
Abstract
Hypertension causes cerebral artery remodeling and increases the risk of stroke. Renin angiotensin system blockade during the development of hypertension has therapeutic effects even after treatment withdrawal. Mineralocorticoid receptor (MR) activation has been implicated in artery remodeling and impaired endothelial function. The possibility that there is a critical therapeutic window for MR antagonism has not been investigated. We hypothesized that temporary MR antagonism while hypertension develops would improve middle cerebral artery (MCA) structure and function in stroke-prone spontaneously hypertensive rats (SHRSP), even after treatment withdrawal. Six-week-old SHRSP were treated with spironolactone (25 mg/kg/day) from 6 to 12 weeks and when aged to 18 weeks, these rats were compared to age-matched untreated SHRSP. Surprisingly, temporary spironolactone treatment reduced the MCA outer and lumen diameter but had no effect on the wall thickness. Temporary spironolactone treatment improved nitric oxide and endothelium-derived hyperpolarizing factor mediated dilation but had no effect on blood pressure. Spironolactone treatment caused a very small reduction in the damage caused by permanent focal cerebral ischemia. These results suggest that temporary MR antagonism during the development of hypertension has divergent effects on the MCA, in that it causes a potentially detrimental reduction in the lumen diameter while improving vasodilation.
Keywords
Introduction
Hypertension increases the risk of stroke.1,2 Hypertension also causes middle cerebral artery (MCA) remodeling, which includes a reduction in the artery lumen diameter and an increase in the wall thickness and wall-to-lumen ratio in arteries from hypertensive rats compared to control rats.3,4 The MCAs and other large cerebral arteries carry a significant proportion of the cerebrovascular resistance. 5 Thus, inward MCA remodeling can detrimentally effect blood flow regulation and increase the risk of end-organ damage including stroke. 6
The mechanisms underlying hypertensive MCA remodeling are not completely understood. 4 Several studies suggest that the renin-angiotensin-aldosterone system (RAAS) is involved in the remodeling process. Angiotensin receptor blockers (ARBs) prevent the inward remodeling observed in spontaneously hypertensive rats (SHR).7,8 Angiotensin converting enzyme inhibitors (ACEIs) and ARBs improve artery function and the control of cerebral blood flow in hypertensive rats.9–12 The third active component of the RAAS, aldosterone, activates the mineralocorticoid receptor (MR). MR activation has significant detrimental effects on the cerebral vasculature.13,14 A link between MR activation and stroke has been established in rodents. MR antagonists (spironolactone and eplerenone) prevent spontaneous hemorrhagic strokes without lowering blood pressure in SHRSP fed a high-salt diet. 15 Compared to control SHRSP, spironolactone treated SHRSP also have smaller cerebral infarcts after the induction of permanent cerebral ischemia. 16 The converse is also true; direct MR activation with deoxycorticosterone acetate (DOCA) in Wistar rats causes an increase in the damage resulting from cerebral ischemia. 14 Increased aldosterone levels have also been linked to an increased risk of stroke in the population. 17 Studies of patients with primary aldosteronism (PA) provided the first links between stroke and aldosterone. 18 Comparisons of PA patients and patients with essential hypertension show that PA patients suffer from more strokes, despite having lower blood pressure than the patients with essential hypertension.19,20 Patients with increased plasma aldosterone, caused by glucocorticoid-remediable hypertension, also have an increased risk of stroke.21,22
We have shown that MR antagonism both prevents 3 and reverses 23 MCA remodeling in SHRSP. While these studies suggest MR blockade is beneficial, it should be noted that MR antagonists do have significant side effects. Both spironolactone and eplerenone can cause significant hyperkalemia 24 and spironolactone has anti-androgenic effects. 25 Eplerenone does not have the same anti-androgenic effects as spironolactone, but it is also not as efficacious and has a shorter half-life. 26 Therefore, identifying a positive effect of temporary MR blockade could be therapeutically important as it could reduce the side effect burden in patients.
The developmental phase of hypertension is a critical therapeutic window, and drug intervention during this time has long-lasting benefits.27–29 ARB treatment from 4 to 8 weeks of age prevents femoral artery remodeling and reduces blood pressure in 12-week-old genetically hypertensive mice. 28 ACEI treatment from 2 to 6 weeks of age 27 and from 4 to 30 weeks of age 29 in SHR lowers blood pressure, even after treatment withdrawal. The beneficial effects of spironolactone treatment while hypertension develops in the SHRSP are remarkable. Spironolactone treatment from 6 to 12 weeks of age completely prevents MCA remodeling and reduces the damage caused by cerebral ischemia to levels similar to that observed in normotensive rats.3,16 The 6–12-week treatment window includes the time when blood pressure is increasing rapidly in the SHRSP,3,30 but is should be noted that spironolactone does not lower blood pressure in the SHRSP.3,23,31 Our goal was to test if the positive effects of MR blockade on the MCA were maintained after treatment withdrawal. We hypothesized that temporary spironolactone treatment followed by withdrawal would improve MCA structure, endothelium dependent dilation, and the outcome of cerebral ischemia.
Materials and methods
Animals and treatments
Male SHRSP were obtained from the breeding colony housed at Michigan State University. Six-week-old male SHRSPs were treated with spironolactone (25 mg/kg/day) in the food for six weeks, the treatment was then terminated and the rats were aged to 18 weeks. This treatment will be referred to as temporary spironolactone treatment. Age-matched untreated SHRSPs were used as controls. The dose of spironolactone used was based on our previous studies3,23 and those of other people.31,32 The dose selected is higher than that required to inhibit the actions of aldosterone in vivo. 33 Rats were maintained in a temperature-controlled environment on a 12:12 h light:dark cycle, with tap water and regular chow ad libitum. The experimental protocol was approved by the Institutional Animal Care and Use Committee at Michigan State University and in accordance with the American Physiological Society’s “Guiding Principles in the Care and Use of Animals.”
Measurement of blood pressure
Blood pressure was measured by tail-cuff plethysmography using a CODA 6 VPR rat tail-cuff blood pressure system (Kent Scientific, Torrington, CT, USA) as described previously. 34
Analysis of MCA structure and serotonin mediated contraction
MCA structure and contractile function was assessed as described previously.3,23 At 18 weeks of age, rats were anesthetized with isoflurane. Blood was collected by cardiac puncture after thoracotomy, the rat was then decapitated and the brain was removed. Body and tissue weights were recorded. The first branch-free segment of the MCA most proximal to the Circle of Willis was dissected and placed in cold physiological salt solution (PSS, in mM: 141.9 NaCl, 4.7 KCl, 1.7 MgSO4, 0.5 EDTA, 2.8 CaCl2, 10.0 HEPES, 1.2 KH2PO4, and 5.0 glucose). Arteries were mounted on two glass micropipettes and secured with silk thread in a pressure myograph (Living Systems Instrumentation, Burlington, VT, USA). A blind-sac, or zero-flow, experiment was created by closing off the distal pipette; arteries that did not hold pressure were discarded. The vessel was then pressurized to 80 mmHg and the chamber was placed atop an inverted microscope connected to a camera and monitor. Vessels were bathed in warm PSS and allowed to equilibrate for 40 min. Videomicroscopy and a calibrated video dimension analyzer were used to obtain vessel outer and lumen diameters and wall thickness in micrometers. Superfusion of serotonin (5-HT, 10−9–10−4 M) was used to determine MCA contractility. The percent diameter change from baseline was calculated using the following formula: % change from baseline = [(vessel diameter − spontaneous tone vessel diameter)/(passive vessel diameter − spontaneous tone vessel diameter)]×100. Myogenic tone generation was measured at the beginning of the experiment. Tone was calculated using the following formula: %tone = [1-(active lumen diameter/passive lumen diameter)]×100. 35 The passive diameter was measured immediately after the MCA was placed in the cannula, and the active diameter was measured after the development of tone. Arteries that did not generate at least 20% spontaneous tone were discarded. To assess passive structure, MCAs were placed in calcium-free PSS containing 2 mM EGTA plus 10−5 M sodium nitroprusside (SNP) and a pressure-response curve was constructed by increasing the intralumenal pressure from 3 to 180 mmHg, and thereafter pressure was raised in 20 mmHg increments. The wall-to-lumen ratio, circumferential wall stress, and wall strain were calculated. 36 Passive distensibility was calculated as described previously. 37 The elastic modulus (β-coefficient) was calculated from the stress/strain curves using an exponential model (y = aeβx) where β is the slope of the curve: the higher the β-coefficient the stiffer the vessel.
MCA dilation
A separate group of rats were generated to assess endothelium-dependent dilation as described previously. 38 MCAs were obtained as described above and were mounted on an inflow and outflow pipette (Danish Myo Technology, Aarhus, Denmark). The inflow pipette was attached to a reservoir perfusion system that allowed the intralumenal pressure to be set at 80 mmHg. The intralumenal flow rate was adjusted to maintain shear-stress at a physiological level of 20 dynes/cm2 using the formula t = 4ηQ/πr3, where t is shear-stress, η is the viscosity of the PSS (0.7cp at 37°), Q is the flow through the lumen (mL/s), and r is the internal radius of the vessel (cm). Experiments were recorded, and the diameter was measured using DMT Vessel Acquisition System 6.1 software (DMT, Aarhus, Denmark). MCAs that did not develop at least 20% spontaneous tone after being warmed and pressurized were discarded. Two endothelium dependent dilators were added to the luminal perfusate in a cumulative fashion, 2-methylthioadenosine 5′-triphosphate (2-MeS-ATP, 10−10–10−5 M) was used to assess nitric oxide (NO) mediated dilation, and uridine 5′-triphosphate (UTP, 10−10–10−5 M) was used to assess the combined effects of NO and endothelium-derived hyperpolarizing factor (EDHF) mediated dilation. 39 Superfusion of SNP (10−9–10−4 M) was used to assess endothelium-independent dilation. Vessel maximum diameter was determined with calcium-free PSS containing 2 mM EGTA plus 10−5 M SNP in the superfusion bath.
MCA occlusion
Cerebral ischemia was induced using the intralumenal suture occlusion model developed by Longa et al. 40 Rats were anesthetized with isoflurane and their body temperature was maintained at 37℃. A midline incision was made on the scalp to expose the skull for measurement of pial flow by scanning laser Doppler as described previously. 41 A laser Doppler flow probe was attached to the skull for the duration of the surgery to measure blood flow to the region supplied by the MCA. The carotid artery was exposed through a midline incision. The lingual and thyroid arteries were cauterized, and the external carotid and pterygopalatine arteries were ligated. A 3-0 nylon monofilament with a rounded end (Doccol, Redland, CA, USA) was inserted into the common carotid artery and advanced through the internal carotid artery to occlude the MCA at its origin in the circle of Willis. MCA occlusion was verified by a drop in flow as measured by both scanning laser Doppler and the Doppler flow probe. After 24 h, rats were anesthetized and the brain was collected, sliced, and stained as described previously. 41 Digital images of brain slices were obtained and the infarct size was expressed as a percentage of the hemisphere infarcted using the flowing equation: ((VL−VC)/VC) × 100 where VL is the volume of the infarcted hemisphere and VC is the volume of the control hemisphere. 42
Plasma analyses
Plasma ion concentrations were measured using a NOVA 5 analyzer (NOVA Biomedical, Waltham, MA, USA). Plasma aldosterone was measured using a commercially available ELISA kit (Cayman Chemical, Ann Arbor, MI, USA) following the manufacturer’s instructions.
Statistical analysis
Data are shown as mean ± SEM. Physiological parameters and logEC50s were analyzed by Student’s t-test. Vessel structure, myogenic reactivity, contractility, and dilation were analyzed by two-way analysis of variance (ANOVA) with a Bonferroni post-test. A P value of 0.05 or below was considered significant.
Results
Physiological parameters
Physiological parameters in 18-week-old SHRSP after temporary spironolactone treatment from 6 to 12 weeks
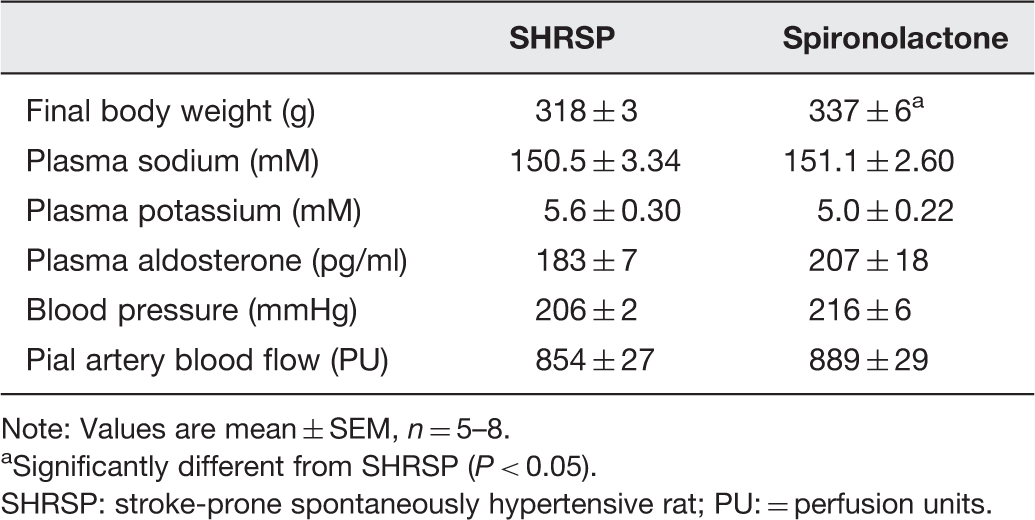
Note: Values are mean ± SEM, n = 5–8.
Significantly different from SHRSP (P < 0.05).
SHRSP: stroke-prone spontaneously hypertensive rat; PU: = perfusion units.
MCA tone and reactivity
Passive vessel structure in 18-week-old SHRSP after temporary Spironolactone treatment from 6 to 12 weeks
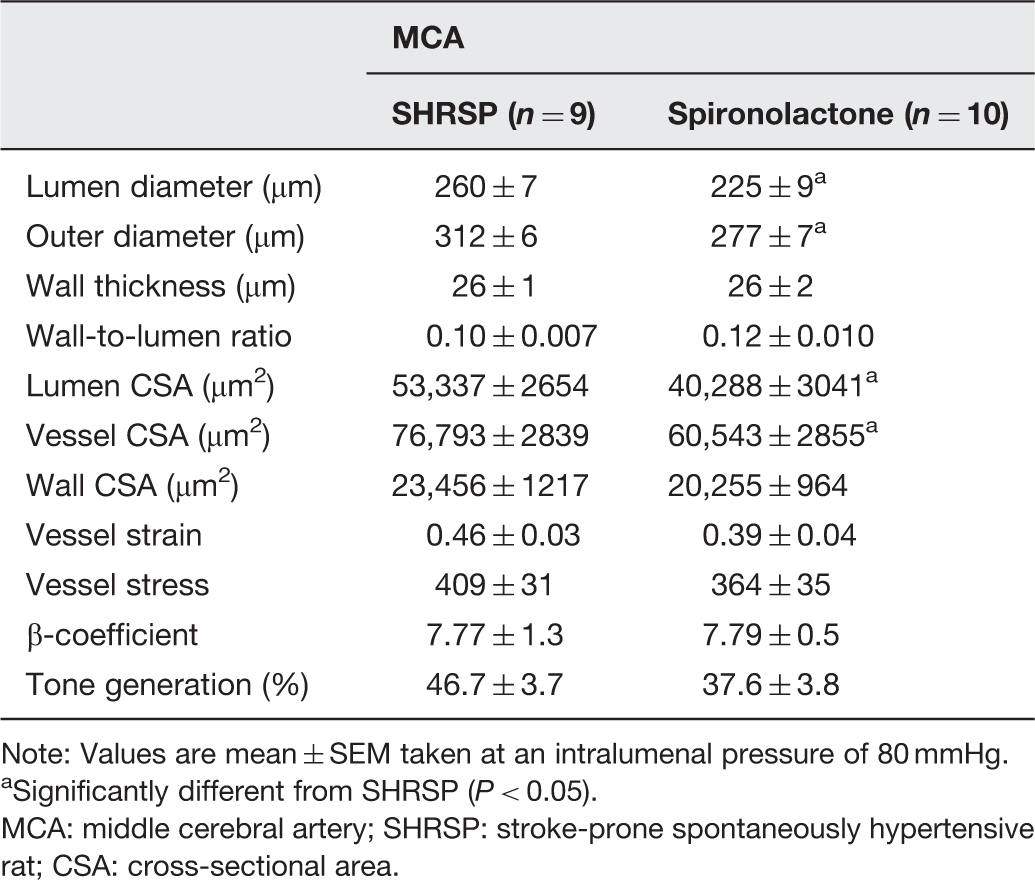
Note: Values are mean ± SEM taken at an intralumenal pressure of 80 mmHg.
Significantly different from SHRSP (P < 0.05).
MCA: middle cerebral artery; SHRSP: stroke-prone spontaneously hypertensive rat; CSA: cross-sectional area.
MCA structure
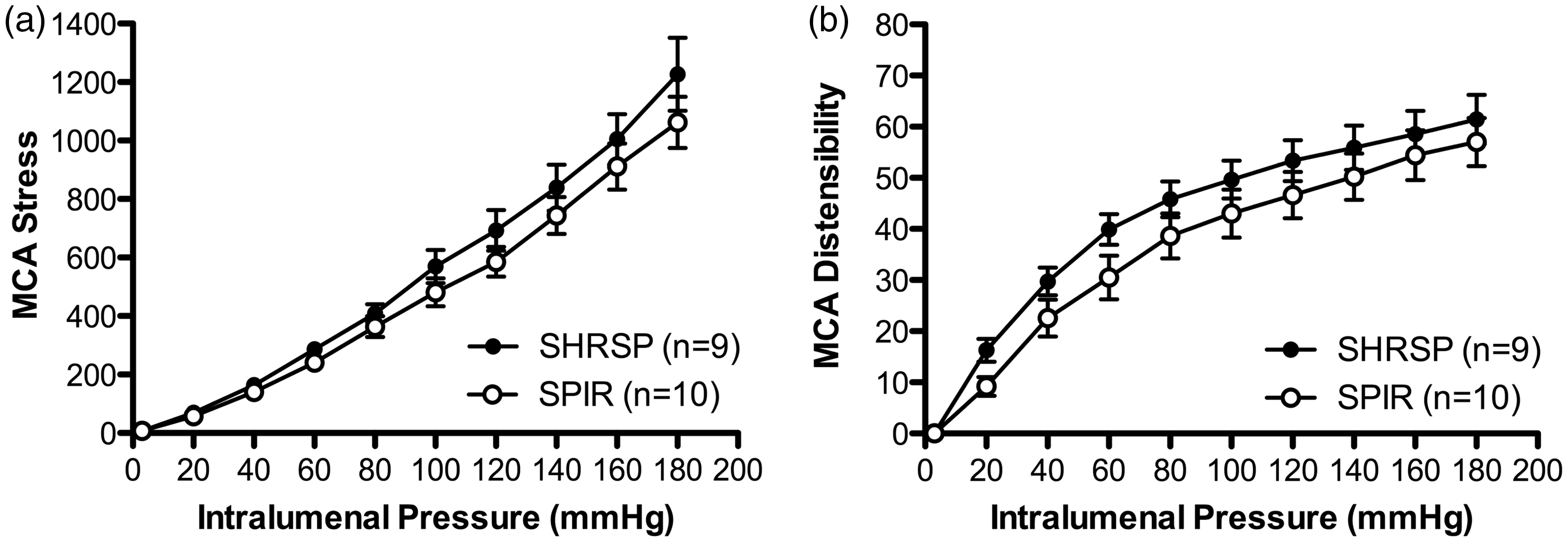
MCA passive structure was assessed by pressure myography under calcium free and zero flow conditions. The MCA lumen and outer diameters were reduced in the temporary spironolactone treated rats compared to control SHRSP (Figure 1(a) and (b), respectively). MCA wall thickness was unchanged by temporary spironolactone treatment (Figure 1c). Artery and lumen cross-sectional areas were decreased in temporary spironolactone treated rats compared to control SHRSP; the data obtained at an intralumenal pressure of 80 mmHg are presented in Table 2. The two-way ANOVA suggested significant differences existed between the control and temporary spironolactone treated groups for wall cross-sectional area, wall-to-lumen ratio (Figure 1d), strain, stress (Figure 2a), and distensibility (Figure 2b); however, the post hoc tests could not determine the location of the differences. The β-coefficient, calculated from the individual stress/strain curves, was used as a measure of MCA stiffness; temporary spironolactone treatment had no effect on this (Table 2).
Temporary spironolactone (SPIR) treatment from 6 to 12 weeks in 18-week-old stroke-prone spontaneously hypertensive rats (SHRSP) altered middle cerebral artery (MCA) passive structure, as evidenced by a reduction in the lumen diameter (a) and outer diameter (b). These changes occurred without a change in wall thickness (c) or post-test difference in wall-to-lumen ratio (c). *P < 0.05 in Bonferroni post-test, SPIR vs. SHRSP, and two-Way ANOVA. Values are mean ± SEM. The MCA was mounted in a pressure myograph and kept in oxygenated warm calcium-free PSS under no-flow conditions Temporary spironolactone (SPIR) treatment from 6 to 12 weeks in 18-week-old stroke-prone spontaneously hypertensive rats (SHRSP) decreased middle cerebral artery (MCA) stress (a) and distensibility (b), with no discernible difference in post hoc testing. *P < 0.05 in Bonferroni post-test, SPIR vs. SHRSP, and two-way ANOVA. Values are mean ± SEM. The MCA was mounted in a pressure myograph and kept in oxygenated warm calcium-free PSS under no-flow conditions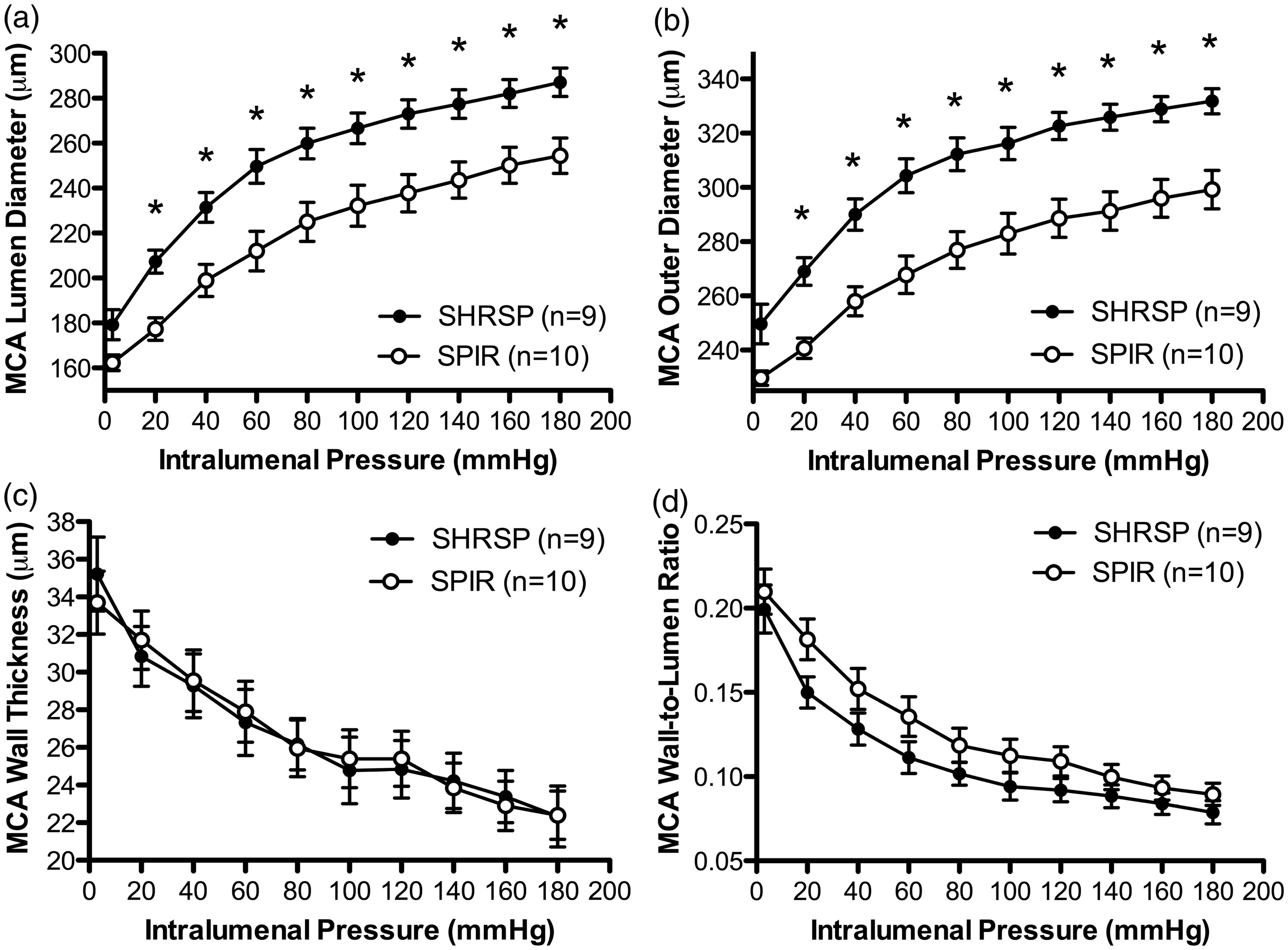
MCA dilation
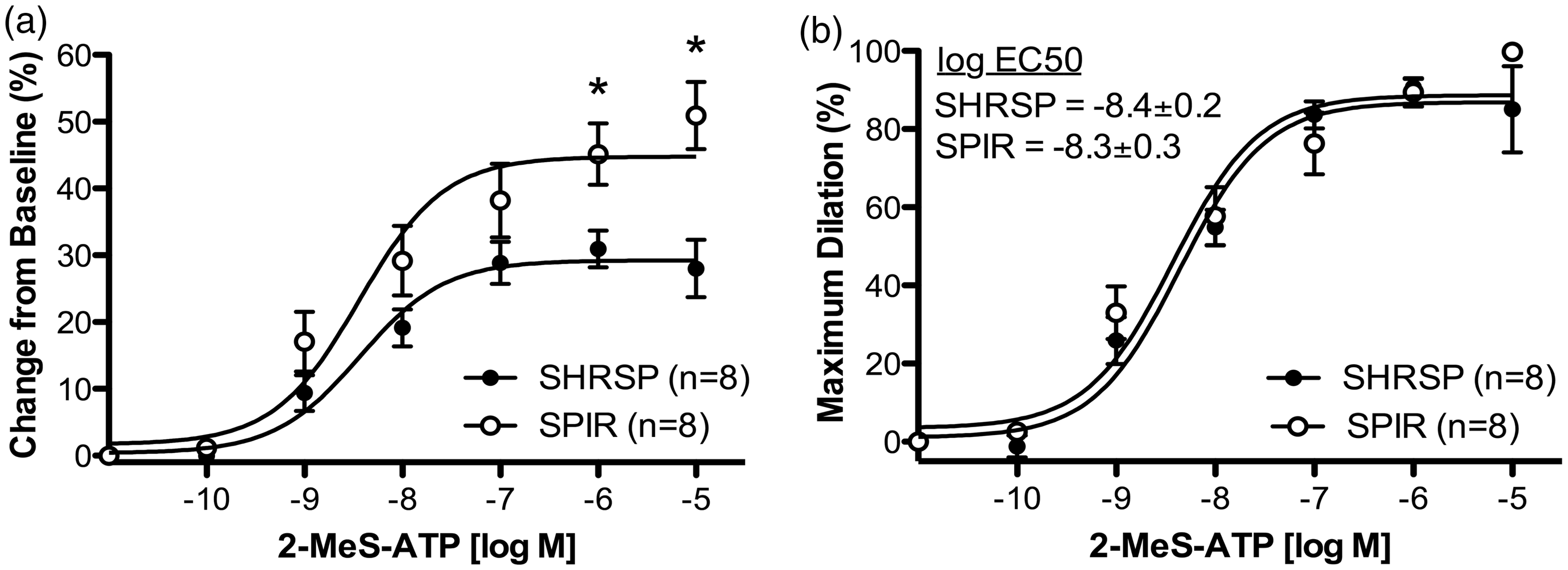
The dilatory capacity of the MCA was assessed by pressure myography with intralumenal perfusion of dilators. Temporary spironolactone treatment did not affect baseline MCA diameter prior to beginning the intralumenal perfusion of dilators (197.7 ± 8.7 vs. 199.1 ± 4.1 µm, spironolactone vs. SHRSP). Temporary spironolactone treatment increased NO mediated MCA dilation in response to 2-MeS-ATP (Figures 3a). The sensitivity of the MCA to 2-MeS-ATP was unchanged as evidenced by the lack of a difference in the EC50 (Figure 3b). Temporary spironolactone treatment also increased EDHF mediated MCA dilation to UTP (Figure 4a). The MCAs from temporary spironolactone treated rats were also more sensitive to UTP as evidenced by a reduction in the EC50 for UTP in the MCAs from the spironolactone treated rats (Figure 4b). Temporary spironolactone treatment did not alter the arteries’ response to the NO donor SNP (Figure 5(a) and (b), respectively).
Temporary spironolactone (SPIR) treatment from 6 to 12 weeks in 18-week-old stroke-prone spontaneously hypertensive rats (SHRSP) improved NO mediated endothelium-dependent dilation of the middle cerebral artery (MCA) to 2-MeS-ATP. Spironolactone treatment increased the change from baseline (a), with no change in sensitivity (b) after intralumenal perfusion of 2-MeS-ATP. *P < 0.05 in Bonferroni post-test, SPIR vs. SHRSP, two-Way ANOVA, and Student’s t-test. Values are non-linear curve fit of mean ± SEM. The MCA was mounted in a pressure myograph and kept in oxygenated warm PSS under 80 mmHg of intralumenal pressure and physiological flow Temporary spironolactone (SPIR) treatment from 6 to 12 weeks in 18-week-old stroke-prone spontaneously hypertensive rats (SHRSP) improved EDHF mediated endothelium-dependent dilation of the middle cerebral artery (MCA) to UTP. Spironolactone treatment increased the change from baseline (a) after intralumenal perfusion of UTP, and increased the sensitivity of the MCA (b). *P < 0.05 in Bonferroni post-test, SPIR vs. SHRSP, two-Way ANOVA, and Student’s t-test. Values are non-linear curve fit of mean ± SEM. The MCA was mounted in a pressure myograph and kept in oxygenated warm PSS under 80 mmHg of intralumenal pressure and physiological flow Temporary spironolactone (SPIR) treatment from 6 to 12 weeks in 18-week-old stroke-prone spontaneously hypertensive rats (SHRSP) did not alter endothelium-independent dilation of the middle cerebral artery (MCA) to the NO donor SNP, as evidenced by no change from baseline (a) or in sensitivity (b) after superfusion of SNP. *P < 0.05 in Bonferroni post-test, SPIR vs. SHRSP, two-way ANOVA, and Student’s t-test. Values are non-linear curve fit of mean ± SEM. The MCA was mounted in a pressure myograph and kept in oxygenated warm PSS under 80 mmHg of intralumenal pressure and physiological flow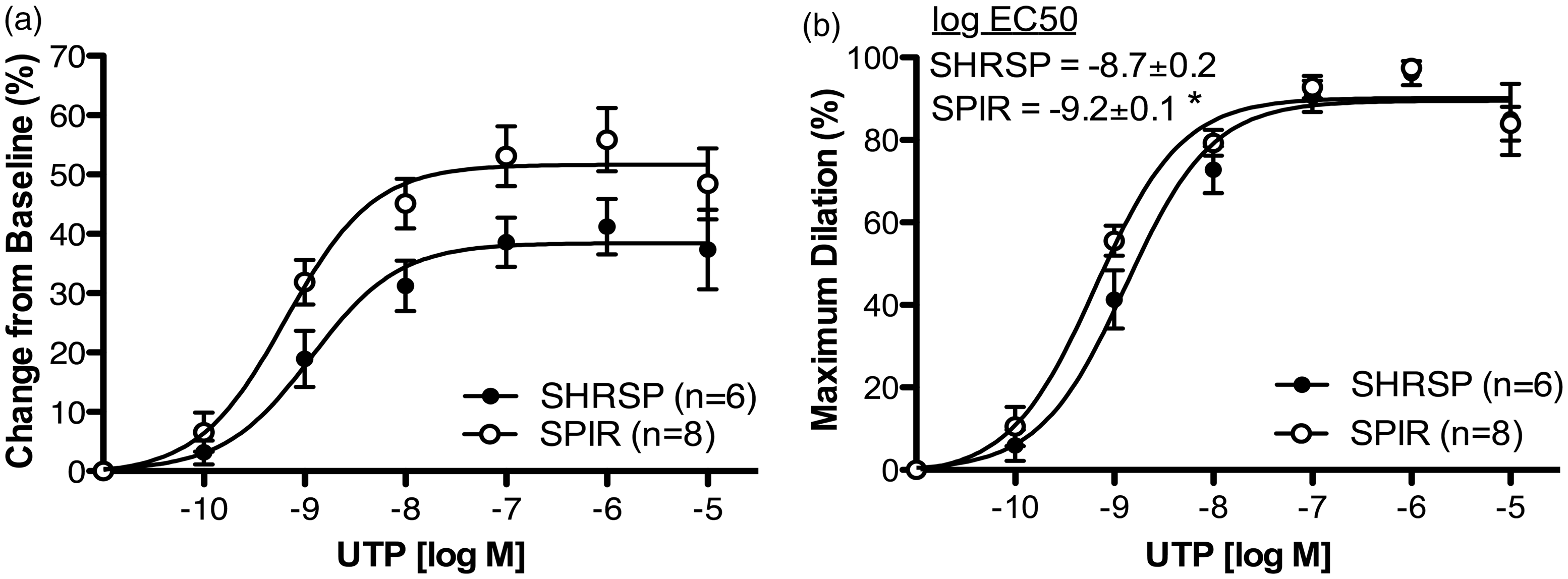

Outcome of MCA occlusion
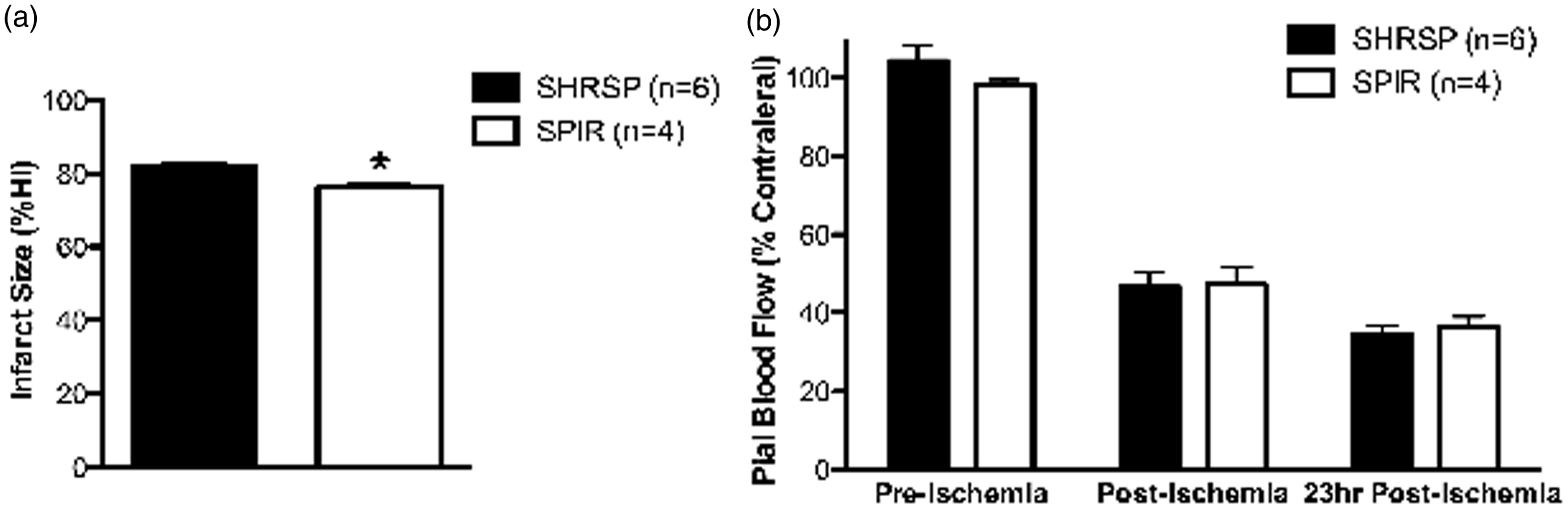
To assess the effects of the temporary spironolactone treatment on the outcome of cerebral ischemia, we conducted MCA occlusion studies using a 24-h permanent ischemia model. Temporary spironolactone treatment caused a small but significant reduction in the cerebral infarct size (Figure 6a). Global pial artery flow was assessed by scanning laser Doppler prior to and immediately after the induction of ischemia and immediately prior to euthanasia. The induction of cerebral ischemia caused a marked reduction in blood flow to the ischemic hemisphere. However, the magnitude of the reduction was similar in both control and temporary spironolactone treated rats (Figure 6b).
Temporary spironolactone (SPIR) treatment from 6 to 12 weeks in 18-week-old stroke-prone spontaneously hypertensive rats (SHRSP) caused a small but significant decrease in cerebral infarct size after permanent MCA occlusion (a), expressed as %hemisphere infarcted (%HI). Temporary spironolactone treatment had no effect on pial blood flow, as measured by scanning laser Doppler and expressed as %contralateral hemisphere. *P < 0.05 in Bonferroni post-test, SPIR vs. SHRSP, two-way ANOVA, and Student’s t-test. Values are mean ± SEM ▪▪▪▪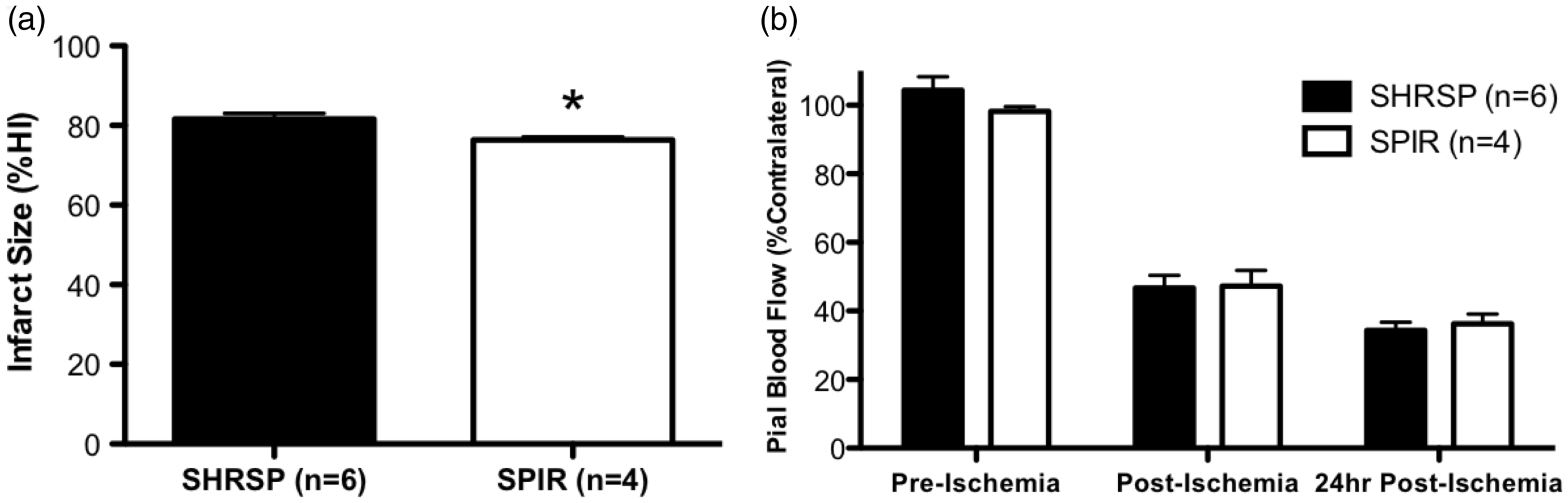
Discussion
Previous studies suggest that interfering with the RAAS during the development of hypertension has prolonged beneficial effects after drug withdrawal.27–29 These studies have focused on the effects of ACEI and ARBs; the temporary effects of MR blockade have not been investigated. Our hypothesis was that MR antagonism during the development of hypertension would increase the MCA lumen diameter, reduce the wall thickness, and improve the endothelium dependent dilation even after drug withdrawal. We found that temporary spironolactone treatment improved endothelium-dependent dilation compared to control rats. We did not observe the predicted improvement in MCA structure with temporary spironolactone treatment. Compared to control SHRSP, temporary spironolactone treatment caused a reduction in the passive lumen and outer diameter of the MCA. The improved dilation and inward remodeling observed in the temporary spironolactone treated rats may have opposing effects on the outcome of cerebral ischemia. However, it appears that the potential negative effects of inward artery remodeling in the temporary spironolactone-treated rats were counteracted by the improved endothelium dependent dilation. The cerebral infarcts produced after 24 h of ischemia were smaller in the temporary spironolactone-treated rats compared to control SHRSP. It is important to note that the reduction in infarct size observed was very small and is not likely to be physiologically relevant.
Comparison on the effects of spironolactone treatment on MCA structure using various treatment regimes
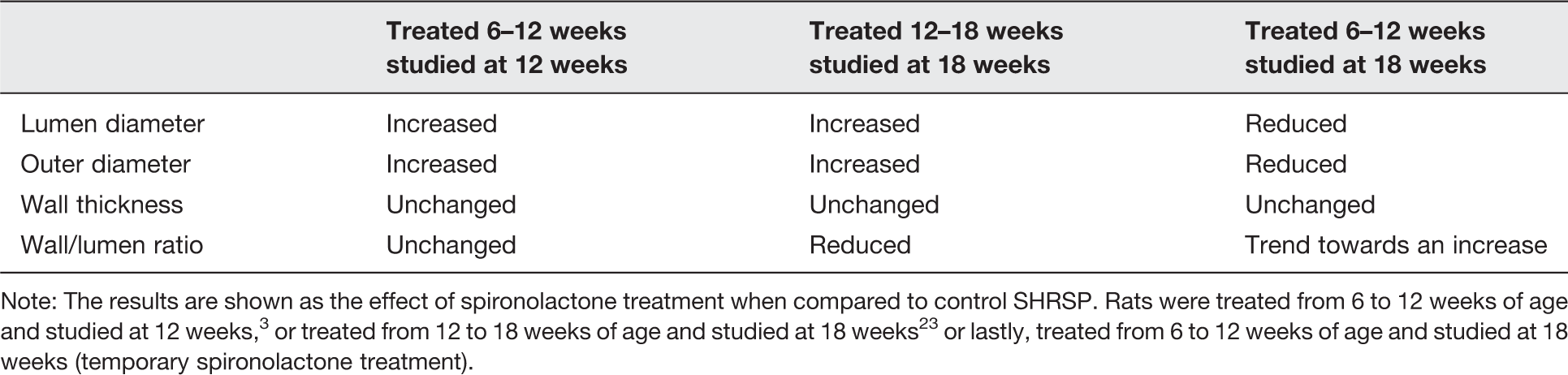
Note: The results are shown as the effect of spironolactone treatment when compared to control SHRSP. Rats were treated from 6 to 12 weeks of age and studied at 12 weeks, 3 or treated from 12 to 18 weeks of age and studied at 18 weeks 23 or lastly, treated from 6 to 12 weeks of age and studied at 18 weeks (temporary spironolactone treatment).
Temporary spironolactone treatment did not lower blood pressure. This is in keeping with previous studies where SHRSP were treated with spironolactone for six weeks beginning at 6 or 12 weeks3,23 and with studies from other groups using SHRSP.31,32 MR antagonists are widely used in humans to treat heart failure, 26 and they are increasingly being used to treat resistant hypertension.43,44 We recognize that the absence of an effect of spironolactone on blood pressure in the SHRSP is at odds with the antihypertensive effects in humans, and this could be a function of the polygenic nature of the hypertension in SHRSP. It should be noted that patients who respond to MR blockade are also taking other RAAS modifying drugs.43–45 In this study, the SHRSP were only treated with spironolactone so that only the effects of MR blockade were investigated. One caveat to our study is that the blood pressure was measured using tail-cuff. However, we have reported that the tail-cuff method used here provides results that are very similar to those obtained by telemetry. 3 The data presented does not rule out the possibility that spironolactone affects the circadian variability in blood pressure, or the blood pressure during the awake cycle. However, in previous studies treating rats from 6–12 3 and from 12–18 23 weeks with spironolactone, we did not observe difference in nighttime blood pressure.
Our analysis of MCA structure showed that arteries from the temporary spironolactone treated rats underwent an inward remodeling process compared to the control SHRSP. We have shown that MR antagonism with spironolactone from 6 to 12 weeks in SHRSP prevents inward MCA remodeling (Table 3). When the MCAs were studied at the end of the 6–12-week spironolactone treatment, we observed an increase in the lumen and outer diameter, without a change in the wall thickness or wall-to-lumen ratio. 3 We have replicated these findings with two other MR antagonists, the more specific drug eplerenone and canrenoic acid, the active metabolite of spironolactone. Both drugs caused an approximately 40 µm increase in the MCA lumen diameter at an intralumenal pressure of 80 mmHg when compared to control untreated SHRSP. Therefore, the finding of a significant reduction in the MCA lumen diameter in the temporary spironolactone-treated rats was surprising. This finding suggests that compared to control SHRSP, the MCAs in spironolactone-treated SHRSP went from being outwardly remodeled to being inwardly remodeled after spironolactone withdrawal. The caveat to this study is that we have no way of knowing in this particular group of rats if the MCA was indeed outwardly remodeled at 12 weeks of age, but the evidence described above suggests it would be.
Hypertension increases the tangential stress on the MCA wall, 46 and the MCA remodels in an effort to maintain the stress in a physiological range in the face of elevated intralumenal pressure. The hypertensive remodeling process in cerebral arteries includes an increase in the wall thickness and wall-to-lumen ratio, and a reduction in the lumen diameter.47,48 Failure of cerebral arteries to remodel in response to hypertension has detrimental effects including vasogenic edema and blood-brain barrier breakdown. 49 Therefore, the inward remodeling of the MCA after spironolactone withdrawal may be an adaptive response to reduce wall stress. This appears to be the case as wall stress was unchanged between the control and temporary spironolactone-treated rats. We have shown that continuous MR antagonism increases the MCA lumen diameter and the tangential stress on the artery wall in SHRSP. 23 While one would expect that this would have detrimental effects on end organ damage, it appears not to be the case. MR blockade in SHRSP from 6 to 12 weeks reduces the damage caused by permanent focal cerebral ischemia when compared to control untreated SHRSP 16 and it reduces the incidence of hemorrhagic stroke in SHRSP fed a high salt-diet. 31 Combined, these studies suggest that MR antagonism holds artery remodeling at bay, but when the drug is withdrawn the remodeling process is reactivated. The potential clinical implications of these findings remain to be elucidated but they may be of potential importance for patients considering terminating MR antagonism therapy. The mechanisms involved in the post-treatment remodeling process remain to be investigated. MR activation has been implicated in collagen deposition, 50 vascular smooth muscle cell proliferation, 51 and vascular inflammation. 52
A reduction in the artery lumen diameters without any other compensatory effects will increase cerebrovascular resistance and therefore reduce cerebral blood flow. Pial artery flow was not different between the temporary spironolactone treated rats and control rats. It is possible that we did not observe a change in blood flow because another mechanism in the artery was compensating for the reduction in the lumen diameter. The baseline lumen diameter data obtained prior to the analysis of artery dilation suggest that this may be the case. Despite the large difference in the passive lumen diameter, the active lumen diameters were similar suggesting that enhanced dilator pathways compensate for the inward artery remodeling in the temporary spironolactone treated rats.
We found a marked improvement in endothelium dependent dilation in the rats that underwent temporary spironolactone treatment compared to control SHRSP. To the best of our knowledge, this is the first study to show that MR antagonism improves the dilator capacity of cerebral arteries. Other studies have shown that MR antagonism improves endothelial function in peripheral arteries.53,54 Temporary spironolactone treatment increased the efficacy of NO-mediated dilation, that was not due to a difference in sensitivity of the smooth muscle to NO, as dilation with the NO donor SNP was not different. This improvement in NO bioavailability could be due to increased NO production or improved bioavailability. The later seems likely; oxidative stress impairs endothelial function and NO bioavailability55,56 and increased MR activation has been linked to increased oxidative stress. 57 Temporary spironolactone treatment also increased dilation through EDHF-dependent mechanisms stimulated by UTP; in this case, both the efficacy and sensitivity were increased.
The finding of an enhanced sensitivity of the MCA to EDHF, but not NO, suggests that the two dilator pathways may be regulated by different mechanisms. Other studies suggest this may be the case. EDHF-mediated dilations are enhanced following stroke and traumatic brain injury, whereas dilations caused by NO are compromised.58,59 An improvement in EDHF-mediated dilation in the absence of cerebral ischemia may translate to improved collateral blood flow following injury. 60 An improvement in EDHF-mediated dilation in the absence of cerebral ischemia, as shown here, may translate to improved collateral blood flow following injury. MR antagonism has been shown to decrease ischemic damage by MCAO, 16 and one could speculate that this is due in part to the improved EDHF-mediated dilation from MR antagonism.
At present, we cannot tell if the enhanced EDHF or NO mediated dilations compensate for the reduction in the MCA lumen diameter when cerebral ischemia is induced. The artery structure data would cause us to predict that the cerebral infarct size would be increased in the SHRSP after temporary spironolactone treatment. We saw a small reduction in the infarct size, but this may be an artifact of survival bias. Six of the eight control SHRSP that underwent MCAO survived to 24 h, whereas only four of the eight spironolactone-treated rats survived. It is therefore possible that the rats that died did have larger cerebral infarcts that caused them to be unable to survive until the 24-h time period.
To the best of our knowledge, these are the first studies to show a situation where the artery is inwardly remodeled and dilation is improved. This suggests that in the MCA the inward remodeling process is not intrinsically linked to impaired artery dilation. These studies also suggest that the MR regulated component of remodeling and endothelial dysfunction in the cerebral arteries are not temporally linked. The studies suggest that MR blockade as hypertension develops has the capacity to improve dilation, but not the artery structure in the long term. The benefits of MR antagonism, temporary or chronic, on blood flow regulation are wide reaching and may improve the outcomes of stroke, Alzheimer’s disease, dementia, and chronic cerebral hypoperfusion. This study adds weight to the idea that vessel function also needs to be taken into account when determining one’s risk of cardiovascular disease.
Footnotes
Author Contributions
Both authors participated in the design, interpretation, and analysis of the data. JLM performed the experiments, wrote the draft manuscript, and reviewed the final manuscript. AMD edited the draft manuscript.
Acknowledgements
This work was supported by a grant from the American Heart Association (0840122N:AMD).