
Abstract
Compared with conventional aortic cross-clamping, endovascular balloon occlusion (EBO) is a valuable strategy in unstable ruptured abdominal aorta aneurysm patients; however, it is unclear how long the balloon may remain safely inflated. Using a porcine model, we evaluated the influence of different EBO time periods on intra-abdominal pressure (IAP) and the association between various pathophysiologic indicators and reperfusion time. Twelve healthy three-month-old domestic piglets were subjected to ischemia/reperfusion injury using EBO within the abdominal aorta. Animals were grouped as A, B, and C based on 30, 60, or 120 min of ischemic time, respectively. Changes in IAP, hemodynamic data, respiratory and renal function, and histology after reperfusion were compared with baseline measurements. All pigs gradually developed intra-abdominal hypertension after ischemia/reperfusion injury. IAP increased significantly after 4 h of reperfusion in all three groups (all P < 0.001) with maximal IAP reaching > 22 mmHg in 10 pigs. However, no significant intergroup differences were found. Cardiac output remained stable, but mixed venous oxygen saturation decreased significantly at 4 h after reperfusion (P < 0.05). The pH decreased significantly at 10 min in all three groups (all P < 0.001). Histological changes in the small intestine, lung, and kidney occurred secondary to aortic ischemia; however, no significant differences were noted between groups (P > 0.05). EBO within the abdominal aorta induced ischemia/reperfusion injury which led to intra-abdominal hypertension, pathological changes within multiple organs, and decreased mixed venous oxygen saturation after only 30 min of abdominal aortic ischemia.
Keywords
Introduction
Major hemorrhage and shock secondary to vessel injury to the torso remain the leading causes of death in military and civilian trauma victims, and most battlefield casualties die of their injuries before ever reaching a surgeon.1–3 In 1954, Hughes 4 attempted to use a balloon catheter to achieve intra-aortic tamponade in two critically injured Korean casualties. However, this invasive procedure was not widely accepted until recent developments in endovascular therapy.
Endovascular balloon occlusion (EBO) of the abdominal aorta appears to be an effective option for the rescue of non-compressible torso hemorrhage, especially in cases of hemorrhage arising from trauma to torso vessels, ruptured abdominal aortic aneurysm (rAAA), and in cases of trauma to solid abdominal organs and disruption of the bony pelvis resulting in hypotension and shock.5–7 Supra-celiac aortic occlusion with a balloon catheter is often performed in clinical practice to control hemorrhagic shock associated with abdominal aortic injury or rAAA. 8 Compared with conventional aortic cross-clamping in hemodynamically unstable patients, EBO is associated with reduced intraoperative mortality in unstable rAAA patients. However, it fails to improve outcomes in other settings.5–7
Hemorrhagic shock is not the only life-threatening condition that occurs in trauma victims. Conditions in which there is a subsequent systemic inflammatory response can cause multiple organ dysfunction even prior to surgical treatment. 9 Altered metabolism accompanied by moderate inflammatory and oxidative stress responses can lead to significant postoperative complications. 10 Significant mortality is also associated with rAAA and the related “damage-control” efforts at surgery, with almost 40% of patients succumbing to hemorrhagic shock and 30% dying as a result of ischemia-induced multiorgan failure. 11 The high mortality associated with multiorgan failure secondary to ischemia underscores the need to detect and treat intra-abdominal ischemia/reperfusion injuries and elevated intra-abdominal pressure (IAP) before the development of organ damage.
In 1953, De Bakey and Cooley12,13 reported their surgical treatment of abdominal aortic aneurysm by clamping the proximal abdominal aorta with an average ischemic time of approximately 1 h (range 48–102 min). Malina et al. 14 used a suprarenal aortic occlusion catheter to rescue cases of rAAAs and two of these cases tolerated 30 min of ischemic time without renal complications. However, it is not known for how long the supraceliac or suprarenal balloon may remain safely inflated without renal or intestinal ischemic complications. Avaro et al. 15 used a porcine model to exam the possible complications of the supraceliac EBO for 40 and 60 min, but pathologic examination disclosed that the ischemic visceral injuries (bowel and kidneys) were not significantly different between the two groups.
The purpose of this pilot study was to develop a porcine model to study the effect of ischemic duration, using endovascular balloon treatment on IAP. Our underlying hypothesis was that a longer abdominal aortic ischemic time would induce a more serious impact on IAP and cause severe physiologic and pathologic findings that were directly related to the duration of intra-abdominal ischemia. In particular, in order to develop a model that simulated conditions encountered by vascular surgeons, the influence of different EBO time periods on IAP and the association between various pathophysiologic indicators and reperfusion time were evaluated.
Materials and methods
Our study protocol was reviewed and approved by the Institutional Animal Care and Use Committee of Kaohsiung Armed Forces General Hospital, Taiwan.
Animal preparation
Twelve healthy three-month-old domestic piglets of both sexes were used for this study. All animals were accommodated in an accredited facility. Each animal was individually housed and cared for and free access to food and water was provided.
Animals were fasted for 12 h prior to the experiment. After premedication with intramuscular 4 mg/kg Stresnil (azaperone 40 mg/mL) and 0.04 mg/kg atropine (1.0 mg/mL), anesthesia was induced by 2 mg/kg of Zoletil-50 (Tiletamine HCl plus Zolazepam HCl; Virbac, Fort Worth, TX, USA) via an ear vein. A heating lamp was used to avoid hypothermia. Endotracheal intubation was performed by laryngoscope and general anesthesia was administered using 2 L/min of oxygen mixed with N2O (1:1) in conjunction with isoflurane. Although N2O is known to cause intestinal distension, in our experience, incomplete fasting rather than the use of N2O is a more likely cause of intestinal distension.
Anesthesia was maintained with continuous intravenous infusion of propofol at a rate of 2 mg/kg/h throughout the experiment. Pulmonary arterial catheterization (OptiQ® Pulmonary Artery SVO2/CCO Catheter, ICU Medical, Inc. San Clemente, CA, USA), arterial pressure catheterization, inferior vena cava catheterization, electrocardiogram, urinary catheterization, and IAP monitor (Intra-abdominal Pressure Monitoring System, Abviser Medical, USA) were set up prior to the interventional procedure.
A surgical towel, 20 cm in width, was wrapped around the circumference of each pig’s abdomen, and the length of the towel was fixed with towel clamps in order to limit distension of the abdominal wall during the observational period. Since the abdominal pressure could be affected by a volume change, the wrapping of towels helped to maintain the abdominal circumference and avoid any possible interference when taking IAP measurements. IAP measurements were performed under anesthesia after the placement of catheters. All the three experimental groups were clamped and wrapped with towels and we believe this procedure did not affect the measurements of IAP and was uniform across the groups.
Reperfusion injury of intra-abdominal organs was induced by an aortic occlusion catheter with a balloon diameter of 11 mm, a diameter of 5 F, and a length of 27 cm (Pruitt Occlusion Catheter, LeMaitre Vascular, Inc. Burlington, MA, USA) which was placed into the abdominal aorta through the left common femoral artery. The occlusion balloon was located in abdominal aorta between the level of the diaphragm and the orifice of the celiac trunk. The location of the balloon in each animal was confirmed after sacrifice to ensure it was uniform in all animals.
Measurements
Baseline data and postischemia/reperfusion data were collected, including hemodynamic data (cardiac output [CO], central venous pressure [CVP], PP [the difference between mean arterial pressure and IAP], mixed venous oxygen saturation [SVO2], lactate [Lac]), peak airway pressure, IAP, arterial blood gas analysis, respiratory functional data (peak inspiratory pressure [PIP], arterial oxygen tension [PaO2], and arterial bicarbonate tension [PaCO2]) and renal functional data (blood urea nitrogen [BUN], creatinine [Cr], and neutrophil gelatinase-associated lipocalin [N-GAL]).
Different time periods of ischemia/reperfusion were applied, including 30 min (group A, n = 4), 60 min (group B, n = 4), and 120 min (group C, n = 4), as previously described. 16 Postischemia/reperfusion data were compared with the baseline data. During the observational period, all pigs were resuscitated with normal saline solution if the mean arterial pressure (MAP) was less than 65 mmHg as an MAP of at least 65 mmHg is essential to maintain normal organ circulation. This MAP value was also chosen to ensure that all changes in arterial pressure were due to ischemia/reperfusion and not due to deflections induced by surgical shock.
All animals were maintained under anesthesia for 20 h of observation (or until their demise) and their kidneys, lungs, and small intestines were harvested, after euthanasia, for histologic analysis. Qualitative and semi-quantitative histologic analysis of the small intestine was performed using hematoxylin and eosin (H&E) staining, as previously described.17,18 The whole tissue sections were independently analyzed under high magnification (100X and 400X) by two pathologists who were blinded to the animal groupings.
For each field, the following parameters were analyzed: necrosis of the villi, hemorrhagic infarction, congestion, and the presence of inflammatory cells. A semi-quantitative scoring of five points was used based on the severity of damage and graded as 0 = negative (normal intestine), 1 = 1–25%, 2 = 26–50%, 3 = 51–75%, and 4 = 76–100% of the observed microscopic field of above changes. Fifteen non-coincident microscopic fields were quantified for each animal, with a total of four animals per group.
Statistical analysis
Continuous data were expressed as mean ± standard deviation or median and range depending on the normality of the data. Categorical data were expressed as numbers and percentages. Comparisons in the baseline characteristics and semi-quantitative analysis of histological changes among the three groups were performed by analysis of variance or Kruskal–Wallis test for continuous data, and by Fisher’s exact test for categorical data, as appropriate. Due to the repeated measurements of physiological parameters across time, a linear mixed model was applied to investigate the effects on the experimental groups (denoted as group), time after reperfusion (denoted as time), and their interactions (denoted as group × time) on physiological parameters adjusted for body weight. Results of physiological parameters across time were expressed as least-square mean and standard error for each group. If main effects or interactions showed significance, further post hoc multiple comparisons were conducted by Bonferroni correction to adjust the overall type I error rates. All statistical analyses were performed with SAS software version 9.2 (SAS Institute Inc., Cary, NC, USA). A two-tailed P-value < 0.05 was considered statistically significant.
Results
Baseline characteristics and survival time
Baseline characteristics among animals by group according to ischemia/reperfusion time of aortic occlusion (group A: 30 min; group B: 60 min; group C: 120 min)
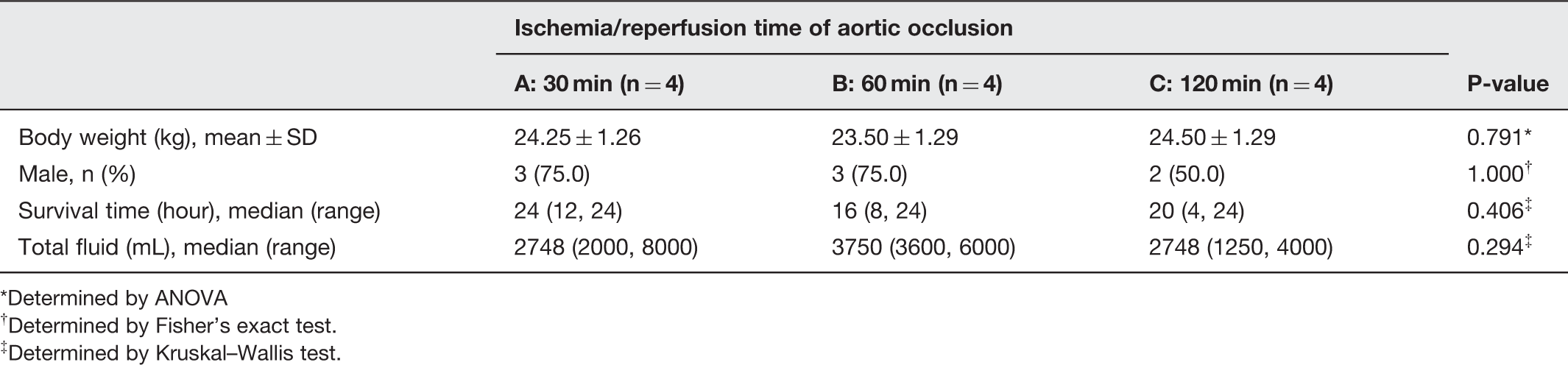
Determined by ANOVA
Determined by Fisher’s exact test.
Determined by Kruskal–Wallis test.
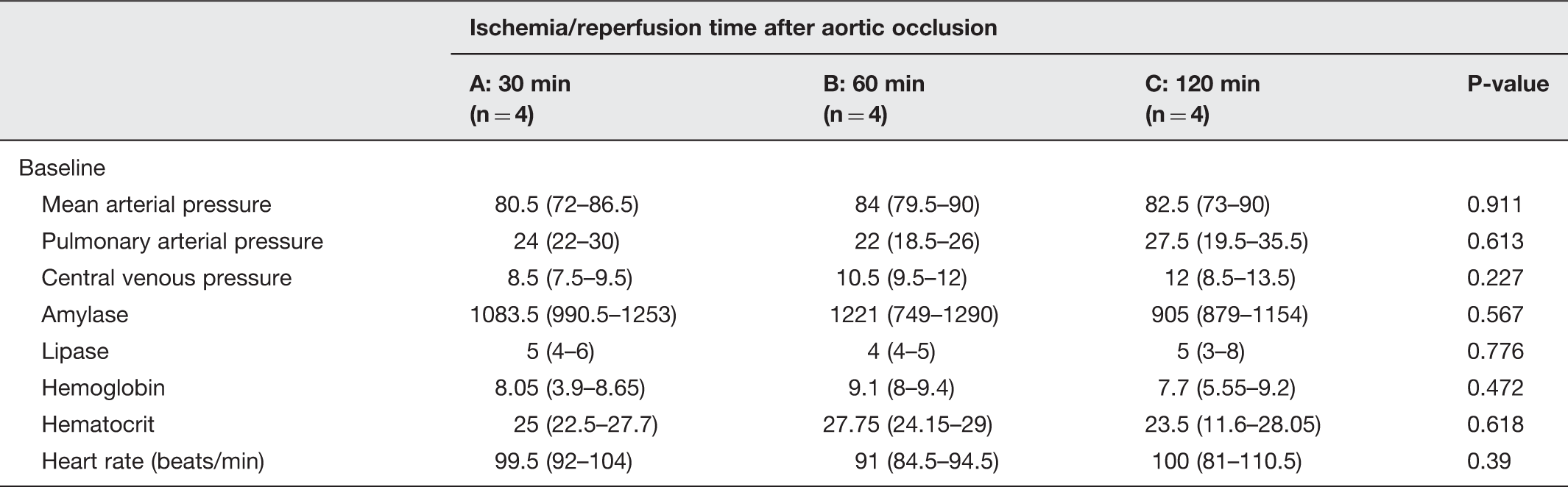
Baseline laboratory measurements among the three groups of animals categorized by increasing ischemia/reperfusion time (group A: 30 min; group B: 60 min; group C: 120 min)
All animals were maintained under anesthesia for 20 h of observation or until their demise, whichever was earlier. Two pigs expired during the first 12 h of reperfusion (one in group B expired at 8 h after reperfusion and one animal in group C expired at 4 h after reperfusion). The surviving animals were humanely euthanized by intravenous KCl (1–2 meq/kg) after 20 h. Signs of fever (body temperature > 38.0℃) and leukocytosis (WBC > 10,000/cumm) were found in all animals.
IAP after reperfusion
All pigs gradually developed intra-abdominal hypertension after ischemia/reperfusion injury. The maximum IAP after reperfusion was greater than 12 mmHg in all pigs (range 14–30 mmHg). IAP increased gradually after reperfusion in all three groups (Figure 1, all P < 0.001). Compared with baseline levels, significantly higher IAP was found at 3 h after reperfusion for group A and at 4 h after reperfusion for groups B and C. In addition, the IAP increased maximally after 60 min of clamp time rather than the expected 120 min of clamp time, when compared with baseline. However, no significant inter-group differences were found in IAP (Figure 1).
Intra-abdominal pressure (IAP) data in animals by group based on reperfusion time after aortic occlusion (group A: 30 min; group B: 60 min; group C: 120 min). Data are expressed as least-square mean (LSM) with standard error (SE) adjusted for body weight. IAP were recorded at baseline (preocclusion period) and at 10 min, 1, 2, 3, 4, 8, 12, 16, and 20 h after reperfusion.* represented significantly different compared with baseline in group A. † represented significantly different compared with baseline in group B. ‡ represented significantly different compared with baseline in group C. (A color version of this figure is available in the online journal.)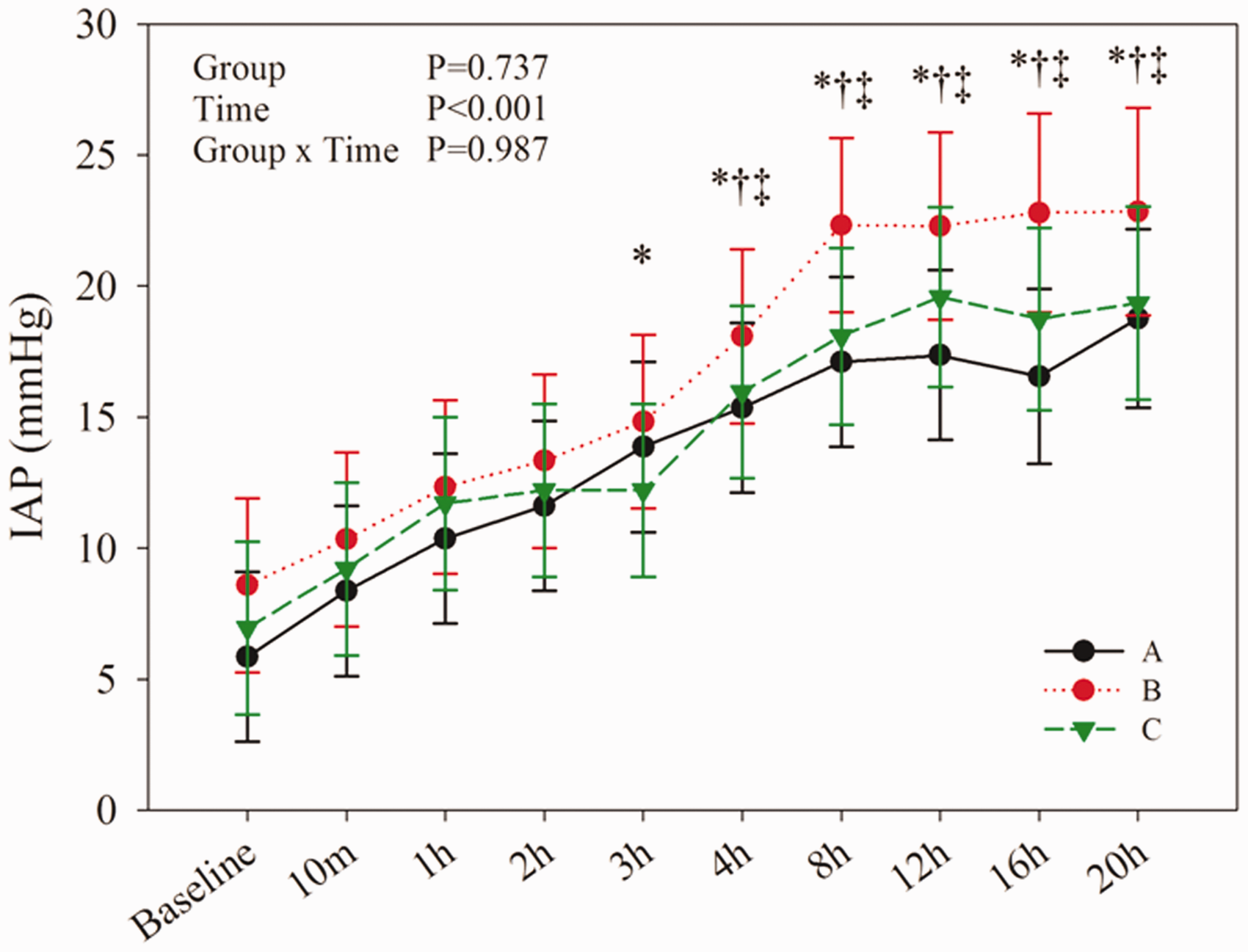
Hemodynamic data after reperfusion
The hemodynamic data, including CO, PP, SVO2, and Lac are presented in Figure 2. No significant time trends were found in CO or PP as a function of reperfusion time. However, compared with baseline results, SVO2 decreased significantly at 20 h after reperfusion for all three groups and at 4 h for group C (Figure 2(c), all P < 0.05). In addition, a significant increase in Lac was observed 10 min after reperfusion for groups B and C, and 1, 2, 3 h for group C (Figure 2(d), all P < 0.05).
Hemodynamic changes in animals by group based on reperfusion time after aortic occlusion (group A: 30 min; group B: 60 min; group C: 120 min). (a) cardiac output (CO), (b) central venous pressure (CVP), (c) intra-abdominal perfusion pressure (PP), (d) mixed venous oxygen saturation (SVO2), (e) lactate (Lac). Data are presented as least-square means (LSM) with standard errors (SE) adjusted for body weight. Hemodynamic data were recorded at baseline (preocclusion period), and at 10 min, 1, 2, 3, 4, 8, 12, 16, and 20 h after reperfusion. * represents a significant difference compared with baseline in group A. † represents a significant difference compared with baseline in group B. ‡ represents a significant difference compared with baseline in group C. (A color version of this figure is available in the online journal.)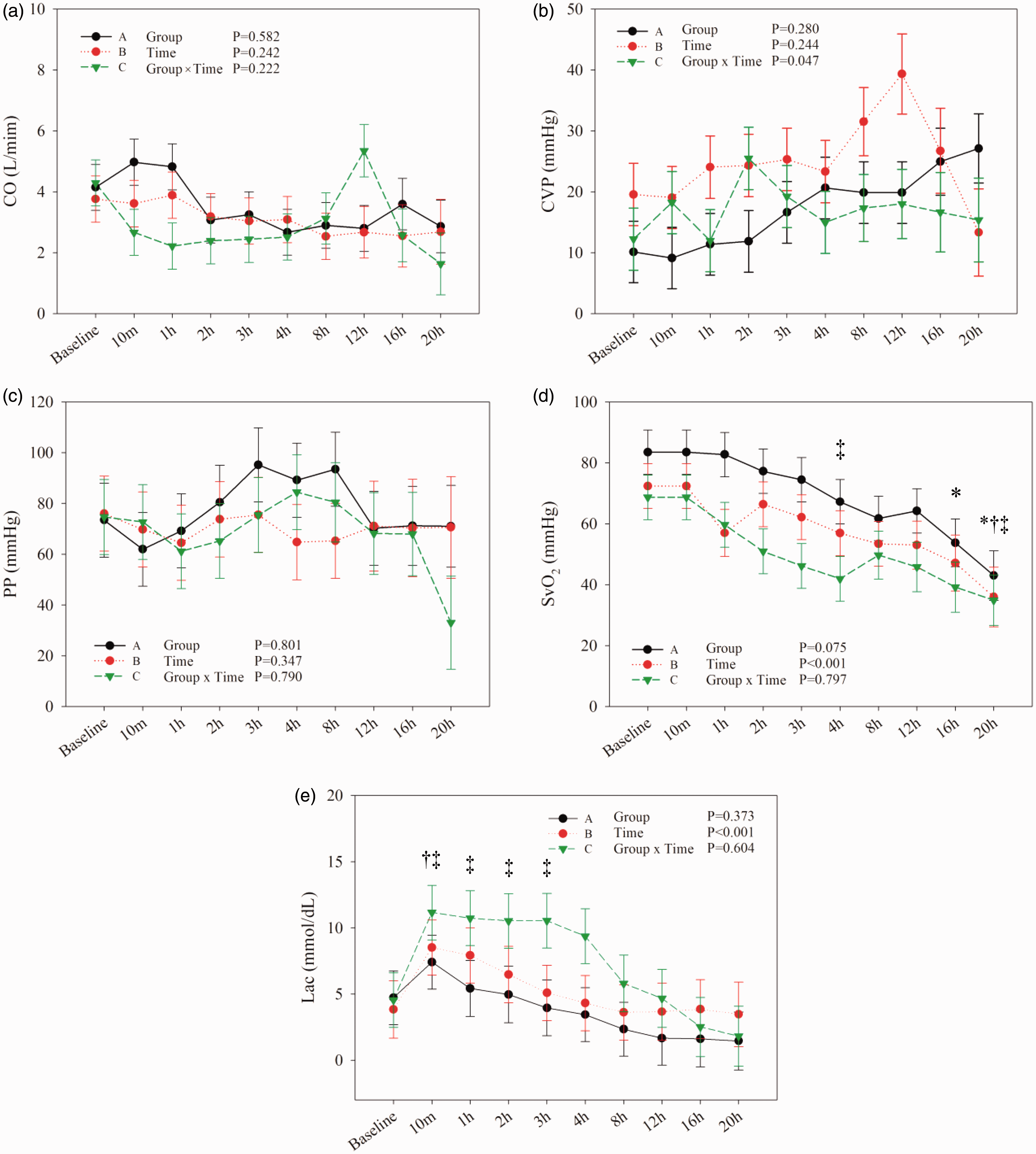
Respiratory function after reperfusion
Respiratory function, as measured by PIP, PaO2, and PaCO2, is presented in Figure 3. No significant inter-group differences were found in the respiratory parameters. However, compared with baseline results, PIP was elevated significantly at 2, 3, 4, 8, and 12 h after reperfusion for group C (P ≤ 0.035) and was elevated significantly at 3 h for group A (P = 0.048). No significant trends were found in either PaO2 or PaCO2 at any given time point after reperfusion, as compared with baseline (Figure 3).
Respiratory functional data by animal group based on amount of reperfusion time after aortic occlusion (group A: 30 min; group B: 60 min; group C: 120 min). (a) Peak inspiratory pressure (PIP), (b) arterial oxygen tension (PaO2), and (c) arterial bicarbonate tension (PaCO2). Data are expressed as least-square means (LSM) with standard errors (SE) adjusted for body weight. Respiratory functional data were recorded at baseline (preocclusion period), and at 10 min, 1, 2, 3, 4, 8, 12, 16, and 20 h after reperfusion. * represented significantly different compared with baseline in group A. † represented significantly different compared with baseline in group B. ‡ represented significantly different compared with baseline in group C. (A color version of this figure is available in the online journal.)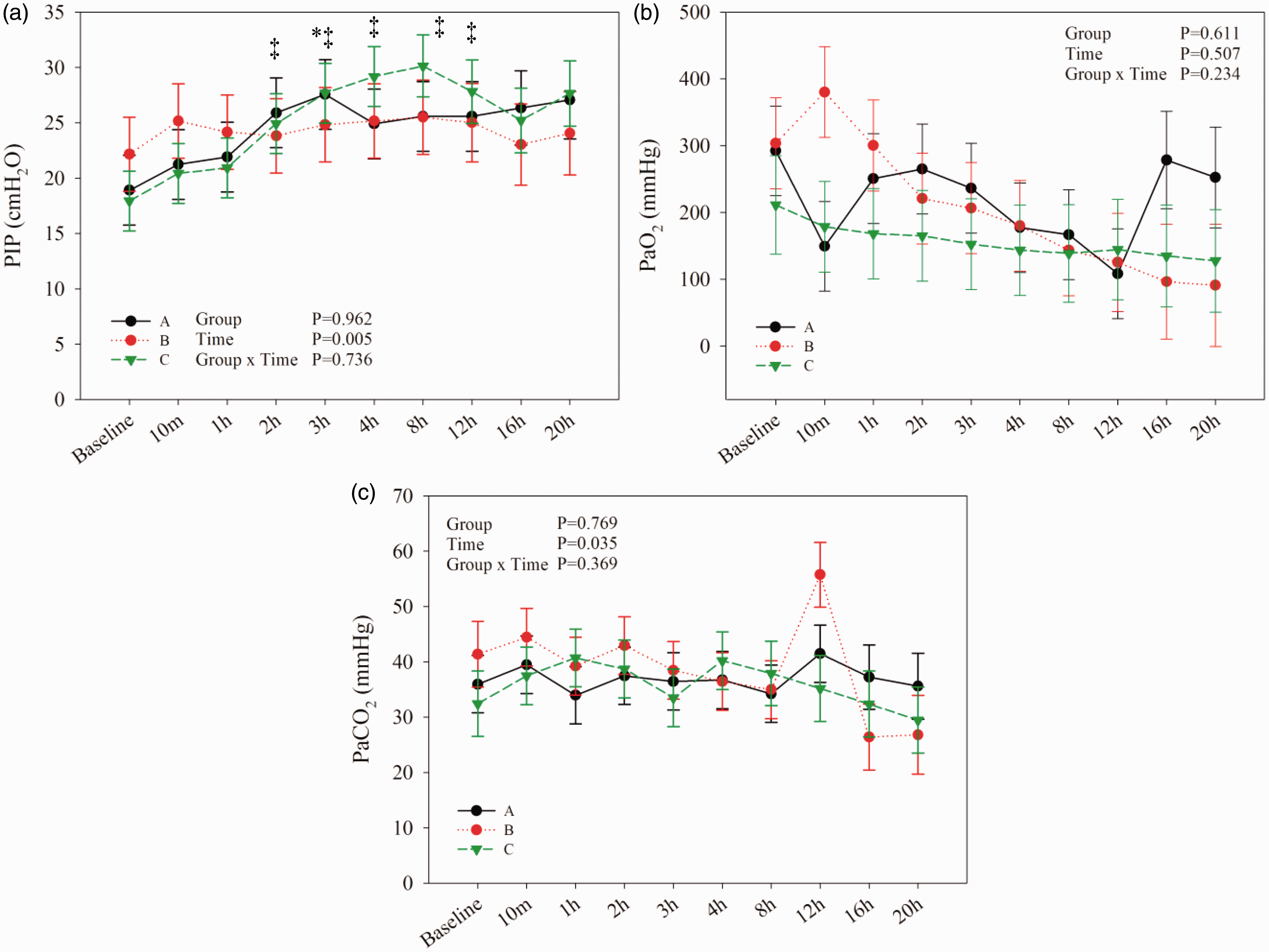
Renal function after reperfusion
Renal function in all three groups, compared with baseline, is presented in Figure 4. BUN increased significantly compared with baseline results beginning at 8 h after reperfusion for group C (P < 0.001) and at 12 h after reperfusion for group B (P < 0.05). In addition, significant increases in Cr as compared with baseline levels were seen at 1 h after reperfusion in group C (P < 0.05).
Renal functional data by animal group based on reperfusion times (group A: 30 min; group B: 60 min; group C: 120 min). (a) Blood urea nitrogen (BUN), (b) creatinine (Cr), and (c) N-GAL. * represented significantly different compared with baseline in group A. † represented significantly different compared with baseline in group B. ‡ represented significantly different compared with baseline in group C. (A color version of this figure is available in the online journal.)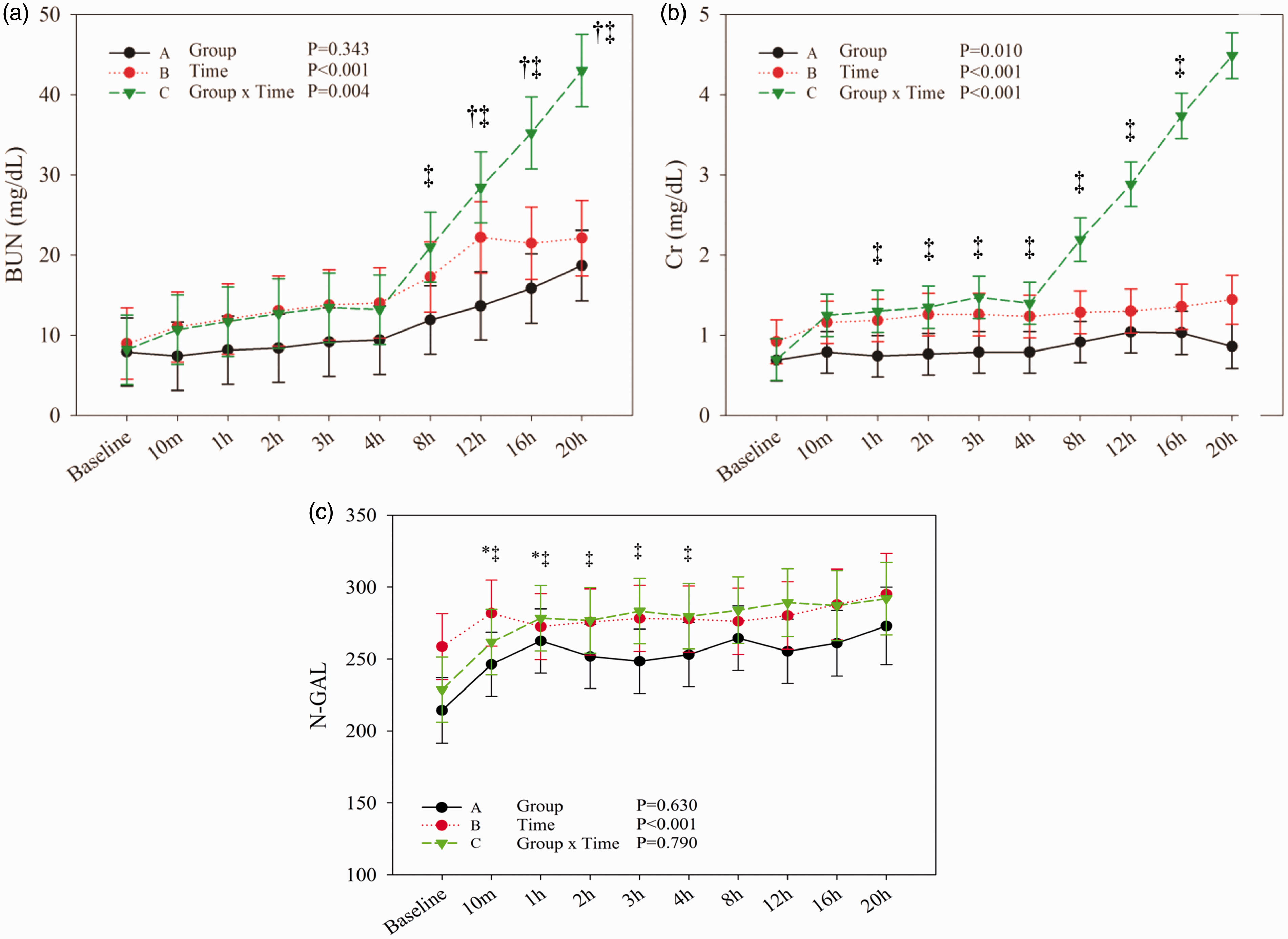
Postreperfusion levels of Cr were significantly different between groups A and C (P = 0.010). In addition, significant differences were found in N-GAL between different time points (P < 0.001). Compared with baseline levels, N-GAL was significantly increased at 10 min and 1 h in group A (P < 0.001) and was significantly increased at 10 min, 1, 2, 3, and 4 h in group C (all P ≤ 0.001).
Biochemical findings
Figure 5 shows the effect of reperfusion time on pH among the three groups. Compared with baseline levels, pH decreased significantly at 10 min in all three groups and significantly decreased at 1 h in group C (all P < 0.001).
The effect of reperfusion time on pH among the three animal groups (group A: 30 min; group B: 60 min; group C: 120 min). * represented significantly different compared with baseline in group A. † represented significantly different compared with baseline in group B. ‡ represented significantly different compared with baseline in group C. (A color version of this figure is available in the online journal.)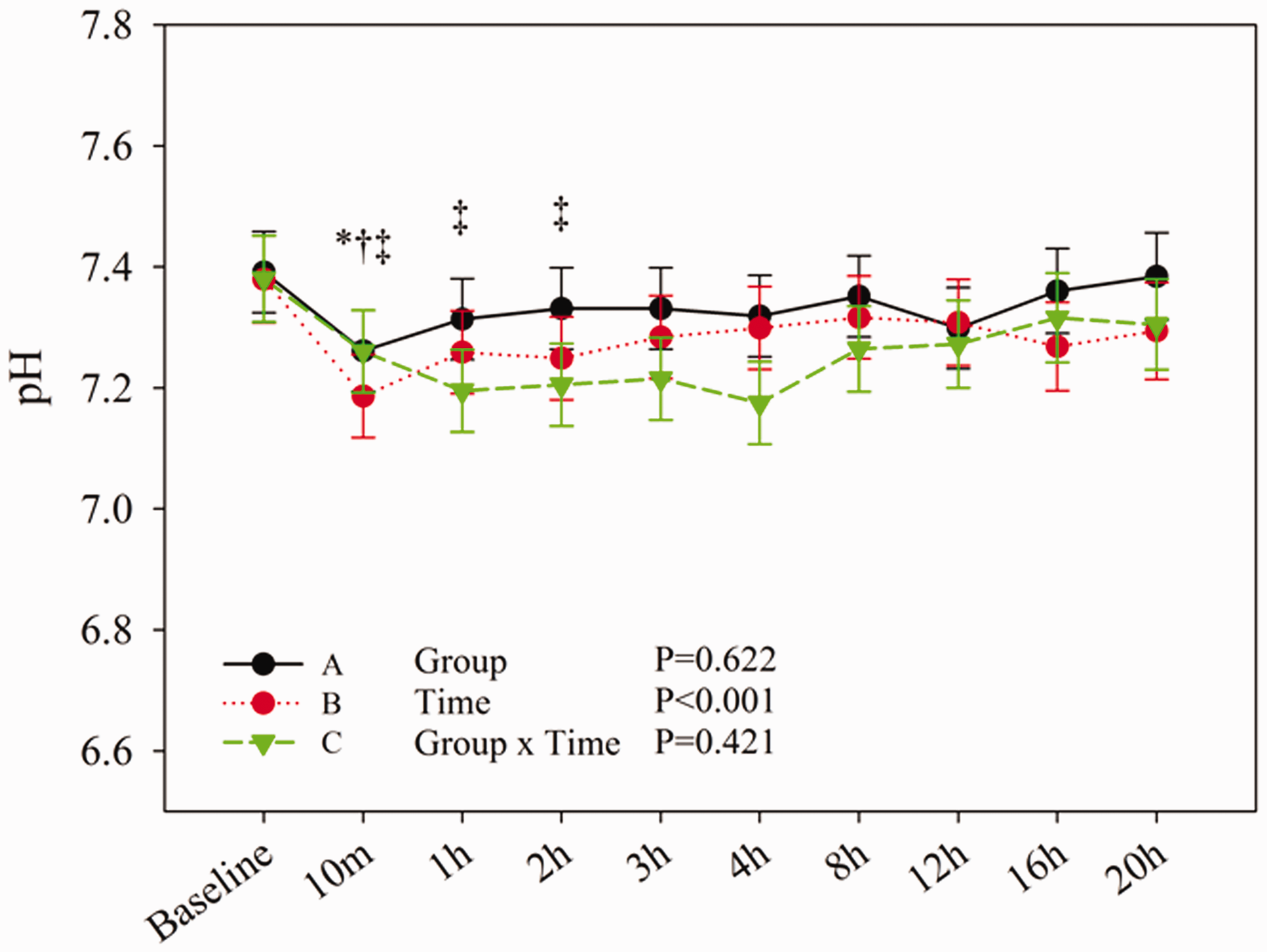
Histopathologic findings
Necropsy performed immediately after the sacrifice/demise of each pig showed massive ascites and dilation of bowel loops in all animals. The parenchymal tissue of kidneys showed edematous changes within the renal tubular epithelium. Alveolar tissue within the lungs showed congestion and atelectasis. Pathology was most prominent within the mucosa of the small intestine, with loss of the surface epithelium, flattening and sloughing of villi, and a high incidence of congestion within the small capillaries of the upper compartment of the mucosa, which was suggestive of hypoxia secondary to poor blood flow through the end-capillary bed (Figure 6). However, no significant differences were noted between groups (P > 0.05; Kruskal–Wallis test).
Histologic findings among the three animal groups based on reperfusion times (group A: 30 min; group B: 60 min; group C: 120 min). (a) Histology of the small intestinal mucosa demonstrates flattening and sloughing of villi (white arrows). (b) The small intestinal serosa shows increased cellularity and edema (white arrows). (c) The kidney shows edematous change within the renal tubular epithelium (white arrow). (d) The lung demonstrates atelectasis, diffuse hyperemia, alveolar edema, and alveolar septal enlargement (white arrows)
Discussion
We found that EBO within the abdominal aorta induced ischemia/reperfusion injury which led to intra-abdominal hypertension, pathological changes within multiple organs, and decreased mixed venous oxygen saturation after only 30 min of abdominal aortic ischemia. Although, both cause ischemia/reperfusion, our current model of intraluminal occlusion has several advantages over the external cross clamp in both surgical procedure and integrity of the abdominal cavity after the treatment. Intraluminal occlusion is minimally invasive, with less injury to the subjects. In addition, it preserves the integrity of the abdominal cavity, thus minimizing any potential confounders of the IAP.
IAH is defined as any IAP > 12 mmHg. All 12 pigs developed IAH after ischemia/reperfusion injury with maximal IAP reaching >22 mmHg in 10 pigs. Evaluation of the possible influence of different time periods of intra-abdominal ischemia/reperfusion on IAP showed that occlusion of the upper abdominal aorta for 30, 60, and 120 min was able to produce intra-abdominal hypertension greater than 20 mmHg within 20 h with varying degrees of organ failure. We only observed animals for 20 h post reperfusion, as our major aim was to observe the changes of IAP during the acute ischemia period.
Interestingly, when compared with baseline, the IAP increased maximally after 60 min of clamp time rather than 120 min of clamp time. From the histopathologic results, we found that the small intestine of subjects in the group C (120 min clamping time) showed more micro-thrombosis in the capillary bed, which might lead to less capillary leak and tissue swelling, resulting in less IAP. However, no significant differences were found in the hemodynamic parameters among the three groups with different ischemia/reperfusion times in the present study.
EBO can stabilize arterial pressure during severe hemorrhagic shock, but a longer duration of ischemia appears to induce worsening dysfunction in vital organs. Therefore, our shortest EBO time period (30 min) appears to represent the best period to use in model construction. Given the results of this study, we believe that our pathologic porcine model may be useful for evaluating EBO pathophysiology and the efficacy of medical and surgical therapeutic approaches.
IAH has important pathophysiologic implications for human organs and systems. If IAH is accompanied by an abdominal perfusion pressure <60 mmHg, it can become associated with multiorgan failure, as demonstrated in studies of gut ischemia/reperfusion leading to abdominal compartment syndrome in porcine models.19,20 A pathologic animal model of septic and ischemia/reperfusion-induced shock and multiple organ injury replicated systemic inflammation and major organ system dysfunction seen in trauma patients and those with sepsis. 21 Similar to our findings, progressive functional deterioration within organs (including histopathologic injury to the lungs, kidney, liver, and intestines of the animals) occurred due to changes in hemodynamic status associated with shock. The pathologic porcine model constructed in the present study was developed according to the hypothesis of ischemia/reperfusion injury as it occurs in human patients. In our animal model, IAP increased quickly to IAH, as expressed by the presence of fever, leukocytosis, deterioration of mixed venous oxygen saturation, and histological findings, which were identical to systemic inflammatory response syndrome. Olofsson et al. 22 applied stepwise increases in IAP to construct a porcine model for assessing gastric, intestinal, and renal cortex microcirculation that paralleled central hemodynamics and respiratory function. In that study of experimentally increased IAP, the peritoneum was inflated with CO2 and IAP was increased in a stepwise manner by 10 mmHg at 10 min intervals up to 50 mmHg and subsequently exsufflated. The study demonstrated that intra-abdominal hypertension had a negative effect on renal and gastrointestinal perfusion and that an IAP over 10–15 mmHg compromises CO. 22 In the present study, our animals compensated their PP during our observation, but the histological findings of edematous intestines and kidneys provided evidence of poor microcirculation, similar to the findings in the previously cited study, 22 where laser Doppler flowmetry revealed reduced microcirculation within the gastric mucosa, renal cortex, and intestinal seromuscular layers, creating subsequent organ damage.
One of the problems with animal models that develop IAH by insufflation of the abdomen with air or liquid is the inability to maintain the IAP over time, which minimizes the deleterious effects on the abdominal organs. In order to simulate human IAH in an animal model, the levels of IAP must remain constant. 18 We circumvented this issue by wrapping towels around the abdomen of each pig to maintain the abdominal circumference at a fixed value, thus, avoiding any possible interference with the IAP measurements. The clamping and towel wrapping were uniform across all animals and experimental groups.
With the exception of the models proposed by Suk et al. 10 and Gong et al., 17 the advantage of our study over other animal models13–15,21,22 was the longer duration of ischemia (2 h), although the different durations of ischemia did not achieve significant differences in the IAP. This may possibly be explained by efficient intra-abdominal collateral blood circulation, as described in previous studies.23–25 In our study, we used occlusion catheters to create the ischemia/reperfusion injury, resulting in intra-abdominal hypertension in all experimental animals. We believe that this model would allow investigators to monitor the increased abdominal pressure and associated factors characteristic of EBO within the research setting.
Our study had several limitations. Although pig is an ideal model for the study of reperfusion injury, the animals used in our study were three-month-old pigs and not mature pigs. They were chosen due to space limitations and because their weight (approximately 20 kg) met animal experimentation guidelines. However, their immaturity may limit the extension of our results to humans as it is known that physiological indicators are more diverse in immature animals compared with mature ones. For example, the level of small intestinal mucosal xanthine oxidase in pig is generally low during the adulthood, which may reduce susceptibility to reperfusion injury. 26 In addition, certain morphological differences exist, including the Paneth cells in the epithelium of the small intestine, which are thought to play an integral role in modulating stem cell self-renewal or differentiation. The evidence to prove the existence of Paneth cells in pigs remains controversial, which makes the study of regenerative events following reperfusion injury more complicated in pig model. 26 Also, domestic piglets may not have been the best choice of experimental animal since the majority of domestic piglets have pre-existing pulmonary infections,20,21 which may have affected our results. In addition, the CO remained stable in our model, but the CVP increased gradually and significantly. Although we did not employ speckle tracking imaging to directly measure cardiac contractility, we surmised that changes in hemodynamic parameters may have stemmed from decreases in cardiac contractility during the development of IAH. Finally, the observational period was limited to 20 h due to funding limitations. In the present model, since the observation period was restricted to 20 h, not all piglets reached the IAP of 25 mmHg that is necessary for ischemia-induced multiple organ failure. Nonetheless, we achieved our primary aim to develop a model for observing changes due to ischemia/reperfusion injury secondary to varying durations of intra-abdominal EBO as seen in clinical practice. Future randomized controlled studies with longer observational periods are needed to delineate the underlying mechanisms involved in the development of IAH.
In conclusion, our pathologic porcine model was simple in construction, easily reproduced, and matched clinical conditions regarding EBO applications to humans. The use of an aortic occlusion balloon to produce a reperfusion injury replicated the pathological effects seen in patients without destroying the abdominal wall architecture. Occlusion of the upper abdominal aorta for 30 min was able to produce an animal model of intra-abdominal hypertension >20 mmHg within 20 h. Our results suggest that the current model may be used to evaluate the efficacy of novel pharmaceutical therapies and surgical interventions used in cases of abdominal aortic injury.
Authors’ contribution
C-SC: guarantor of integrity of the entire study, study concepts, study design, definition of intellectual content, literature research, clinical studies, experimental studies, data acquisition, data analysis, statistical analysis, manuscript preparation, manuscript editing, manuscript review.
C-ST: guarantor of integrity of the entire study, definition of intellectual content, data analysis, statistical analysis, manuscript review. Y-HW: experimental studies, data acquisition. Y-HL: literature research, clinical studies, experimental studies, data acquisition. J-MC: literature research, clinical studies, experimental studies, data acquisition. Y-PC: guarantor of integrity of the entire study, literature research, clinical studies. H-KC: literature research, clinical studies. S-TC: experimental studies, data acquisition. T-ML: guarantor of integrity of the entire study, experimental studies, data acquisition. S-CY: guarantor of integrity of the entire study, data analysis, statistical analysis, manuscript review.
Footnotes
Acknowledgements
We are grateful to the two registered nurses, Hseu-Fang Shao and Pei-Lun Ma, who volunteered to collect the blood samples and record the data. There was no grant support for this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.