
Abstract
Renalase is a recently described enzyme secreted by the kidney into both plasma and urine, where it was suggested to degrade catecholamines contributing to blood pressure control. While there is a controversy regarding the relationship between renal function and plasma renalase levels, there is virtually no data in humans on plasma renalase activity as well as on both urine renalase levels and activity. We prospectively examined the time course of plasma and urine renalase levels and activity in 26 end-stage renal disease (ESRD) patients receiving a cadaver kidney transplant (cadaver kidney recipients [CKR]) before surgery and during the recovery of renal function up to day 90 post transplant. The relationship with sympathetic and renal dopaminergic activities was also evaluated. The recovery of renal function in CKR closely predicted decreases in plasma renalase levels (r = 0.88; P < 0.0001), urine renalase levels (r = 0.75; P < 0.0001) and urine renalase activity (r = 0.56; P < 0.03), but did not predict changes in plasma renalase activity (r = −0.02; NS). Plasma norepinephrine levels positively correlated with plasma renalase levels (r = 0.64, P < 0.002) as well as with urine renalase levels and activity (r = 0.47 P < 0.02; r = 0.71, P < 0.0005, respectively) and negatively correlated with plasma renalase activity (r = −0.57, P < 0.002). By contrast, plasma epinephrine levels positively correlated with plasma renalase activity (r = 0.67, P < 0.0001) and negatively correlated with plasma renalase levels (r = −0.62, P < 0.003). A significant negative relationship was observed between urine dopamine output and urine renalase levels (r = −0.48; P < 0.03) but not with urine renalase activity (r = −0.33, NS). We conclude that plasma and urine renalase levels closely depend on renal function and sympathetic nervous system activity. It is suggested that epinephrine-mediated activation of circulating renalase may occur in renal transplant recipients with good recovery of renal function. The increase in plasma renalase activity observed in ESRD patients and renal transplant recipients can be explained on the basis of reduced inhibition of the circulating enzyme.
Introduction
In patients with chronic kidney disease (CKD), plasma catecholamines are increased and this is accounted for by both heightened sympathetic nerve activity and reduced catecholamine clearance. 1 On the other hand, a decrease of renal dopaminergic system activity that correlated well with the degree of deterioration of renal function was previously reported in CKD patients. 2 Given that plasma norepinephrine and renal dopamine exert antagonistic effects on tubular sodium reabsorption, it was suggested that heightened sympathetic activity and the accompanied reduced renal dopaminergic tonus in CKD may contribute both to reduce sodium excretion and increase blood pressure in this population.2,3 The participation of sympathetic and renal dopaminergic disturbances on hypertension and the enhanced cardiovascular risk in CKD has become more complex with the recent discovery of renalase, a new regulator of cardiac function and blood pressure.4,5
Renalase is a flavin adenine dinucleotide (FAD)- and nicotinamide adenine dinucleotide (NADH)-dependent enzyme expressed mainly in glomeruli and proximal tubules of the kidney, but also in cardiomyocytes and other tissues.4,6–10 In contrast to other monoamine oxidases, renalase is secreted into both plasma and urine where it was suggested to metabolize catecholamines and other substrates.4,11 Under basal conditions, plasma renalase was suggested to circulate as an inactive proenzyme that can be converted to the active form by brief surges in catecholamine levels and increases in blood pressure whereas urine renalase exhibits robust amine oxidase activity at baseline. 12 The difference in activity between blood and urine renalase was suggested to be related with the presence of a renalase inhibitor in plasma. 12
In their first study describing renalase, Xu et al. 4 provided evidence that plasma renalase expression in eight end-stage renal disease (ESRD) patients on hemodialysis was markedly reduced in comparison with a group of four healthy volunteers. However, a series of recent studies suggested that plasma renalase levels are negatively correlated with renal function in several populations, namely in kidney transplant recipients, 13 heart transplant recipients, 14 patients on peritoneal dialysis 15 and patients on hemodialysis. 16
In addition to the unsolved and controversial issue of the relationship between renal function and plasma renalase expression/levels it remains to be established whether activation of plasma renalase occurs in CKD, in the presence of catecholamine excess and increase in blood pressure. 12 On the other hand, although it has been suggested that renalase may contribute to degrade dopamine,17,18 there is virtually no data on urine renalase levels and activity in humans, namely in relation with changes in either renal function or renal dopamine system activity.
In this study, we prospectively examined the time course of plasma and urine renalase levels and activity in a group of cadaver kidney recipients (CKR), before surgery and during the recovery of renal function up to day 90th post transplant. The relationship with changes in both sympathetic and renal dopaminergic activities was also examined throughout the study period.
Subjects and methods
All participants were recruited in the Department of Nephrology and Renal Transplant of São João Hospital Center. The research was approved by the Ethics Committee for Health and the Local Institutional Review Board of São João Hospital Centre, and was carried out in accordance with the Declaration of Helsinki (2008) of the World Medical Association. All participants were informed about the purpose and methods of the study and voluntarily gave their written informed consent.
We carried out a prospective study among a group of 26 ESRD patients receiving a cadaver kidney transplant before surgery and during the recovery of renal function up to day 90th post transplant. Before surgery, all CKRs were on chronic dialysis therapy and the daily residual diuresis was greater than 100 mL in all patients. The standard immunosuppressive regimen in all kidney recipients studied consisted of a calcineurin inhibitor (cyclosporine or tacrolimus) together with mycophenolate mofetil and prednisone. In some cases, the Synphony protocol was applied with basiliximab or antithymocyte globulin (ATG).
Blood pressure was measured in all CKRs in the sitting position on day 0 before surgery as well as on days 14 and 90 post transplant, using an automatic manometer. Blood samples were collected in all CKRs before renal transplant (day 0) as well as on days 14 and 90 post-surgery for the assessment of renal function parameters, plasma catecholamine levels and plasma renalase levels and activity. Urine samples were also collected in all participants throughout the same time periods for the assessment of urinary renalase levels and activity and for evaluation of the urinary excretion of free dopamine. Urine samples for quantification of dopamine were collected in vials with hydrochloric acid (6 mol/L) to avoid the spontaneous oxidation of the amine.
In order to have information on the values of the parameters evaluated in CKRs, in the presence of normal renal function, blood and urine were also collected in a group of four ESRD patients receiving a living kidney transplant (LKR) and in their corresponding healthy donors (LKD), on day 0 before surgery. The inhibitory status of plasma renalase was also examined in these LKD/LKR pair groups on day 0 before surgery as well as on days 14 and 90 post-surgery.
Catecholamines in both plasma and urine were measured by HPLC with electrochemical detection, as previously described. 19 The lower limit of detection varied from 350 to 1000 fmol.
Plasma renalase levels were assessed in all participants by a commercially available enzyme-linked immunosorbent assay (ELISA) kit from Uscn Life Science Inc. (Wuhan, China) using a monoclonal primary antibody specific for renalase. Experiments were carried out according to the manufacturer's instructions.
The assessment of urinary renalase levels was performed by Western blot (WB) in all participants. Urine samples were adjusted to equalize urine creatinine concentration through a precipitation protocol using 50% of trichloroacetic acid. A sample corresponding to 50 µg of creatinine was used in each assay. The immunoblots were incubated with the anti-human renalase polyclonal primary antibody (1:1000, Proteintech, Chicago, USA) and secondary antibody rabbit IgG (H&L) IRDye800® conjugated antibody (1:25,000, Rockland Immunochemicals, Gilbertsville, USA).
Amine oxidase activity of renalase in both plasma and urine was measured in all participants by the ability of renalase to oxidize the biogenic amine epinephrine, using the Amplex Red Monoamine Oxidase Assay Kit (Invitrogen, Life Technologies Ltd, Paisley, UK). Experiments were carried out in duplicates of plasma and urine (100 µL) samples according to the manufacturer's instructions with a final substrate concentration of 2 mmol/L, using 0.5 µmol/L of semicarbazide as a specific inhibitor of semicarbazide-sensitive amine oxidase (SSAO), and 250 µmol/L of NADH (Sigma, St. Louis, USA) as a cofactor. The inhibitory status of circulating renalase in the LKD/LKR pair groups on day 0 before transplant as well as on days 14 and 90 post-surgery was evaluated by adding 50 µL of plasma obtained from either LKD or LKR groups to 50 µL of urine from LKR obtained on day 0. In the control samples (basal), 50 µL of reaction buffer was added to 50 µL of urine obtained from LKR on day 0.
Statistics
All data are presented as means ± standard error of the mean (SEM). A P < 0.05 was assumed to denote a significant difference. One-way analysis of variance (ANOVA) for repeated measures was used to evaluate statistical significance between different time periods within the same group. For group comparisons between LKD/LKR pairs, one-way ANOVA followed by post hoc Tukey test or standard unpaired Student′s t-test were used when appropriate. Pearson correlation was used to evaluate the relationship between two continuous variables and a two-tailed P is presented. Data were analyzed using Microsoft Excel 2010 (WA, USA) and GraphPad Prism 5 (CA, USA) software.
Results
Demographic, clinical and analytical parameters of the cadaver kidney transplant recipients (n = 26), on day 0 before surgery.
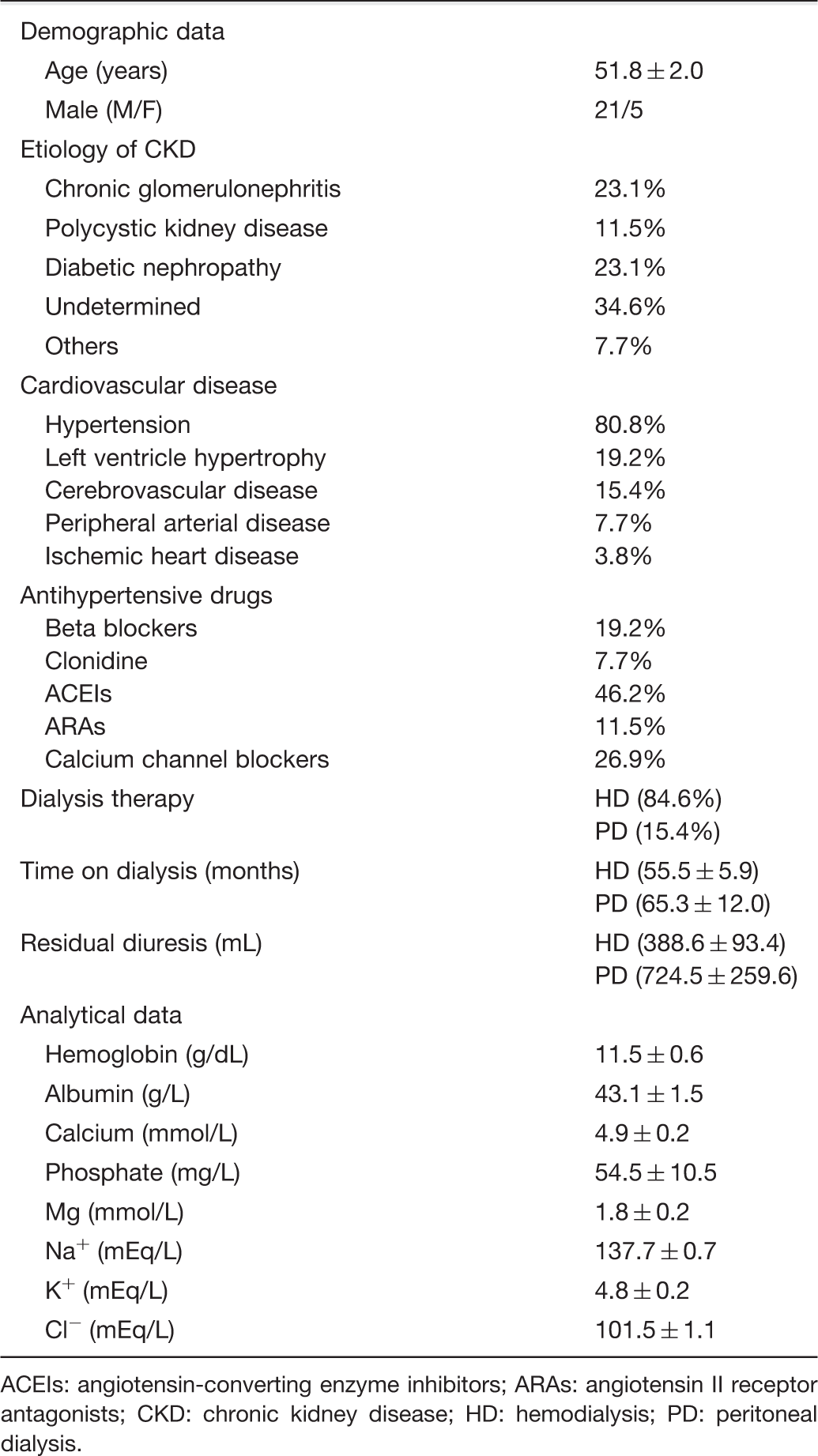
ACEIs: angiotensin-converting enzyme inhibitors; ARAs: angiotensin II receptor antagonists; CKD: chronic kidney disease; HD: hemodialysis; PD: peritoneal dialysis.
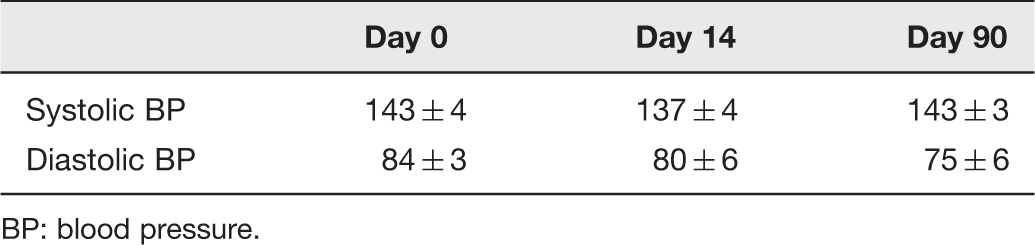
Renal function consistently recovered after transplant in CKRs as evidenced by marked decreases in serum creatinine levels on both days 14 and 90 post-surgery, in comparison with day 0 (Figure 1). However, no significant changes were observed in either systolic or diastolic blood pressure in CKRs throughout the study period (Table 2).
Renal function. Plasma creatinine levels in cadaver kidney recipients (CKR, n = 26) before surgery (day 0) and on days 14 and 90 post-surgery. Bars indicate means ± SE. #Significantly different from corresponding values on day 0 (P < 0.05) Systolic and diastolic blood pressure (in mmHg) of the cadaver kidney transplant recipients (n = 26), before surgery (day 0) and on days 14 and 90 post transplant. BP: blood pressure.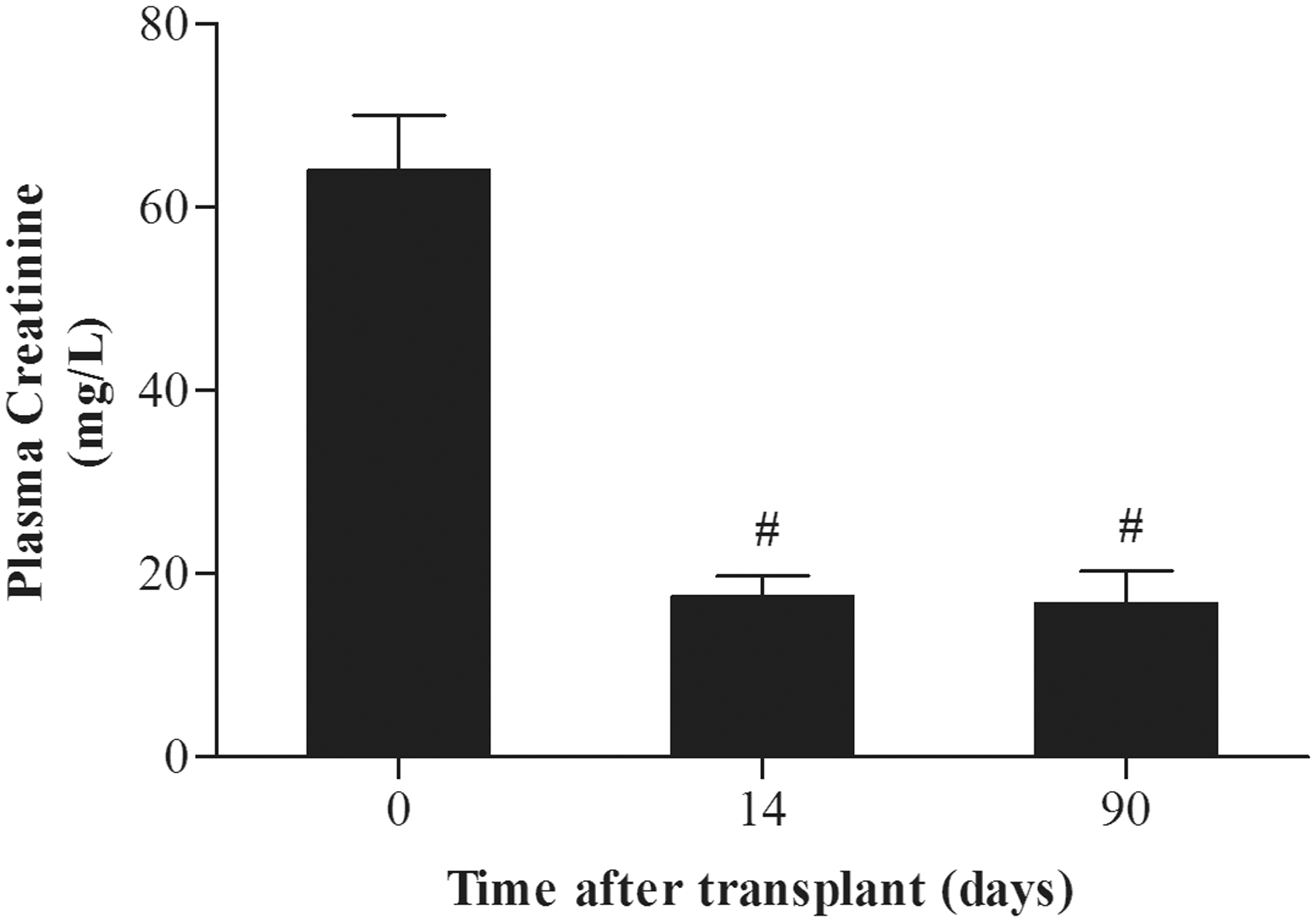
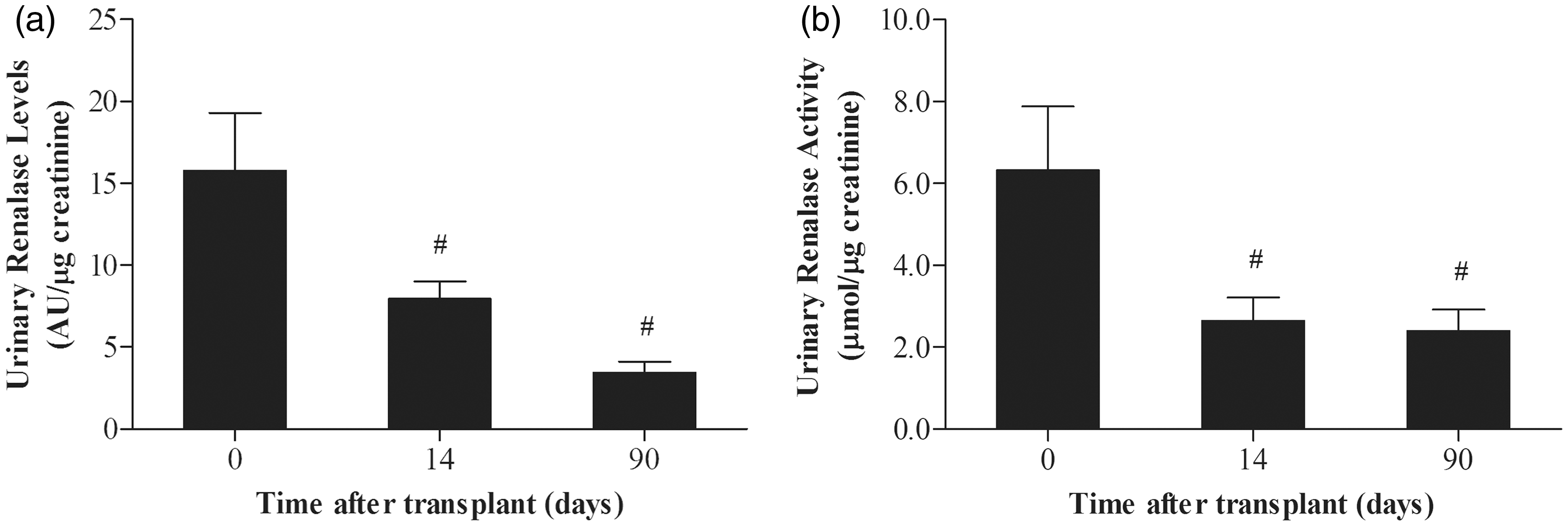
The recovery of renal function in CKRs was accompanied by significant decreases in plasma renalase levels on both days 14 and 90 post-surgery by ∼42% and ∼59%, respectively, in comparison with day 0 (Figure 2a). The recovery of renal function in CKRs was also accompanied by significant decreases in both urinary renalase levels and activity overtime (Figure 3a and b). By contrast, plasma renalase activity was significantly increased on day 14 post-surgery by ∼39%, in comparison with day 0 (Figure 2b). In addition, plasma renalase activity on day 90 post-surgery did not differ from that observed on day 0.
Plasma renalase levels and activity. Plasma renalase levels (a) and activity (b) in cadaver kidney recipients (CKR, n = 26) before surgery (day 0) and on days 14 and 90 post-surgery. Bars are means ± SE. #Significantly different from corresponding values on day 0 (P < 0.05) Urinary renalase levels and activity. Urinary renalase levels (a) and activity (b) in cadaver kidney recipients (CKR, n = 26) before surgery (day 0) and on days 14 and 90 post-surgery. Bars are means ± SE. #Significantly different from corresponding values on day 0 (P < 0.05)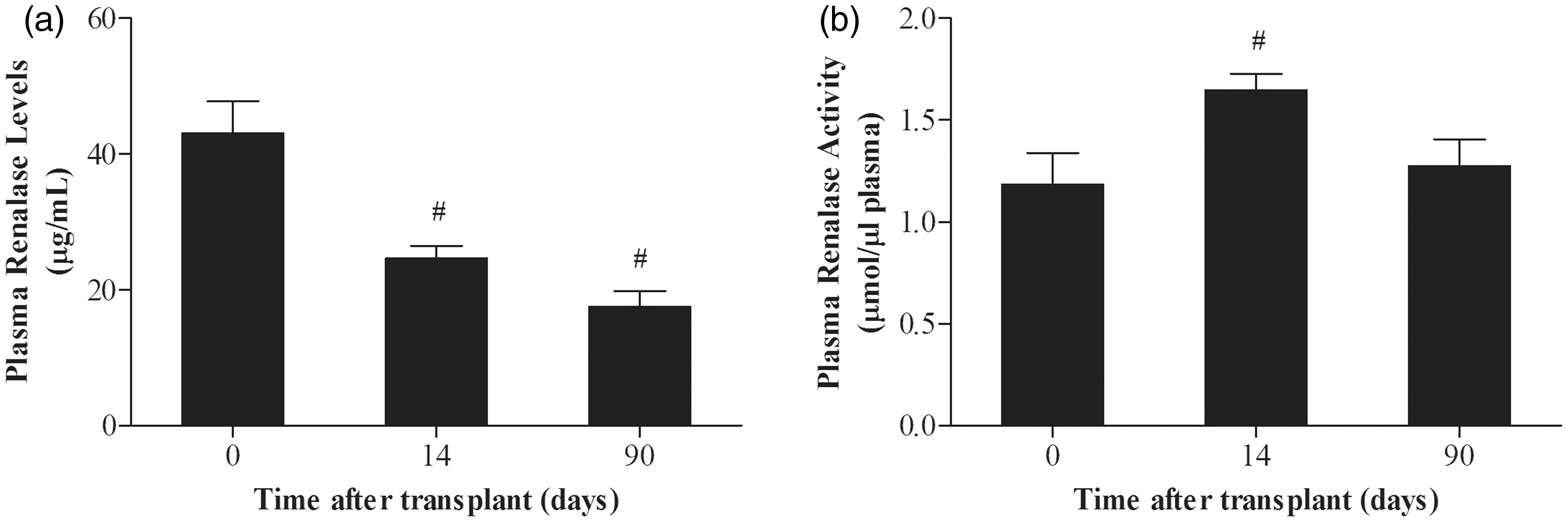
Correlations between blood pressure, plasma creatinine and catecholamine levels with (a) plasma renalase levels and activity and (b) urine renalase levels and activity, during the recovery of renal function in cadaver kidney transplant recipients (n = 26).
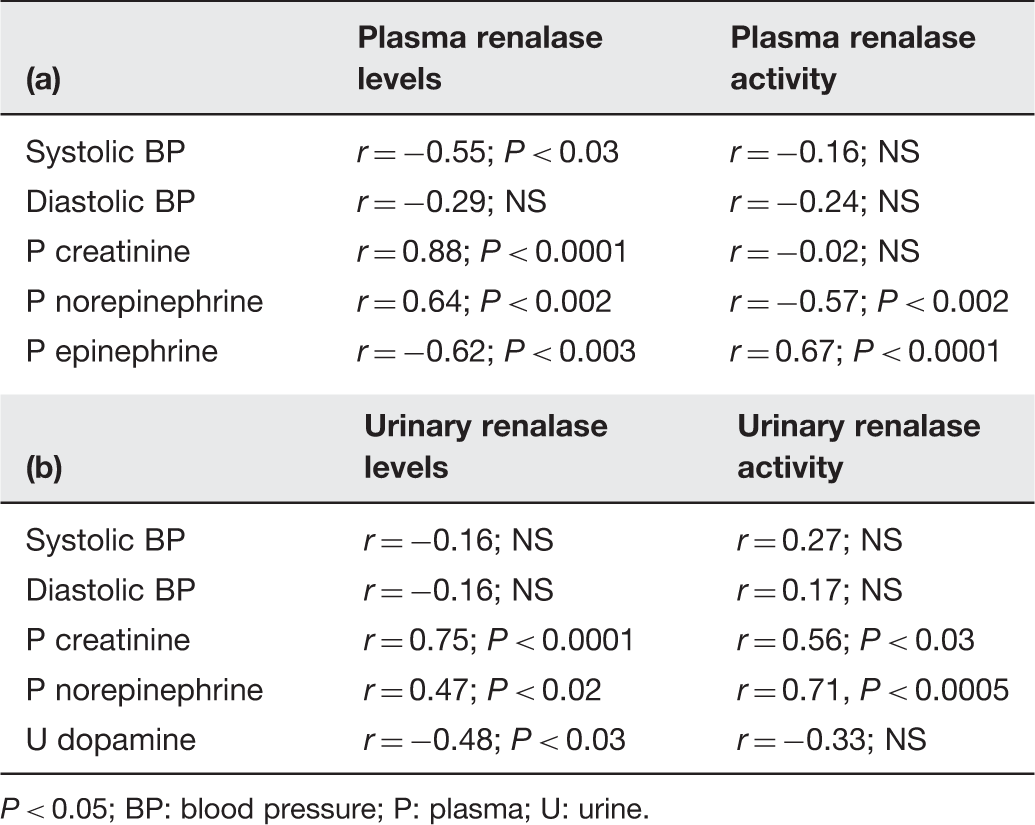
P < 0.05; BP: blood pressure; P: plasma; U: urine.
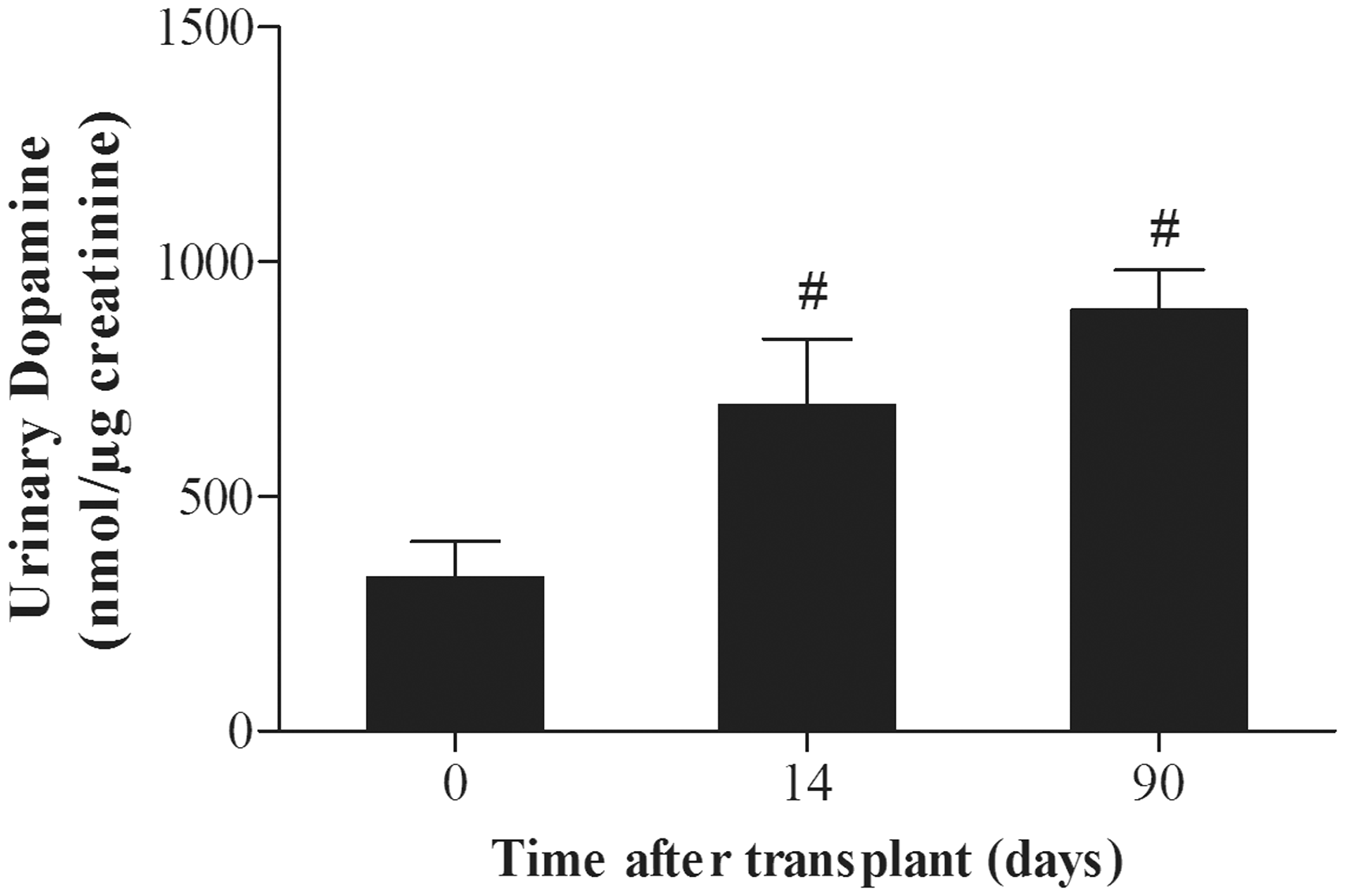
The recovery of renal function in CKRs was accompanied by a marked decrease in plasma norepinephrine levels on both days 14 and 90 post-surgery (Figure 4a), whereas a significant increase in plasma epinephrine levels was observed in CKRs on both days 14 and 90 post transplant in comparison with day 0 (Figure 4b). Urinary excretion of free dopamine significantly increased in CKRs by ∼two-fold and ∼three-fold on days 14 and 90 post-surgery, respectively, in comparison with day 0 (Figure 5).
Plasma catecholamines. Plasma norepinephrine (a) and epinephrine (b) levels in cadaver kidney recipients (CKR, n = 26) before surgery (day 0) and on days 14 and 90 post-surgery. Bars are means ± SE. #Significantly different from corresponding values on day 0 (P < 0.05) Urinary dopamine. Urine dopamine output in cadaver kidney recipients (CKR, n = 26) before surgery (day 0) and on days 14 and 90 post-surgery. Bars are means ± SE. #Significantly different from corresponding values on day 0 (P < 0.05)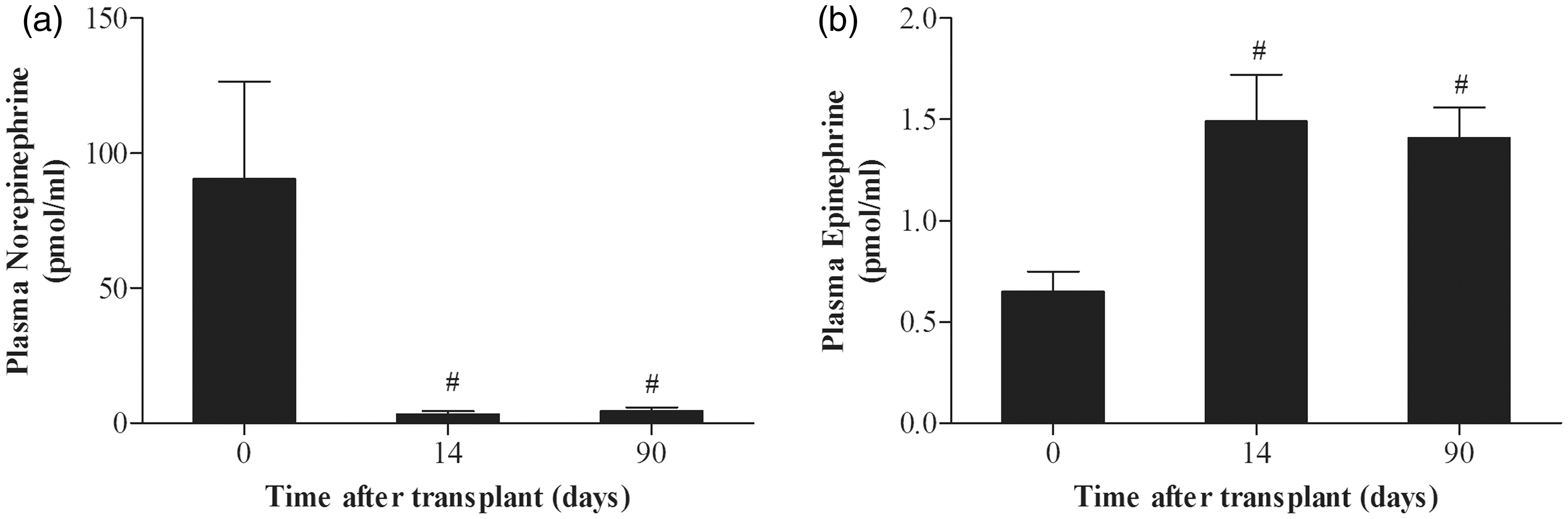
Plasma norepinephrine levels positively correlated with plasma renalase levels and negatively correlated with plasma renalase activity (Table 3a). By contrast, plasma epinephrine levels positively correlated with plasma renalase activity and negatively correlated with circulating renalase levels (Table 3a). Urine renalase levels positively correlated with plasma norepinephrine levels and negatively correlated with urine dopamine output (Table 3b). Urine renalase activity was also positively correlated with plasma norepinephrine levels but did not correlate with urine dopamine excretion (Table 3b).
Blood pressure, renal function, plasma and urine renalase levels and activity and plasma and urine catecholamine levels in four living kidney donor-recipient pairs (LKD/LKR) on day 0 before surgery.
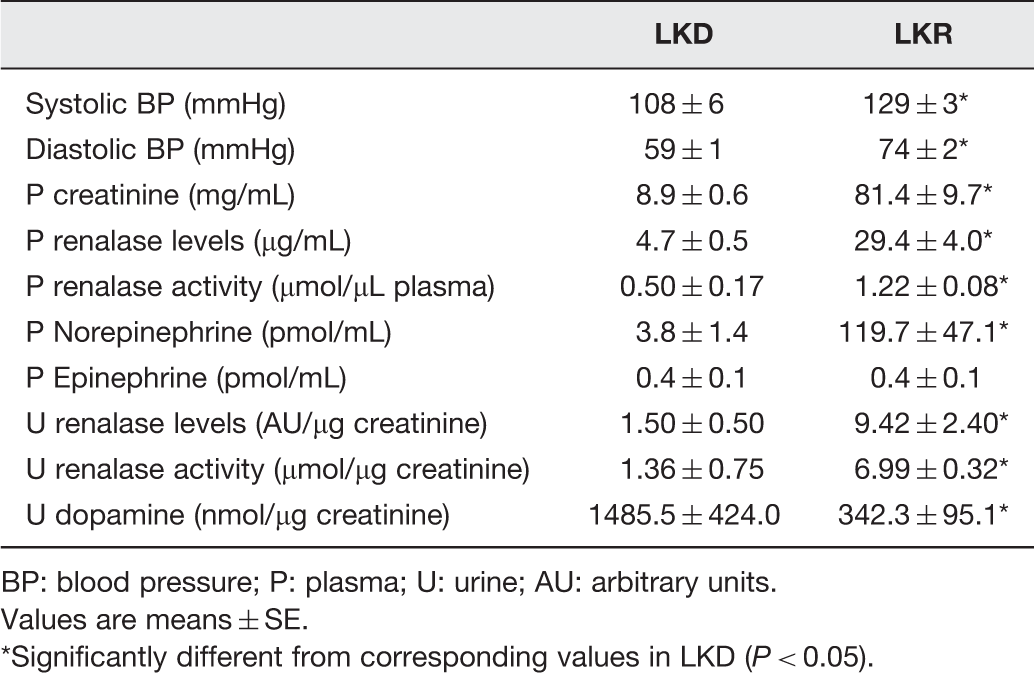
BP: blood pressure; P: plasma; U: urine; AU: arbitrary units.
Values are means ± SE.
*Significantly different from corresponding values in LKD (P < 0.05).
In the studies examining the inhibitory status of plasma renalase in the LKD/LKR pair groups we found that plasma obtained from LKDs on days 0, 14 and 90 significantly inhibited the urinary renalase activity by ∼60%, ∼58% and ∼45%, respectively (Figure 6). By contrast, plasma obtained from LKR group on day 0 before transplant as well as on days 14 and 90 post-surgery did not significantly change urine renalase activity (Figure 6).
Influence of the addition of plasma from living kidney donors (LKD) and living kidney recipients (LKR) on urine renalase activity, before surgery (day 0) and on days 14 and 90 post-surgery. Bars indicate means ± SE. *Significantly different from urine renalase activity with no plasma addition (P < 0.05)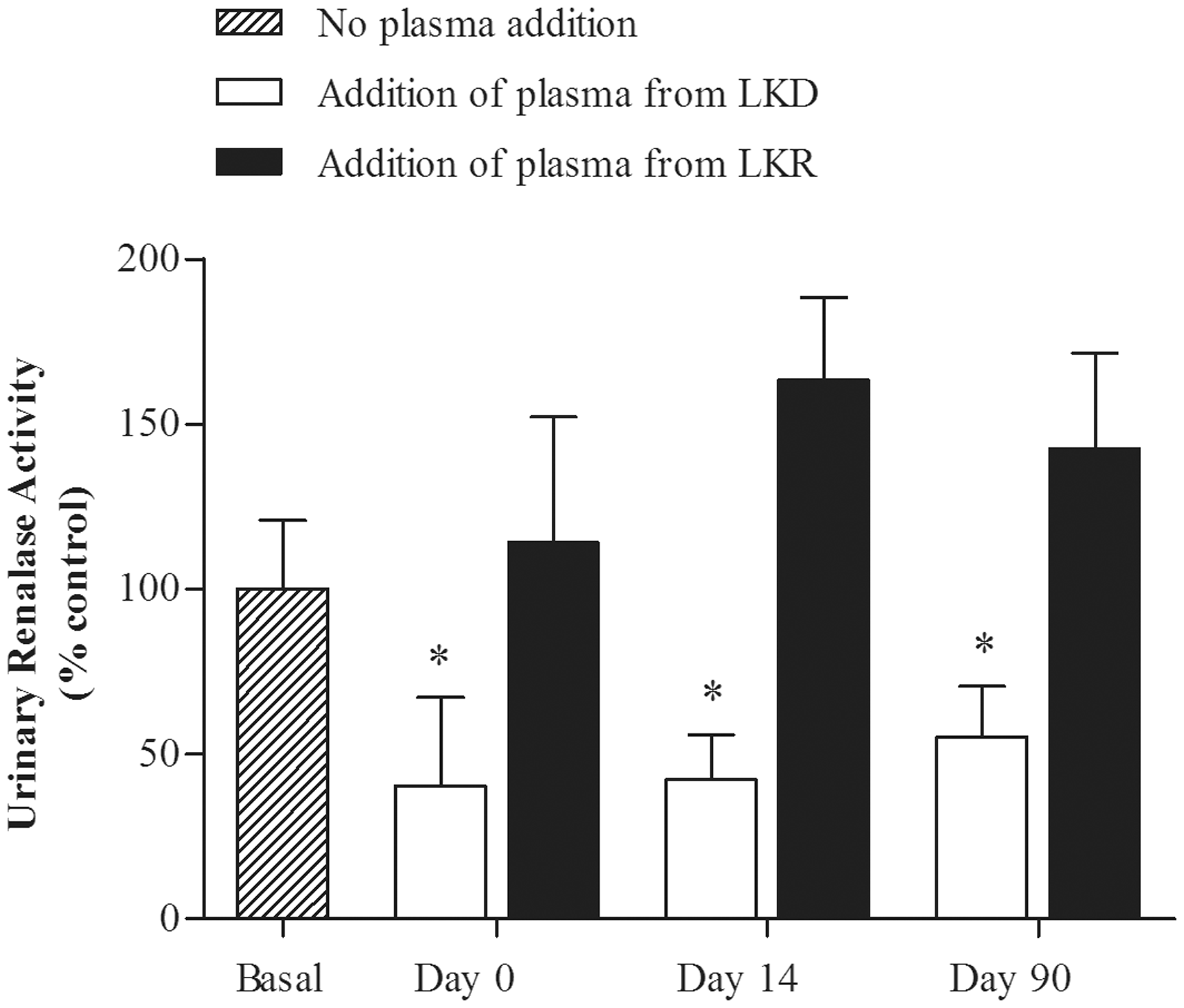
Discussion
The present study provides evidence favoring the view that the secretion of renalase in both plasma and urine is increased in patients with CKD. This suggestion is supported by the finding that both plasma and urine renalase levels were markedly increased in ESRD patients in comparison with healthy donors and is further reinforced by the observation that the recovery of renal function in kidney transplant recipients closely predicted decreases in both plasma and urine renalase levels.
Plasma and urine renalase activities were also significantly increased in patients with ESRD in comparison with healthy donors, thus suggesting that the CKD status may contribute to the activation of the enzyme. However, differently to urinary renalase activity, plasma renalase activity did not decrease in ESRD patients receiving a kidney transplant and was even significantly increased on day 14 post-surgery, notwithstanding the good recovery of renal function. Taken together, our findings indicate that plasma renalase levels may not predict plasma renalase activity in renal transplant recipients with good recovery of renal function and further suggest that this may be accounted for by a reduced inhibition of the circulating the enzyme.
In 2005, Xu et al. 4 first reported that plasma renalase levels are virtually undetectable in the blood of patients with ESRD on hemodialysis. In the mentioned study, renalase levels in human plasma were assessed by WB technique using an anti-renalase polyclonal antibody generated by Proteintech Group Inc. By contrast, using a commercially available ELISA kit with a monoclonal antibody specific for human renalase from Uscn Life Science, Zbroch et al. 16 recently reported a seven-fold increase in renalase blood levels in patients with ESRD, compared to control subjects with normal renal function. Several factors may justify these discrepant results: (1) ELISA may recognize epitopes different from those detected by the polyclonal antibody in the original studies using WB; (2) a cross-reaction with unrelated proteins or degradation products of renalase itself may occur with different antibodies; and 3) different technical approaches may favor the detection of different renalase isoforms.
Using the same ELISA kit used by Zbroch et al.16 we found in the present study that circulating renalase levels were increased by ∼six-fold in ESRD patients in comparison with healthy donors. The finding that the recovery of renal function in CKRs was paralleled by a progressive decrease in plasma renalase levels further reinforces the view that circulating renalase strongly depends on renal function. It is possible that the increase in plasma renalase levels in CKD may represent a compensatory response to plasma norepinephrine levels. 12 This suggestion is supported by the observation that plasma norepinephrine levels were markedly increased on day 0 before transplant in ESRD patients in comparison with healthy donors and is further reinforced by the close relationship observed between plasma norepinephrine and plasma renalase levels after transplant. Because renalase immunostaining was found markedly decreased in the renal cortex from patients with ESRD as well as in the rat remnant kidney, 20 one can hypothesize that an enhanced extra renal secretion of renalase may contribute to the increased plasma renalase levels in this condition.
The increase in plasma renalase levels observed in patients with ESRD was accompanied by an increased plasma renalase activity. However, circulating renalase activity did not decrease after transplant in CKRs, notwithstanding the good recovery of renal function and was instead significantly increased on day 14 after surgery. Taken together, our results indicate that plasma renalase levels may not predict plasma renalase activity. This dissociation between plasma renalase levels and activity in renal transplant recipients can be explained on the basis that plasma renalase circulates as a proenzyme that lacks enzymatic activity under baseline conditions. 12 It was suggested that the mechanism underlying the inhibition of plasma renalase at baseline may involve the interaction of the enzyme with an inhibitory substance in plasma. 12 Thus, one can hypothesize that plasma renalase might be less inhibited in CKRs, not only before transplant but also after the recovery of renal function.
The present results in patients with ESRD showing an increased plasma renalase activity fit well with our recent observations in the rat remnant kidney 20 and further suggest that circulating renalase may be less inhibited, not only in patients with ESRD but also in kidney transplant recipients, with good recovery of renal function. The results of our experiments evaluating the inhibitory effect of plasma on urinary renalase activity are in agreement with this hypothesis. Actually, the addition of plasma from healthy donors markedly inhibited the urinary renalase activity throughout the study period whereas the addition of plasma from corresponding LKR did not inhibit urinary renalase activity overtime.
It was suggested that the mechanism underlying the inhibition of plasma renalase at baseline may involve the interaction of the enzyme with an inhibitory substance in plasma. 12 Although the molecular identity of the putative plasma renalase inhibitor is currently unclear, evidence has been provided that activation of plasma renalase can be triggered by increases in blood pressure and/or surges in catecholamine levels, namely epinephrine. 12 In the present study, we found a strong positive correlation between plasma epinephrine levels and plasma renalase activity. This finding is particularly interesting given that epinephrine was found to be the preferred substrate for renalase. 11
Another interesting finding of the present study was the observation that urinary renalase levels and activity were markedly increased in patients with ESRD. Similarly to that found with circulating renalase levels, the changes in urine renalase levels overtime closely correlated with both renal function and plasma norepinephrine levels.
The observation that measured urine renalase activity closely accompanied the changes observed in urine renalase levels is not unexpected if one takes into consideration that, differently to plasma renalase, urine renalase possesses full enzymatic activity at baseline. 12
The daily urinary levels of dopamine were markedly decreased in patients with ESRD and the recovery of renal function in CKRs was accompanied by a progressive increase in urine dopamine output. These findings agree well with the previous findings showing that the decrease in renal function is accompanied by decreased renal dopamine output.2,21 These findings, when viewed collectively with the recent observations that renalase metabolizes dopamine, 11 suggest that urinary renalase might play a role in the regulation of renal dopamine output. In the present study, urine dopamine levels negatively correlated with urine renalase levels but did not correlate with urine renalase activity. Further studies are needed to prove or disprove the possible role of renalase on regulation of the renal dopaminergic system activity.
In summary, the present study shows that plasma and urine renalase levels and activity are significantly increased in patients with ESRD when compared to healthy donors. Plasma and urine renalase levels closely depend on both renal function and sympathetic nervous system activity whereas plasma renalase activity may be not predicted by changes in plasma renalase levels. It is suggested that epinephrine mediated activation of circulating renalase may occur in renal transplant recipients with good recovery of renal function. The increase in plasma renalase activity observed in ESRD patients and renal transplant recipients can be explained on the basis of reduced inhibition of the circulating enzyme.
Footnotes
Author contributions
JQS and MP participated in the experimental design. JQS, ISS, CFC, LSS, IF, CC, LC and RV participated in sample collection and conducted the experiments. JQS, MP, ISS, CFC and BSM participated in interpretation of the studies and analysis of the data and review of the manuscript. JQS and MP wrote the manuscript.
Acknowledgments
We thank Paula Serrão and the Institute of Pharmacology and Therapeutics, Faculty of Medicine, University of Porto for the facilities. We also thank the nursing staff from Nephrology Department of São João Hospital Center. This study was supported by grants PIC/IC/83029/2007 and PEst-OE/SAU/UI0725/2011 from Fundação para a Ciência e a Tecnologia/COMPETE/FEDER. Janete Quelhas-Santos is a PhD student supported by the fellowship SFRH/BD/39066/2007 from Fundação para a Ciência e Tecnologia/FSE.