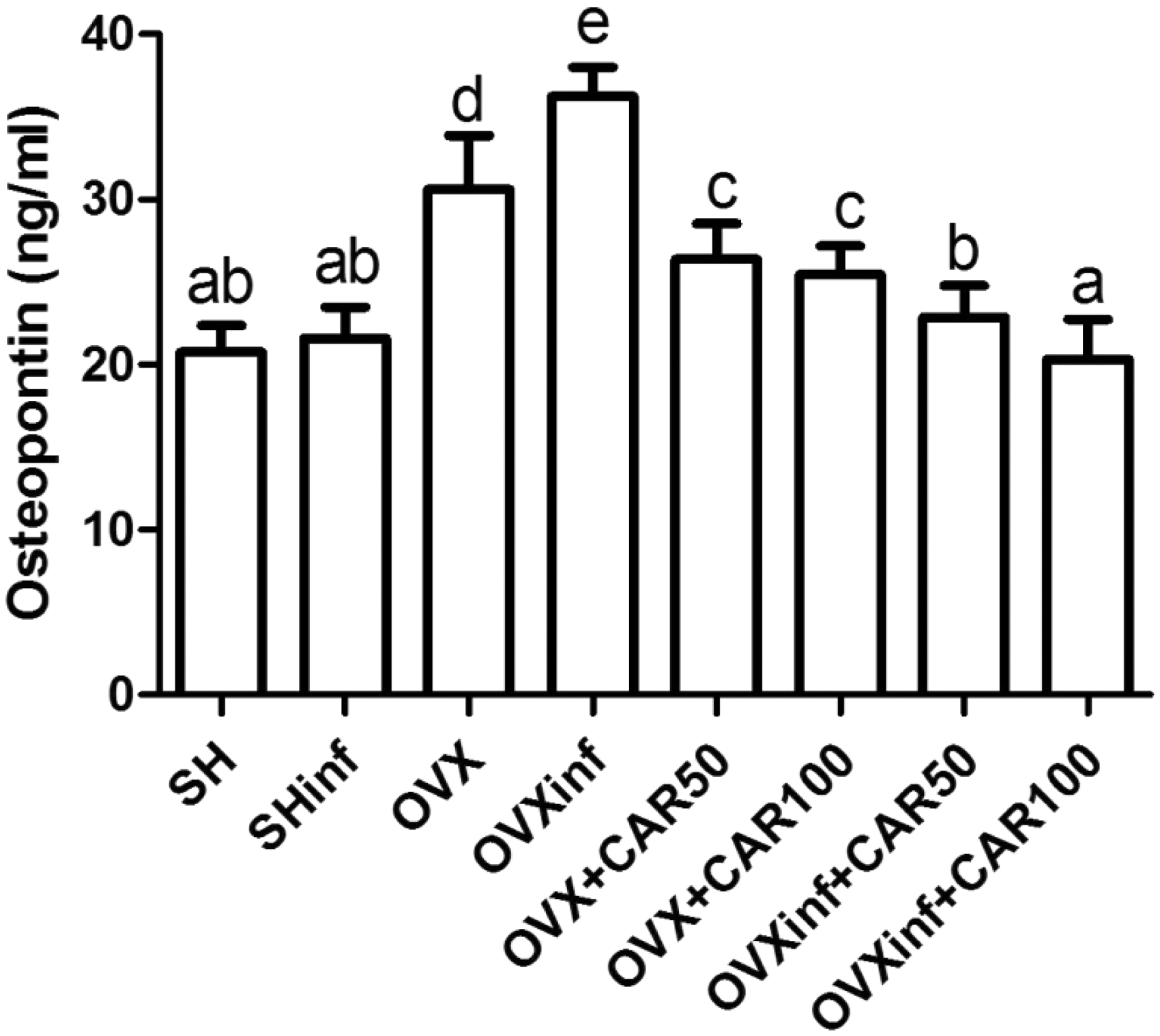
As compared to sham, serum markers of bone turnover (OC and OP) were significantly increased in the OVXinf groups (Figures 2 and 3) (P < 0.05). The OC and OP levels in the OVXinf groups exposed to the talc were significantly higher (62.27 ± 5.76 and 36.26 ± 1.77, respectively) than those in the sham group (34.39 ± 3.12 and 20.76 ± 1.62, respectively) (P < 0.05). Following CAR 50 or 100 mg/kg administrations, the levels of OC and OP decreased to 38.42 ± 5.94 and 22.89 ± 1.89 and to 33.54 ± 5.94 and 20.32 ± 2.44 in the OVXinf + CAR1 and the OVXinf + CAR2 groups, respectively. In addition, the increased level of the bone turnover markers in the OVX groups was recovered with CAR administration.
Mean serum osteocalcin levels for all experimental groups. The means in the same column by the same letter are not significantly different, and the means in the same column by different letters demonstrate significant differences between the groups according to the Duncan test (α = 0.05). The results are the means ± SD. All statistical comparisons were performed within the same column. In the above table, the letter for the osteocalcin level in the SH and Shinf is the same: “a”. This demonstrates that the values in these lines are not statistically different from each other. However, the lines with the letter “a” are statistically significant from the lines with the letters “b”, “c” and “d” Mean serum osteopontin levels for all experimental groups. The means in the same column by the same letter are not significantly different, and the means in the same column by different letters demonstrate significant differences between the groups according to the Duncan test (α = 0.05). The results are the means ± SD. All statistical comparisons were performed within the same column. In the above table, the letter for the osteopontin level in the SH and Shinf is the same: “a,b”. This demonstrates that the values in these lines are not statistically different from each other. However, the lines with the letter “a” are statistically significant from the lines with the letters “b”, “c” and “d”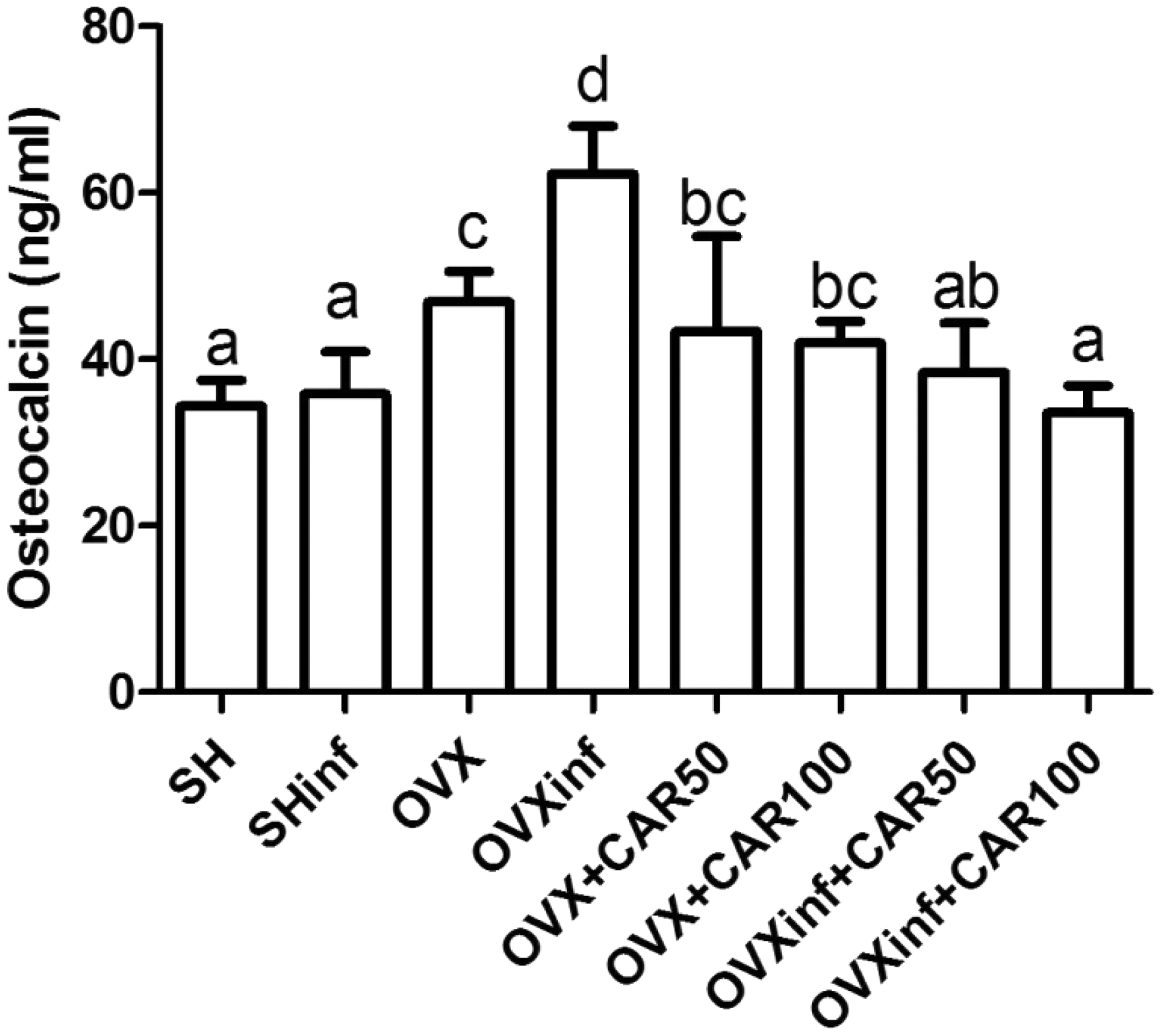
Markers of inflammation
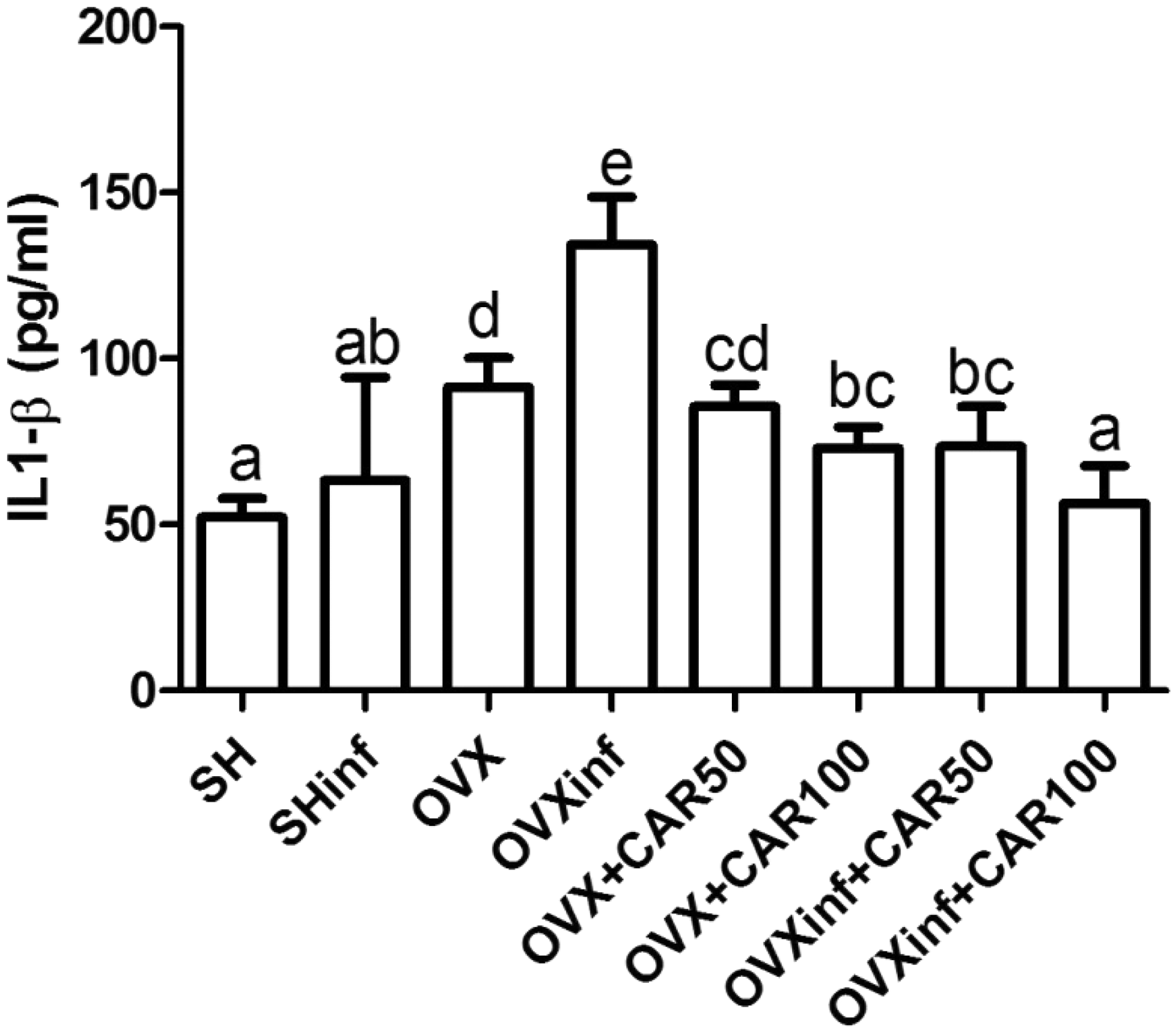
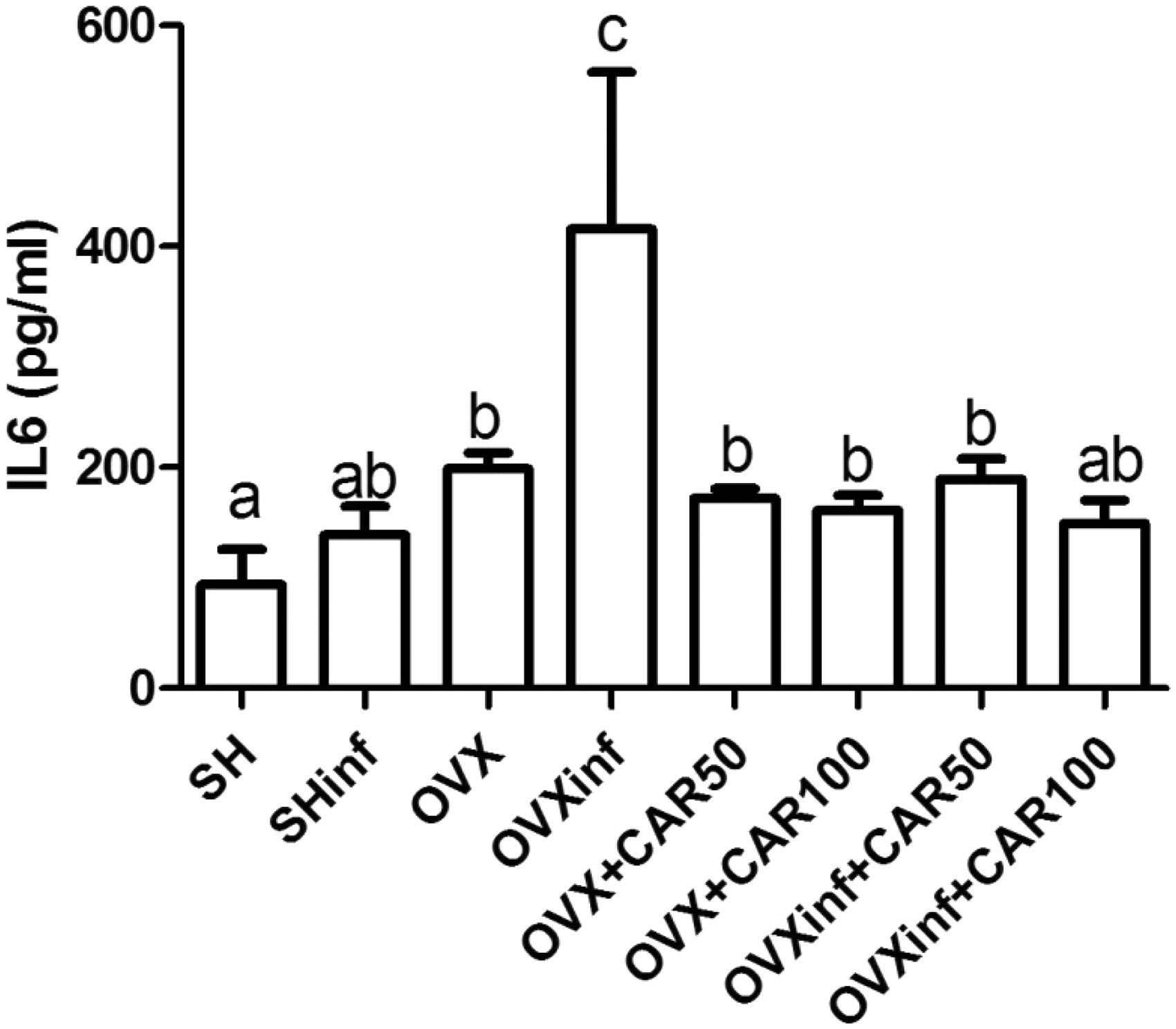
To determine talc-induced inflammation changes, we examined the proinflammatory cytokines in the serum by using ELISA (Figures 4–6). TNF-α, IL-1β, and IL-6 serum levels were significantly elevated in OVXinf (47.11 ± 5.87, 134.47 ± 14.25, and 415.97 ± 141.62, respectively) groups in comparison to SH group (24.07 ± 1.32, 52.28 ± 5.63, and 93.82 ± 31.99, respectively) (P < 0.05). The observed elevations of TNF-α, IL-1β, and IL-6 in the serum of the OVXinf rat groups decreased significantly in response to both CAR 50 mg/kg (33.35 ± 4.99, 73.59 ± 11.94, and 189.18 ± 187.74, respectively) and 100 mg/kg (25.02 ± 4.16, 56.35 ± 9.39, and 149.14 ± 21.30, respectively) compared with the OVXinf group (P < 0.05). Moreover, both CAR treatments decreased these serum cytokines in the OVX + CAR1 and the OVX + CAR2 rat group compared with the OVX only group. In correlation examination, it was also found that there was a negative correlation among BMD-TNF-α, BMD-IL-1 and BMD-IL-6, respectively (Figure 7) (P < 0.0001).
Mean serum TNF-α levels for all experimental groups. The means in the same column by the same letter are not significantly different, and the means in the same column by different letters demonstrate significant differences between the groups according to the Duncan test (α = 0.05). The results are the means ± SD. All statistical comparisons were performed within the same column. In the above table, the letter for the TNF-α level in the SH and OVXinf + CAR100 is the same: “a”. This demonstrates that the values in these lines are not statistically different from each other. However, the lines with the letter “a” are statistically significant from the lines with the letters “b”, “c”, and “d” Mean serum IL-1β levels for all experimental groups. The means in the same column by the same letter are not significantly different, and the means in the same column by different letters demonstrate significant differences between the groups according to the Duncan test (α = 0.05). The results are the means ± SD. All statistical comparisons were performed within the same column. In the above table, the letter for the IL-1β level in the SH and OVXinf + CAR100 is the same: “a”. This demonstrates that the values in these lines are not statistically different from each other. However, the lines with the letter “a” are statistically significant from the lines with the letters “b”, “c”, and “d” Mean serum IL-6 levels for all experimental groups. The means in the same column by the same letter are not significantly different, and the means in the same column by different letters demonstrate significant differences between the groups according to the Duncan test (α = 0.05). The results are the means ± SD. All statistical comparisons were performed within the same column. In the above table, the letter for the IL-6 level in the OVX + CAR50, OVX + CAR100, and OVXinf + CAR50 is the same: “b”. This demonstrates that the values in these lines are not statistically different from each other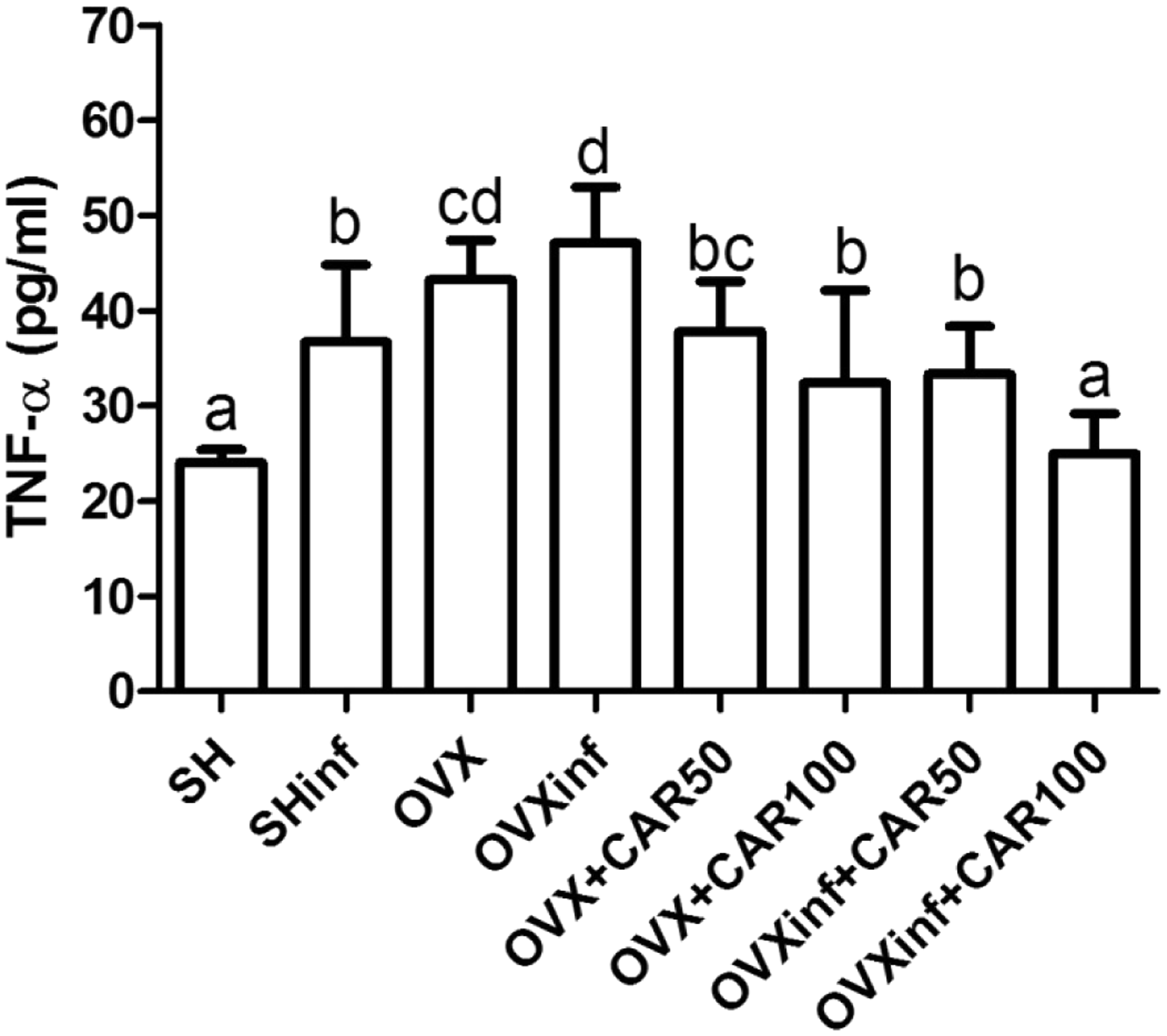
Discussion
The data obtained in the our study showed that CAR may play a positive role in bone health and may prevent bone loss induced by OVX/inflammation in a traditional experimental model of osteoporosis and an extensively used model of postmenopausal bone loss. The bone loss due to aging is associated not only to hormonal deficiency but also to impairment of bone turnover in the inflammatory status. 32 Estrogen has the ability to suppress the production of proinflammatory cytokines, and postmenopausal estrogen withdrawal associated with aging leads to inducing an unregulated chronic inflammatory process by increasing the local production of various cytokines. The OVX rat is the most widely used preclinical rodent model for postmenopausal osteoporosis. In our study, we investigated OVX-induced bone loss provoked by chronic inflammation which was induced with talc in rats.
BMD significantly decreased in the OVX group when compared to the sham group. The BMD levels enhanced the OVX group compared with the OVXinf group due to the inflammatory effect of magnesium silicate. Reduction in BMD may be linked by magnesium silicate-induced inflammation in the rat, which closely resembles the chronic inflammation-induced osteoporosis and chronic inflammatory bone loss seen in human. In contrast, OVX-induced osteoporotic rats given CAR showed a marked increase in BMD compared with the OVX group. Another approach to evaluate bone health involves the measurement of biochemical markers that are produced or released during bone turnover. OP and OC are sensitive markers of bone health which reflect the total body skeletal metabolism. Therefore, these markers may be useful in monitoring osteoporosis therapy and in assessing the rate at which bone loss occurs.
Circulating osteocalcin which is a bone-specific protein produced primarily by osteoblasts during bone formation has been used in clinical investigations as a marker of bone metabolism and has been used as a preliminary biomarker of the effectiveness of a given drug.33,34 Serum osteocalcin levels increase in OVX-induced osteoporosis in rats has been demonstrated in previous studies.35,36 Increased serum osteocalcin levels in OC in the OVX rats was higher than the sham control group, which was in accordance with previous studies. The highest level of OC level was found in the OVXinf group, and after administering CAR, the level of OC was recovered. This finding suggests that CAR has positive effects on osteoblast activation following magnesium silicate-induced inflammation in osteoporosis. Another biochemical marker of bone formation is OP, which has been implicated as an important factor in bone remodeling. A number of studies have shown that OP not only inhibits mineral deposition but also actively promotes its dissolution by physically blocking hydroxyapatite crystal growth.37–40 Our findings were similar to those of previous studies.41,42 As expected, serum osteopontin levels were significantly higher in ovariectomized rats when compared to SH group. Also, OVXinf group showed the highest OP levels. Due to the antioxidant/anti-inflammatory effect of CAR the inhibition of OP and OC was more significant in the OVX and OVXinf groups compared with the administered CAR groups. These findings suggest that CAR switched the bone formation/resorption balance in a positive direction in terms of osteoblastic activity. On the other hand, osteoporotic conditions involved in stimulating osteoblastic activity released many proinflammatory cytokines such as IL-1, IL-6 and TNF-α. These cytokines are thought to make an important contribution to stimulating bone resorption and suppressing bone formation.43–45 Proinflammatory cytokines, such as IL-1, IL-6, and TNF-α, are correlated negatively with changes in BMD.46,47 We demonstrated in this study that administration of CAR increased levels of BMD and decreased serum levels of IL-1, IL-6, and TNF-α. Those effects may also be related to antioxidant-anti-inflammatory properties of CAR. Our results were in accordance with previous studies that show antioxidant properties of carnitine.48,49 It has also been shown in previous studies that carnitine administration reduces cytokine levels in serum.50,51
Nowadays, the treatment of senile osteoporosis is designed in clinical state with various drugs such as bisphosphonates, parathyroid hormone, estrogen, selective estrogen receptor modulators, calcitonin, and vitamin D, which act by targeting the resorptive pathway and bone loss or by amplifying or mimicking steps in the anabolic pathway to build new and improved skeletons. However, whether these drugs are effective in helping patients with osteoporosis is unclear. It has been shown in several previous studies that CAR has many beneficial properties such as anti-inflammatory effects.52–55
In conclusion, our study showed that inflammation induced by magnesium silicate aggravated osteoporosis in OVX rats. CAR was able to demonstrate protective effects on bone loss in this rat model of OVX associated with inflammation probably by manipulating cytokines, which are parameters of inflammation. The preventive effect of CAR in the OVX and OVXinf models also depended on declining levels of OP and OC in the serum.
Finally, this information may illuminate the potent protective effect of carnitine in osteoporosis treatment and may lead to finding a novel therapeutic target for bone diseases such as osteoporosis clinically and also carnitine can be used as a first-choice supplementary material in osteoporotic women.
Authors’ contributions
OE and HZ contributed in the concept and design of the study as well as in the analysis and interpretation of data. CE participated in the analysis of data. HZ, FI, and OS carried out animal handling and experiments. BY and OS made biochemical analysis. BH, AAK, SB, and AA participated in the interpretation of data and in the revision of the manuscript critically. All authors read and approved the final manuscript.
Scatter plots of bone mineral density (BMD) versus IL-1β, IL-6, and TNF-α concentrations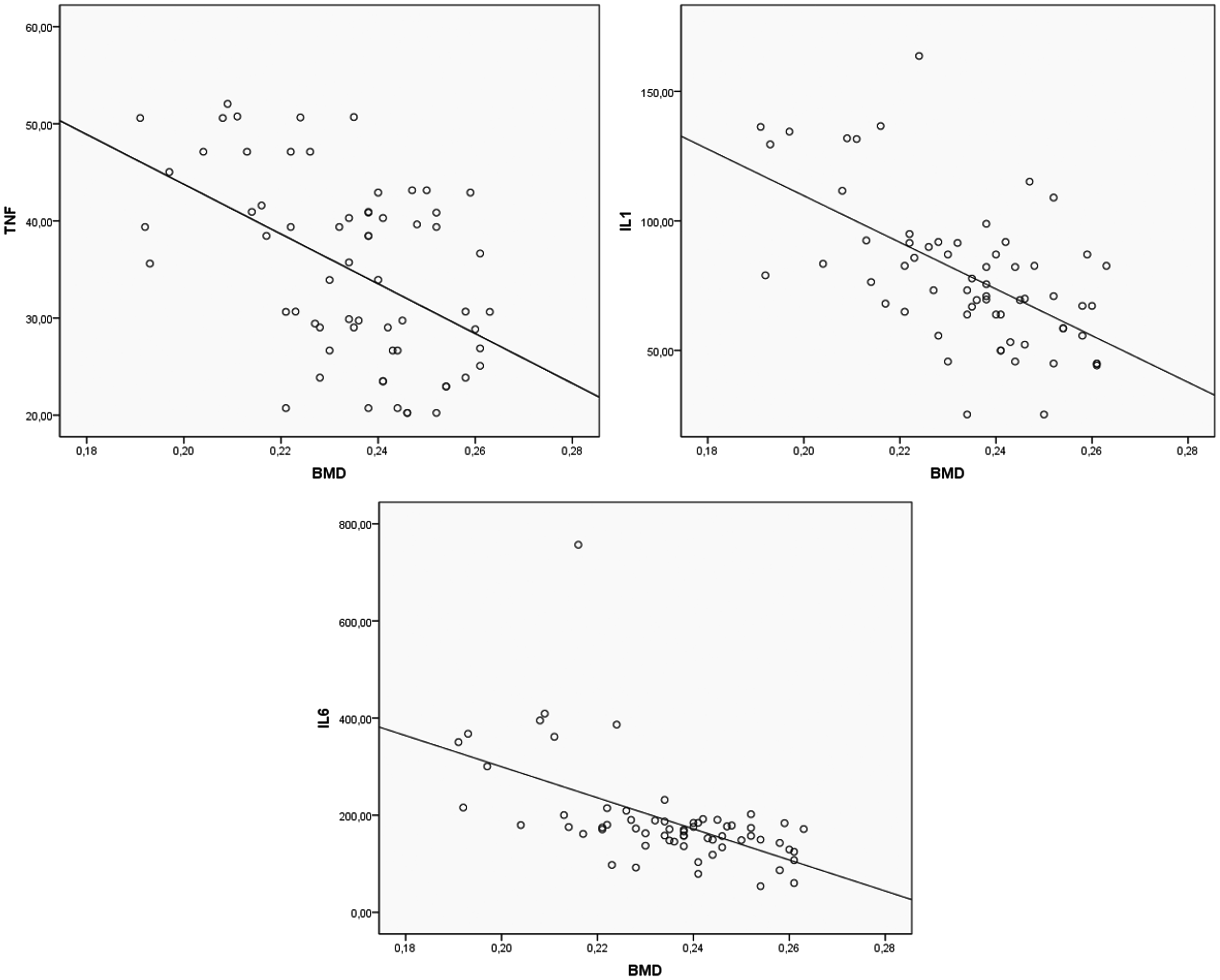
Footnotes
ACKNOWLEDGEMENT
This work was supported by the Ataturk University Medical Research Council (grant number 2012/4).