
Abstract
Accidental or intended radiation exposure in mass casualty settings presents a serious and on-going threat. The development of mitigating and treating agents requires appropriate animal models. Unfortunately, the majority of research on radiation enteritis in animals has lacked specific assessments and targeted therapy. Our study showed beagle dogs, treated by intensity-modulated radiation therapy (IMRT) for abdominal irradiation, were administered single X-ray doses of 8–30 Gy. The degree of intestinal tract injury for all of the animals after radiation exposure was evaluated with regard to clinical syndrome, endoscopic findings, histological features, and intestinal function. The range of single doses (8 Gy, 10–14 Gy, and 16–30 Gy) represented the degree of injury (mild, moderate, and severe, respectively). Acute radiation enteritis included clinical syndrome with fever, vomiting, diarrhea, hemafecia, and weight loss; typical endoscopic findings included edema, bleeding, mucosal abrasions, and ulcers; and intestinal biopsy results revealed mucosal necrosis, erosion, and loss, inflammatory cell infiltration, hemorrhage, and congestion. Changes in serum diamine oxides (DAOs) and
Introduction
If the 11th September, 2001, terrorist attacks caused extreme worry about terrorist activities, including biological and chemical weapons and radiological or nuclear attacks, then the 11th March, 2011, Fukushima nuclear crisis in Japan, triggered by the earthquake and tsunami, and the recent third nuclear test by the North Koreans have transformed these fears into panic. People enjoy the great convenience that is provided by civil nuclear energy; at the same time, we should not ignore its negative effects. Clinically, almost all patients receiving pelvic or abdominal radiotherapy experience some form of gastrointestinal (GI) symptoms, which significantly reduces their quality of life as well as adding a significant economic burden. 1 One of the medical countermeasures to prevent radiation threats is comprehensive understanding of the diseases induced by radiation exposure.
Research into the pathological mechanisms, prevention, treatment, and mitigation of radiation injury must be based on the development of animal models, which could promote radiation science. Radiation-induced enteropathy animal models date back to the latter part of the last century, with some having occurred even earlier. Most of the studies on large animal models of radiation-induced enteropathy have been related to exposure modality, radiation dose, irradiation dose rate, and preliminary studies of the mitigation of radiation injury. Subsequently, limited by study conditions, the pace of research on radiation-induced enteropathy slowed until advances in technology and methods in rodent-based research in recent years prompted significant, important progress in radiation-induced enteropathy. Unfortunately, there has also been significant controversy. One cause for concern is the species, strains, and genetic backgrounds of the animals. Radiation counter-measures that show promise in small animals should be further confirmed in larger animal models, such as in canines. 2 Moreover, radiation-induced GI toxicity, clinical symptoms, and treatment efficacy in canines are similar to those in humans, so the further application of large animal radiation-induced enteropathy models is an important research topic.
Our study focused on large animals to analyze acute radiation enteritis by clinical and endoscopic characteristics, as well as histology and serology, after different doses of abdominal X-ray irradiation. Further understanding of acute radiation-induced enteropathy could provide references and guidance for subsequent treatment.
Materials and methods
Animals and ethics statement
All ordinary level female 11 - to 26-month-old beagles weighing 12.03 ± 0.53 kg were used in the experiment after one week of adaptive feeding in the laboratory. The animals were obtained from the Department of Animal Experiments at the General Hospital of Shenyang Military Command. All of the experiments were approved by the Institutional Animal Ethics Committee of Shenyang Military General Hospital (Permit Number: SYXK[JUN2012-0002]) and were in accordance with the Declaration of the National Institutes of Health’s Guide for the Care and Use of Laboratory Animals (Publication No. 85-23, revised 1985); some principles were adapted from the Animal Models Workshop (Centers for Medical Countermeasures against Radiation [CMCRs], 2008).
The ‘‘3Rs’’ serve as the cornerstone for our animal research guidelines. Rational design of experiments included reduction of experimental animals, choosing 2 Gy as dose interval of variation and endoscopic specimen collection. Necessary experimental measures were taken as follows: use of 5% local hemostatic agent (Monsell's solution, 5.5 mL sulfuric acid, 7.5 mL nitric acid, 10.45 g ferrous sulfate, and 100 mL distilled water), shortening of surgery time, intraoperative energy supplement and given indomethacin (1 mg/kg per os [po]) twice daily after irradiation exposure. We conducted humane endpoints by intravenous injection of KCl (2 mmol/kg) under anesthesia along with incurable hemorrhage, and/or beyond the control of bloody stools, and/or unable to walk and take in food, and/or persistent hypothermia.
Irradiation
Thirty-three dogs were randomly divided into 11 groups according to single irradiation dose (8, 10, 12, 14, 16, 18, 20, 22, 24, 26, and 30 Gy). The animals were anesthetized and intubated with a continuous intravenous infusion of propofol (0.5 mL/kg), using a micromedicine infusion-pump. Spiral computed tomography (CT) scanning accurately fixed the position of the intestine and ADAC Pinnacle 3.0 treatment planning system was used for dose calculation before X-ray irradiation. Plan acceptance criteria required that at least 95% of the dose covered 99% of the planning target volume (PTV). All of the animals were irradiated to the PTV at a single-dose range from 8 to 30 Gy using a 6 MeV linear accelerator (Siemens Primus, Germany). Additionally, irradiation region was located in small intestine avoiding the surrounding vital organs, such as spine, kidney, spleen, and stomach. Dose distribution with isodose lines of different colors and dose volume histogram (DVH) were used to evaluate plans (Figure 1).
Example dose distribution and DVH of IMRT irradiation plan for one dog. CT slices show irradiation dose distribution in the abdomen at the level of intestine treated with 12 Gy. DVH represents the target coverage of the plan in accordance with the initial goal for the target volume. Prescription was for the 95% isodose. (A color version of this figure is available in the online journal.)
Clinical observation, assessment, and supportive care
Beginning on the purchase date, clinical observation of the beagles was performed and continued throughout the entire process of the animal experiments. The basic characteristics, including the weight and rectal temperature, and a series of symptoms, such as nausea, diarrhea, bloody stool, and vomiting, were all recorded every day. The method was modified from Nicholas Dainiak et al. and the Medical Treatment Protocols (METREPOL) team and European Organization for Research and Treatment of Cancer/Radiation Therapy Oncology Group (RTOG/EORTC) grade to assess the severity of changes in the clinical signs and symptoms.1,3
If oral intake was poor and the dog continued to lose weight, intravenous Ringer's solution (15–20 mL/kg) was administered twice per day until the dog recovered from GI toxicity. 4 Supportive care was largely based on the animals’ weights and conditions to determine the correct energy supplement.
Intestinal function experiments (serum d-xylose test and DAO test)
The animals were administered 5%
Blood samples were deposited in disposable vacuum storage vessels (heparin) and centrifuged to obtain plasma. Plasma diamine oxide (DAO) activity was measured in the test groups before irradiation and within seven days after X-ray treatment. The serum was diluted 10-fold with ultra-pure water according to the method of the Canine DAOElisa Kit (My BioSource, San Diego, USA)
Endoscopy and tissue preparation
The animals completed the necessary bowel cleansing preparation by being oral administered a 1 -L polyethylene–glycol solution four times within 2 h, followed by an overnight fast. A magnesium sulfate enema (25 g/100 mL saline solution) was administered at least 6–8 h prior to the start of observation. The animals were given general anesthesia during the enteroscopic examination, and representative injury findings were obtained for tissue samples under endoscopy (EC-450ZW, EC-590ZW/M, FUJINON, Tokyo, Japan). All of the procedures were performed by experienced endoscopists. The evaluation of the endoscopic observations used the Vienna Rectoscopy Score (VRS) system. 7
Intestinal histology was also performed on intestinal tissues within five days after radiation exposure as well as on autopsy within 4 h after death. Tissue specimens, washed with 0.9% saline for five times, were cut to suitable sizes to fix and save in 4% formalin and 2.5% glutaraldehyde solutions, respectively. Tissue samples (4 -µm paraffin-embedded sections) were processed and prepared for standard histological procedures using paraffin slicing machine (CUT4062, SLEE, Mainz, Germany).
Transmission electron microscopy (TEM)
Fixed specimens were washed by 0.1 mmol/L sterile phosphate-buffered saline (PBS) (pH 7.4), postfixed with 2% osmium tetroxide solution, and washed by 0.1 mmol/L sterile PBS (pH 7.4) again. After washing, samples were dehydrated first through a series of graded alcohols, then with propylene oxide, and finally infiltrated and embedded in Spurr resin, sectioned, and stained with uranyl acetate and lead citrate. Examination was made with a TEM (JSM-1200EX, Jeol, Tokyo, Japan) at an accelerating voltage of 80 kV.
Scanning electron microscopy (SEM)
A portion of fixed specimens was washed by 0.1 mmol/L sterile PBS (pH 7.4), then dehydrated in a series of ethanol gradients before it was dried to the critical point. The dried specimens were sputter-coated with gold by a sputter coater at 10–15 nm and were then examined with a SEM (JSM-T300, Jeol) at 15 kV.
Evaluation of intestinal damage
Light microscopy analysis
Radiation-induced intestinal mucosal injury was measured in all of the tissues. hematoxylin and eosin (H&E)-stained sections were evaluated at 10× and 40× magnification by an unbiased observer. Mucosal damage was classified as follows:8,9 0 (normal); 1 (surface epithelium damaged); 2 (<50% mucosa damaged); 3 (>50% mucosa damaged); and 4 (entire mucosa damaged). The intensity of the inflammatory infiltration was graded as mild, moderate, or severe, according to the number of inflammatory cells and their intensity (from + to ++++). Vascular congestion was analyzed for absence or presence with intensity (from + to ++++).
Based the appearance of the mucosal damage, vascular congestion, and inflammatory infiltration, specific scores from 0 (absent) to 4 (maximum intensity of each variable alone) were assigned. These points were totaled to obtain a new study parameter, called the damage grade, which ranged in value from 0 (absence of inflammation) to 12 (maximum inflammation found). In each section, the damage grade was determined based on these summed results. According to the score, the intestinal damage was stratified as absent or slight (0), mild (1, 2, 3 and 4), moderate (5, 6,7 and 8), or severe (9, 10, 11 and 12).
Electron microscopy analysis
Mucosal injury was quantified under TEM and SEM. Each specimen was graded as follows: normal or minor (alterations that could not be correlated with radiation with certainty); mild (intestinal villi partially damage and/or cell apoptosis present); moderate (most loss of intestinal villi and/or inflammatory infiltration and blood cell leakage); severe (complete loss of the intestinal villi and/or aggravated inflammatory infiltration and/or changes in smooth muscle cells).
Statistical analysis
All of the experimental data are expressed as means ± SDs, and the data were analyzed using SPSS software (version 16.0 for Windows). The following tests were used: one-way analysis of variance (ANOVA) and Spearman’s rank correlation. P < 0.05 was considered statistically significant.
Results
General observations
Grading system for clinical observations after irradiation a
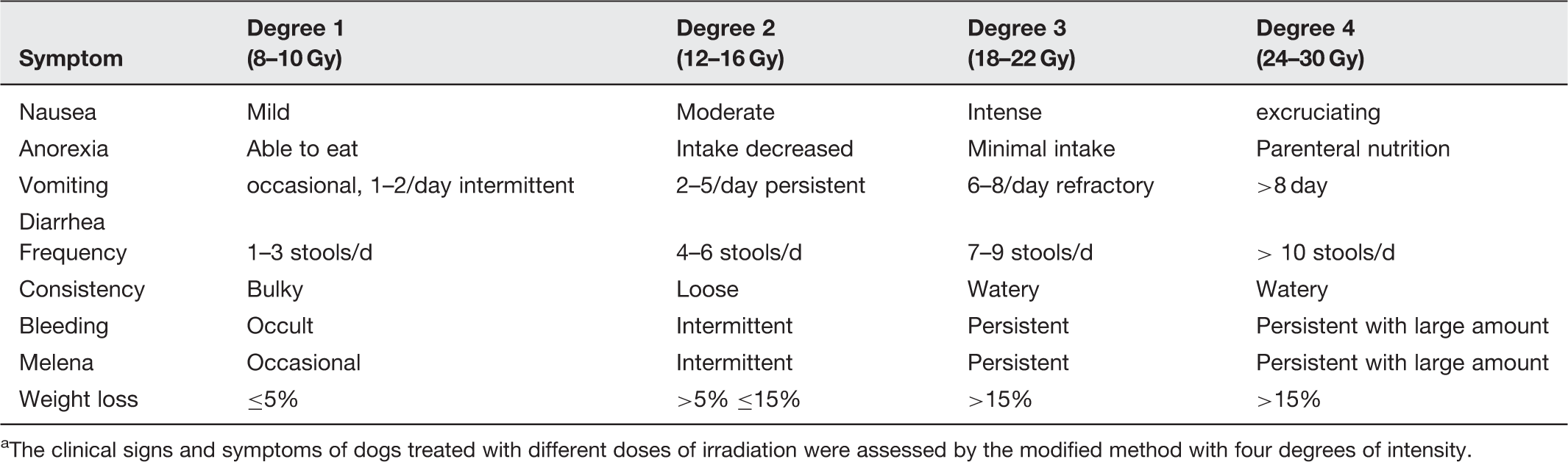
The clinical signs and symptoms of dogs treated with different doses of irradiation were assessed by the modified method with four degrees of intensity.
Vomiting
Animals treated with <10 Gy developed nausea and vomiting on day 4, and their symptoms disappeared within one week. Animals subjected to doses of 12, 14, and 16 Gy exhibited nausea and vomiting on day 2, and their symptoms were more frequent and heavier. When the doses exceeded 18 Gy, the symptoms developed 8 h after irradiation, following the introduction of a quantity of food and liquid, and the symptoms did not improve without any treatment. In addition, the stomach contents included largely yellow secretions.
Diarrhea
Diarrhea became more severe with increased irradiation doses. Changes in the stool were particularly apparent in the irradiated animals. Animals treated with 8 or 10 Gy began to develop diarrhea on day 4 or day 3, respectively. The animals treated with 12–16 Gy intermittently exhibited bloody stools. At doses greater than 18 Gy, the symptoms became progressively more severe. Furthermore, mucopurulent bloody stool might have indicated poor prognosis.
Early toxicity and mortality were dependent upon the single dose. High-dose abdominal irradiation has been linked to severe intestinal toxicity and increased mortality (Figure 2).
Kaplan–Meier survival analysis of dogs (n = 41, 11–26 mo old) receiving different treatments revealed that all dogs given 18–30 Gy died acutely within seven days. Among three dogs treated with 16 Gy, one died on day 15 and the others died on days 10 and 7. All three dogs that received 14 Gy survived for an average of 15 days. Two out of three dogs treated with 12 Gy survived more than 15 days, and the 3rd died on day 15 from septicemia. All of the dogs treated with 10 Gy (n = 3) and 8 Gy (n = 3) survived beyond one month (P < 0.05). (A color version of this figure is available in the online journal.)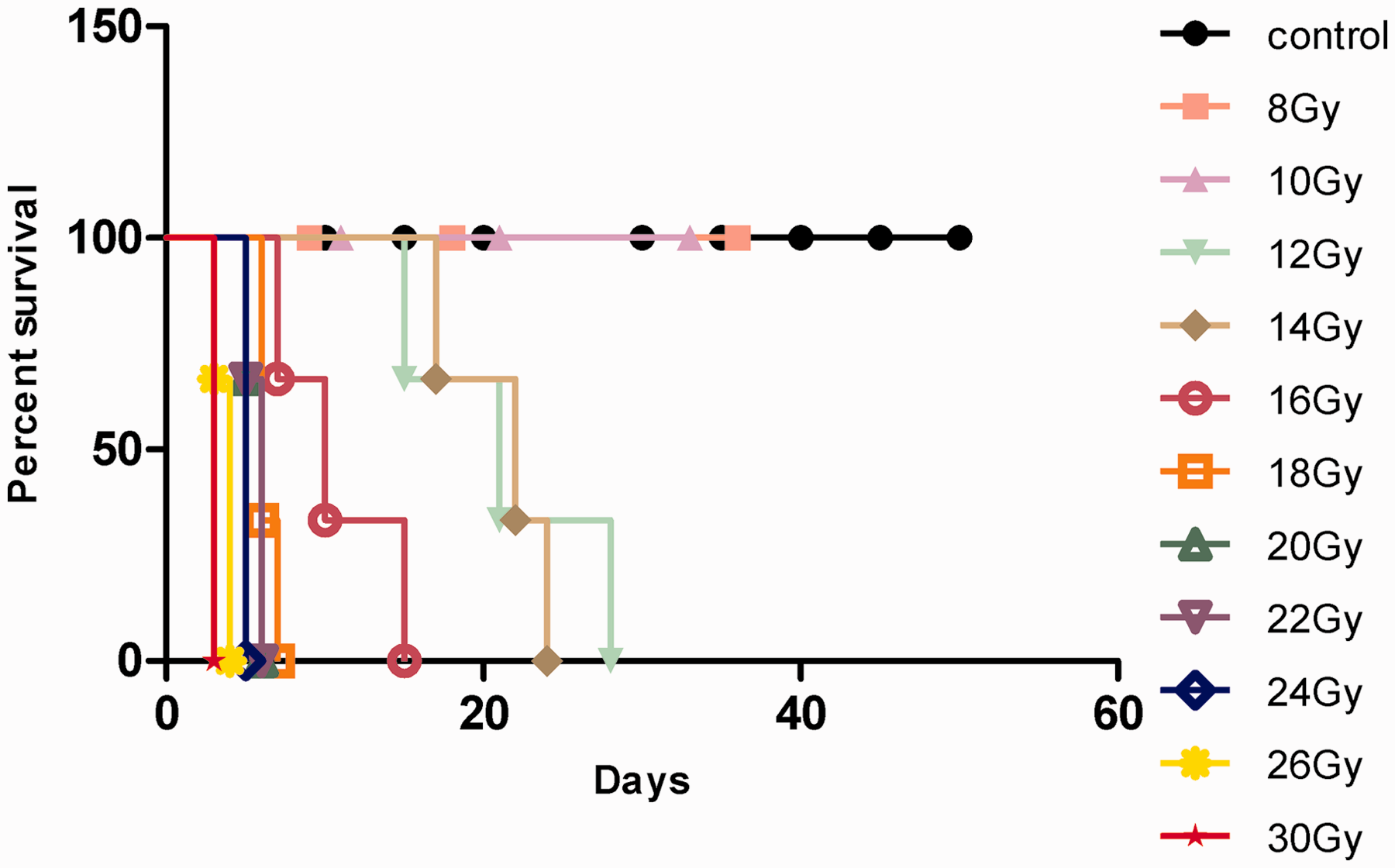
Changes in body temperature and weight
After irradiation, all of the animals exhibited changes in body temperature, with different ranges. An early hyperthermia phase was usually observed following irradiation. The temperature increased to a peak and then decreased to various degrees. During the period of recording, the temperature of dogs treated with less than 10 Gy changed within 1℃, but animals treated with doses greater than 10 Gy exhibited temperature fluctuations within the range of 2–4℃ with the same supportive care (Figure 3a, b, c).
The body temperature and weight curves for acute radiation in dogs administered different single doses. (a–c) The X-axis indicates days post-irradiation, and the Y-axis indicates body temperature in degrees celsius. (d–f) There was no difference between the treated groups and control group with regard to body temperature on the 1st day after irradiation. The temperature sharply increased on day 2 and day 3 after irradiation, especially for dogs administered >16 Gy (n = 21). The subjects exhibited peak hyperthermia on day 9 for the 12 Gy (n = 3) and 14 Gy (n = 2) groups and on day 5 for the 16 Gy (n = 2) and 18 Gy (n = 3) groups. Among the administered doses, dogs treated with 16 Gy are marked in red due to the last observation time point on days 10,11, or 12. The 8 Gy group (n = 3) did not exhibit significant weight loss, and the >10 Gy groups (n = 30) exhibited weight loss at different time points after irradiation, compared with the control group (n = 8) (P < 0.05). (A color version of this figure is available in the online journal.)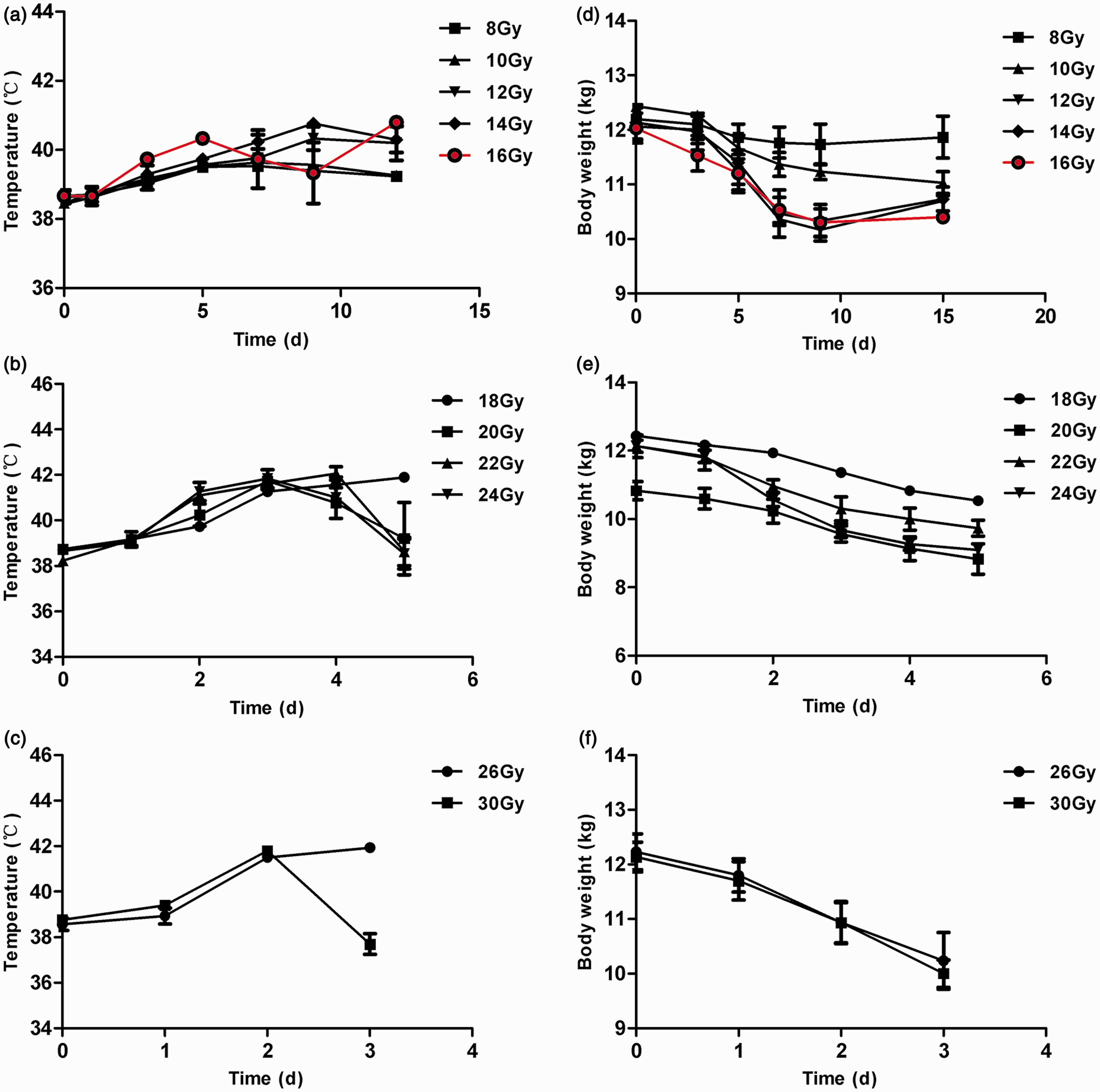
The changes in weight were related to the treatment doses, and as the radiation dose increased, there was a declining trend in weight at each detection time point (Figure 3d, e, f). Compared with pre-irradiation, severe weight loss was 25% for the dogs administered 24 Gy. Weight loss appeared much earlier at high irradiation doses, compared with the control group. The groups treated with ≥20 Gy exhibited apparent weight loss on day 2 and day 3 after irradiation, whereas weight loss in the 12–18 Gy and 10 Gy groups appeared on days 5 and 7 or days 9 and 12, respectively.
Effects of irradiation on intestinal function
We performed Serum 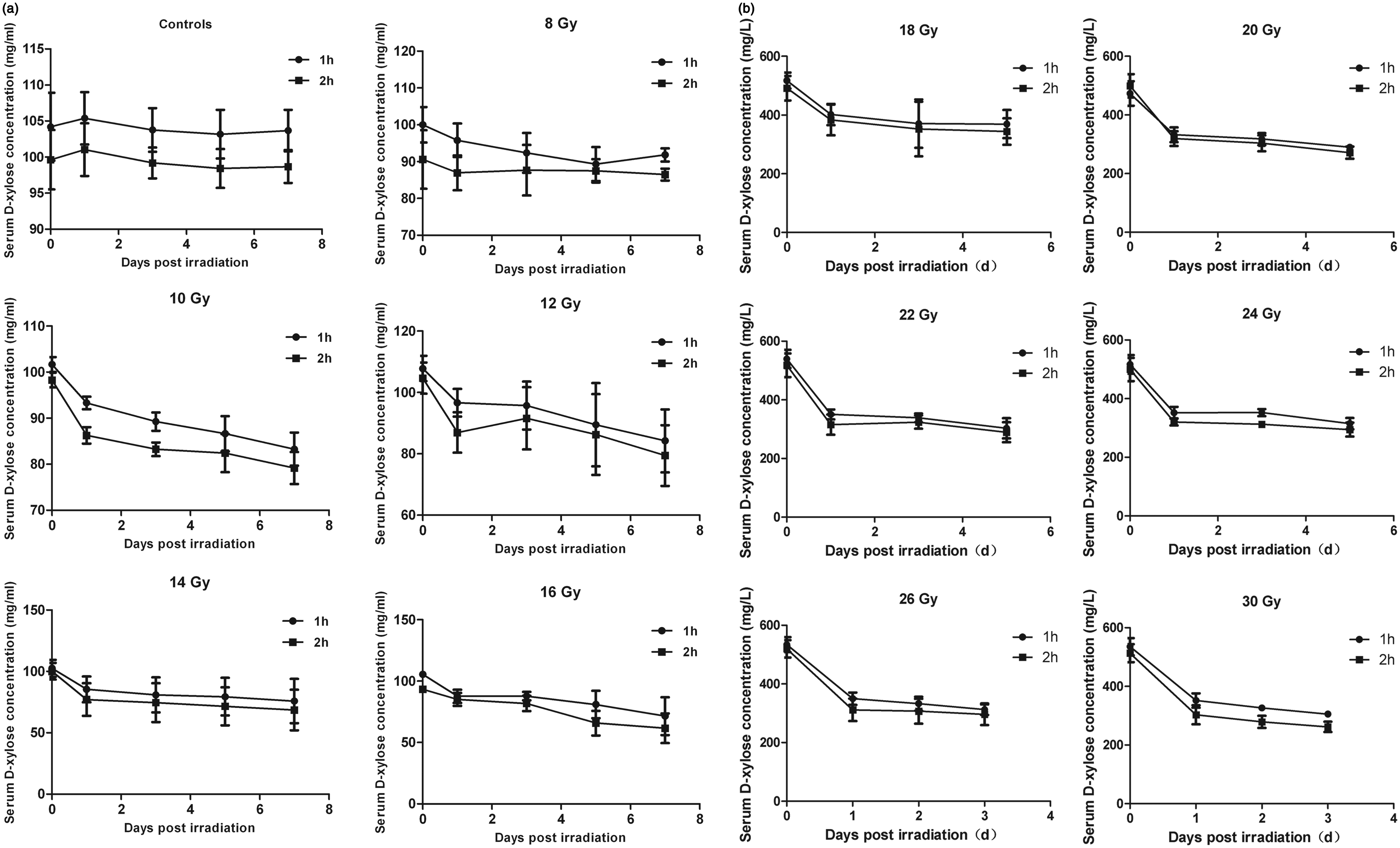
Serum DAO exhibited major increases on day 1 or day 3 in each group after irradiation (P < 0.05). Compared with the control group, the groups receiving greater than 14 Gy exhibited concentration changes on the 1st day, and groups receiving 10–14 Gy exhibited changes on the third day. The level of serum DAO exhibited a trend from high to low values with time in each radioactive group; furthermore, the high irradiation dose groups exhibited more obvious trends than the lower dose groups. However, there were no significant changes between the 8 Gy-treated group and the control group (Figure 5a, b).
The level of serum DAO reflected the barrier function of the intestine, and it varied with different irradiation doses. The changes of serum DAO appeared early on the 1st day after irradiation exposure, with a trend from high to low values. (a) The control group and 8–16 Gy groups showed changes in the DAO level at 0–7 days after exposure. (b) The 18–24 Gy groups exhibited obvious changes in the DAO level at day 1. day 3, and day 5 after irradiation. The 26–30 Gy groups showed significant DAO concentration changes at days 1–3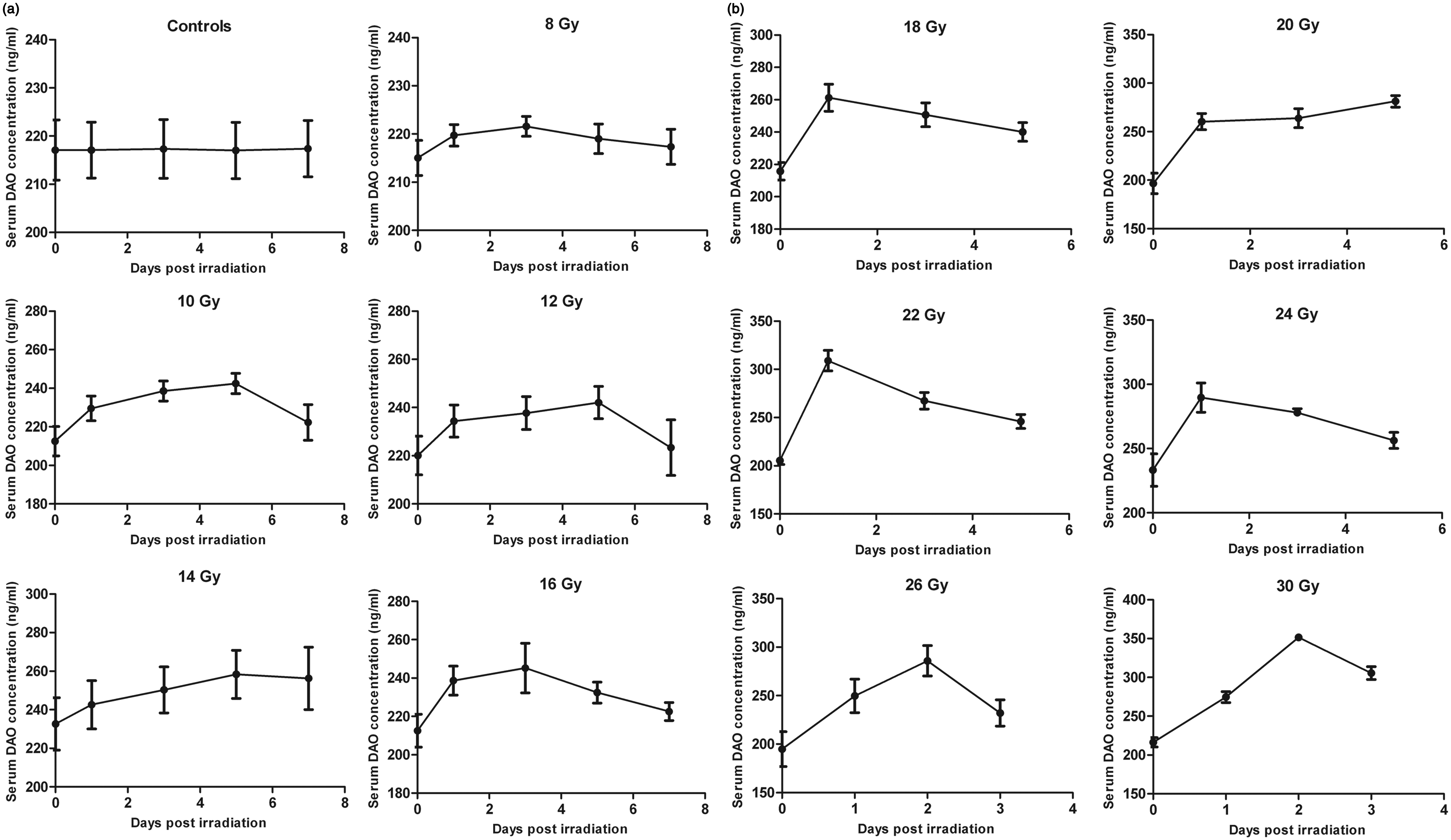
Endoscopic observation
The endoscopic images were correlated with the irradiation doses on the 3rd and 5th day after irradiation (Figure 6). This normal mucosa was smooth, and the mucosa began to appear slightly hyperemic, with edema at a dose of 8 Gy. With 10 and 12 Gy of irradiation, the mucosal inflammation was more severe and exhibited multifocal congestion, edema, and petechial hemorrhage. The 14 and 16 Gy doses resulted in lesions with diffuse hyperemia, edema, and flaky hemorrhages. Diffuse hemorrhages or erosion and different mucosal damage were observed at irradiation doses of 18–30 Gy. Typical ulcers were observed at 24 and 26 Gy of irradiation. The visible injury at 30 Gy included extensive mucosal exfoliation and loss of vascular architecture on the 3rd day after irradiation. The VRS system resulted in a score of 1 at less than 10 Gy, a score of 2–3 for 10–22 Gy, and a score of 4 at greater than 24 Gy. The endoscopic observation varied with the time after irradiation at the same dose (data not showed).
Intestinal damage as observed by endoscopy after different irradiation doses (8–30 Gy). The VRS corresponded with the irradiation doses as follows: 0, control; 1, 8 Gy; 2, 10 Gy; 2, 12 Gy; 2, 14 Gy; 2, 16 Gy; 2, 18 Gy; 2, 20 Gy; 2, 22 Gy; 4, 24 Gy; 4, 26 Gy; and 4, 30 Gy. This experiment was performed with fixed observation time at days 3, 5, and 7 after irradiation exposure. Due to there being no significant changes under endoscopic observation of the 8–14 Gy groups at three days after irradiation (data not shown), the endoscopy results were shown for the 8–14 Gy groups at five days after irradiation and the 16–30 Gy groups at three days after irradiation (n = 3 dogs/group). Each result is from one out of three independent experiments, respectively. (A color version of this figure is available in the online journal.)
Histological changes related to the radiation dose
Histology
Relationship between mucosal damage and radiation dose a

Scores represent the means ± SDs of three dogs in each group except the control group (n = 8). The sum of the individual scores from each category was divided by the number of animals in the group. The histologic changes were correlated well with the radiation doses, as tested by Spearman’s rank correlation test (P < 0.05, r = 0.965). Tissue specimens were obtained from endoscopic biopsies or postmortem histology specimens. The time points of endoscopic biopsy were at day 3 (16–30 Gy groups) and day 5 (8–14 Gy groups) after irradiation (n = 3 dogs/group).
The histological changes in the irradiated animals were detected in the intestinal specimens (Figure 7). These changes consisted of mucosal damage, inflammatory infiltration, and vascular congestion, with the extent of damage dependent on the irradiation dose. With 8 Gy of radiation, samples taken from the small intestine exhibited mild-grade changes on day 3 post-irradiation. Moderate mucosal damage was detected in dogs treated with 10–14 Gy. These animals exhibited partially damaged mucosa, glandular dilatation, inflammatory infiltration (+−+++), vascular congestion, and hemorrhage (+−+++). The mucosal damage was worse for dogs administered more than 14 Gy, with severe histologic findings, including diffuse intestinal necrosis, erosions, and exfoliation. In the higher-dose groups, additional prominent histologic changes included mixed inflammatory cell infiltration (neutrophils mainly), extensive congestion, and blood.
Characteristics of the intestinal tissue specimens after 8–30 Gy irradiation and hematoxylin and eosin (H&E) staining (n = 3 dogs/group). Compared with control group (n = 8), the 8 Gy group exhibited mild mucosal damage, inflammatory infiltration, and vascular congestion; the 10–14 Gy groups showed worse mucosal damage with moderate inflammatory infiltration and vascular congestion; and the 16–30 Gy groups showed even more severe mucosal damage or exfoliation, extensive congestion, and blood. Bars, 500 µm. (A color version of this figure is available in the online journal.)
Electron microscopy findings
Electron microscopic examination of the intestinal mucosa revealed some changes as follows: Figure 8a–d and Figure 9e–j were observed by TEM and SEM, respectively. Figure 8a reveals normal intestinal mucosa in the control group. Figure 8b exhibits partial mucosal damage, irregular karyotypes, and the condensation and margination of nuclear chromatin. The major injury modes were apoptosis and necrosis in the intestinal mucosa at mild doses (8 Gy). Moderate damage included loss of intestinal villi, inflammatory cell infiltration, and intravascular congestion with blood cell leakage (Figure 8c). With 20–30 Gy of irradiation, the common findings included aggravated inflammatory infiltration, severe diffuse hemorrhage, and complete loss of the intestinal mucosa (Figure 8d).
Transmission electron microscopy of the intestinal mucosa after radiation injury. (a) Normal intestinal villi and epithelial cells. (b) Apoptosis and partial loss of the intestinal villi in the marked epithelial cells could be found in the 8 Gy groups. (c) The 10–18 Gy groups had marked areas that indicated additional loss of microvilli of intestinal epithelium inflammatory cell infiltration, and intravascular congestion with blood cell leakage. (d) Note the inflammatory infiltration, diffuse hemorrhage, and complete loss of the mucosa. The 20–30 Gy groups were represented by severe damage. Bars, 2 µm Scanning electron microscopy findings of radiation intestinal injury. (a) Normal intestinal mucosa (control group, n = 8). (b) Partial loss of mucosa (8–14 Gy groups, n = 3/group). (c) The 16–18 Gy groups showed major loss of mucosa (n = 3/group). (d) Complete loss of mucosa and collagen fiber exposure were found in the 20–30 Gy groups (n = 3/group). (e) The disappearance of mucosa caused vascular structure exposure and blood cell leakage. (f) Marked new cell emergence was occasionally found in the high-dose irradiation groups (22 Gy group, once). a–e: Bars, 100 μm. f: Bars, 10 μm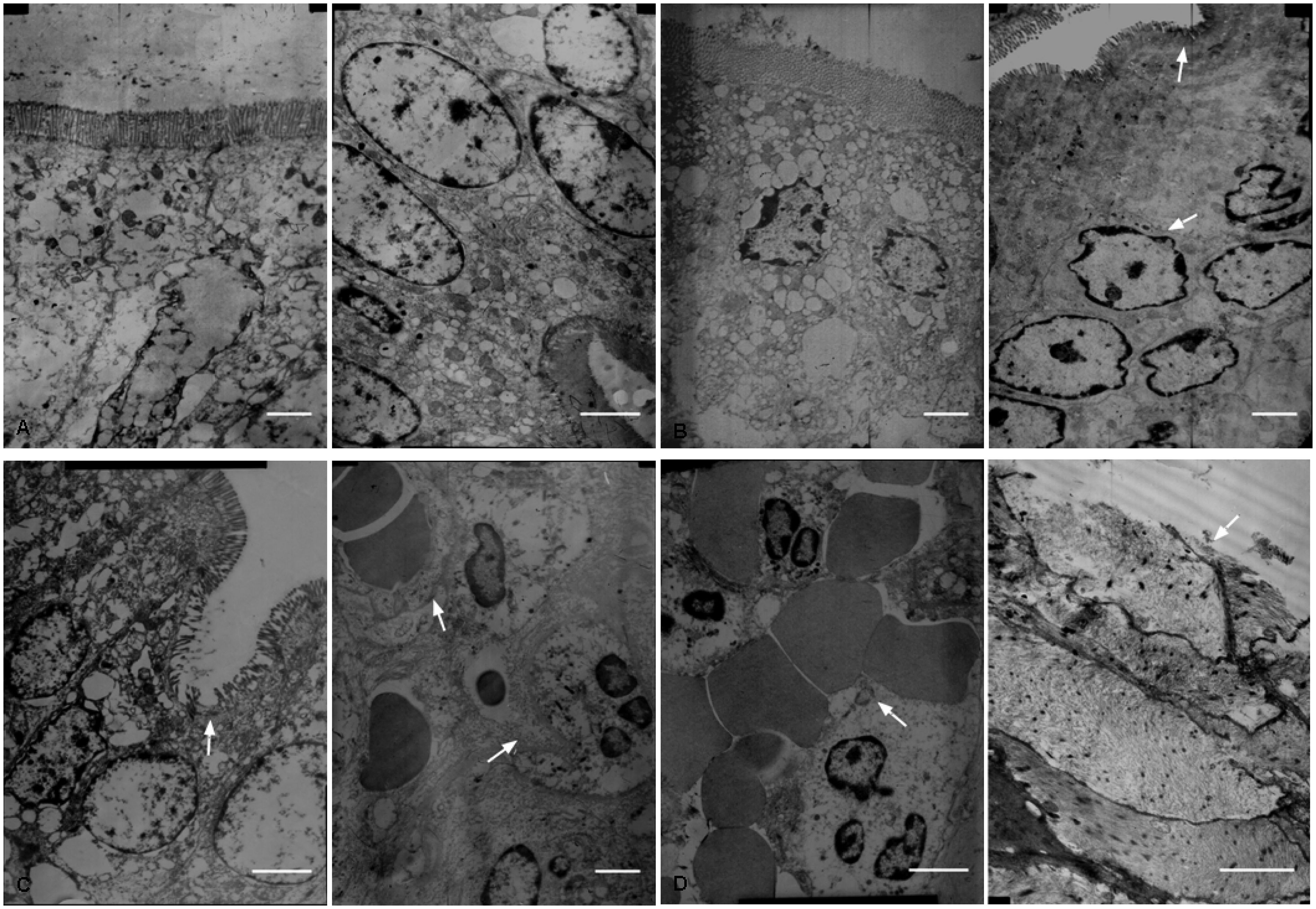

The findings of mucosal damage under SEM were also classified into three groups (mild, moderate, and severe), corresponding to observations by TEM. Compared with the controls (Figure 9e), mild damage included partial loss of mucosa in Figure 9f, and Figure 9g and h reveals expansion of mucosal loss. Severe damage was observed in the collagen fiber structure and blood vessel architecture, in addition to blood cell leakage and the emergence of new cells (Figure 9h–j).
Discussion
Clinically, there is no specific treatment for radiation enteropathy; treatment continues to rely on symptomatic relief. In developing new treatments, the patient's individual factors and the disease pathogenesis must be considered. For different conditions, it is therefore critical to explore pharmacodynamics, the timing of administration, and the dose and mode of administration to develop specific treatments. These factors have been our starting points for such research.
Our research on large canines attempted to analyze the injury severity of acute radiation enteritis induced by different radiation doses. Studies on large animal models of radiation intestinal damage have been performed since early during the last century. Most studies have focused on the radioactive source, radiation dose or dose rate, 10 exposure mode or time, and bone marrow or bone marrow stem cell treatment.11–13 Studies on mice administered total body irradiation (TBI) or total-abdominal irradiation (TAI) demonstrated two distinctly different modes of death, and TBI resulted in complex organ damage. 14 High total doses increased acute toxicity and early mortality, while low exposure rates were better tolerated than higher exposure rates, and dose fractionation reduced long-term toxicity compared with single-dose irradiation in the case of a total dose less than a critical threshold. 15 On the basis of this research, we developed for the first time an acute radiation enteritis model based on single-dose abdominal irradiation administered at different doses at a moderate dose rate by intensity-modulated radiation therapy (IMRT). In agreement with previous studies, we found that acute toxicity and mortality were correlated with different single doses.
The advantages of large animal radiation-induced enteropathy models are as follows: similar clinical manifestations to human beings; feasible diagnosis and treatment methods; and enrichment of species differences in radiation injury research.16,17
Compared with the classic initial symptoms of human acute radiation syndrome during the prodromal phase, the prodromal symptoms of canine acute radiation enteritis models also include the following: apathy, frequent emesis, diarrhea, nausea, vomiting, and bloody diarrhea.18,19 For humans exposed to TBI, vomiting can occur within minutes to hours, and diarrhea may also occur within 48 h after higher-dose exposure. 2 These early symptoms can occur during the first two weeks following abdominal radiotherapy. Furthermore, the time of onset of prodromal symptoms induced by TBI or TAI is dose-dependent. Dogs treated with <10 Gy developed vomiting and diarrhea on day 4 after irradiation, whereas vomiting and diarrhea in the 12–16 Gy groups occurred on days 2, and in the 18–30 Gy groups symptoms appeared within a few hours after irradiation. According to clinic observations of dogs, we found that radiation GI toxicity in the dogs was similar to that in humans, and the changes in body temperature and weight were correlated with different irradiation doses, which should be considered in clinical management.
We used the
Endoscopy examinations can visually observe changes in the intestinal tract in the same animals without sacrificing them; moreover, endoscopy can identify occult bleeding after radiation injury. This simple and practical method is suitable for dogs. To our knowledge, this is the first extensive study on radiation-induced intestinal damage by endoscopic examinations for dogs treated with different single irradiation doses. Clinical endoscopic researches on humans with radiation enteritis show that intestinal mucosal damage caused by radiation may exhibit elangiectasia, edema, hyperemia, erosion, ulceration, stricture, and necrosis depending on intensity of irradiation. 7 Most of mucosal changes were also observed by endoscope in dog models. Hamilton et al. 25 reported that a high dose of radiation may increase the risk for duodenal ulcerations and perforations in oncologic patients who receive abdominal irradiation. In our study, typical ulcers were found at irradiation dose of 24 Gy or more, moreover the mucosal damage was more serious with irradiation dose increased. The intestinal damage observed was consistent with the histological changes. The most significant changes were observed on different days after irradiation. Our findings were similar to those from a report by Northway et al. 26 However, the sequential appearance of the earliest endoscopic changes on different days depended on the single irradiation doses. The irradiation position or species perhaps plays an important role.
We combined histological scores with electron microscopic results to determine that the intestinal damage induced by X-rays depended on the single irradiation dose. This finding is in agreement with those of Kan et al. in rats. 27 However, the histological scores and sequential changes post-irradiation differed and could not be effectively compared due to differences in the species and irradiation fields.
The combination of clinical manifestations, intestinal function, endoscopy, and histological scores suggest a new means for classifying the severity of intestinal damage. The purpose of these observations was to develop a proper large animal model for studying acute radiation enteritis that mimics the human condition, to develop a suitable means to evaluate post-irradiation intestinal damage and to provide some diagnostic references and treatment basis. The ultimate goal is to find new medical countermeasures to cure radiation enteritis for therapeutically locally irradiated oncological patients. Using this methodology, we found that the dogs administered 8 Gy exhibited Degree 1 clinical signs and symptoms, slight function changes, and mild endoscopic and histologic lesions. In contrast, 10–14 Gy irradiation resulted in Degree 1 or Degree 2 clinical manifestations, obvious function changes, and moderate endoscopic and histologic damages. Irradiation at 16–30 Gy resulted in Degree 2–4 clinical characteristics, significant intestinal function changes, and severe endoscopic and histologic damages. There has been no related research to which to compare our results.
In summary, the study presented for the first time a dog model for studying acute radiation enteritis caused by different single irradiation doses at a moderate dose rate by IMRT. The model exhibited clinical, functional, endoscopic, and histologic intestinal damage correlated with the abdominal irradiation dose. We also presented a method to evaluate radiation damage to the intestine. There are many potential contributory sources of heterogeneity in the assessment of acute radiation enteritis. For example, supportive care can affect disease progression and animal survival, and the luminal contents of the intestine can enhance acute radiation-induced small-bowel injury. 28 We will fully account for these influences in developing new and effective therapeutic methods for different degrees of intestinal damage after irradiation.
Footnotes
Author contributions
GX and LH conceived and designed the experiments. XW and CJ carried out experiments and analyzed data. LX contributed to the animal housing and caring. GX aided in the writing of the manuscript.
ACKNOWLEDGMENTS
This work was supported by the Military Key Program during the Twelfth Five-year Plan Period (BWS12J009). The authors are grateful to the numerous individuals who participated in this study.