
Abstract
Synthetic glucocorticoids (GCs) are widely used in the variety of dosages for treatment of premature infants with chronic lung disease, respiratory distress syndrome, allergies, asthma, and other inflammatory and autoimmune conditions. Yet, adverse effects such as glucocorticoid-induced osteoporosis and growth retardation are recognized. Conversely, 2-oxoglutarate (2-Ox), a precursor of glutamine, glutamate, and collagen amino acids, exerts protective effects on bone development. Our aim was to elucidate the effect of dietary administered 2-Ox on bone loss caused by neonatal treatment with clinically relevant maximal therapeutic dexamethasone (Dex) dose. Long bones of neonatal female piglets receiving Dex, Dex+2-Ox, or untreated were examined through measurements of mechanical properties, density, mineralization, geometry, histomorphometry, and histology. Selected hormones, bone turnover, and growth markers were also analyzed. Neonatal administration of clinically relevant maximal dose of Dex alone led to over 30% decrease in bone mass and the ultimate strength (P < 0.001 for all). The length (13 and 7% for femur and humerus, respectively) and other geometrical parameters (13–45%) decreased compared to the control (P < 0.001 for all). Dex impaired bone growth and caused hormonal imbalance. Dietary 2-Ox prevented Dex influence and vast majority of assessed bone parameters were restored almost to the control level. Piglets receiving 2-Ox had heavier, denser, and stronger bones; higher levels of growth hormone and osteocalcin concentration; and preserved microarchitecture of trabecular bone compared to the Dex group. 2-Ox administered postnatally had a potential to maintain bone structure of animals simultaneously treated with maximal therapeutic doses of Dex, which, in our opinion, may open up a new opportunity in developing combined treatment for children treated with GCs.
Impact statement
The present study has showed, for the first time, that dietary 2-oxoglutarate (2-Ox) administered postnatally has a potential to improve/maintain bone structure of animals simultaneously treated with maximal therapeutic doses of dexamethasone (Dex). It may open the new direction in searching and developing combined treatment for children treated with glucocorticoids (GCs) since growing group of children is exposed to synthetic GCs and adverse effects such as glucocorticoid-induced osteoporosis and growth retardation are recognized. Currently proposed combined therapies have numerous side effects. Thus, this study proposed a new direction in combined therapies utilizing dietary supplementation with glutamine derivative. Impairment caused by Dex in presented long bones animal model was prevented by dietary supplementation with 2-Ox and vast majority of assessed bone parameters were restored almost to the control level. These results support previous thesis on the regulatory mechanism of nutrient utilization regulated by glutamine derivatives and enrich the nutritional science.
Introduction
Glucocorticoids (GCs) are widely used in pediatric practice.1–6 GCs administration is an established therapy to lessen chronic lung disease, in the treatment of asthma and croup, and to reduce mortality in premature infants with respiratory distress syndrome.4,7–10 A growing group of children is chronically exposed to steroids through the increasing incidence and prevalence of childhood atopy, related to environmental pollution and processed food, and it is estimated that 10% of children and adolescents have or require some form of GCs treatment.3,6
Despite this variety of beneficial applications of GCs, often lifesaving, there is a growing body of evidence for their adverse effects, i.e. suppression of the hypothalamic–pituitary–adrenal axis, decrease in weight gain, bone loss and growth retardation, and many more.3–7,11–13 Furthermore, glucocorticoid-induced osteoporosis (GIO) is the most common iatrogenic cause of secondary osteoporosis as a long-term side effect of clinical use of GCs. 4 Children treated with GCs have lower spine bone mineral density (BMD) and higher rates of morphometric fractures compared to healthy ones. 2 Nevertheless, several possible mechanisms of GIO are proposed in this regard. On the one hand, inhibition of bone formation by bone cells imbalance caused by increased apoptosis and lower activity of osteoblasts and osteocytes along with additional effect of GCs on regulatory proteins ratio. On the other hand, a rapid bone loss related to diminished synthesis of proteins such as collagen or osteocalcin (OC) as well as disturbance in cell signaling leading to malfunction of repair mechanisms and bone fragility following microdamage accumulation.1,2,4,9 However, evidence-based management guidelines for children who require a long-term GC therapy are not well established. Since clinical trials involving children on GCs are sparse, treatment options for GIO in children are greatly limited.1,2 Recent studies show limited information on bisphosphonates, vitamin K2, D, calcitriol, and calcium supplementation in this regard.1,3,4,9 On the other hand, studies in animals and humans revealed protective effects of 2-oxoglutarate (2-Ox) (alpha-ketoglutarate) on bone loss caused by gastrectomy, ovariectomy, menopause, and GCs prenatal administration.14,15
2-Ox is a crucial intermediate in the tricarboxylic acid cycle, taking part in the cellular energy metabolism and in a variety of metabolic pathways as an important nitrogen transporter. It bridges cellular energy metabolism with the metabolism of amino acids, does not show toxic properties, and is highly stable in water solutions. However, since it is impossible to utilize 2-Ox from the tricarboxylic acid cycle in the synthesis of amino acids, it has to be provided as a pure dietary supplement in order to do so. Further, such enteric supplementation of 2-Ox can increase plasma levels of insulin, growth hormone (GH), and insulin-like growth factor-1(IGF-1). 2-Ox is converted into proline, leucine, and other amino acids in the enterocytes. In addition, it has been demonstrated that 2-Ox is involved in collagen metabolism through a variety of mechanisms and that it counteracts bone loss.14,16
In our previous studies we showed bone loss caused by dexamethasone (Dex), a synthetic GC, administered pre- and postnatally in animal models. We also showed that dietary supplementation with 2-Ox has beneficial effects on growth and performance and that it can prevent bone loss after prenatal Dex treatment.15,17,18 Based on the above knowledge about GCs’ adverse effects in children and on our previous studies, we hypothesize that 2-Ox may have a potential to prevent or at least diminish bone loss after neonatal GCs treatment. Hence, the aim of this study was to elucidate the effect of dietary administered 2-Ox on bone loss caused by neonatal treatment with maximal Dex dose.
Materials and methods
The experiment was approved by The Local Ethics Committee on Animal Experimentation of University of Life Sciences in Lublin, Poland.
Animal breeding and experimental design
Ten clinically healthy multiparous sows (Large Polish White) were mated naturally with the same boar of the same breed and their litters were used in this experiment. All sows showed similar care about their previous offspring. The time of parturition was calculated from the second day of the mating, which lasted three days. Sows were singly housed in separate cages under standard rearing conditions (constant temperature, humidity, and 12/12 h day night cycle) with free access to fresh water and fed twice a day with standard commercial diets for pregnant and lactating sows (2.3 kg/day). All piglets were born naturally, had no congenital infections, and litters contained eight or more piglets. On the day of birth, litters were weighed and sexed before suckling. Female piglets were used in the subsequent study to account for sex differences. Piglets were not separated from mother after farrowing and were held in the same cage, thus were not transferred from one sow to another. During suckling piglets did not receive feed, iron, or other medication. Piglets were randomly divided into three experimental, weight-matched groups (N = 12 in each): the Dex group, in which piglets received intramuscular injections of Dex at the dose of 0.5 mg/kg b.w. daily (Dex pro inj. 0.2%, Eurovet Animal Health B.V., Bladel, The Netherlands); the Dex plus 2-oxoglutaric acid group (Dex+2-Ox), in which piglets received Dex at the same dose, manner, and time, and additionally a solution of 2-oxoglutaric acid at the dose of 0.4 g/kg b.w./day administered orally and the control group, in which piglets received injections with physiological saline at the volume and manner corresponding to Dex-treated groups. Powdered 2-oxoglutaric acid of 99% purity (Protista Biotechnology AB, Lund, Sweden) was mixed with distilled water and buffered by NaOH to a final pH of 7.3. Animals from Dex and control groups also received orally a solution of physiological saline to balance the amount of Na ions in all three groups. The duration of all described treatments lasted from one to 35 day of piglets life and animals were weighed every second day to calculate Dex and 2-Ox doses. At the end of the experiment all piglets were weighed and euthanized by intravenous injections of a lethal dose of pentobarbitalum natrium (Morbital, Biowet, Puławy, Poland).
Bone analysis
Left femora, humeri, and four ribs (sixth and seventh taken from each side) were isolated from all piglets. Once cleaned of remaining soft tissues, the bones were weighed and measured. Each limb bone and ribs was wrapped in gauze, soaked in isotonic saline, and stored at −25℃ for further analysis.
BMD and bone mineral content (BMC) were determined by dual energy X-ray absorptiometry using a Discovery W Hologic X-ray densitometer (Bedford, MA, USA) and APEX 3.0.1 software with Small Animals Studies option for investigation of bones from various types of animals. Densitometer self-calibration was performed before the measurements using Hologic Automatic Internal Reference System. An optional scout scan was available to assist the operator in defining the scan region. The analysis was performed on the scan data using an operator-defined region of interest and numeric results were calculated and displayed. The measurements of BMC and BMD were performed using the following parameters: additional calibration with a phantom provided by the manufacturer, the resolution 0.5 line pairs/mm. The region of interest after the scout scan was defined manually. Measurements were performed for the whole bone samples and for proximal part of the limb bone including both the trabecular and cortical bone compartments, and for the neck of ribs (i.e. the flattened portion which extends laterally from the head, about 2 cm in length).
Volumetric bone density of the femora and humeri was measured by quantitative computed tomography using a GE LightSpeed VCT 64 Slice CT apparatus (GE Healthcare, Pollards Wood, United Kingdom) supplied with LightSpeed VCT Select with 64-channel upgrade 12HW14.6 software (GE Healthcare, Little Chalfont, United Kingdom) in terms of both trabecular and cortical bone by means of 2 mm thick, cross-sectional, metaphyseal and diaphyseal scans. Trabecular bone density (Td) of femur was measured in the distal metaphysis with the scan positioned just below the distal growth plate, proximal to the distal growth plate. Td of humerus was measured in the proximal metaphysis with the scan positioned just below the proximal growth plate. Cortical bone density (Cd) was assessed at 50% of the length of both bones. 19
Mechanical properties of bones were determined after thawing at room temperature using a three-point bending test in INSTRON 4302 apparatus (Instron, Canton, MA, USA). The distance between supports was set at 40% of total bone length and bone samples were loaded with a constant speed of 10 mm/min. The maximum elastic strength (Wy) and the ultimate strength (Wf) of the bones were determined as described previously. 17
Geometry of bones was estimated on the basis of horizontal and vertical diameter measurements of the mid-diaphyseal cross-section of bone. The cross-section area (A), the mean relative wall thickness (MRWT), cortical index (CI), and the second moment of inertia (Ix) were determined.17,20
Histomorphometry
The fragments of femora, humeri, and ribs were subjected to histology as previously described, 21 except sections were cut 4 µm thick. Samples of rectangular shape, 2 mm thick, from the surface of epiphysis to 5 mm below the growth plate of metaphysis, were cut out from each femur (from the central part of the lateral condyle, sagittal section) and each humerus (from the central part of the head, transverse section). Fragments of rib bone from the head of the rib through the neck to a distance of 5 mm past the tubercles were also taken. Eighteen sections from each bone (at 40 µm intervals after each series of three sections) were cut from each individual piglet with a microtome (Microm HM 360, Microm, Walldorf, Germany). Total thickness of section plane was 272 µm for each bone. For histological analysis, the sections were stained with hematoxylin and eosin. Microscopic (two-dimensional) images of fluorescence (10 images magnification ×50 and 25 images magnification ×630) of each slice were taken using a confocal microscope (AXIOVERT 200 M, Carl Zeiss, Jena, Germany) equipped with a color digital camera (AxioCam HRc, Carl Zeiss, Jena, Germany) and a fluorescent lamp (excitation wavelength 450–490 nm). 22 The analysis of collected images was performed using graphic analysis software ImageJ 1.50 a (National Institute of Health USA, http://rsb.info.nih.gov/ij/index.html) equipped with BoneJ, a series of plugins dedicated for bone analysis. The following parameters were analyzed for epiphysis and metaphysis of each bone: the fractal dimension of the trabecular bone, the trabecular bone volume (BV/TV%), mean and maximum trabecular thickness (Tb.Th), mean and maximum trabecular separation (Tb.Sp). Additionally, for the trabecular bone, the number of osseous lacunae per square millimeter of trabeculae, the total area of osseous lacunae per square millimeter of trabeculae, and the mean cross-sectional area of osseous lacunae were assessed as previously described.18,21,23
Blood sample collection and analysis
Blood samples collection and analysis were carried out as described previously.15,24 Briefly, blood of not fasted piglets was collected from subclavian vein. Serum and plasma samples, following blood centrifugation (clotted or total blood, respectively) (20 min at 3000 rpm; Versatile Sigma 2-16P centrifuge, Sigma Laborzentrifugen GmbH, Harz, Germany), were partitioned and stored at −80℃ until further analysis.
Selected hormones serum concentrations were determined using commercially available Enzyme-Linked Immunosorbent kits according to manufacturer’s protocols: GH, OC, and leptin (Diagnostic System Laboratories, Inc., Webster, USA), bone-specific alkaline phosphatase (BAP) (METRA, Quidel Corporation, San Diego, USA), IGF-1 (Uscn Life Science Inc., Wuhan, P. R. China), and cortisol (MyBioSource, Inc., San Diego, USA). The determination of serum hormonal concentrations was performed using Benchmark Plus microplate spectrophotometer supplied with Microplate manager Software Version 5.2.1. (Bio-Rad Laboratories, Inc., Hercules, CA, USA).15,17,24
The plasma concentrations of glycine, glutamine, glutamate, and proline were analyzed using ion-exchange chromatography on an INGOS AAA 400 automatic analyzer (Ingos, Praha, Czech Republic). 25 Serum concentration of calcium, phosphorus, and sodium was determined using energy-dispersive X-ray spectrometry (ED 2000 Spectrometer, Oxford Instruments, Buckinghamshire, UK) in dry matter of the lyophilized samples as described previously. 25 Urea, uric acid, creatinine, albumin, and total protein were determined in the blood serum using kits from Cormay (Warsaw, Poland). 26
Statistical analysis
All results are expressed as mean ± standard deviation. Differences between means were tested with the use of one-way analysis of variance (ANOVA) and a post hoc Tukey’s honest significant difference test as a correction for multiple comparisons. Normal distribution of data was examined using the W. Shapiro–Wilk test and equality of variance was tested by the Brown–Forsythe test. When there was a lack of a normal distribution and/or an unequal variance of data, the Kruskal–Wallis test was used to analyze the differences between means and post hoc tests for mean range for every pair of groups. The two-sided significance level (P value) of less than 0.05 was considered statistically significant. All statistical analyses were carried out by means of STATISTICA (data analysis software system), version 12. StatSoft, Inc. (2014). STATISTICA Power Analysis tool was used to calculate the size of the sample and the statistical power as a function of the error and the type and size of the effect for the one-way ANOVA. High power of statistical tests (86–99%) was reached for assessed parameters. The effect size was calculated and interpreted according to Cohen f according to Kotrlik et al. 27 All presented statistically significant differences had large effect sizes (over 0.56), except for the cross-sectional area of osseous lacunae where medium effect size (0.38) was noticed.
Results
Dex treatment resulted in significant weight loss in both groups receiving Dex (Dex 3300 ± 246 g, Dex + 2-Ox 4612 ± 285 g) compared to the control group 5045 ± 482 g (P < 0.001 and P = 0.013, respectively). However, weight loss was considerably lower in piglets supplemented with 2-Ox compared to the Dex group (P < 0.001).
The mechanical, geometrical, and densitometry properties of selected bones of 35-day-old female piglets treated neonatally with dexamethasone (Dex) or Dex and 2-oxoglutaric acid (2-Ox)
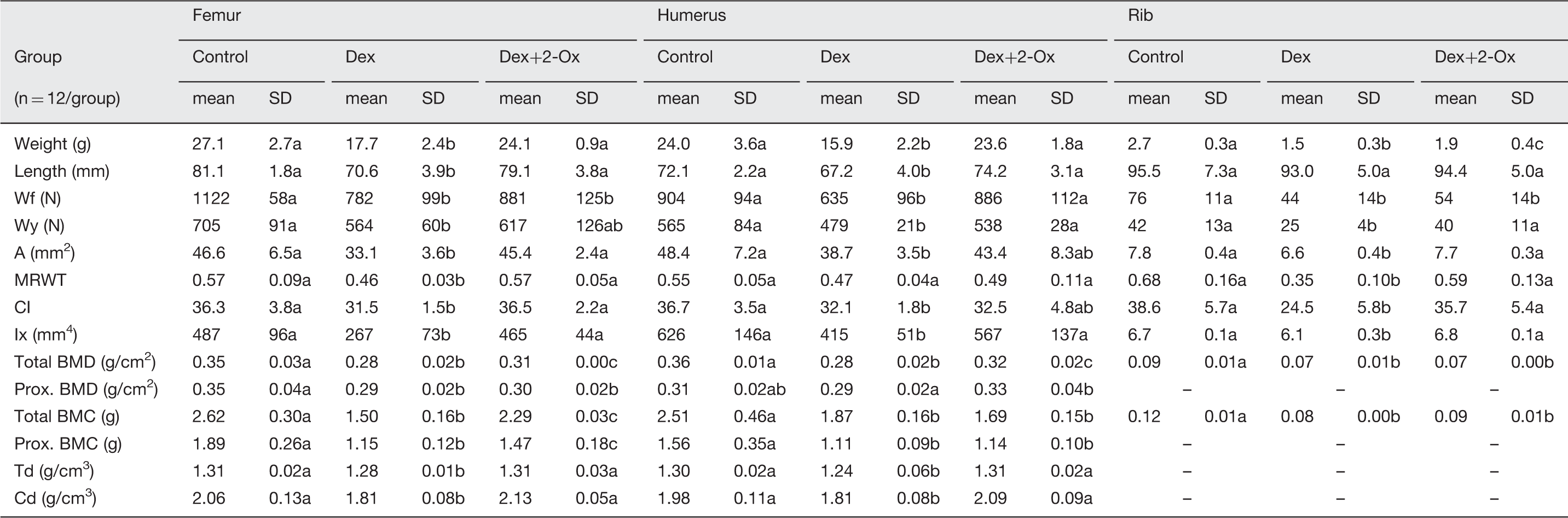
A: cross-sectional area; BMC: bone mineral content; BMD: bone mineral density; Cd: cortical volumetric bone mineral density; CI: cortical index; Ix: second moment of inertia; MRWT: mean relative wall thickness; prox.: proximal; Td: trabecular volumetric bone mineral density; Wf: ultimate strength; Wy: maximal elastic strength.
Data are given as mean and SD. Dex (0.5 mg/kg b.w. daily), 2-Ox (0.4 g/kg b.w. daily). Differences between letters mean significant differences with P < 0.05. Comparisons are made within particular bones.
The histomorphometry properties of selected bones of 35-day-old female piglets treated neonatally with dexamethasone (Dex) or Dex and 2-oxoglutaric acid (2-Ox)
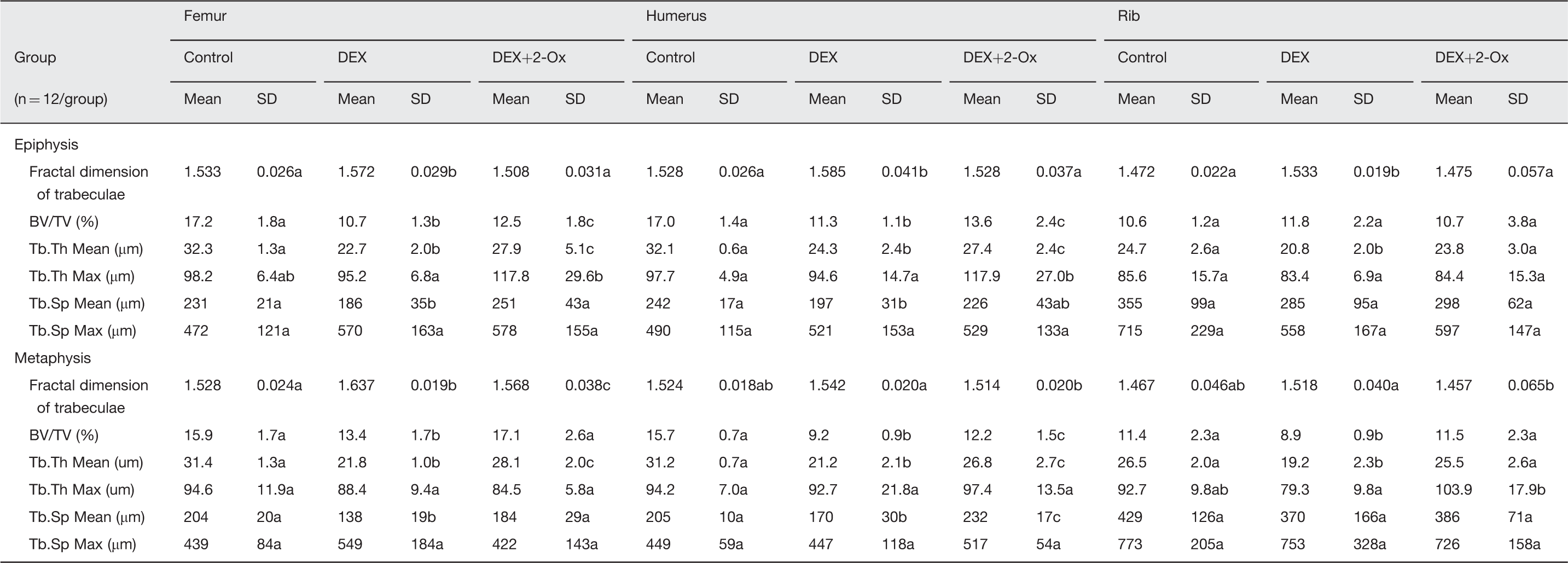
BV/TV: trabecular bone volume; Tb.Th: trabecular thickness; Tb.Sp: trabecular separation.
Data are given as mean and SD. Dex (0.5 mg/kg b.w. daily), 2-Ox (0.4 g/kg b.w. daily). Differences between letters mean significant differences with P < 0.05. Comparisons are made within particular bones.
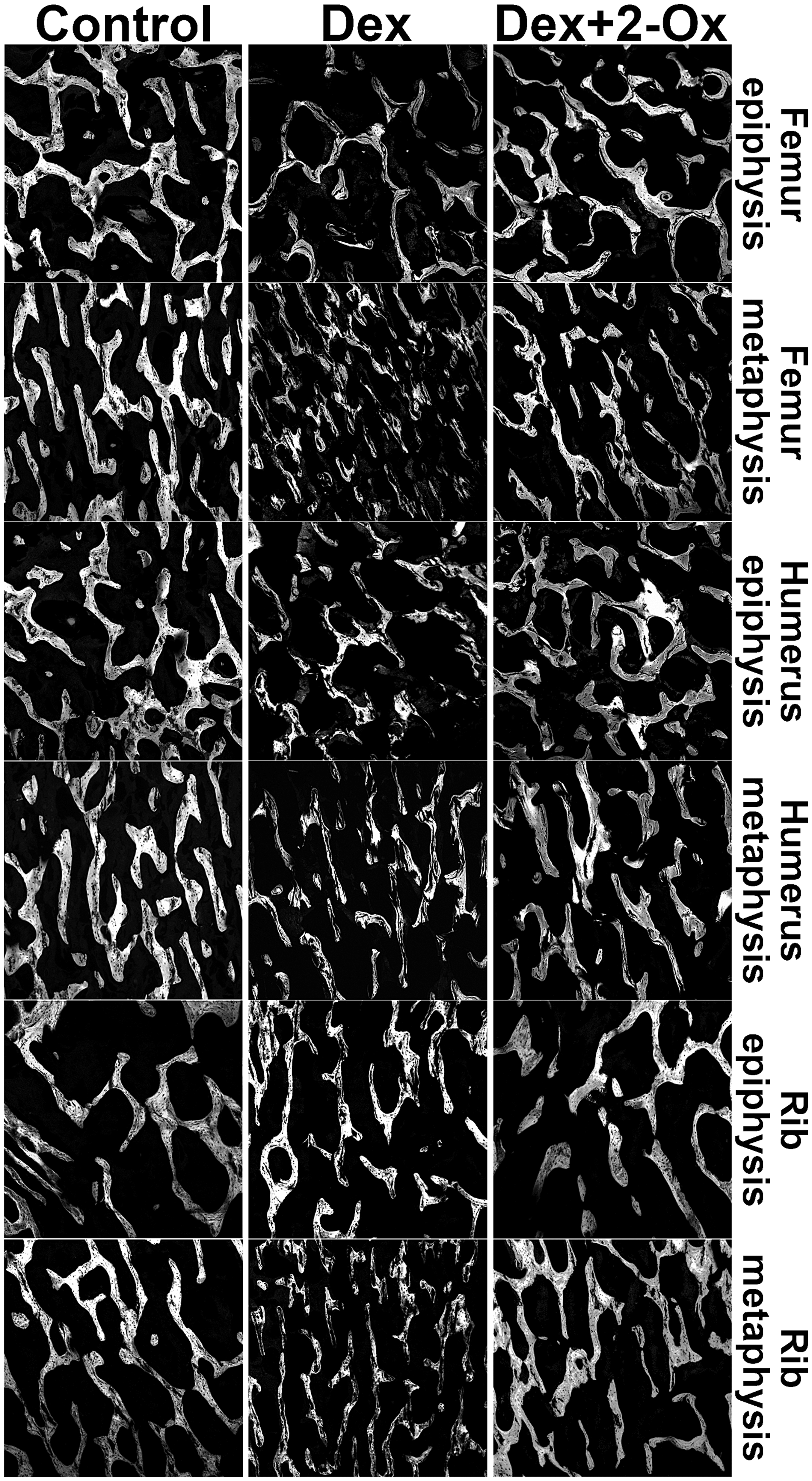
The effect of Dex or Dex with 2-Ox administered neonatally on cancellous bone of female piglets. Gray color—bone trabeculae, black color—bone marrow space. Magnification in all microphotographs is ×50. Dex: dexamethasone; 2-Ox: 2-oxoglutarate
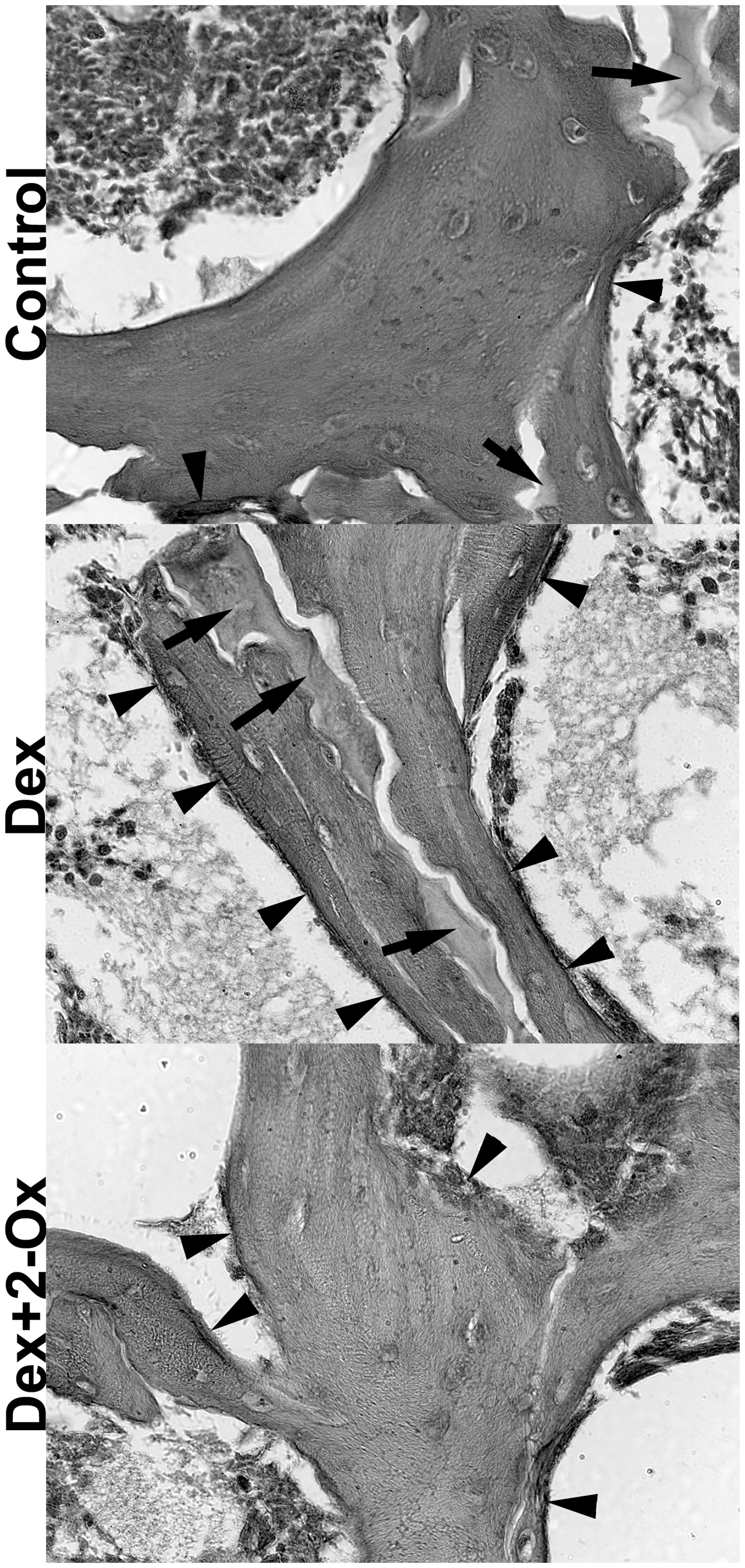
The effect of Dex and Dex with 2-Ox administered neonatally on amount and area of unstructured and acellular bone material as well as structural disturbances observed in trabecular bone. Black arrows indicate areas with unstructured and acellular bone, arrowheads indicate osteoid areas. Magnification in all microphotographs is ×630. Dex: dexamethasone; 2-Ox: 2-oxoglutarate
The serum levels of bone markers, selected hormones, nitrogen metabolites, and proteins of 35-day-old female piglets treated neonatally with dexamethasone (Dex) or Dex and 2-oxoglutaric acid (2-Ox)
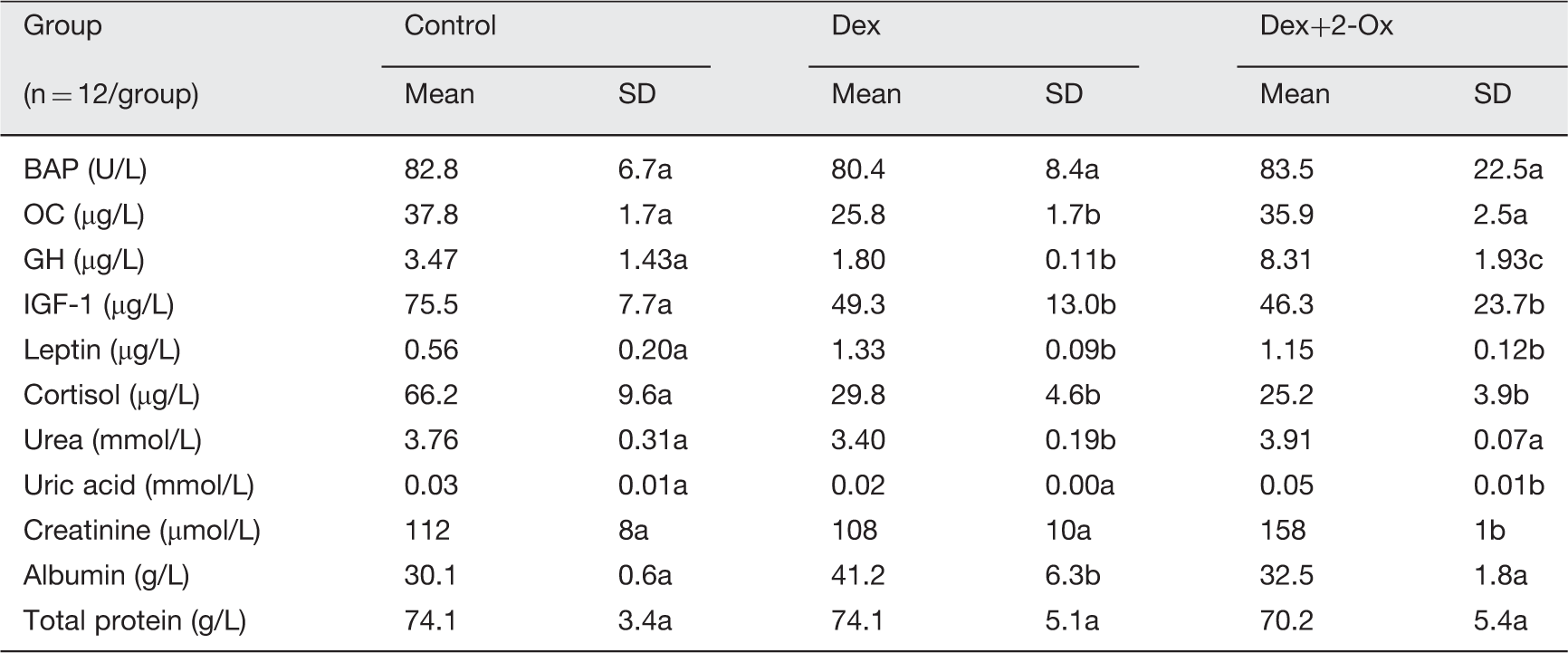
BAP: bone alkaline phosphatase; GH: growth hormone; IGF-1: insulin like growth factor 1; OC: osteocalcin; 2-Ox: 2-oxoglutarate.
Data are given as mean and SD. Dex (0.5 mg/kg b.w. daily), 2-Ox (0.4 g/kg b.w. daily). Differences between letters mean significant differences with P < 0.05.
The plasma concentration of glycine, glutamine, and glutamate was significantly elevated in the Dex group (709 ± 24, 299 ± 28, 180 ± 15 µmol/L, respectively) compared to the control (498 ± 38, 171 ± 33, 91 ± 33 µmol/L, respectively) P < 0.001. Conversely, proline level decreased after exclusive Dex treatment (540 ± 41 µmol/L) compared to the control (614 ± 10 µmol/L) P = 0.001. Supplementation with 2-Ox had, to some extent, a protective effect, since glycine, glutamine, and glutamate concentrations decreased (632 ± 38, 248 ± 28, and 133 ± 31 µmol/L, respectively) and proline increased (624 ± 36 µmol/L) relating to the Dex group (P = 0.001, P < 0.001, P = 0.013, and P < 0.001, respectively).
The serum concentration of calcium, phosphorus, and sodium did not differ between control, Dex, and Dex + 2-Ox groups (Ca: 1234 ± 130, 1245 ± 86, and 1222 ±152 ppm; P: 2897 ± 243, 2737 ± 263, and 2566 ± 298 ppm; Na: 4.6 ± 0.4, 4.0 ± 0.6, and 4.3 ± 0.9%, respectively).
Discussion
In the present study neonatal administration of Dex alone led to osteoporosis that was demonstrated in geometry, durability, density, mineralization, histology, and histomorphometry of bones examined (Tables 1 and 2 and Figure 1). These findings were in accordance with variety of earlier studies on rats, mice, and piglets treated pre-, neo-, or postnatally with GCs.15,17,24,25,28–31 The clinically relevant maximal dose of Dex used impaired bone growth, which was evident in shorter long bones in the Dex group. Such growth impairment was also found in previous studies on animals and reviewed in children’s clinical trials.4,31–33 For example, mice and rats treated with Dex had femur growth reduced by 47 and 31%, respectively, so much more than in the present experiment. Four and two times higher doses were however used (for mice and rats, respectively) in these referred studies.31,32 Nevertheless, other studies show that GC-induced bone quality aggravation is partly reversible. 3 Indeed, impairment caused by Dex in piglets’ long bones was prevented by 2-Ox dietary supplementation and vast majority of assessed bone parameters were restored almost to the control level, as presented in Tables 1 and 2. Also, according to the best of our knowledge, this is the first study utilizing 2-Ox to prevent osteopenia induced by neonatal administration of GCs. Moreover, dietary 2-Ox appears to be even more effective in preserving bone structure and mineralization in GCs induced rather than in gastrectomy-induced osteopenia, since there was no improvement in femoral and tibial BMD and BMC of gastrectomized rats receiving even higher dose of 2-Ox in our previous study. 21
The ability to withstand the mechanical forces acting upon a bone and to resist fractures is related to its geometry, mineralization, and quality of structural components such as shape, microarchitecture of trabecular bone, the turnover, collagen and cells regularly spaced throughout the mineralized matrix.19,28 There are several possible mechanisms of GIO presented in literature: inhibition of bone formation by suppression of genesis and activity of osteoblasts with accelerated osteocyte and osteoblasts apoptosis as well as acceleration of bone resorption by extension of osteoclasts life span. Furthermore, GCs interrupt regulatory proteins ratio by stimulating osteoclastogenesis-inducing RANKL and inhibiting antiresorptive osteoprotegerin.1,4,9,28,30,34 Such cellular imbalance contributes to disruption of the osteocyte signaling network, which is responsible for damage detection and repair initiation, leading to microdamage accumulation and further increased bone fragility. This leads to higher frequency of fractures and at higher BMD values than in patients with osteoporosis not induced by GCs.4,28
A rapid bone loss (mostly trabecular mass), loss of BMD, and bone strength/quality after the initiation of GCs therapy is likely to be associated with the loss of structural integrity as well as loss of osteoblast-generated proteins such as collagen or OC referred to as microarchitectural deterioration.1,3,4 Although OC level was decreased in the Dex group, our results do not differentiate between cell types and cannot directly confirm cellular proportion/imbalance. However, we have noticed microstructural and architectural bone deterioration reflecting in significant enlargement of trabecular fractal dimension in the Dex group which implies impaired, irregular surface structure and the complexity/integrity of trabecular bone. Thus, not only did we show the reduced trabecular bone volume, thinner trabeculae, less mineralized bone, but also cracked trabeculae and impaired trabecular microstructure. Furthermore, GCs can modify osteocyte microenvironment by causing changes in bone material, including an enlargement of their lacunar space and generation of areas with hypomineralized bone. 35 Suchlike expansion of osseous lacunae and its total area as well as more osteoid were also observed in the present study in piglets from the Dex group.
On the other hand, animals supplemented with 2-Ox had preserved microarchitecture of trabecular bone, since trabecular thickness, amount of osteoid, lacunar cross-sectional area, and trabecular fractal dimension were very similar to the control. This observed effect of glutamine precursor presumably involves mechanisms related to stimulation of bone anabolism, since 2-Ox acts as an energy donor and as a substrate for the synthesis of amino acids—principally proline—leading to increased collagen synthesis and formation in the cell and organism. Several mechanisms by which 2-Ox is involved in collagen metabolism were distinguished beginning from being a cofactor of prolyl-4-hydroxylaze which catalyze 4-hydroxyproline, crucial for the formation of collagen triple helix, through facilitate collagen synthesis by increasing the pool of proline residues via glutamate, and finally by being also a precursor of pyrroline-5-carboxylate an intermediate in the interconversion of proline.14,16 Moreover, enteral 2-Ox administration may cause an anabolic effect on bone tissue metabolism via glutamate innervation as well as significantly increased plasma level of GH and IGF-1 as reviewed previously.14,16,19 In addition, 2-Ox affects bone tissue probably also by its effect on the endocrine system by conversion to glutamine and glutamate followed by transformation into ornithine and then arginine. Both ornithine and arginine stimulate secretion of GH and IGF-1, thus well-described functional axis GH-IGF-1 with strong osteotropic effect. 14 Such stimulation of growth was observed in our study by highest GH level in the Dex+2-Ox group, which might have a direct effect on osteoblasts reflected in higher OC concentration than in the Dex group. This observation highlights the effect of 2-oxoglutarate, especially since OC is known to be negatively regulated by GCs. 30 Conversely, Dex alone decreased GH secretion which was consistent with previous review. 6 And again, although our results do not distinguish cell types, the elevated OC level in the Dex+2-Ox group may suggest at least increase in osteoblast metabolism, if not increase in osteoblast number. Conversely, while IGF-1 was reported to be negatively correlated with bone resorption, treatment with 2-Ox in first 14 days of postnatal life had no significant effect on plasma IGF-1 concentration in growing lambs. 19 Our results confirm these findings since we showed no effect of 2-Ox on IGF-1 concentration, lowered by Dex. It seems that even if enteral 2-Ox treatment early in postnatal development can have a long lasting effect on bone structure, these changes are probably independent of the plasma concentration of IGF-1, and not only in growing lambs.14,19 Moreover, since all animals receiving Dex had decreased plasma IGF-1, a potent inhibitor of programmed cell death, we assumed that GC-induced structural changes might have been related to the increased apoptosis as observed previously. 32
GCs accelerate bone resorption by extension of osteoclasts life span and stimulation of osteoclastogenesis. 4 Further, osteoclast activation can be promoted by hypoxia-inducible factor 1 (HIF-1α) stabilization followed by increased bone resorption and decreased bone mass. Whereas, 2-Ox is known inhibitor of HIF-1α, and by such properties and inhibitors of HIF-1α can protect from osteoclast activation and bone loss. Hence there is another possible mechanism of positive effects of 2-Ox on bone tissue maintenance.14,36,37
Changes in bone remodeling, e.g. increased trabecular surface remodeling are responsible for altered trabecular bone volume and architecture, which may further influence fracture risk and further confirm, however indirectly, prevalence of cellular regulation by GCs. 35 Structural changes caused by GCs in the trabecular fractal dimension were completely different from these observed in gastrectomy-evoked osteopenia in our previous study. 21 Gastrectomized rats had lower trabecular fractal dimension than control animals, suggesting greater reduction in the amount of extracellular matrix rather than in its quality, since BV/TV and BMD and BMC decreased as well. 21 Although piglets receiving Dex alone also had reduced bone volume and mineralization, the mechanism behind this present observation is most probably different from the lack of gastric factor promoting trabecular bone formation and calcium absorption and its transport from blood to bone, as postulated for gastrectomy.21,22 Nevertheless, supplementation with 2-Ox in both these cases revealed stimulating effect on bone structure. In this regard, dietary 2-Ox may maintain bone structure regardless of mechanism of action of damaging agent, probably by being involved in regulatory mechanism of nutrients utilization. 2-Ox may act by improving protein anabolism and absorption from the gut, namely by stimulating the gut mucosa to synthetizing proline, the main amino acid required for bone collagen synthesis.14,16 Moreover, proline concentration in the Dex+2-Ox group was indeed significantly higher than in animals receiving only Dex. On the other hand, the excess of GCs showed catabolic effect revealed by elevated glutamine, glutamate, and glycine levels in animals receiving Dex. This might have been related to increased proteolysis in skeletal muscle as assumed previously.3,29 Nevertheless, what is substantial is that this effect was also largely abolished by supplementation with 2-Ox.
Chronic GCs therapy is related also to reduced intestinal calcium absorption and promotion of renal calcium excretion, resulting further in an increase in PTH secretion, which may promote bone resorption.1,34 However, no differences in serum calcium or phosphorus levels were noticed in the present study which leads us to the strengthening of previously presented mechanism related rather to the GC-induced bone remodeling by alterations in bone cells viability. 35 Moreover, particular life period and length of Dex treatment may also be important factors, and there were several studies regarding long period of GCs treatment and its outcomes.1,2,4,6,8,11,13 The duration of the presented experiment, 35 days, was imposed by the moment of natural weaning of piglets, a point until when continuous and uninterrupted growth occurs. We have chosen this particular time in order to avoid the changes in digestive system caused by weaning which affects both nutrient absorption and skeleton.
The main problem associated with the GCs treatment is that they act simultaneously on various organs and systems, e.g. immune system, metabolic organs, and bone. Concomitantly, GCs affect the levels of other hormones by negative-feedback loops influencing the hypothalamic–pituitary–adrenal axis. 38 In the present study, the Dex treatment, regardless of 2-Ox supplementation, resulted in decreased level of cortisol and increased leptin, similarly as described previously.5,25,30,38 Therefore, there are two main ways to prevent GCs’ side effect: the use of weaker GCs and lowering the most effective dose of systemic steroids, or the implementation of combined therapies to ameliorate GC-induced adverse effects. 7 However, although weaker GCs are less harmful, they are also less effective in promoting beneficial effects. 7 The second approach, regarding combined therapies, involve vitamins C, E, K, and D as well as bisphosphonates.1,3,4,7,34,39 Nonetheless, bisphosphonates themselves have many adverse effects and raise safety concerns related to reproduction and gastrointestinal side effects. Moreover, although vitamin D derivatives as well as vitamin K can be considered suitable treatment options, it still lacks Food and Drug Administration approval, since hypercalcemia and hypercalciuria are well-known unwanted effects of vitamin D derivatives. 1 Nevertheless, there are also glutamine derivatives widely described in the context of bone health which have beneficial influence on the whole organism, e.g. 2-oxoglutaric acid.14,16,18,19,21,22 Moreover, recently described antioxidative action of 2-Ox strengthens the possible use of this natural glutamine derivative in ameliorating of the GC-induced side effects in the skeleton.7,14,40
In conclusion, the present study has showed, for the first time, that dietary 2-Ox administered postnatally has a potential to improve/maintain bone structure of animals simultaneously treated with maximal therapeutic doses of Dex which, in our opinion, may open a new direction in developing combined treatment for children treated with GCs. Moreover, present findings also support our previous thesis on the regulatory mechanism of nutrient utilization regulated by glutamine derivatives.18,22 Presumably, 2-Ox may take part in the specific mechanism of metabolic regulation activated in a state of health problems by utilization of proteins and amino acids depending on the stage of development in which the organism is to facilitate better use of nutrients. Also the mechanism of action of 2-Ox on the functional axis GH-IGF-1 and its osteotropic effect needs further studies.
Footnotes
Author’s contributions
All authors participated in acquisition, analysis, and interpretation of the data; final approval of the article; provision of study materials; administrative, technical, or logistic support; PD—conception and design, collection and assembly of data, statistical expertise, drafting of the article; PD, ET, SGP—critical revision of the article for important intellectual content.
Acknowledgement
This research received no specific grant from any funding agency in the public, commercial, or non-profit sectors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.