
Abstract
The vitamin D receptor (VDR) gene polymorphisms have been reported to be involved in the development of many musculoskeletal disorders, including osteoarthritis (OA). However, results were inconsistent and there is no definite conclusion regarding the association between any VDR polymorphism and the risk of OA. In this study, we conducted a meta-analysis to determine whether BsmI, TaqI, and ApaI polymorphisms in the VDR gene are associated with OA susceptibility. Literature research was performed using PubMed and EMBASE databases. Studies illustrating the association between the three VDR polymorphisms and OA were included, and their qualities were assessed using Newcastle–Ottawa scale. Eight eligible studies, recruiting 1626 cases and 2024 controls were identified. Their methodological qualities were generally good, with scores ranging from 6 to 8 points. However, throughout all summary analyses, which were performed for multiple categories and on four contrasts (allele contrast, contrast of homozygotes, recessive and dominant models), none of the VDR BsmI, TaqI, and ApaI gene polymorphisms were found to be significantly associated with the risk of OA. On the other hand, there was no significant publication bias. Results from this meta-analysis suggested that the VDR BsmI, TaqI, and ApaI gene polymorphisms might not be important predictors of OA. More studies further investigating these associations, especially taking into account of gene–gene, gene–environment interactions, and other confounding factors are warranted.
Introduction
Osteoarthritis (OA) is one of the most common causes of musculoskeletal disability. It is related to aging, characterized by progressive degeneration of articular cartilage, and can lead to chronic joint pain and discomfort.1,2 There are several pathologic mechanisms implicated in the development of OA, such as obesity, geographic factors, occupational knee bending, bone and joint malformations, injury and metabolic diseases, etc. 3
Family studies revealed that OA appeared to be transmitted in a clear Mendelian dominant fashion.4,5 Moreover, a study of twins demonstrated that in women up to 65% of the variance of radiologic OA of the knee and hand could be explained by genetic factors. 6 They all suggested that genetic factors might be involved in OA susceptibility. Identification of potential genetic risk factors may be significant for primary and secondary prevention of consequent disability, and also could be used for early diagnosis and monitoring the course of the disease.
So far a number of candidate genes have been demonstrated to be associated with this disorder, including vitamin D receptor (VDR) alleles, which is a kind of steroid nuclear receptor and polymorphisms in this gene are known to play a role in bone mineralization and remodeling. 7 Since serum 25-hydroxyvitamin D deficiency was reported to be associated with increased risk of knee OA, 8 hypothesis exists that allelic variation in VDR gene might also be associated with OA. Furthermore, OA may primarily be a bone disorder, in which a cascade of changes in joint structure take place starting from subchondral bone expansion. 9 The more dense bone, the less shock subchondral bone could absorb. Thus, the stress of loading is transferred directly to the articular cartilage, leading to cartilage loss and radiographic OA at late stage.9,10
The VDR gene is located on human chromosome 12q, and three VDR gene polymorphisms, i.e. BsmI and ApaI (both in intron 8), and TaqI (in exon 9), in strong linkage disequilibrium, 11 have been most frequently investigated. However, not all studies supported the proposed hypothesis that the three VDR gene polymorphisms were in significant association with OA susceptibility.12–33 The inconsistent results may be attributed to various factors, including the differences in the VDR genotype distribution, the genetic environment and age structure of the studied population, small sample sizes, and failure to take into account possible confounding factors that modulate the effect of VDR gene on OA susceptibility. On the other hand, one previous meta-analysis reported that no significant association between the VDR BsmI, TaqI, or ApaI polymorphisms and the risk of OA was found. 34 Among its 10 included studies, two focused on lumbar disc degeneration,23,26 and one investigated lumbar spinal stenosis, 35 pathologic mechanisms of which were not the same as that of OA. This clinical heterogeneity should not be neglected. What is more, since its publication, there are new relevant researches published,19–22 which may meet the inclusion criteria and an updated meta-analysis is warranted. Therefore, we conducted this research, using the method of meta-analysis in a comprehensive way, to determine whether BsmI, TaqI, and ApaI polymorphisms in the VDR gene are associated with the risk of OA.
Materials and methods
Identification and eligibility of relevant studies
Pertinent studies were identified by a systematic literature search using PubMed and EMBASE databases until August 2013 with combinations of keywords, i.e. “vitamin D,” “vitamin D receptor polymorphisms,” “VDR polymorphisms,” “VDR,” “polymorphism,” “osteoarthritis,” and “OA,” following the Meta-analysis Of Observational Studies in Epidemiology (MOOSE) guidelines. 36 Full texts were scrutinized if studies addressed the association between VDR polymorphisms and OA in humans. Furthermore, previous reviews and reference lists of the achieved full text were manually screened to identify further relevant studies. When multiple reports were published on the same population or subpopulation, we included only the most recent or informative one. No studies were excluded a priori for weakness of design or data quality.
Two reviewers independently evaluated studies for inclusion and any disagreement was resolved by consultation with a third one. Studies eligible for inclusion in this meta-analysis were required to meet the following criteria: (a) genotype-based study, rather than family-based study of pedigrees, focusing on any of the three VDR polymorphisms: BsmI, TaqI, and ApaI; (b) study investigating primary or idiopathic OA; (c) data regarding genotype distributions were sufficient to calculate odds ratio (OR) and the corresponding 95% confidence interval (CI); (d) The VDR genotype frequencies not significantly deviating from Hardy–Weinberg equilibrium (HWE).
Data extraction and assessment of study quality
Two investigators independently extracted the data and assessed the qualities of included studies using a standardized data-collection form and the Newcastle–Ottawa scale (NOS), respectively. In case of discrepancy, a third investigator was consulted to reach consensus.
According to the MOOSE guidelines, 36 for each study, we extracted the following information whenever possible with the aim to explore reasons for possible discrepancies among study findings: first author’s last name, publication year, study design, study location, ethnicity, diagnostic criteria, manner in which the controls were selected, numbers of cases and controls and genotype distribution in both groups, female percentages among cases and controls, OA sites, demographics, laboratory methods to detect VDR polymorphisms, and information regarding HWE.
The same two investigators assessed the qualities of included studies independently using the NOS, as proposed by the Cochrane Collaboration. It uses a “star” rating system to judge quality based on three domains: selection (four criteria), comparability (one criterion), and exposure (three criteria). The total number of stars an individual study may receive ranges from 0 (worst) to 9 (best). Studies with a score of 7 stars or greater were considered to be of high quality, while those with a score of 3 stars or lower were deemed to be of low quality. Disagreement was settled as mentioned earlier.
Statistical analysis
The strength of association between BsmI, TaqI, ApaI polymorphisms and OA was assessed by summary ORs and their corresponding 95% CI. Meta-analyses were performed on allele contrast, contrast of homozygotes, and recessive and dominant models. Relevant data were pooled with random-effects models or fix-effects models using the inverse of the corresponding variances as weights. Z-test was used to evaluate the significance of the pooled ORs with threshold P value = 0.05. We also assessed the departure of frequencies of VDR polymorphisms in controls by Chi-square test under HWE.
Statistical heterogeneity among studies was estimated using I2 statistics. It indicated low heterogeneity with a value < 25%, moderate heterogeneity with a value between 25% and 75%, and high heterogeneity with a value > 75%. In case significant heterogeneity was detected, sensitivity analysis (leave-one-out procedure) was planned, with the aim to explore possible source of it. Additionally, summary analyses in different populations were performed based on ethnicity, OA site, and sex difference. Possible publication bias was evaluated by funnel plot visual analysis, and the degree of asymmetry was assessed with Begg’s and Egger’s tests. All statistical analyses were performed using Cochrane Review Manager software version 5.2 (Cochrane Collaboration, Oxford, United Kingdom) and STATA 11.0 (Stata Corporation, College Station, Texas, USA). P value < 0.05 was considered statistically significant.
Results
Search results and study characteristics
The detailed process of study selection from the initial search to final inclusion is presented in Figure 1. Eight studies recruiting 1626 cases and 2024 controls were included in this meta-analysis.12–19 Among the included studies, four containing 670 cases and 559 controls were analyzed for BsmI polymorphism,13,14,16,17 four investigated the association between TaqI polymorphism and OA with 1106 cases and 959 controls,12,14,15,18 and three including 773 cases and 988 controls were on the ApaI–OA association.14,18,19 Studies identified and their main characteristics were listed in Table 1.
Flow diagram of the process of article selection for meta-analysis Main characteristics of all studies included in the meta-analysis Mean ± standard deviation(range). UK: United Kingdom; NR: not reported; NOS: Quality score assessed using Newcastle–Ottawa Scale.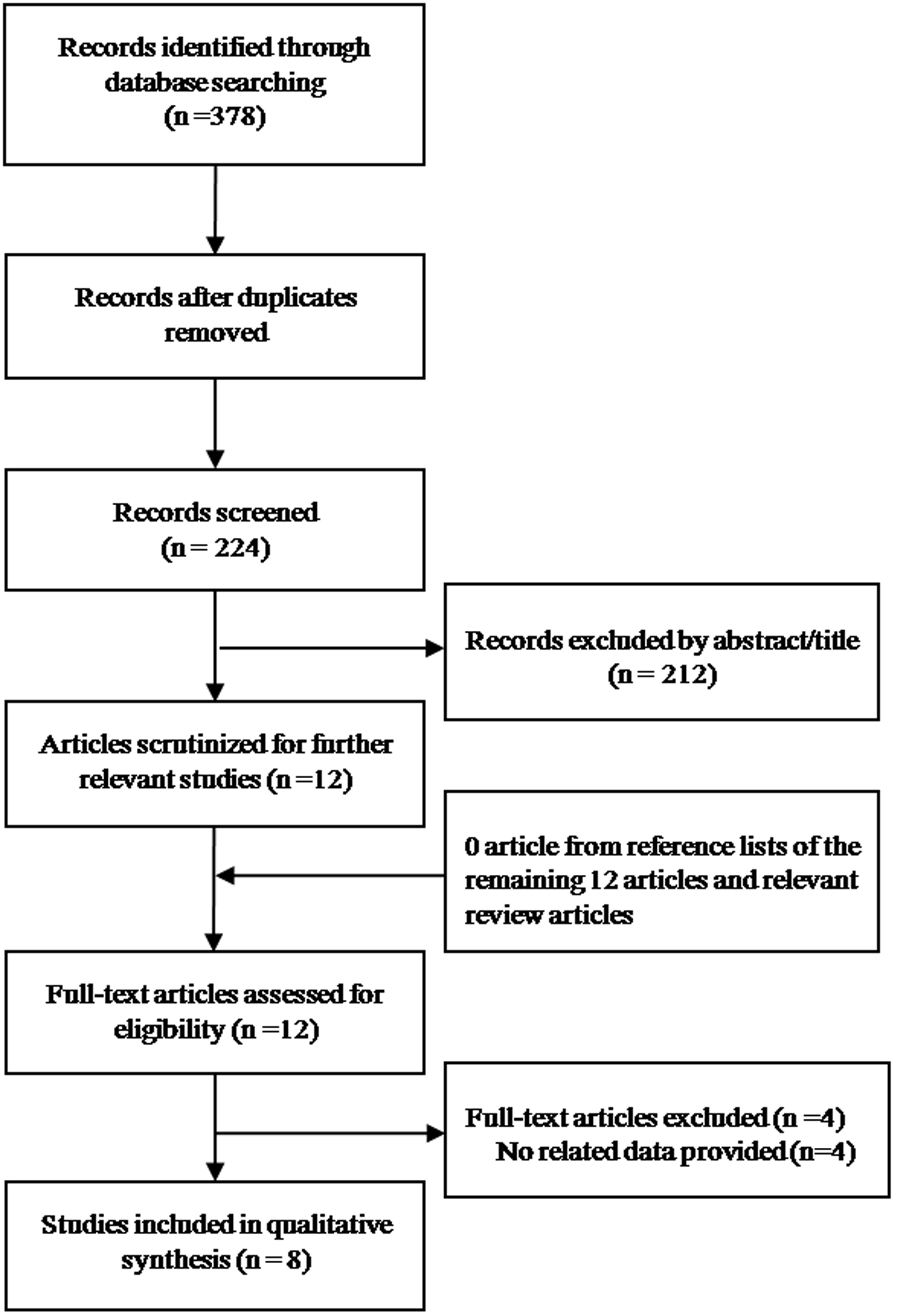
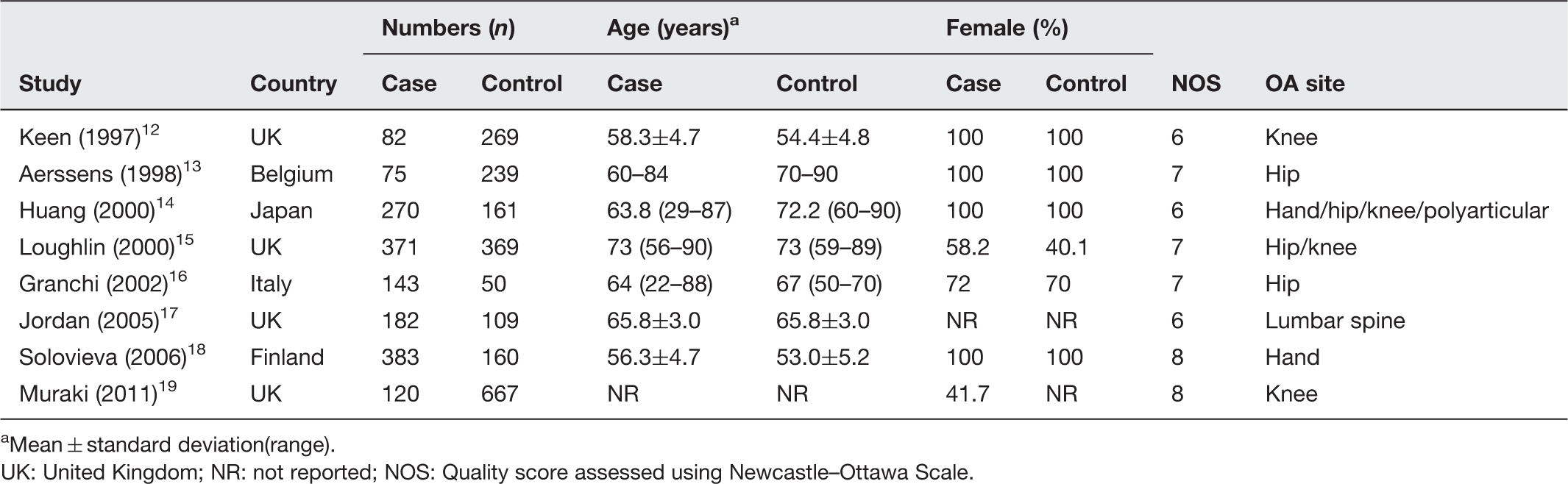
All studies were conducted in Europe except that of Huang et al., 14 which was performed in Asia. Five studies defined OA according to the methods of Kellgren and Lawrencewas,12,14,17–19 with a grade of 2 or higher, 37 while the other three included cases who underwent surgery due to OA.13,15,16 With respect to the selection of controls, four studies recruited population-based controls12,17–19 and that of the remaining four were hospital based.13–16 Furthermore, information on Hardy–Weinberg proportion in controls was not reported in three studies,15,17,19 while that of the other five were all reported to be consistent with HWE.12–14,16,18 However, using Chi-square test, no departure of frequencies of VDR polymorphisms in controls was detected in any of the eight included studies. At last, genotyping method of BsmI, TaqI, and ApaI polymorphisms was all performed using the polymerase chain reaction-restriction fragment length polymorphism technique, but no one mentioned blinding of the personnel who performed the genotyping.
Furthermore, results of study quality assessment were presented in Table 1. The average score (the number of stars awarded) was 7 (out of 9) with a range of 6–8 points, indicating generally good methodological quality.
Meta-analysis results
For the study conducted by Huang et al., 14 although it presented data for three comparisons with respect to hand, hip, and knee OA, respectively, patients with OA in multiple sites were included in more than one comparison. It was similar for controls that some of which were included in multiple comparisons. So if the three comparisons on OA site entered into meta-analyses simultaneously, multiple counting shared participants would probably create a unit-of-analysis error. Therefore in the investigating of overall association and that among women, to explore the impact of this error, we performed two categories of meta-analyses. One treated the three comparisons on hip, hand, and knee OA independently, regardless of the correlation among the three, and the other only included its data referring to polyarticular OA. The latter ones were regarded as our primary analyses. Detailed results were described below.
BsmI polymorphism
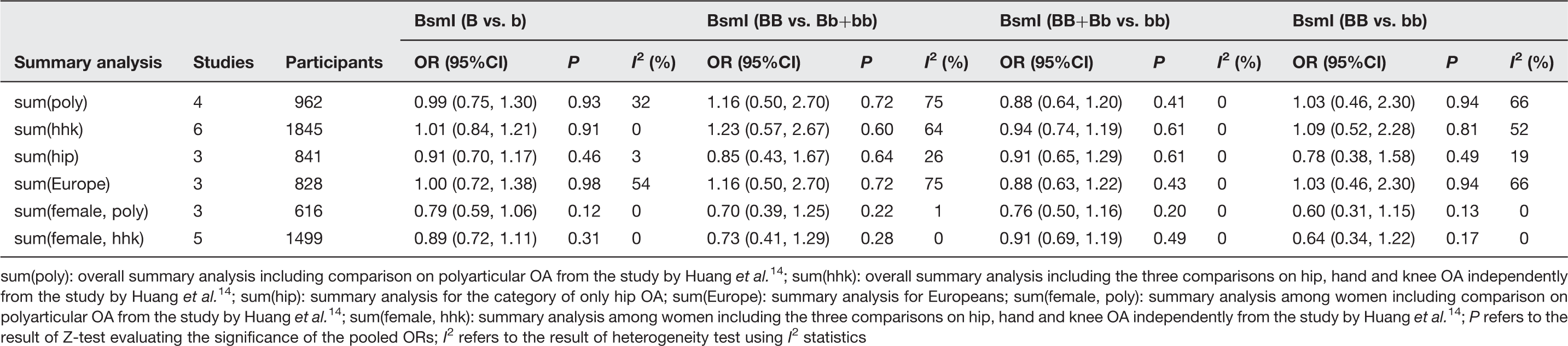
We performed summary analyses for six different categories, i.e. overall summary analyses including data only referring to polyarticular OA and treating the three comparisons independently from the study by Huang et al.,
14
the category considering hip OA, Europeans, and among women including comparison on polyarticular OA and treating the three comparisons independently from the study by Huang et al., separately.
14
However, no significant allele (Table 2, Figure 2(a) and 2(b)) or genotype association was detected. On the other hand, there were low to moderate heterogeneities among the studies (Table 2). Furthermore, no significant evidence of publication bias in any of these analyses was found. Take the overall summary analyses referring to the allele association for example, publication bias was absent as illustrated by the funnel plots (Figure 2(c) and (d)), which was further supported by Begg’s and Egger’s tests. When treating the three comparisons from the study by Huang et al.
14
independently, PBegg and PEgger were 0.71 and 0.87 while PBegg and PEgger were 0.31 and 0.22 for the comparison on polyarticular OA.
Meta-analysis of association between BsmI alleles and OA susceptibility. The strength of association was assessed by summary ORs and their corresponding 95% CI: (a) overall summary analysis including comparison on polyarticular OA from the study by Huang et al.
14
OR on the right axis (greater than 1) indicates B is more prevalent in cases than in controls, and B is more dangerous than b; (b) overall summary analysis including the three comparisons on hip, hand, and knee OA independently from the study by Huang et al.
14
OR on the right axis (greater than 1) indicates B is more prevalent in cases than in controls, and B is more dangerous than b; (c) funnel plot of the overall analysis including comparison on polyarticular OA from the study by Huang et al.
14
; (d) funnel plot of the overall analysis including the three comparisons on hip, hand, and knee OA independently from the study by Huang et al.
14
(A color version of this figure is available in the online journal) BsmI polymorphism and risk of OA sum(poly): overall summary analysis including comparison on polyarticular OA from the study by Huang et al.
14
; sum(hhk): overall summary analysis including the three comparisons on hip, hand and knee OA independently from the study by Huang et al.
14
; sum(hip): summary analysis for the category of only hip OA; sum(Europe): summary analysis for Europeans; sum(female, poly): summary analysis among women including comparison on polyarticular OA from the study by Huang et al.
14
; sum(female, hhk): summary analysis among women including the three comparisons on hip, hand and knee OA independently from the study by Huang et al.
14
; P refers to the result of Z-test evaluating the significance of the pooled ORs; I2 refers to the result of heterogeneity test using I2 statistics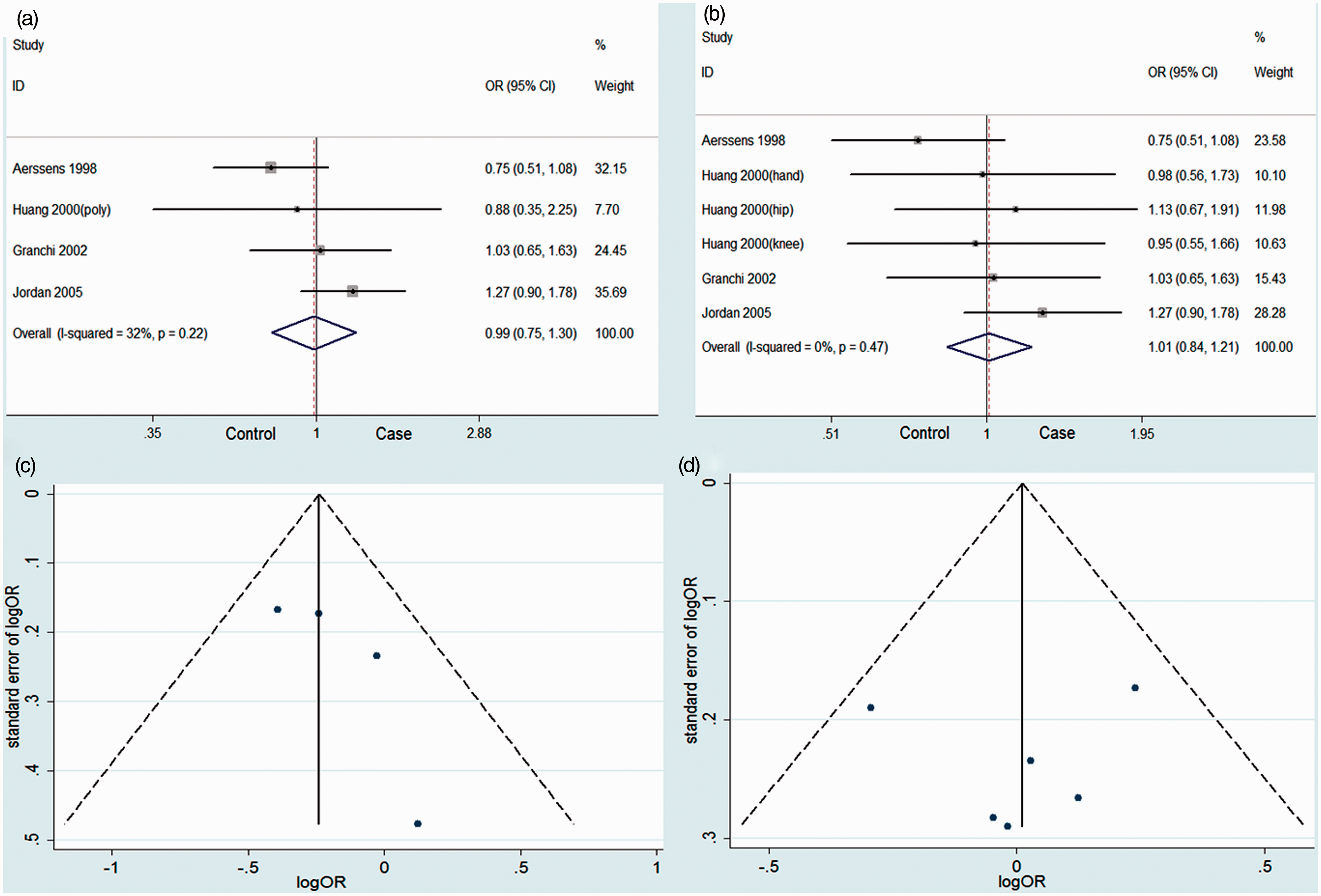
TaqI polymorphism
TaqI polymorphism and risk of OA
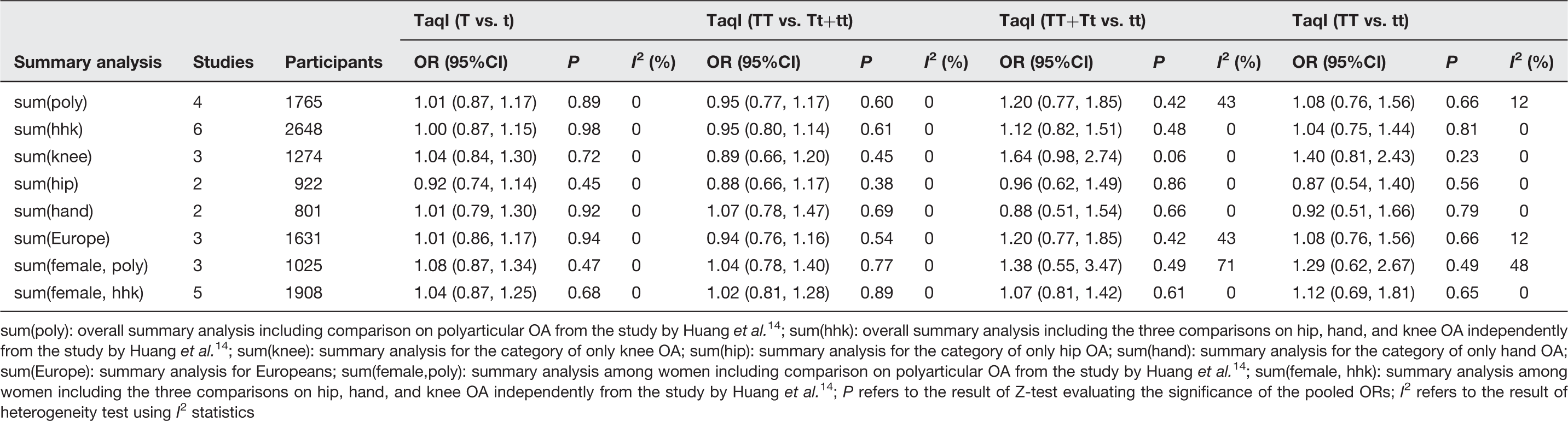
sum(poly): overall summary analysis including comparison on polyarticular OA from the study by Huang et al. 14 ; sum(hhk): overall summary analysis including the three comparisons on hip, hand, and knee OA independently from the study by Huang et al. 14 ; sum(knee): summary analysis for the category of only knee OA; sum(hip): summary analysis for the category of only hip OA; sum(hand): summary analysis for the category of only hand OA; sum(Europe): summary analysis for Europeans; sum(female,poly): summary analysis among women including comparison on polyarticular OA from the study by Huang et al. 14 ; sum(female, hhk): summary analysis among women including the three comparisons on hip, hand, and knee OA independently from the study by Huang et al. 14 ; P refers to the result of Z-test evaluating the significance of the pooled ORs; I2 refers to the result of heterogeneity test using I2 statistics
ApaI polymorphism
ApaI polymorphism and OA association
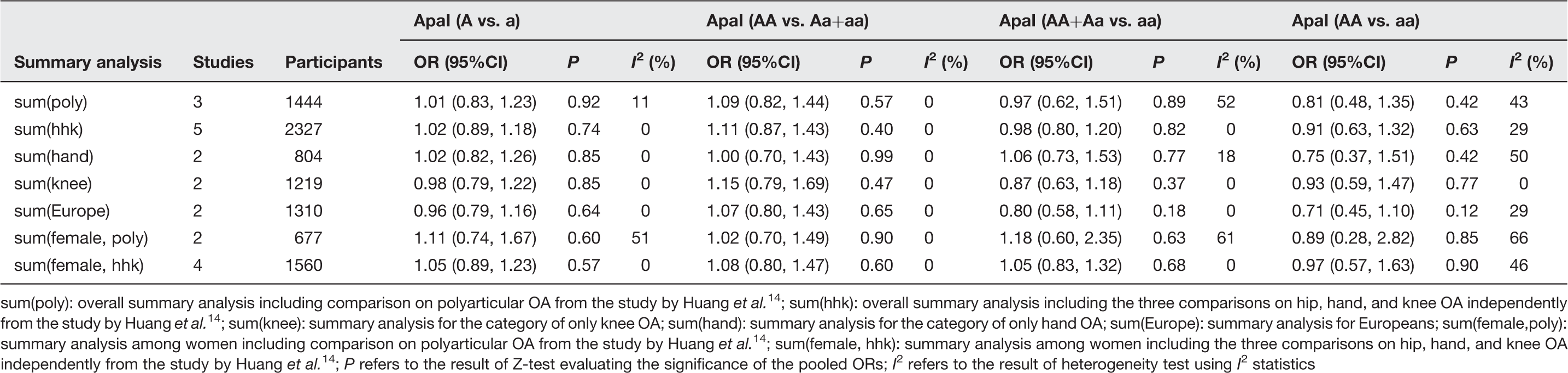
sum(poly): overall summary analysis including comparison on polyarticular OA from the study by Huang et al. 14 ; sum(hhk): overall summary analysis including the three comparisons on hip, hand, and knee OA independently from the study by Huang et al. 14 ; sum(knee): summary analysis for the category of only knee OA; sum(hand): summary analysis for the category of only hand OA; sum(Europe): summary analysis for Europeans; sum(female,poly): summary analysis among women including comparison on polyarticular OA from the study by Huang et al. 14 ; sum(female, hhk): summary analysis among women including the three comparisons on hip, hand, and knee OA independently from the study by Huang et al. 14 ; P refers to the result of Z-test evaluating the significance of the pooled ORs; I2 refers to the result of heterogeneity test using I2 statistics
Since the number of studies included in the three association analysis between BsmI, TaqI, and ApaI polymorphisms and OA susceptibility was limited, we chose random-effect model for all analyses described earlier.
Discussion
Our findings indicate that with available research data and using the method of meta-analysis, none of the three VDR gene polymorphisms, i.e. BsmI, TaqI, and ApaI, confers risk of OA.
Vitamin D plays a key role in musculoskeletal function and calcium homeostasis, 7 and the VDR gene polymorphisms have been reported to be the reason for some of the genetic variation in bone mineral density (BMD) and osteoporosis development.38–44 For example, Ferrari et al. 38 investigated the association between VDR alleles and rate of change of lumbar BMD over 18 months in 72 elderly participants. They found that the effect of calcium intake on maintenance of bone mass could relate to VDR gene polymorphisms. Similar results were also presented by Fleet et al. 39 that lower BMD was significantly prevalent in women with BB genotype than that with the other two genotypes. Moreover, it was suggested that a high femoral neck-BMD was associated with the TT genotype of VDR TaqI gene polymorphisms while low femoral neck-BMD was associated with the tt genotype. 45 Then Seremak-Mrozikiewicz et al. 46 explored the relationship in Polish postmenopausal women and found the presence of T allele of TaqI polymorphism could predict higher risk to develop osteoporosis, while t allele could have protective effect. Most recently it was revealed that the presence of single alleles a, b, and T of ApaI, BsmI, and TaqI VDR gene polymorphisms, respectively, might serve as an indicator of non-vertebral fractures. 42
However, for another musculoskeletal disorder, OA, although genetic factors are also suggested determinants,4–6 and serum 25-hydroxyvitamin D deficiency was showed to be associated with knee OA, 8 researches focusing on the association between VDR gene polymorphisms and OA susceptibility got more controversial results. Keen et al. 12 initiated the investigation in a population cohort of 351 postmenopausal women (ages 45–64 years) with the restriction enzyme TaqI. It suggested that the frequency of the VDR genotype differed significantly between OA cases and controls and the VDR allele “T” was associated with an increased risk of knee OA compared with the “t” allele, with an OR of 2.82 (95% CI = 1.16–6.85). Using molecular haplotyping of anonymous intragenic DNA polymorphisms, Uitterlinden et al. 32 studied the relationship between knee OA and VDR genotype in a population-based sample. They demonstrated that VDR haplotype allele was significantly over-represented in individuals with knee OA and associated with a 2.27-fold increased relative risk (95% CI = 1.46–3.52). Their result was robust since after adjustment for bone density at the femoral neck, it did not change, indicating that the association is not mediated by bone density. However, Aerssens et al. 13 did not found significant difference of genotype frequency distributions of BsmI polymorphism between hip OA patients and normal controls in Belgian postmenopausal women. Similarly, Huang et al. 14 assessed the association between VDR gene BsmI, TaqI, and ApaI polymorphisms and hand, hip, and knee OA among Japanese women without significant findings. After that, Granchi et al. 16 observed a significantly higher frequency of homozygous bb in patients with OA secondary to hip dysplasia. Inversely, Jordan et al. 17 reported that subjects with the BB genotype were significantly more likely to have severe osteophyte scores (P = 0.03). Furthermore, they detected a significant interaction between birth weight and the VDR gene as determinants of spinal osteophytes. So existing evidence is inconsistent and it is assumed that the discrepancy may be due to small sample sizes, differences in the genetic environment and VDR genotypes distribution, etc.
In our research, none of the three VDR gene polymorphisms, i.e. BsmI, TaqI, and ApaI, was found to be significantly associated with OA susceptibility. The results were obtained through an exhaustive search, selection, data extraction, statistical analysis, and results explanation. Specifically for the data processing part, we have performed analyses on allele contrast, contrast of homozygotes, recessive and dominant models, and conducted summary analyses for different categories to make full use of data. Furthermore, to avoid unit-of-analysis error which might be introduced by multiple counting shared participants from the study conducted in Japan, 14 we performed two categories of meta-analyses when investigating overall association and that among women. One used data of the three comparisons on hip, hand, and knee OA simultaneously, and the other included its data referring to polyarticular OA. As it turned out, the two summary analyses produced similar results, which made our findings more convincing and demonstrated that the unit-of-analysis error did not exert material impact on the results. On the other hand, considering there is little evidence that vitamin D affects risk of OA in most observational studies,47–49 our negative findings seem interpretable and supporting. Furthermore, since osteoporosis is generally regarded to be of genetic susceptibility to VDR gene polymorphisms,38–46 our results may reveal that OA and osteoporosis have different etiology, at least in regard to relationships with the VDR gene polymorphisms.
This research is different from the previous meta-analysis conducted by Lee et al., 34 although we got similar negative results. First, we did not consider three previously included studies,23,26,35 whose focuses were lumbar disc degeneration or lumbar spinal stenosis, rather than OA. In addition, we updated it with a new published research. 19 Second, with respect to data from the original study by Huang et al., 14 it seems that the previous one neglected the unit-of-analysis error by multiple counting shared participants. So to avoid this error and explore the impact of it, we performed additional meta-analyses only including its comparisons for polyarticular OA, which are more objective and convincing.
The present study has some limitations. First, the pooled risk estimates were calculated without adjustment for potential confounding factors. Since gene–gene and gene–environment interactions may involve in the pathogenesis of OA, possible covariates may exist. For example, apart from VDR polymorphisms, wnt/b-catenin pathway, environmental factors, family history, and lifestyle may also involve in its etiology.3,50,51 But unfortunately in our research, these effects could not be evaluated without available data. Second, linkage equilibrium was found for the BsmI, TaqI, and ApaI polymorphisms,11,52 so haplotype analysis may be more powerful and provide more clinically practical information than single polymorphism analysis. Also without sufficient related data, this kind of analysis could not be achieved. Third, our results may be applicable to only European and Asian patients because of the source of included studies. Fourth, with respect to the recruitment of subjects, half of our included studies were hospital based.13–16 Then selection bias may be introduced although this kind of clinical heterogeneity between population- and hospital-based studies was not detected using our statistical method.
In spite of these limitations, our meta-analysis also had some advantages. First, to explore potential clinical heterogeneity, we performed comprehensive summary analyses among different populations, i.e. patients with different types of OA, patients from European countries, and women separately. Second, individual studies are usually underpowered in detecting modest genetic effects that indicate susceptibilities to OA. In this regard, by integrating previous research, our meta-analysis increased statistical power and the precision of effect estimates. Third, quality of all included studies was satisfactory and the VDR genotype frequencies in controls were all not deviating from HWE. Fourth, on the whole, heterogeneity and publication bias were not significant throughout our analyses, suggesting that the whole pooled results may be unbiased.
In conclusion, VDR BsmI, TaqI, and ApaI gene polymorphisms might not be significant genetic risk factors for OA. However, our results should be interpreted with caution because of small number of studies included. More in-depth research taking into account of gene–gene, gene–environment interactions, and other confounding factors is needed to further investigate these associations.
Footnotes
Author contributions
HL and CH designed the study; HH, LY, and PW performed the search strategy for identification of studies; SL, HL, and CH extracted the data; HL, CL, XW, and TW analyzed and interpreted the data; HL, HH, SL, and CH wrote and revised the manuscript. All the authors participated in the study design, implementation, analysis and interpretation of the data, and review of the manuscript.
Acknowledgements
This study was supported by Grant 81171865 from the National Natural Science Foundation of China.