
Abstract
Prostate cancer is a common disease and, while detection and treatment have advanced, it remains a significant cause of morbidity and mortality in men. Research suggests significant involvement of the immune system in the pathogenesis and progression of prostate cancer, indicating that immunologic therapies may benefit patients. Two immunologic factors, interleukin-2 and transforming growth factor-β, may be especially attractive therapeutic targets for prostate cancer. Specifically, an increase in interleukin-2 signaling and a decrease in transforming growth factor-β signaling might help improve immunologic recognition and targeting of tumor cells. The purpose of this review is to highlight the evidence that interleukin-2 and blockade of transforming growth factor-β could be used to target prostate cancer based on current understanding of immune function in the context of prostate cancer. Additionally, current treatments related to these two factors for prostate and other cancers will be used to strengthen the argument for this strategy.
Keywords
Introduction
Prostate cancer (PCa) remains common in spite of advancements in screening and treatment, with almost 190,000 new cases and 26,000 PCa-related deaths anticipated in 2016. 1 Roughly one in seven men will develop PCa in their lifetimes and, while deaths caused by PCa have declined, it remains a significant cause of morbidity and mortality. 1 PCa is often diagnosed following elevation of a serum biomarker, prostate-specific antigen (PSA), which is checked routinely in some populations of men. 2 Treatment strategies for localized PCa currently include surgery and radiation or hormonal therapies for metastatic disease. 2 However, these therapies are not without adverse effects, and continued research has the potential to improve treatment and quality of life outcomes. Treatment efficacy is followed in multiple ways, including by imaging and serial PSA levels. 2 Biochemical response can be considered significant when either the PSA level falls or the rate of PSA increase, or PSA doubling time, slows. 2 A rise in PSA after a period of remission is considered a biochemical recurrence. 2 Several immunologic targets have been identified that could serve as potential therapeutic targets, but more study is needed to refine these approaches, which have been extensively reviewed.3,4 Two such targets, transforming growth factor-β (TGF-β) and interleukin-2 (IL-2), have demonstrated potential to synergistically improve outcomes in PCa, which is the subject of this review.
Evidence for immune involvement in PCa
There is significant evidence for the involvement of the immune system in the pathogenesis of PCa. PCa-associated macrophages have been reported and are associated with disease activity, metastasis, and progression.5–9 Phagocytosis of apoptotic PCa cells polarizes these tumor-associated macrophages toward an M2 anti-inflammatory phenotype, which express high levels of TGF-β1 RNA. 5 Impairment of TGF-β1 expression in macrophages might prevent the development of this M2 phenotype. 10 Additionally, macrophage density and propensity to have more M2 macrophages both appear to be associated with negative outcomes, including biochemical recurrence and invasive tumor phenotype.6,7 Furthermore, these macrophages appear to synergize with tumor-associated fibroblasts, which are prostate stromal cells that are also capable of producing and responding to TGF-β and possibly IL-2. 7
In addition to macrophages, other immune cells have also been implicated in PCa and may be involved in the response to, or production of, IL-2 and TGF-β in the tumor microenvironment. Several T-lymphocyte subsets, many of which produce and are responsive to IL-2 and TGF-β, have also been studied in association with PCa. One study demonstrated higher levels of CD4+ T-helper cells (THCs), especially TH2-cells, T-regulatory (T-reg) cells, and TH17 cells in PCa tissue compared with peripheral blood. 11 Both natural killer (NK) and TH17 cells but not the others were more common in tumors with a lower grade, the histologic tumor severity as determined by a pathologist.11,12 This inverse correlation with grade could be because NK and TH17 cells are beneficial in PCa or due to cytokine influence within the tumor. 11 The TH1 of THCs, on the other hand, is associated with a decreased risk of developing PCa. 13 TGF-β also favors the development of T-reg cells, which may argue for the cytokine milieu influencing immune cell development at the tumor site. 14
Other T-cell subsets appear to play a role in the antitumor response. THCs and some CD8+ cytotoxic T-lymphocytes (CTLs) are recruited to PCa tumors following androgen ablation. 15 These T-cells target a specific antigen indicating that they may be part of the body’s adaptive immune response to the tumor. 15 Furthermore, it has been shown that PCa tumor cells treated in vitro with histone deacetylase inhibitors are more susceptible to CTL killing, indicating that PCa cells may be employing mechanisms of immune escape that could be overcome with treatment. 16 CTLs also tolerate tumor antigens, which can be overcome by a blockade of lymphocyte-activating gene 3, a factor that decreases the number and activity of CTLs. 17 T-regs accumulate in both the tumor and peripheral blood of patients with PCa, indicating a possible role in PCa pathogenesis and identifying them as a possible therapeutic target. 18 Additionally, T-regs have been shown to inhibit other immune cells, notably THCs, by depriving them of IL-2, which may contribute to PCa immune escape.18,19 Furthermore, IL-2 promotes a pro-inflammatory M1 macrophage phenotype over an M2 anti-inflammatory macrophage phenotype. 20 Thus, in the lymphocyte subsets and macrophages identified in the pathogenesis of PCa, IL-2 is a strong candidate for improving immune recognition and targeting of the tumor.
Targeting the immune system to treat PCa has been the subject of significant research interest. One immunologic anti-PCa treatment is clinically available in the United States, adding evidence that employing the immune system in the treatment of PCa is a viable strategy. Sipuleucel-T® is a therapeutic strategy in which peripheral blood mononuclear cells, specifically the dendritic cell subset, are isolated, stimulated with an antigen consisting of conjugated prostatic acid phosphatase and granulocyte-macrophage colony-stimulating factor (GM-CSF), and reinfused into the patient. 21 This therapy has demonstrated a survival benefit with tolerable side-effects, although time to clinical progression remained similar compared to androgen deprivation therapy.21,22 Sipuleucel-T® has also been shown to increase T-cell infiltration into prostate tumors, including both THCs and CTLs. 23 Thus, the effectiveness of sipuleucel-T® coupled with its changes in immune response to PCa demonstrates that immunologic modulation can be exploited to treat PCa.
Transforming growth factor-β in PCa
TGF-β is a cytokine with three isoforms secreted as a latent peptide by a variety of cell types and activated by protease cleavage following secretion.24,25 Its receptor (TGF-βR) also has three isoforms, which are serine-threonine kinases that activate several pathways intracellularly, notably the SMAD pathway.24,25 TGF-β signaling is complicated in that it can affect the same cells differently depending on context. For example, TGF-β treatment stimulated colony growth of 3T3 fibroblast cells when platelet-derived growth factor was applied, but prevented colony formation in conjunction with epidermal growth factor treatment. 26 TGF-β has been shown to be pro-apoptotic in a B-cell lymphoma-2-dependent manner and lead to cell cycle arrest, but has also been shown to promote tumor invasiveness.27–29 TGF-β can prevent immune cell activation and also plays a role in TH17 cell proliferation.30,31 TGF-β promotes a T-reg phenotype over a THC phenotype in a variety of contexts and increases activation of TH1 THCs.14,32–34 Additionally, deletion of TGF-β2 in dendritic cells has been shown to induce autoimmunity through a mechanism involving poor T-reg induction, which hints that blockade of TGF-β in dendritic cells might be pro-inflammatory and might allow tumor recognition and targeting by the immune system. 35 γδ T-cells, which express TGF-β, appear to augment antitumor responses and might be part of the immune escape mechanism tumors employ. 36 Furthermore, TGF-β signaling promotes an M2 macrophage phenotype, which is the same phenotype that is associated with prostate tumors.6,10 Thus, TGF-β plays a nuanced role in the immune system, often inducing tolerant cell phenotypes, which could affect many of the immunologic processes and cell types implicated in PCa.
Evidence for TGF-β blockade in treating PCa
Data suggest that TGF-β promotes PCa proliferation, invasion, and metastasis through multiple mechanisms. Serum TGF-β1 has been shown to positively correlate with metastasis and PSA levels in patients with PCa.29,37 Additionally, increased prostate tissue co-localization of TGF-β receptors with some of its signaling partners is more common in higher grade tumors.38,39 In vitro data also support a role for TGF-β in PCa aggression and clarify some of its cooperating factors in these processes. In a comparison of malignant and benign cell lines, Yu et al. 40 found that malignant cell lines expressed higher levels of TGF-β1 and were more responsive to TGF-β autoinduction and inhibition with an anti-TGF-β antibody. This aberrant autoinduction was caused by inappropriate recruitment of a protein phosphatase, PP2A, by TGF-βR1, a process which could serve as a therapeutic target. 40 The intracellular domain of TGF-βR1 also co-localizes with amyloid precursor protein-like (APPL), and this interaction promotes invasive behavior in PCa cells in vitro. 38 This study further demonstrated that APPL1-TGF-βR1 co-localization was more common in higher grade tumors from human patients. 38 Another factor that co-localizes with TGF-β receptors, cbl-interacting protein of 85 kDa (CIN85), has also been shown to increase PCa cell migration in vitro. 39 Additionally, CIN85 levels positively correlate with tumor grade and treatment of cells in vitro with TGF-β increases CIN85 expression, which the authors of this study conclude that it suggests a feed-forward loop by which TGF-β signaling upregulates CIN85, promoting invasiveness. 39 The mechanism by which TGF-β1 increases cell migration and invasiveness in vitro in PCa has also been shown to require SMAD3, hypoxia-inducible factor-1α, and TWIST1, implicating canonical TGF-β signaling via SMADs in this process. 28 TGF-β is also connected with epithelial to mesenchymal transition (EMT) in PCa cells as demonstrated by the finding that the tumor suppressor cytoplasmic promyelocytic leukemia protein (cPML) drives invasion in a TGF-β-dependent manner and that TGF-β inhibition decreases cell migration in vitro. 27 TGF-β induces IL-6 production in an in vitro model of PCa, and this inflammatory process leads to invasiveness and growth promotion. 24 Thus, studies of TGF-β in PCa suggests that blocking TGF-β would prevent invasion and metastasis in PCa.
Challenges in treatment with TGF-β blockade
While TGF-β may be involved in metastasis and tumor aggression, TGF-β signaling has also been shown to be antiproliferative, which argues against TGF-β blockade as a treatment strategy for PCa. TGF-βR2-mediated antiproliferative effects are blocked when androgen receptors cooperate with miR-21, a microRNA associated with tumor invasiveness.41,42 TGF-β decreases proliferation and microinvasion in a tumor model, an effect which can be blocked by p21-activated kinase-1 (PAK-1).43,44 Treatment with shRNA to PAK-1 was shown to increase TGF-β and decrease matrix metalloprotease 9 expression leading to decreased invasion as demonstrated by in vitro tumor cell migration across a fibronectin matrix. 43 These data indicate that inhibition of TGF-β in prostate tumors could increase invasive behavior. 43 Furthermore, Al-Azayzih et al. 44 demonstrated that TGF-β overexpression impairs tumor growth in a mouse xenograft model. However, this group also demonstrated that TGF-β promoted EMT as demonstrated by higher levels of EMT markers such as Snail and N-Cadherin in cells with PAK-1 inhibited. 44 Others have also demonstrated a role for TGF-β in EMT through a variety of mechanisms.25,27,45–47 Thus, anti-TGF-β therapy could still be useful in more advanced tumors or in certain types of tumors. Finally, the immune system may be involved in determining whether TGF-β is growth promoting or growth regulating. For example, one study demonstrated that pretreatment with TGF-β prevented PCa apoptosis induced by SB-431542, an anaplastic lymphoma kinase inhibitor. 48 Interestingly, this group also demonstrated that TGF-β treatment of bone marrow-derived mesenchymal stem cells impaired their cytotoxic potential, thereby demonstrating that anti-TGF-β treatment for PCa may be best directed at the immune system rather than the tumor itself. 48 Thus, more clarification of the exact role of TGF-β in PCa is warranted to determine how best to treat tumors by targeting this pathway.
Interleukin-2 and PCa
Many of the immune cells implicated in PCa produce and respond to IL-2, a cytokine that binds to a multisubunit receptor and signals via Janus kinase-signal transducer and activator of transcription phosphorylation. 32 IL-2 is produced by T-cell subsets, dendritic cells, and other immune cell subsets and many immune and non-immune cells in the body possess its receptor.32,49 IL-2 has a variety of pro-inflammatory roles in the immune system, including promotion of TH1 cell and M1 macrophage development, making it a very attractive immunologic candidate for treating cancer.20,50 Additionally, individuals with a polymorphism in IL-2 are at an increased risk for PCa, although the mechanism for this susceptibility has not been determined. 51 This susceptibility due to an IL-2 polymorphism hints that, in the context of PCa, IL-2 may be especially important.
Clinical trials using IL-2 in PCa
IL-2 has been suggested as a potential PCa therapeutic based on human data, and some IL-2-based therapies have been tested in clinical trials. TG4010 is a recombinant viral vector that expresses Muc1, a factor expressed by prostate tumors and associated with a poor prognosis, and IL-2 to increase immune response. 52 TG4010 was associated with a prolonged PSA doubling time and improved progression-free survival, although its phase II clinical trial did not meet its primary endpoint of a 50% reduction in PSA. 52 This treatment has gone on to further clinical trials for lung cancer, meeting its endpoints to progress to a phase III trial, and may be commercially available in the future. 53 A trial using IL-2 in combination with the γδ T-cell agonist zoledronate improved survival in PCa over zoledronate alone and was associated with increased levels of γδ T-cells in the blood. 54 A PCa cell line expressing interferon-γ and recombinant IL-2 has also showed promise in PCa treatment, and, in a phase I/II trial, the vaccine was well tolerated.55,56 Median survival was 32 months among patients receiving the vaccine and PSA doubling time slowed in a majority of the patients.55,56 Other strategies that have been explored are the delivery of IL-2-fusion proteins within a liposome or fusion to an antibody.57–59 Leuvectin, a liposomal delivery of IL-2, was studied as an intraprostatic injection for the treatment of cancer, with the intent to stimulate immune cells to kill PCa cells. 57 The treatment was well tolerated in a phase I clinical trial and appeared to cause a drop in PSA in 2/3 of patients. 57 Two trials of leuvectin in PCa have been terminated, although it is unclear whether this treatment remains in development. 60 A study using an antibody to prostate-specific membrane antigen (PMSA) in combination with low-dose IL-2 treatment also yielded promising results, with tolerable toxicities and PSA stabilization in patients receiving the treatment.60,61 However, this study ended in 2007 and has not yet led to a commercially available therapeutic.60,61 Another study used a vaccine containing PSA as well as IL-2 and GM-CSF in a crossover design with nilutamide, an antiandrogen, as the comparative treatment. 62 The combination treatment showed some efficacy in treating patients with hormone-refractory PCa.62,63 While there were some toxicities attributable to the use of IL-2, patients receiving the three-component treatment first had a trend towards increased survival over the course of the study, and many patients experienced a decrease in PSA or a decrease in rate of rise of PSA.62,63 Additionally, a phase IA/IB clinical trial is underway regarding the use of this vaccine in recurrent hormone naïve and hormone refractory PCa, which will hopefully yield promising results. 60 Finally, there are several clinical trials using IL-2 in PCa that have been completed but have not yet reported their results, indicating that this treatment remains an active area of research. 60 Thus, the results of trials in human patients are very promising and may yield IL-2-related therapies may be able to improve PCa treatment.
Experimental models studying IL-2 in PCa
In vitro and in vivo models also indicate that IL-2 may be useful in treating PCa, and this potential therapeutic remains an active area of research. Sugimoto et al. 58 created a fusion of IL-2 to an anti-PSMA antibody. The addition of IL-2 to this antibody enhanced its cytotoxicity as demonstrated by co-culture of PCa cell lines with human peripheral blood mononuclear cells. 58 The anti-PMSA-IL-2 conjugate antibody also caused more tumor regression in an in vivo mouse model than the anti-PMSA alone. 58 IL-2 was also used as an adjuvant for ex vivo immune cell activation as part of an antibody fused to an IL-15-receptor-α with IL-2 attached. 59 Thus, a variety of engineered antitumor treatments utilizing IL-2 are efficacious in PCa, demonstrating that its use warrants further study.
PCa can also be treated by activating immune cells in vitro or ex vivo using IL-2 and other cytokines, which has been demonstrated to be effective both in vitro and in vivo in animal models. 64 This strategy could prevent the excessive inflammation seen in systemic IL-2 treatment, if the ideal antitumor immune cell subsets are identified, stimulated ex vivo, and then used to treat the patient. 65 Additionally, treatments that act by increasing IL-2 activity may be another approach to favor immunologic reaction to PCa with fewer off-target IL-2-mediated side-effects. For example, use of an agonist of the cell surface marker OX40, a tumor necrosis factor family member that increases IL-2-receptor (IL-2R)-α expression on CTLs and promotes tumor-specific lytic activity, led to tumor regression in vivo. 66 The tumor specificity of OX40 was shown to be dependent on IL-2. 66 Furthermore, combination of OX40, cytotoxic T-lymphocyte-associated protein blockade, and human epidermal growth factor receptor-2 (HER2) vaccination improved survival in a mouse PCa model by enhancing CTL recognition of and response to HER2 found in the tumor and increasing their IL-2 production. 67 These data indicate that inducing IL-2 signaling in the body’s immune system could be used in place of IL-2 itself, especially with more understanding of the IL-2 pathway elements that are most relevant to PCa.66,67
Challenges in treatment with IL-2
IL-2 treatment can lead to hypotension, fever, and nausea, which make it difficult to use clinically.65,68 Numerous strategies have been proposed to prevent toxicity, which may be mediated by downstream targets of IL-2 rather than the IL-2 itself. 68 Strategies for improving IL-2 toxicity have included careful patient selection, appropriate dosing, use with other treatments that decrease the toxicity mediated by downstream targets or engineering of IL-2 treatments in ways that minimize toxicity.65,68–70 Another concern regarding the use of IL-2 in PCa is that one in vitro study showed that IL-2 increased proliferation and PSA secretion in androgen-sensitive cell lines, although this finding was absent in androgen-insensitive cells. 71 These findings indicate that IL-2 may be capable of stimulating PCa cells to grow in some contexts. 71 However, given the success of IL-2 treatment in other models and based on evidence that immune cells are part of the mechanism by which IL-2 could be used to treat cancer, it seems likely that IL-2 treatment is a viable treatment strategy, provided its toxicity can be mediated.
Combination therapies employing interleukin-2 and transforming growth factor-β
IL-2 and TGF-β signaling
The expression and regulation of IL-2 and TGF-β are intertwined, especially in the context of the immune system, and often have antagonistic effects as summarized in Figure 1. These interactions could be exploited to promote immune recognition and attack of PCa cells (Figure 2, Table 1). It has previously been demonstrated that TGF-β attenuates T-cell secretion of IL-2 and prevents IL-2-mediated differentiation of T-cells in vitro.26,72 IL-2 stimulates monocytes and induces expression of its own receptor, while TGF-β inhibits these effects, decreasing IL-2R-γ expression and inhibiting monocyte activation.
73
These two factors also have opposite effects on NK cells, in which IL-2 enhances and TGF-β attenuates killing potential.74,75 When used as components of CD4-targeting nanoparticles, TGF-β and IL-2 promote the transition of T-cells into T-regs in vitro and lead to T-reg expansion in vivo.
33
However, blockade of downstream TGF-β targets prevented TGF-β-mediated upregulation of IL-2-receptor-α and expression of FoxP3, a factor necessary for T-reg development, promoting a CTL phenotype.
76
Treatment of T-cells with a larger volume of IL-2 and use of a TGF-β blocking agent in these nanoparticles might have promoted THC or CTL expansion. Thus, IL-2 and TGF-β interact immunologically and antagonistically, which makes IL-2 enhancement and TGF-β blockade an attractive treatment strategy for activating the immune system against PCa.
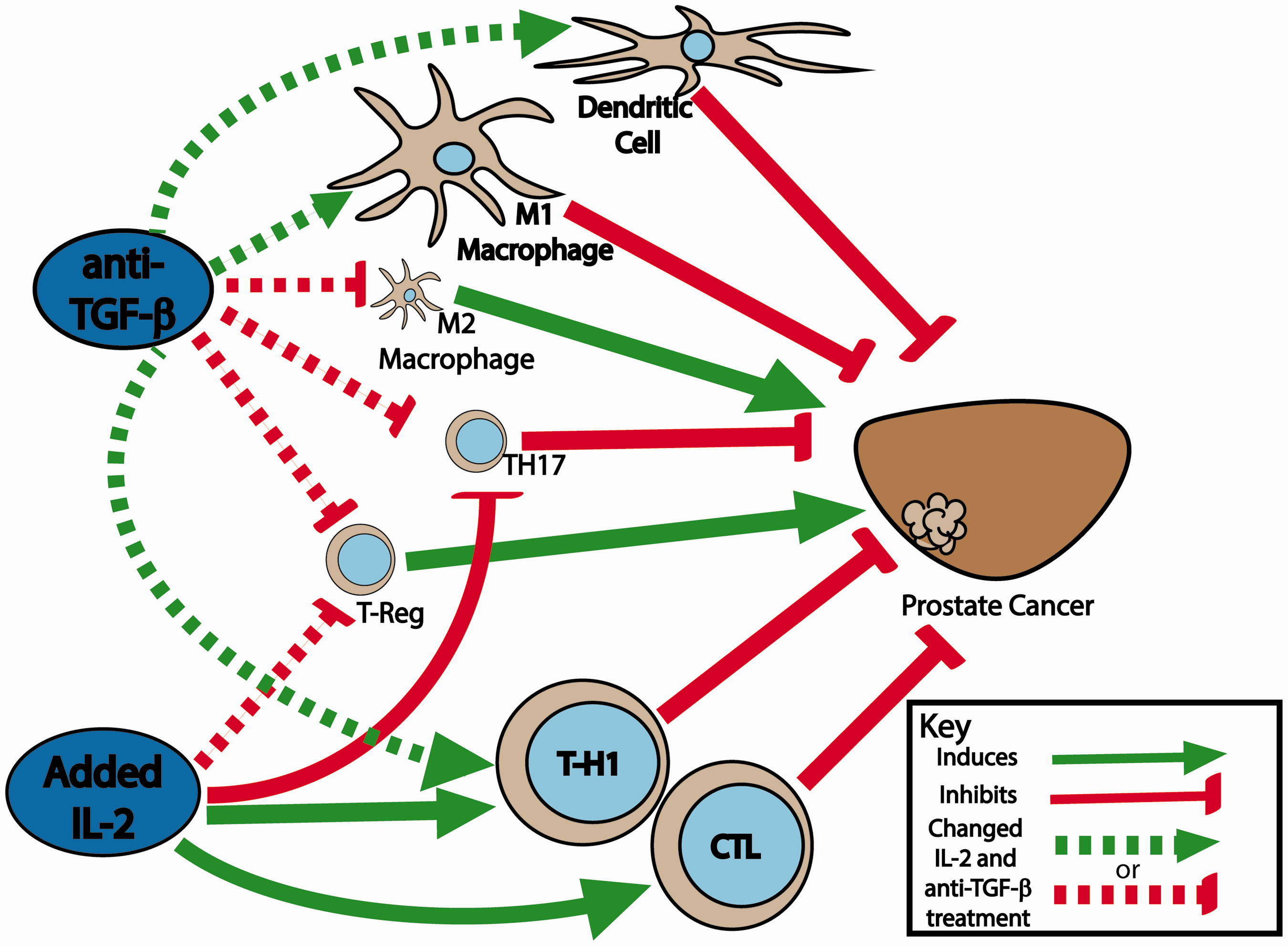
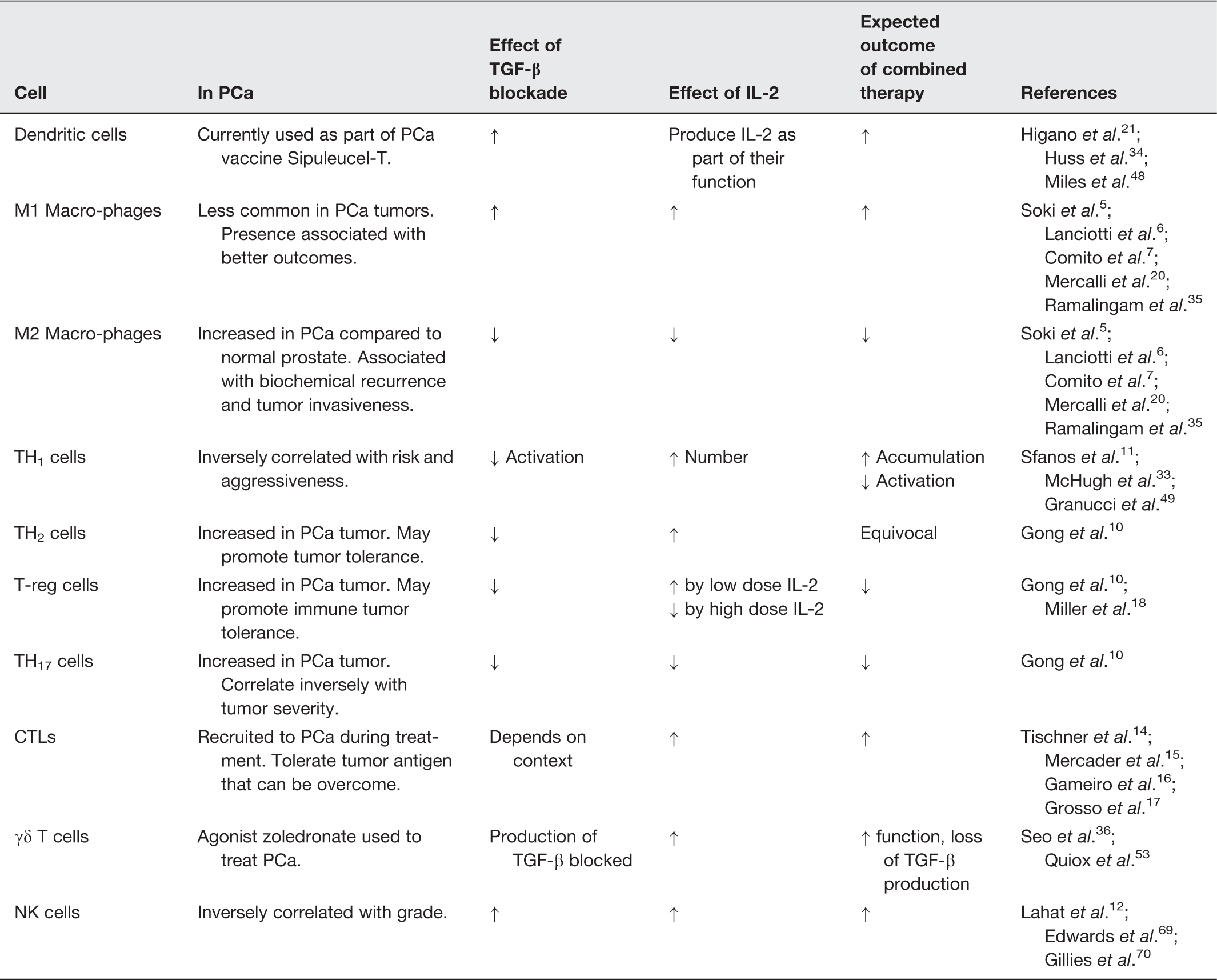
Effects of IL-2 and TGF-β in PCa. TGF-β promotes M2 Macrophages, TH17 cells and T-reg cells, while IL-2 promotes CTLs and TH1 or T-reg cells depending on concentration. Anti-inflammatory cells like M2 macrophages and T-regs promote PCa development while pro-inflammatory cell types like dendritic cells, M1 macrophages, TH1 THCs and CTLs act against PCa. (A color version of this figure is available in the online journal.) Effects of IL-2 combined with TGF-β blockade in PCa. Blockade of TGF-β in combination with IL-2 treatment would promote the development and action of TH1 THC, CTL, M1 macrophages and dendritic cells while inhibiting the development and action of T-regs, TH17, and M2 macrophages. This combination therapy would tip the balance towards an inflammatory phenotype that would favor prostate tumor regression. (A color version of this figure is available in the online journal.) Anticipated reaction of immune cell subsets to PCa in response to combined TGF-β and IL-2 treatment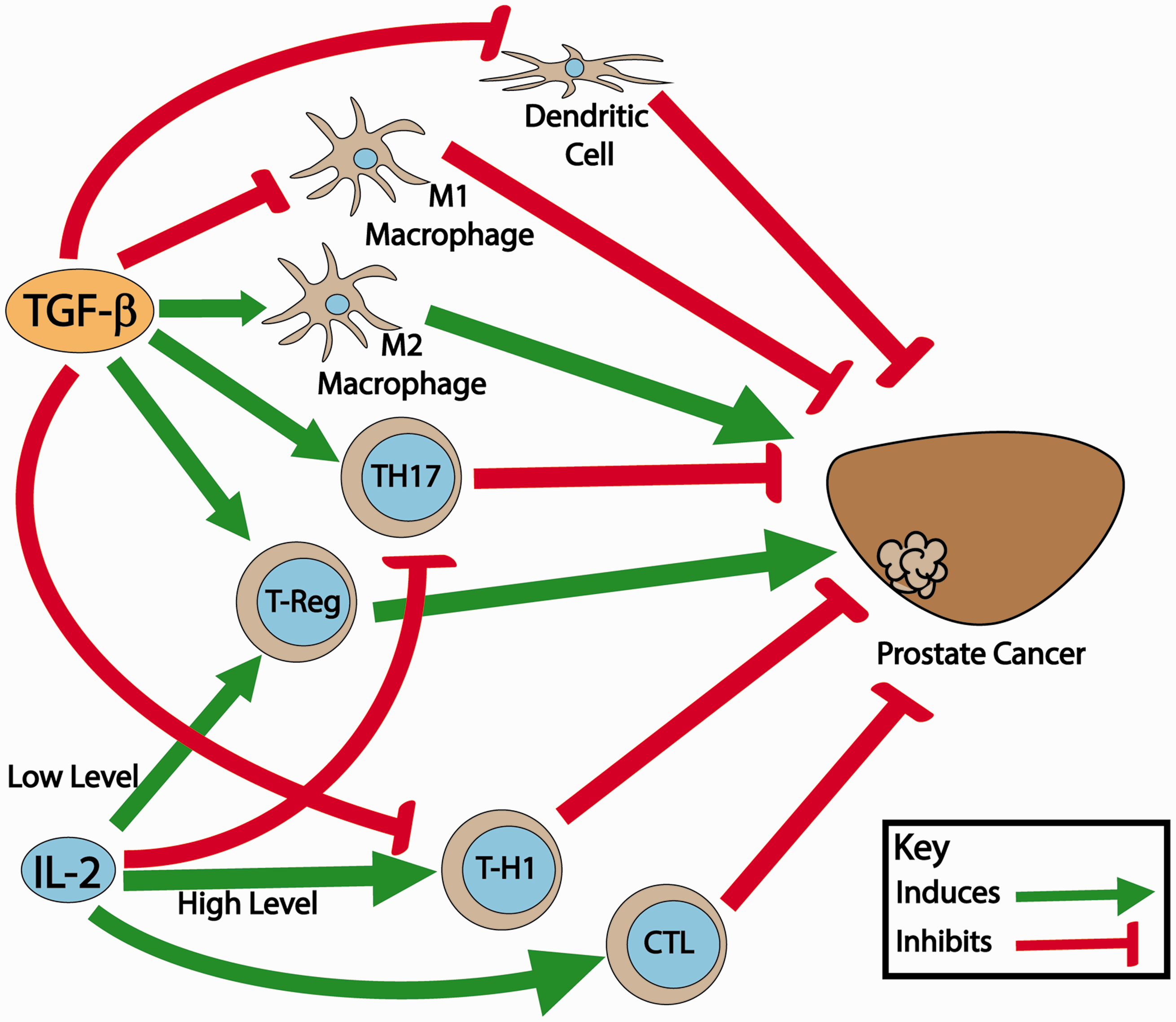
Anti-TGF-β and IL-2 combination therapy in cancer
Combination therapy in PCa
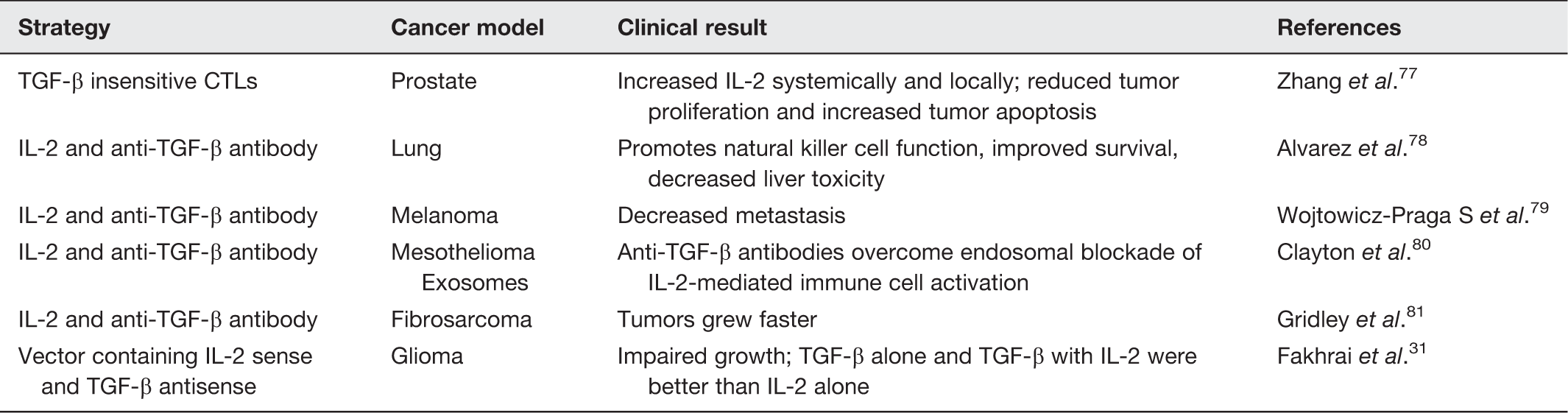
Few studies have addressed both TGF-β and IL-2 in PCa specifically. Zhang et al. 77 demonstrated that TGF-β-insensitive CTLs decreased tumor growth in a PCa model. Interestingly, these mice had increased IL-2, both systemically and locally around the CTLs that invaded the tumors. 77 This indicates that the mechanism behind TGF-β-blockade-mediated tumor attenuation may be modulated by IL-2, meaning that strategies blocking TGF-β and adding IL-2 might be therapeutic in PCa. Additionally, other combination therapies, including some that involve IL-2, have demonstrated promising results in human patients with PCa, indicating that strategies combining immunomodulating agents are viable in this disease. Such strategies include combination approaches using IL-2 along with anti-PSA vaccines, GM-CSF, zoldedronate, anti-PMSA antibodies, and interferon (IFN)-γ.54,55,60–63 The success of combination therapies that include IL-2 in treating PCa indicate that a strategy employing IL-2 and blockade of TGF-β warrants further exploration, especially in light of preliminary evidence using anti-TGF-β and IL-2.
IL-2/anti-TGF-β combination therapy in other cancers
Cancer treatments currently employing combined TGF-β and IL-2
Challenges of IL-2/Anti-TGF-β combination therapy
There is also evidence that IL-2 and anti-TGF-β antibodies could worsen some tumors. Fibrosarcoma cell line tumor xenografts in mice grew faster in the presence of IL-2 and anti-TGF-β antibodies together. 81 The authors of this study attributed this effect to immune hyporesponsiveness, and demonstrated that by a multiple of measures, splenic cells were less prepared to respond to insults. 81 However, cells in the blood, which are more likely to be relevant to PCa, were equally or more able to respond to the same insults. 81 It is possible that the tumor cells themselves were capable of responding to growth signals via IL-2, which has been demonstrated in other fibroblast-like cells.81,82 Furthermore, when the same group repeated their experiments with a lower dose of IL-2, the tumors in the IL-2 alone and anti-TGF-β alone treatment groups grew more slowly when the injection was not at the tumor site but tumors directly injected with either treatment grew more quickly. 83 The researchers concluded that these results indicated a growth effect on the tumors locally but possibly a tumor-inhibitory effect on the immune system caused by the combination therapy, when these factors were administered systemically. 83 Additionally, TGF-β appears to have multiple effects on PCa, potentially promoting its growth and invasion or decreasing tumor size. Park et al. 24 attempted to clarify this by demonstrating that different PCa cell lines reacted differently to incubation with TGF-β1, either increasing or decreasing their growth, indicating that individual tumors may react differently to an anti-TGF-β treatment. This group also demonstrated that TGF-β-mediated induction of replication depends on the Ras/mitogen-activated protein kinase signaling pathway but not on the SMAD pathway. 24 Thus, dosing, timing, and location of administration for TGF-β blockade and IL-2 may be important in determining the response of PCa to this therapeutic strategy.
Strategies for combination therapy
TGF-β and IL-2 are both complicated signaling pathways which could be exploited to treat PCa. Based on current evidence, the mechanism by which IL-2-stimulation and TGF-β-blockade could be used to treat PCa appears multifactorial. Together, these strategies would promote immune activation against prostate tumors. The use of this treatment strategy could prevent metastasis by preventing EMT and promoting IL-2-mediated immune activation against cancer cells outside the primary tumor. Together, these factors could prevent T-reg proliferation and activation in the tumor microenvironment, which could be beneficial in immune detection of primary and metastatic tumors.
To implement a combined therapy to combat PCa, a TGF-β-antibody could be conjugated to IL-2, similar to the work of Sugimoto et al. 58 It might be possible to use this antibody on isolated bone marrow or blood immune cells to avoid stimulating growth in the tumor itself or overactivating the immune system systemically. Additionally, a nanoparticle containing an antibody or TGF-β blocking agent and IL-2-stimulating factors, like McHugh et al. 33 suggest, might be effective for delivery of this combination therapy. Tumor vaccines using tumor cells, viruses, liposomes, or nanoparticles, could employ both TGF-β blocking factors and IL-2 to stimulate the immune system against a prostate tumor or its metastases.33,52,55–57,84 Furthermore, as downstream targets of both factors are identified and their roles in TGF-β and IL-2 are clarified, these factors may serve as more attractive targets. For example, determining how TGF-β signaling decreases tumor growth while increasing EMT might allow for targeting of the EMT-promoting pathway specifically. Furthermore, determining which of the downstream mediators of IL-2 promote immune attack on tumors and which promote toxicity might improve tolerability and efficacy of IL-2-targeted treatments. Several studies have also suggested immune cells activated in vitro using IL-2 can be used to target a tumor. 64 There may be a role for anti-TGF-β treatment in augmenting this type of approach, either in preventing the formation of M2 macrophages and T-regs during in vitro treatment or in treating patients in combination with the stimulated cells.6,7,14,21–23 Finally, more study of IL-2 promotion and TGF-β inhibition might reveal that TGF-β blockade improves IL-2-mediated toxicities and that IL-2 blocks some of the tumor growth-promoting effects of TGF-β by stimulating the immune system. 78
Future research for combined IL-2 enhancement and TGF-β blockade
In order to effectively utilize blockade of TGF-β and IL-2 as a combination therapy, more research must be done defining the roles of these factors and refining their use. IL-2 has multiple receptor subunits, which have variable effects, and TGF-β has multiple isoforms and multiple receptors, each of which utilizes different signaling cascades.24,26,32,75 Therefore, it is important to drill down on which isoforms or downstream mediators are important for mediating synergistic effects. Additionally, because TGF-β signaling may prevent growth or enhance metastatic potential, TGF-β blocking treatments may be beneficial or detrimental depending on the stage of the tumor, and the ideal timing for its use requires clarification. For both factors, doses would need to be determined and efficacy in human PCa would need to be documented. Furthermore, like many treatments, there are probably patient populations who would benefit more significantly from a combined TGF-β blockade and IL-2 treatment strategy. These patients would need to be identified and markers for their identification would need to be selected.
The immune cells involved in TGF-β- and IL-2-mediated effects on PCa would also need to be studied to effectively utilize these factors as a treatment strategy. Because IL-2 can select for the development of T-regs or effector T-cells, the dose would need to be adequate to support antitumor immune response but not so high as to induce systemic inflammation.14,19,65,68 Additionally, because IL-2 treatment in combination with γδ T-cell stimulation demonstrated efficacy in PCa, the role of γδ T-cells in PCa and the effect of IL-2, as well as TGF-β, on these cells warrants further characterization to guide the design of PCa-targeted therapies. 54 Additionally, cells that respond to TGF-β, which include macrophages and TH17 cells, need to be studied in the context of TGF-β blockade and IL-2 treatment in PCa to further clarify which cells might respond to anti-TGF-β treatments. 85
Furthermore, it would be expected that IL-2 and TGF-β blockade would be synergistic based on evidence in other cancers.31,74,75,78,79 More clarification of the intersection points of the IL-2 and TGF-β signaling pathways and cooperative processes mediated by both are needed to understand how they interact in PCa and adequately design therapies exploiting these pathways. TGF-β has been shown to inhibit IL-2 production, but the mediators of this inhibition have not been completely studied. 86 Additionally, TGF-β has been shown to prevent IL-2-mediated T-cell proliferation and synergize with IL-2 to promote T-reg, especially inducible T-reg, development, and blocking T-reg induction might improve the immune response to tumors.14,26,87 T-reg cells may also possess surface TGF-β, which may mediate some of their suppressive functions and might also be subjected to blockade by an anti-TGF-β approach. 88 Additionally, while TGF-β has been shown to favor the anti-inflammatory M2 macrophage phenotype, M1 pro-inflammatory macrophages produce IL-2 and express IL-2Rα, indicating that macrophages may be another target for anti-TGF-β and IL-2 combination therapy.6,7,20 Finally, there is evidence that anti-TGF-β treatment might attenuate IL-2 toxicity. 78 This effect also warrants further exploration for PCa and other applications of IL-2.
Conclusions
In spite of separate evidence for blocking TGF-β and treatment with IL-2 as PCa therapy and evidence for the two factors together in other tumor models, to our knowledge, there have been no studies of these therapies combined in PCa. To utilize this promising combination, more evidence needs to be gathered about components of each pathway and their interaction together especially in the context of PCa. Because of several encouraging results using the combination of IL-2 and TGF-β in other cancers and because of evidence for each individually in PCa, this subject warrants future study.
Footnotes
Author contributions
All the authors performed the literature search, wrote, and created the tables and figures. KAM assisted with the literature search, writing, and editing and provided expert opinion as a practicing urologist. KMD and WEZ served as co-contributing authors.
Acknowledgments
There was no funding to support this minireview. KMD is a recipient of a Sigma Xi Grant-in-Aid entitled ‘Defective Interleukin 2 Signaling in System Lupus Erythematosus Impairs Wound Healing’.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.