
Abstract
We evaluated the clinical value of flexible ureteroscopic lithotripsy for the treatment of upper urinary tract calculi in infants. Fifty-five infants with upper urinary tract calculi were included in this study: 41 males and 14 females. Retrograde intrarenal surgery was performed by an 8 Fr/30 cm flexible ureterorenoscope (POLY®) combined with a holmium laser. CT scanning or radiography of the kidneys, ureters, and bladder region was performed one month after the operation to confirm the clearance of calculi. All the 55 infants with calculi in 74 sides underwent 66 flexible ureteroscopic lithotripsy procedures. The median operation time was 30 min. The median amount of flushing fluid was 500 mL. The stone-free rate after a single session treatment was 94.6%, within which 10 infants underwent simultaneous bilateral flexible ureteroscopy lithotripsy. Catheters were retained in 45 infants for 24–48 h after the operation. Continuous high fever due to reflux was present in two cases. Flushing fluid extravasation was found in one infant. Some patients with minor complications, such as mild hematuria, irritation symptoms, and low fever, recovered without treatment. The duration of hospitalization time after the operation was approximately 1–5 days. Flexible ureteroscopic lithotripsy is a safe, highly efficient, minimally invasive, and reproducible operation for removal of upper urinary tract calculi in infants. This technique is a convenient method for postoperative management of patients that enhances their rapid recovery. It is a promising option for therapy of infants ineffectively treated by extracorporeal shockwave lithotripsy.
Introduction
The incidence and prevalence of pediatric urolithiasis are approximately 1–3% of those in all-age patients but are steadily increasing.1,2 The stones of upper urinary tract include ureter calculi and kidney calculi. The use of an efficient, safe, less invasive, and reproducible surgical procedure that can be followed by easy postoperative care is important to pediatric patients.
Extracorporeal shockwave lithotripsy (ESWL), percutaneous nephrolithotomy (PCNL), and ureteroscopy (URS) have been the major choices to remove stones in the upper urinary tract in infants so far. However, multiple ESWL treatments can cause long-term and irreversible damage to the kidneys and ureter. In addition, this type of lithotripsy needs special equipment for infants and children, and the residual stone fragments may lead to recurrence of urolithiasis. 3
PCNL is commonly used in the treatment of upper urinary tract stones. This method is suitable for patients with larger stones or hydronephrosis. However, the renal size of infants is only half that of adults. Thus, it is exceedingly difficult for the operator to manipulate in the small space available, and the risk of bleeding and surgical complications in infants is higher than that in adults. The treatment of complications is also difficult due to the poor tolerance of the developing kidneys in infants.4,5 Most infantile urolithiasis is secondary to metabolic disorders and usually has high recurrence rates, resulting in a need for repeated treatments. However, repeated PCNL procedures performed in the developing kidneys of infants might lead to an increase in the risk of long-term renal atrophy. Therefore, mini-PCNL was suggested for the treatment of infantile urolithiasis.6,7 Until now, only few hospitals can accomplish surgical treatment of infantile urolithiasis. Thus, an eventual delay in the treatment is possible after lingering in several hospitals without successful admission.
URS has been used in the treatment of upper urinary tract urolithiasis in children. 8 However, its application usually results in residual calculi due to the stones moving into the kidneys. 9 Flexible URS is a novel and natural orifice transluminal surgery approach. Recently, the applications of flexible URS in the diagnosis and therapy of upper urinary tract urolithiasis in adults have been broadened dramatically. 10 However, the reports of the utilization of this technique in infants and children are still limited. Kim et al. performed 170 ureteroscopic procedures in 167 children (mean age, 62.4 months) with urinary calculi. The researchers achieved good results with no significant intraoperative or postoperative complications after a mean follow-up of 19.7 months. 11
In the present study, flexible URS lithotripsy was performed in 55 infants with upper urinary tract calculi in our institute to evaluate its efficacy and safety.
Patients and methods
Patients
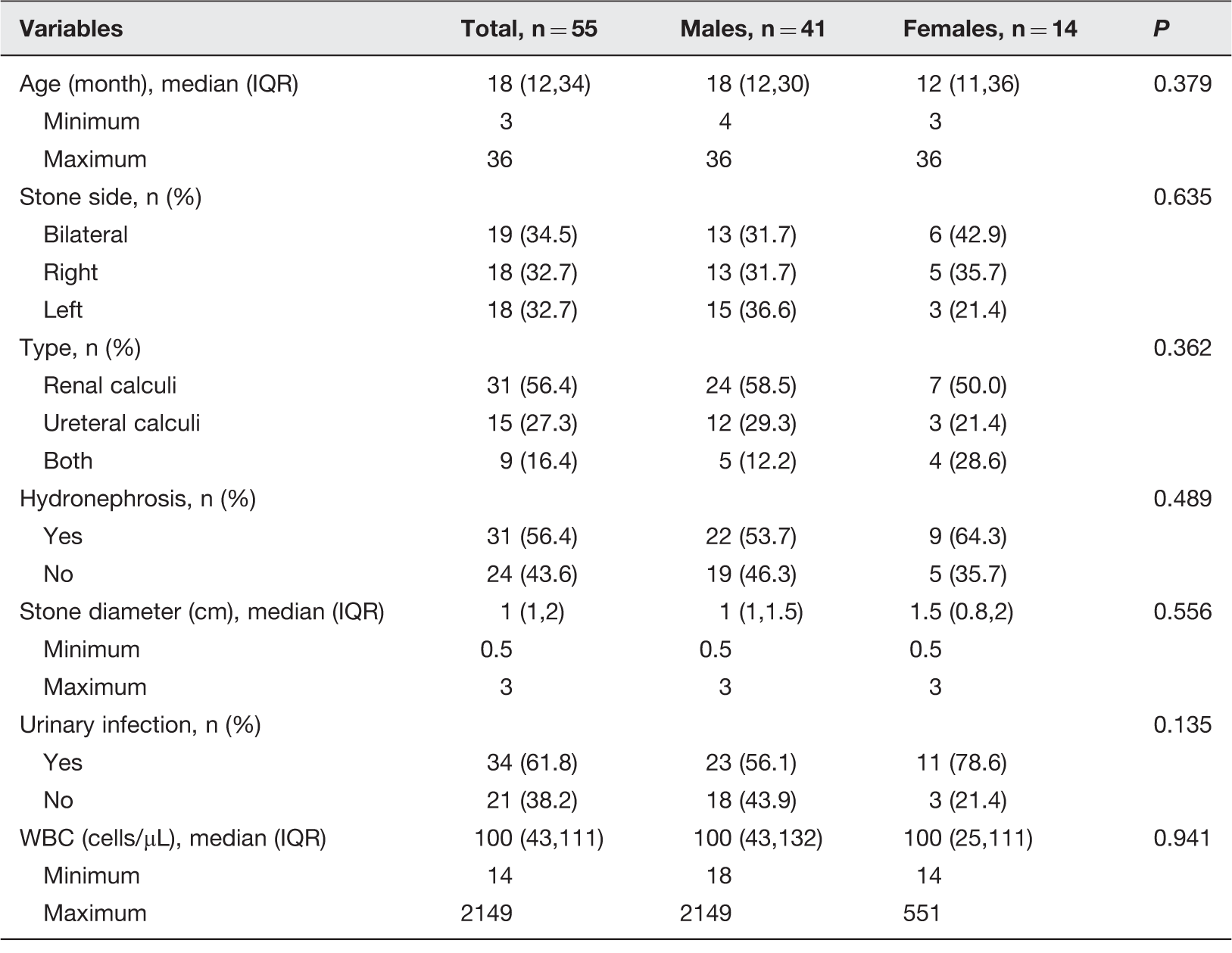
Fifty-five infants, 41 males and 14 females aged from 3 to 36 months (median age, 18 months), of consecutive case series with upper urinary tract calculi treated in the Urology department of Beijing Friendship Hospital were included from June 2014 to May 2015 (Figure 1(a) and Table 1). Retrospective information of the 55 infants was analyzed to investigate the efficacy and safety of the flexible URS lithotripsy in treatment of pediatric urolithiasis of upper urinary tract. Before operation, diagnosis was performed by routine ultrasound, plain radiograph of the abdomen (kidney, ureter, and bladder (KUB)), intravenous urography, and urinary tract CT scan in all patients.
(a) A standard rigid ureterorenoscope for adult and a flexible ureterorenoscope for infants are shown (POLY®, Germany); (b) A 14-month-old boy with bilateral staghorn renal Cys calculi (B1), or after surgery (B2) detected by using flexible ureteroscopy lithotripsy fiber; (c) a radiographic image of a 24-month-old girl which depicts bilateral ureter reimplantation with a 3 cm calculus in her right ureter. Two 4.7-Fr/12 cm ureteral stents were inserted into the ureter forward (c1). The calculi were crushed by a flexible URS (c2); (d) radiography of the KUB indicates primary hyperoxaluria (d1) and reconstruction by using CT scan (d2). (A color version of this figure is available in the online journal.) Clinicopathological characteristics of subjects according to sex IQR: interquartile range. Remark: Two infants with two-sided calculi accompanied by oliguria; two infants with neurogenic bladder; two infants with previous ureteral reimplantation with stones located in the replantation of ureter.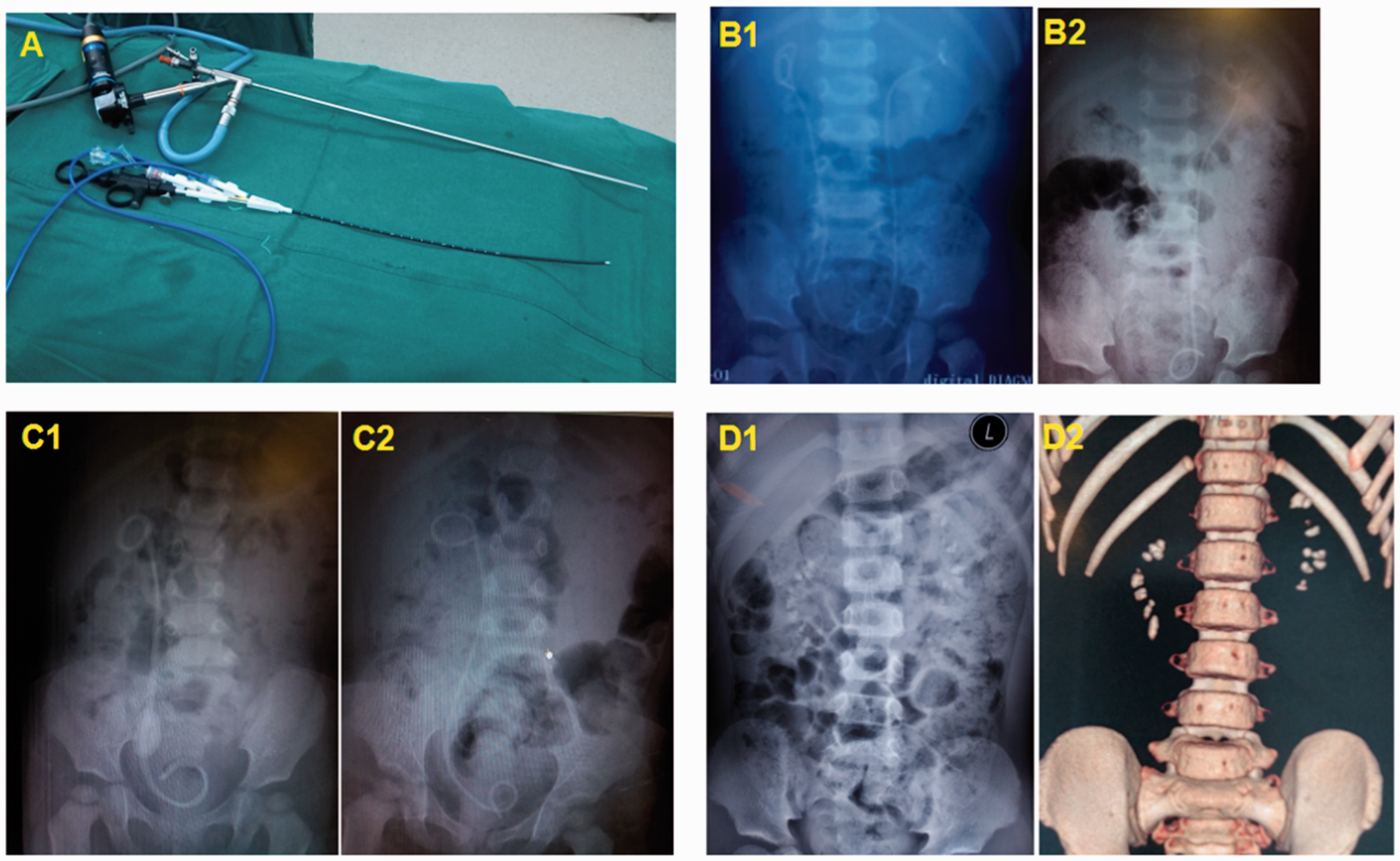
Surgical technique
We did not have a short length (less than 16 cm) stent whose caliber was larger than 6 Fr. Therefore, ureteral stents 4.7 Fr/12–16 cm (COOK, USA) were indwelled in all infants under vein anesthesia prior to operation. For general anesthesia prior to lithotripsy, laryngeal mask was used, or endotracheal intubation was performed. Special insulation blankets for infants were used. Isotonic flushing fluid and iodine disinfectants were heated to 36℃. After conventional disinfection of the perineum, the double-pigtail ureteral stents were removed by 8/9.8 Fr rigid ureteroscope. The bladder was filled with flushing fluid, and then suprapubic bladder puncture was undertaken by a 14 G vein detained needle. The flushing fluid was discharged continuously during the operation. URS was performed by a 4.5 Fr rigid ureteroscope to confirm the clearance of the ureteral line. The ureteral calculi were crushed by holmium laser or pushed into the pelvis. A 0.035 in. nickel–titanium guide wire was left.
After the 8 Fr/30 cm flexible ureterorenoscope (POLY®, Germany) was placed into the renal pelvis (Figure 1(c)), the guide wire was withdrawn. The flexible ureterorenoscope was used to detect each renal calyx and position the calculi. Then, the 200 µm laser fiber was placed in the pelvis to crush calculi layer by layer. Laser power was set to 20–40 W (0.6–0.8 J × 24–50 Hz). After the retrograde intrarenal surgery, the 0.035 in. nickel–titanium guide wire was left, and the 4.7 Fr/12–16 cm ureteral stent was inserted. Antibiotics were used for 24–48 h after the operation. Twenty-four hours and one month after surgery, CT scan or KUB radiography was performed to confirm the clearance of calculi. The absence of existing residual calculi was the standard criteria for complete clearance. The ureteral stents were removed 1–2 months after surgery.
Statistical analysis
Count data were presented by percentage (%). Chi-square or Fisher statistical tests were used for comparison of the two groups. Quantitative data were presented by median and interquartile range statistics. The t-test or the two-sample Wilcoxon test was utilized in the comparison of the two groups. SAS 9.3 program was employed for the statistical analyses.
Results
Clinicopathological characteristics of subjects according to stone diameter
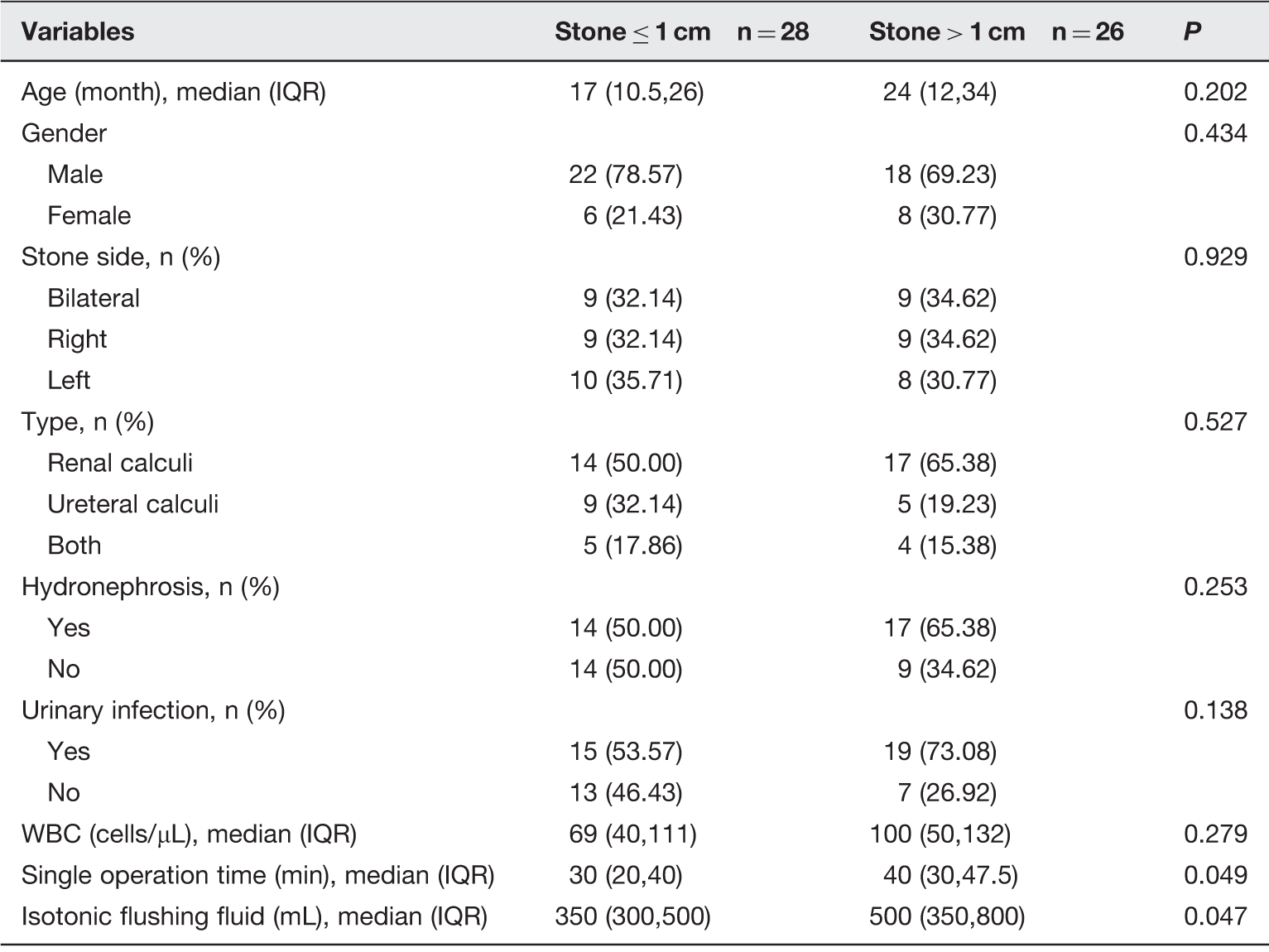
IQR: interquartile range.
The median diameter of the calculi was 1.0 cm (range 0.5–3.0 cm) (Table 1). The results of urinalysis and urine culture indicated that 34 infants had urinary tract infection with median accounts of 100 WBCs/µL (range 14–2149 cells/µL). Furthermore, there were differences between small stone subgroup (>1 cm) and large stone subgroup (≤1 cm) in the incidence of urinary infection (53% versus 73%, Table 2). Only single operation time (P = 0.049) and isotonic flushing fluid (P = 0.047) had significant differences in various stone sizes (Table 2). The small population of subgroups should be also concerned. Two cases with high fever belonged to large stone subgroup, and one of them also had uretero pelvic junction (UPJ) obstruction.
Thirty-one infants suffered from hydronephrosis, two infants had bilateral calculi accompanied by oliguria, and two infants experienced neurogenic bladder symptoms (Table 2). In addition, two infants with previous ureteral reimplantation had stones located in their ureter–bladder junction (Table 1). According to the results of urine culture, sensitive antibiotics were used two days before the operation.
Operation and complications after operation.
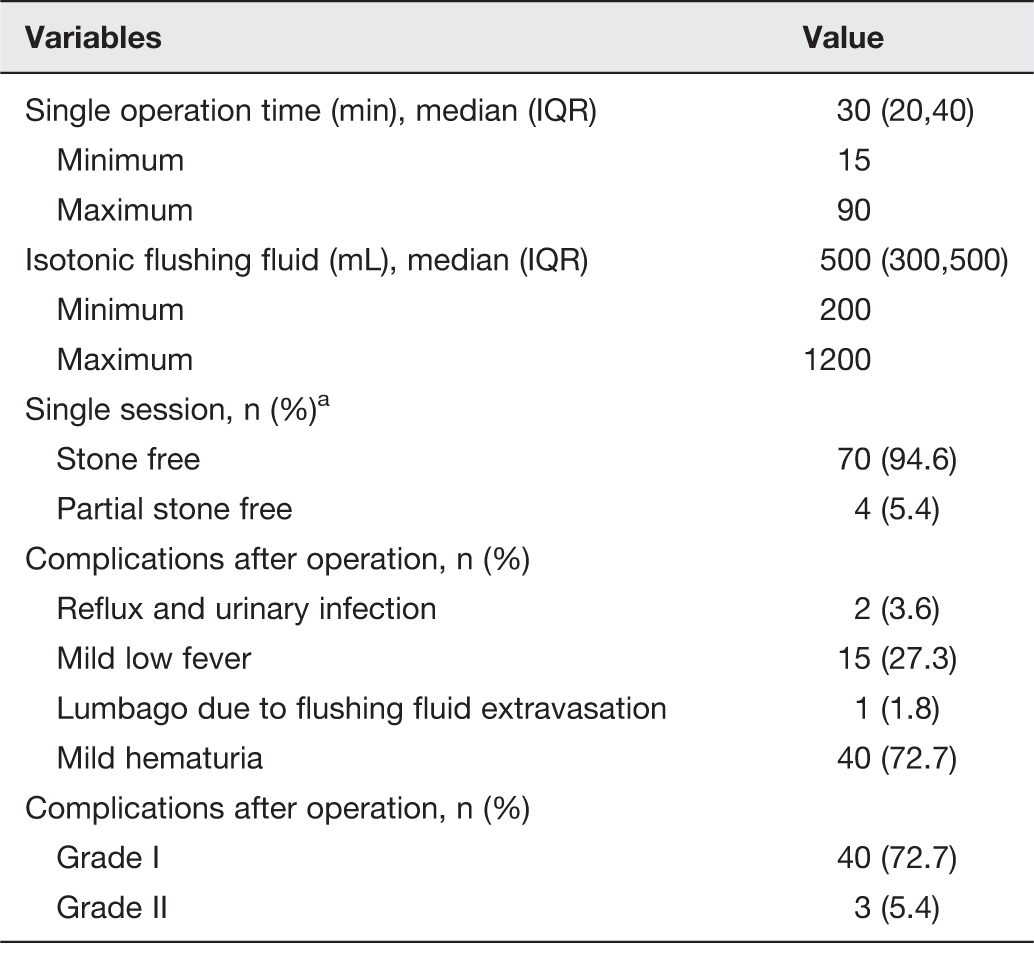
IQR: interquartile range.
aRemarks: Fifty-five patients had calculi in 74 sides. All complications were I–II grade according to Common Terminology Criteria For Adverse Events.
Cohen ureterovesical reimplantation was performed in one reimplantation case, in which the ureteral orifice could not be identified; a 0.035 in. nickel–titanium guide wire was initially inserted anterogradely through ultrasound-guided renopuncture. Then, the guide wire was pulled out by cystoscopy through the urethra. A double-lumen catheter was pushed retrogradely into the pelvis via the guide wire. Further, another guide wire was inserted retrogradely through the double-lumen catheter. Finally, two 4.7 Fr ureteral stents were simultaneously retrogradely inserted to dilate the ureteral mouth (Figure 1(b)).
Forty-five catheters were retained in some infants for a period from 24 to 48 h after operation. All patients were willing to drink 1 h and eat 2 h after operation. Routine ultrasound was performed after 24 h, and no hydronephrosis and perirenal effusion were found. Due to the powder formation, calculi fragments were collected only in 14 cases to analyze their composition. In four of the cases, calcium oxalate monohydrate and dihydrate were predominant, whereas in 10 of the cases Cys calculi were formed. Primary hyperoxaluria was clinically diagnosed in three cases by CT scan and KUB radiography; the diagnoses in these cases were further confirmed by genetic analysis (Figure 1(d)).
Nevertheless, complications were also found after the operation (Table 3). There were two cases with continuous high fever (39–40℃, 3–5 days), because of active painful urination leading to reflux and urinary infection. These patients were treated by venous injections with carbapenems and γ-globulin. There were minor complications in some patients without treatment, such as low fever (37–38℃, 15/55 cases) due to overheating during operation, lumbago (one case) due to flushing fluid extravasation, mild irritation symptoms (one case) during urination, and mild hematuria (72.7%, 40/55 cases) for 1–3 days. Therefore, hospitalization time after the operation was 1–2 days after operation, if no complications were found. Only two infants with high fever after operation needed longer hospitalization time (3–5 days). The ureteral stents were removed, and KUB radiography was performed for a period from one to two months to recheck whether there was reoccurrence of stones after the surgery.
Discussion
Urolithiasis is less prevalent in children than in adults. However, the exact incidence of infantile urolithiasis is still unknown. Due to the lack of expression ability, clinical manifestations of urolithiasis in infants are different from those in adults. Subjective symptoms are rare, and often no typical renal colic is observed. Therefore, illnesses in pediatric patients are usually more severe than observed due to their insidious onset. The main manifestations include oliguria, hematuria, or absence of urine formation, which are accompanied by fever, crying or listlessness, poor diet, and other systemic symptoms. The disease progresses rapidly leading to renal failure in the severe cases. 13 Therefore, urolithiasis in infants is more dangerous than in adults.
In this study, two of 55 children expressed oliguria and renal insufficiency. They were all in complete remission through emergent indwelling bilateral ureteral stents. The upper urinary tracts of infants were still undergoing development. Generally speaking, metabolic abnormalities-associated urolithiasis is more common in infants than in adults, which usually results in frequent recurrence of urolithiasis. Alpay et al. evaluated the clinical features of 93 children diagnosed with urolithiasis one year earlier. 14 They reported that 79.5% of all the children had urinary metabolic abnormalities, most of which presented by hypercalciuria. Analysis of the stone composition in the 14 infants indicated that there were 10 cases with cystine urolithiasis and four cases with calcium oxalate urolithiasis. The mini-PNL has high safety and slight trauma, SWL can prevent the previous traditional surgery patients suffering bleeding and restore slow shortcomings, and the semirigid ureteroscope is easy to achieve the target position in ureteric stones.6,7 However, we do not recommend Mini-PCNL to treat infant’s stones less than 3 cm, because PCNL cannot be performed repeatedly due to the recurrence of stones. In addition, ESWL can only be performed within two times in one position, because the infant’s kidney is too small to be manipulated repeatedly. Therefore, minimal invasion, reproducible surgery, less drainage catheter indwelled, and convenient nursing after the operation must be the feature of operations to respond adequately to the trend of high recurrence rate of urolithiasis in infants. Rigid, semirigid, and flexible URS all belong to the RIRS procedure. Flexible URS lithotripsy is the only choice to achieve all these desired properties.
Nerli et al. reported that approximately 90% of complete stone-free rate was achieved after a single ureteroscopic session in a total of 80 children with 88 ureteroscopic procedures. They suggested that single and small (< 1 cm) calculi could be cleared completely after a single ureteroscopic session. 15 The stones were larger in our 55 patients with 74 sides of calculi. Median diameters of the calculi were 1.0 cm (range 0.5–3.0 cm). The complete stone-free rate was 94.6% (70/74) after a single ureteroscopic session. Only two patients underwent three ureteroscopic sessions. In addition, only partial stone-free rate was achieved in four patients with various sizes of Cys calculi. The largest diameter of the calculi was between 2.0 and 3.0 cm (Table 2).
So far, there are no reports concerning the applications of flexible URS in the treatment of upper urinary tract urolithiasis in infants. Unsal and Resorlu reported that 16 urolithiasis patients (mean age 4.2 years), including some infants, were treated successfully by using flexible URS. They suggested that the utilization of flexible URS in the therapy of infantile urolithiasis can enhance operational safety and ensure high efficiency by minimal invasion. 16 The median age of our 55 patients was 18 months (range 3–36 months). By using flexible URS, we succeeded in 66 lithotripsy procedures of 55 infants, including 10 infants undergoing bilateral flexible URS. In some infants, catheters were retained for 24–48 h after operation. Only two of the patients had postoperative high fever, and one had flushing fluid extravasation. Some infants had mild transient urinary tract irritation, mild fever, and visible hematuria, but did not need special treatments (Table 3). All infants were discharged from the hospital from day 1 to 5 after surgery. Our findings indicate that flexible URS can be used safely and efficiently in patients younger than three years of age.
Unlike adults, the tolerance of infants to surgery and anesthesia is poor.17,18 Four novel features were revealed in our study. First, the male infants had a narrow urethral caliber (8–10 Fr), which could only be inserted by flexible URS but could not retain the access sheath of flexible URS. Thus, it was prone to induce body fluid overloading during operation due to the lower body weight and total circulation volume of infants. Therefore, less perfusate used in a single ureteroscopic session was allowed. The median amount of isotonic perfusion of single operation in our 66 ureteroscopic procedures was 500 mL (range 200–1200 mL).
Second, the development of infants is not complete, and their ability to control body temperature is poor. Therefore, disinfection, flushing fluid in circulation, and the naked body might lead to a rapid drop in body temperature. The low body temperature would result in a slow heart rate, which is unable to maintain a normal blood pressure leading to metabolic disorders and eventually threatening the lives of infants. Therefore, thermostat measures and real-time body temperature monitoring are necessary. We performed 66 ureteroscopic procedures under real-time control of body temperature, which maintained the body temperature of patients at 36.0–36.8℃ and the heart rates at 110–130 beats/min.
Third, the diameter of the infant kidney is only a half of that of the adults. The cramped renal pelvis or calyces is not conducive to the steering of flexible URS in the kidney without fluids. Access sheath cannot be used because of the small caliber of babies’ ureter and urethra. Therefore, low-energy and high-frequency laser is required to smash the stones to remove them easily. The operation time in infants is slightly more extended than that in adults with the same size of calculi. However, the formation time of calculi in infants is shorter resulting in the more fragile structure of the latter, which is easier to powder by holmium laser. The median calculi diameter of our patients (74 sides) was 1.0 cm (range 0.5–3.0 cm). By using laser lithotripsy (20–40 W; 0.6–0.8 J × 24–50 Hz), the calculi were completely smashed to powder. The median operation time was approximately 30 min (range 15–90 min).
Fourth, the length of ureters in infants is only 10–12 cm. The fragile kidney can easily be hurt by operation instruments. On the other hand, the length of adult’s flexible URS is approximately 60–70 cm, making the surgical manipulations difficult in infants. A short-length combined flexible URS (8 Fr/30 cm) was applied in the surgery, which was suitable for use in infants. The device was more flexible than the ones used before, which allowed shortening of the time needed and increased the efficiency of clearance. Furthermore, the core components can be replaced easily. In our investigation, the distal end of the optic fiber sheath was covered by a slide, which separated the optic fiber from infant’s kidney, ensuring the safety of the operation.
One limitation of our studies is the lack of possibility to explore the causes of calculi formation in infantile urolithiasis. It is extremely important to address the formation pathway to block the development of calculi in the urinary tract of infants, which can definitely prevent the recurrence and efficiently reduce the number of operations required for complete treatment. Therefore, we will further elucidate the causes of formation of calculi in infantile urolithiasis and examine the methods to be performed for the prevention of calculi formation in infants. In addition, it was difficult to describe the exact position of renal stones, because the structure of infant’s calyxes was undeveloped, their stones were mostly located in pelvis. Furthermore, the small population of subgroups should be increased to improve the statistic significances (Table 1 and 2). Requirement of three sessions (stent insertion, URS, stent removal) to clear even a small ureteric stone might also be a drawback of flexible URS.
Taken together, flexible URS lithotripsy is a safe, highly efficient, minimally invasive, and reproducible surgery technique for therapy of upper urinary tract calculi in infants. It is also convenient for postoperative management of patients to get rapid recovery. It might be a promising method for the patients ineffective to the treatment by ESWL.
Footnotes
Author’s contribution
All authors participated in the design, interpretation of the studies and analysis of the data and review of the manuscript, and all participants contribute equally.
Acknowledgements
This study was funded by Beijing Municipal Science and Technology (Z151100004015106).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.