
Abstract
Our hypothesis was to investigate the fatty acid potential as a bone induction factor. In vitro and in vivo studies were performed to evaluate this approach. Oleic acid was used in a 0.5 wt.% concentration. Polycaprolactone was used as the polymeric matrix by combining solvent-casting and particulate-leaching techniques, with a final porosity of 70 wt.%, investigated by SEM images. Contact angle measurements were produced to investigate the influence of oleic acid on polycaprolactone chains. Cell culture was performed using adipocyte-derived stem cells to evaluate biocompatibility and bioactivity properties. In addition, in vivo studies were performed to evaluate the induction potential of oleic acid addition. Adipocyte-derived stem cells were used to provide differentiation after 21 days of culture. Likewise, information were obtained with in vivo data and cellular invagination was observed on both scaffolds (polycaprolactone and polycaprolactone /oleic acid); interestingly, the scaffold with oleic acid addition demonstrated that cellular migrations are not related to the surrounding tissue, indicating bioactive potential. Our hypothesis is that fatty acid may be used as a potential induction factor for bone tissue engineering. The study’s findings indicate oleic acid as a possible agent for bone induction, according to data on cell differentiation, proliferation, and migration.
Impact statement
The biomaterial combined in this study on bone regeneration is innovative and shows promising results in the treatment of bone lesions. Polycaprolactone (PCL) and oleic acid have been studied separately. In this research, we combined biomaterials to assess the stimulus and the speed of bone healing.
Introduction
The advance of scaffolds for tissue engineering brings an extensive investigation on materials to act as inductors. Bioactive materials, such as ceramics, glasses, and phosphates have been explored due to their contribution to the osteogenic activity. Likewise, soluble factors, such as ascorbic acid and dexamethasone are known to regulate cell differentiation. 1 Proteins present in the extracellular matrix (ECM) and cell membrane also have an important role in active biochemical signaling network. 2
Oleic acid is a unsaturated fatty acid that it is biocompatible, which can be found in abundance in blood plasma and non-human sources. 3 Currently, this molecule has proved itself effective on stem cell modulation, since it causes mesenchymal stem cell secretion of angiogenic mediators and regulates immunomodulatory functions 4 ; moreover, it improves skin wound healing, due to the increase in ephrin receptors that affects cell migration and adhesion during wound healing. 5
The use of oleic acid as surfactant has been successfully demonstrated in the literature; however, how it could induce bone fracture healing remains unknown. Thus, to test the hypothesis that fatty acid is a bone induction factor, PCL/OA scaffolds were fabricated using combined techniques: solvent casting and particulate leaching. Samples were characterized using scanning electron microscopy (SEM) and contact angle measurement. In vitro and in vivo studies were done to investigate the influence of biocompatibility and bioactivity.
Materials and methods
Poly (ɛ-caprolactone) (PCL, Mw = 80,000) and sodium chloride (NaCl) were purchased from Sigma Aldrich, chloroform from Merck and oleic acid from Synth. The polymeric matrix was produced using a concentration of 12.5 w/v%, with 70 wt.% of NaCl with particle diameters ranging from 177 to 350 µm as the porogenic agent. Oleic acid was added in 0.5 wt.% concentration. The technique used to produce the scaffold was salt-leaching; after casting, it was proceeded with 48 h for solvent evaporation, followed by 48 h of salt-leaching in deionized water.
Characterization
Surface morphology was imaged by SEM with Jeol JXA 840, samples sputter-coated with gold (Bal-tec SCD 050) with conditions of 40 Ma,5 × 107 for 200 s. The static contact angle (θ) was measured with a KSV-CAM 200 goniometer (KSV Instruments) equipped with an auto dispenser, video camera, and drop-shape analysis software. The static measurements were acquired from a 5 µL sessile water droplet at 15 and 120 s (short and longtime responses), following deposition. Values reported are an average of three measurements carried out on different areas of the same composition: PCL and PCL/OA
Cell culture
Human adipose tissue (ADSC) was collected from healthy donors (aged 25–50) undergoing liposuction, after informed consent and approval by CEP/FCM/UNICAMP number 838/2008. ADSCs were obtained by digestion procedure performed with type 1 A collagenase (Gibco). The cells were then harvested and expanded in growth media Dulbeco's Modified Eagle's Medium low Glicose (DMEM-LG) supplemented with 10% fetal bovine serum (FBS). The ADSCs within three to five passages were grown to at least 80% confluence before being cultured in the induction medium. To induce osteogenic differentiation, 105 ADSCs were cultured for three weeks (21 days) in scaffold PCL and PCL/OA samples on DMEM(Gibco) supplemented with 10% FBS, 0.1 µM dexamethasone(Sigma), 50 µM ascorbate-2-phosphate, 10 mM beta-glycerolphosphate and kept in incubator with 5% CO2 at 37℃; the media was changed every two days. PCL and PCL/OA samples were sterilized by multiple 70% ethanol wash and then washed in medium. Mineralization of the ECM was visualized by staining with Alizarin Red. The protocol of quantitative assay of Alizarin red was described by Gregory et al. The absorbance was measured using µQuant equipment (BioTek Instruments, Inc.) with a filter of 405 nm. Images were captured at 0, 14, and 21 days of culture, and UV-vis measurement was likewise produced. Cell morphology on scaffold surface was evaluated after 4, 7, 14, and 21 days of culture using field emission SEM (Jeol- JXA 840 A) and fluorescence images were produced to observe the cellular penetration on the porous with four days of cell culture.
In vivo
Eighteen male Wistar rats (Rattus norvegicus), four months old and weighing approximately 380 g were used under the approval of the Ethics Committee of the School of Medicine of Jundiaí (Protocol 276/13). The animals were divided into three groups of six animals each. A bone defect was created in the left tibia and either left without any graft (Group 1), a PCL scaffold (Group 2) or a PCL/CHDA whiskers scaffold (Group 3). Animals were anesthetized with intramuscular injection of ketamine hydrochloride and xylazine hydrochloride at a proportion of 1:1 (0.10 mg/100 g body weight). After anesthesia and sterilization of the surgical field, a skin incision was made in the anterior region of the left limb in order to expose the anterior and proximal surface of the left tibia. A bone defect was drilled in the left tibia with a 3.0 mm trephine drill coupled to the pen of a mini-motor until the medullary canal was reached. 6 Grafts (3 × 2 mm) were inserted in the defect, followed by skin and musculature repositioning and sutured. The animals were sacrificed 32 days after bone defect creation with anesthetic overdose, followed by CO2 inhalation. The left tibiae were removed for morphological analysis of bone healing in the wound area. The samples were radiographed with a Rigaku RU-200 apparatus using a focal spot size of 0.8 × 0.8 mm and Kodak films (7.6 × 5.7 cm). Samples were also submitted to histological processing and semi-serial 5-mm cross-sections were cut and stained with hematoxylin-eosin and masson’s trichrome. The formed bone at the implant site was quantified using the following formula: Vv = Pp/Pt(%), where Vv is the volume density or relative density; Pp is the number of points (line intersection) on newly formed bone; and Pt is the total number of points of the system. 7
Statistical analyses
Statistical analyses were conducted using in vitro and in vivo data. The results are expressed as mean ± SD. Comparisons between groups were made using ANOVA, followed by Tukey’s correction factor for multiple comparisons as a posthoc.
Results
Figure 1 reports the SEM micrographs of the PCL/OA scaffold and contact angle data. Sample dimensions were 3 × 2 mm for the in vivo studies; high porosity was obtained using the solvent-casting and particulate-leaching techniques, whose porogenic agent was NaCl at a range of 177–350 µm in diameter. As seen in Figure 1(a), SEM images demonstrate the porous interconnectivity and small porous, due to solvent evaporation – with 10 µm. Figure 1(b) reports the contact angle data; both compositions are hydrophobic because of the polymeric matrix, 104.6 ± 3.5° and 97.3 ± 1.3°, PCL and PCL/OA, respectively.
PCL and PCL/OA scaffolds (a) Macroscopic sample picture, on details surface porosity of PCL/OA composition scale bar 500 and 250 µm; (b) Contact angle values 104.6 ± 3.5° and 97.3 ± 1.3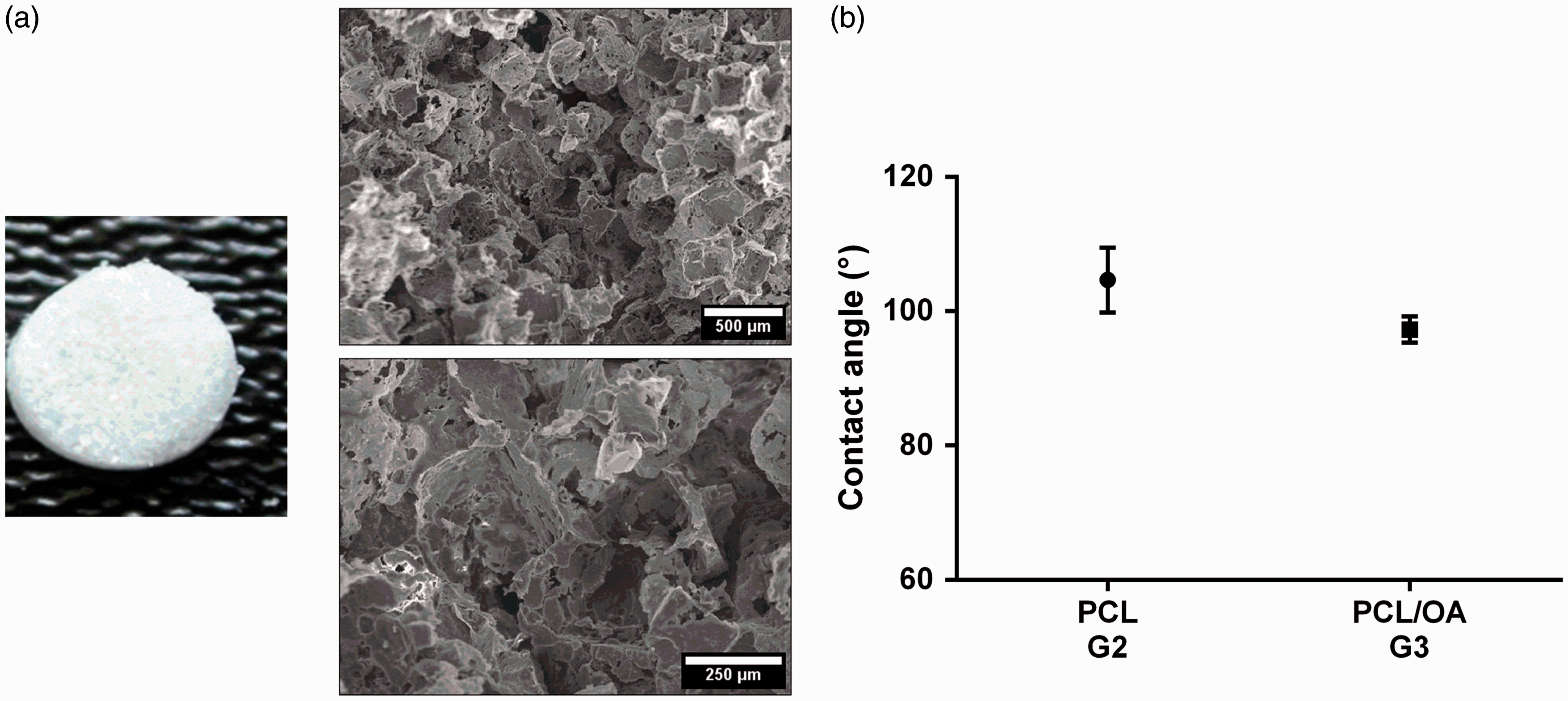
° PCL and PCL/OA, respectively
Figure 2 shows the cell culture data, using ADSC cell line. ADSC tests were produced to investigate the behavior at bone healing process; all data are represented in Figure 2(a) to (c). ADSC morphology was observed with SEM images, the observation on a different period leads to an alteration of the morphology, indicating a possible cell differentiation. Fluorescence microscopy was used to observe cells inside the porous of the scaffold, indicating the correct range for cell migration. Alizarin Red-S staining was performed on samples with a long culture period of 14 and 21 days, which can provide osteogenic data. Indeed, both samples presented levels of calcium detected by UV-vis. Interestingly, the OA addition leads to higher values of 0.37 ± 0.053 and 0.72 ± 0.091, 14 and 21 days of culture, when compared with PCL data (0.167 ± 0.081 and 0.378 ± 0.051, 14, and 21 days of culture).
Cell culture data (a–c) ADSC cell culture during 4, 7, 14 and 21 days (a) SEM images of samples surface cultured with ADSC at different culture period (100 µm scale bar); (b) Scaffold PCL/OA-G3 was observed with bright field and fluorescence microscopy with 4 × and 10 × (500 µm and 100 µm, respectively); (c) Alizarin Red-S staining for calcium mineralization in ADSC on PCL-G2 and PCL/OA-G3 samples after 14 and 21 days of culture qualitative and quantitative data, bright field images 6 mm samples (scale bar 1 mm). (*P > 0.001, ***P > 0.05). (A color version of this figure is available in the online journal.)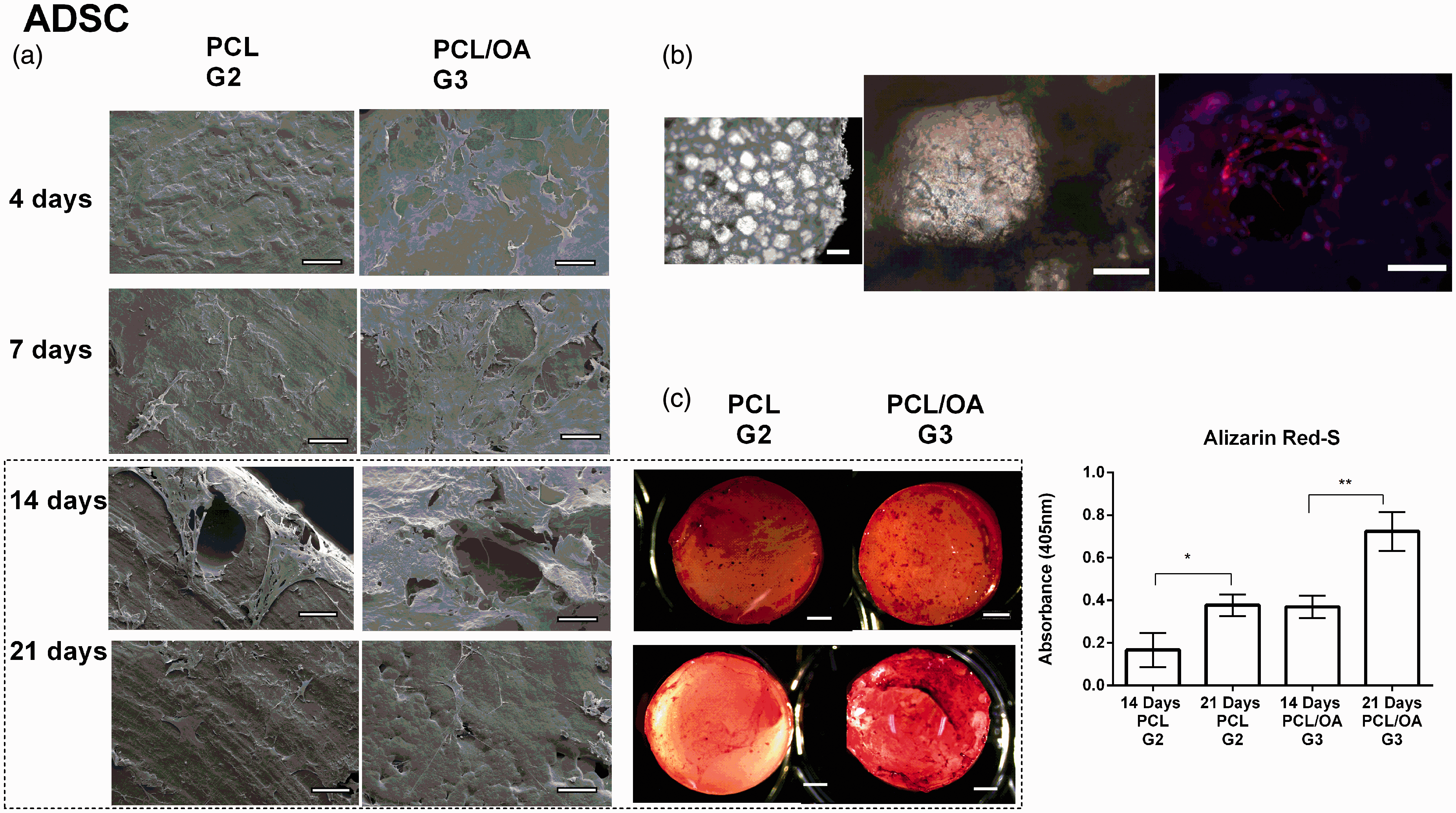
Figure 3 demonstrates the histological data on G1-G3 defects. G1 had low new bone formation compared with biomaterials groups, and the neo-bone was thin and disperse with discontinuous structure, due to the infiltration of connective tissue. In opposition, G2 and G3 had thicker neo-bone with higher concentration of trabecular structures on areas near the border and thinner on the defective center. The medullary channel was repaired and presented healthy hematopoietic tissue. Quantitative data indicate the statistical difference between control and biomaterials groups, likewise among biomaterials groups. The volume of neo-bone was decreasing G3(PCL/OA)> G2(PCL)> G1 (control), 56.24 ± 3.0%, 48.59 ± 0.3%, and 33.15 ± 1.8, respectively.
In vivo regenerated control (G1), PCL (G2), and PCL/OA (G3) arrangement after 32 days (a, b) histological data with 4–10 × magnification (500 and 250 µm scale bar, respectively), (c) 20 × magnification (100 µm scale bar) and (d) volume of neo-bone 5. *** Indicates statistically differences from control and groups and *indicates differences from G2 with G3, P < 0.05. Arrow indicates neo bone with invagination; O: original bone; ON: new bone; TC: conjunctive tissue; M: material. (A color version of this figure is available in the online journal.)
To evaluate the formation of bone tissue, collagen was located by Picrosirius Red staining in the healing areas, as shown in Figure 4. Under cross-polarized light it is possible to visualize collagen fibers as yellow-red and green/blue, suggesting that the fibers may be characterized by collagen type I and III, respectively. Overall, Picrosirius Red analysis demonstrates compatible data with histological findings; G3 had higher Collagen formation than G2 and G1.
In vivo regenerated control (G1), PCL (G2) and PCL/OA (G3) arrangement after 32 days (a) histological view- H&E staining; (b) Picrosirius Red staining. Scale bar 500 µm*, collagen fibers; O: original bone; ON: new bone. (A color version of this figure is available in the online journal.)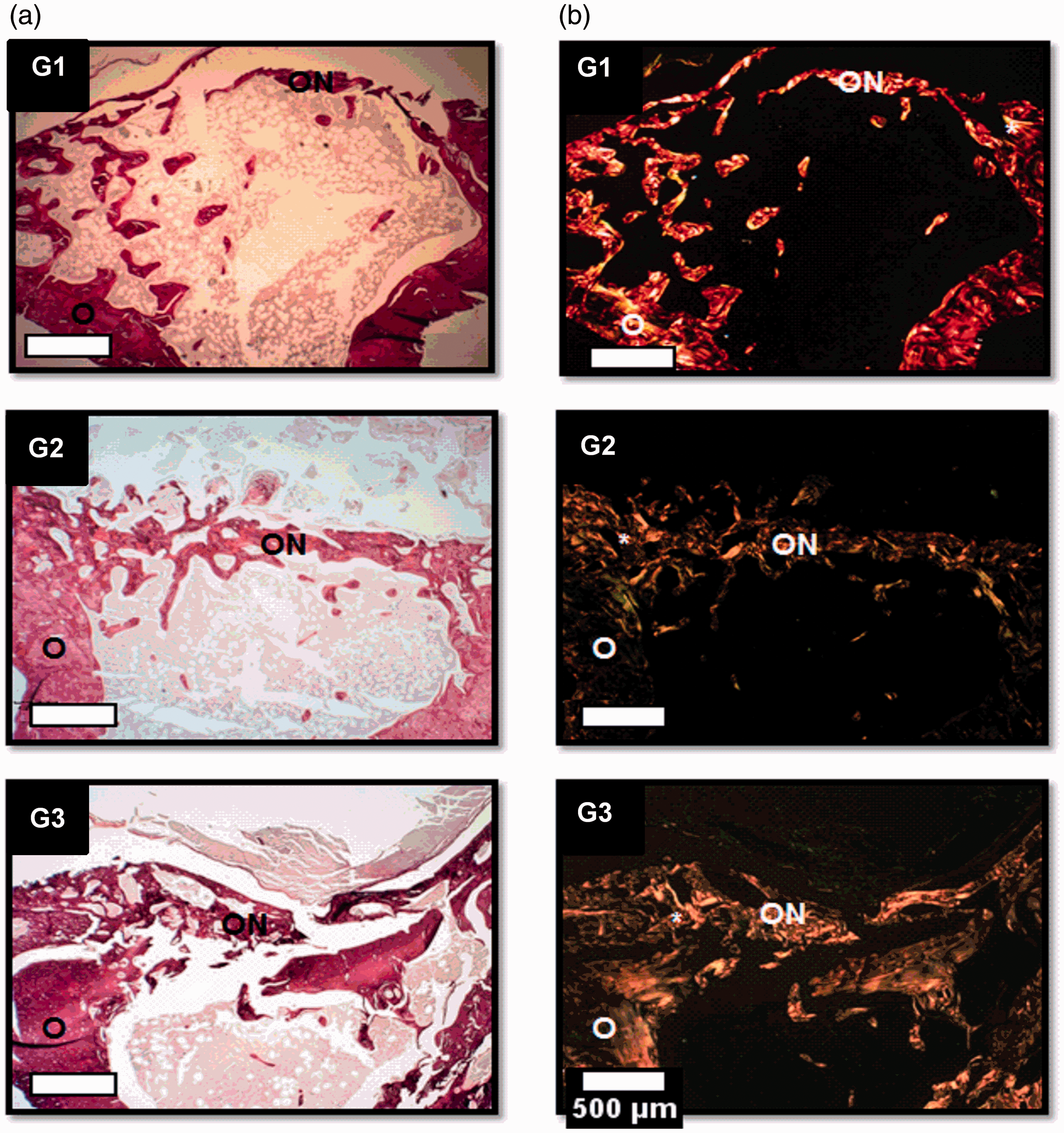
Discussion
Oleic acid is a fatty acid that is often used as dispersion agent for nano/micro particle systems. The chemical structure allows interaction between hydrophilic and hydrophobic elements, e.g. a homogeneous dispersion of hydroxyapatite with polycaprolactone (PCL) matrix.8,9 The use of this biomolecule also plays a role on cellular structures. Present in the human plasma, oleic acid is an important source of energy and is important for cell membrane assembly; indeed, it influences stem cell secretion of angiogenic mediators that regulates immunomodulatory functions.10,11
New approaches have been tested using OA to modulate the immune response in different tissues, since it is known that this biomolecule can affect gene expression on pro and anti-inflammatory mediators. 9
Polyunsaturated fatty acids are primary elements on lipoic mediators of inflammation reaction. Interleukin-17 (IL-17) is an inflammatory cytokine that has pleiotropic biological activity on various types of cells, including immune cell population and chondrocytes.12–14 Recently, the influence of linoleic and oleic acid in IL-17 cytokine release during healing process was investigated, which was shown to be increased followed by increased collagen III expression in the final inflammation phase, suggesting that the use of oleic acid on wound lesion may have accelerated the healing process. 15 Different approach was carried out by Kokubu et al., 12 which demonstrated the multistep cascade of cytokines and morphogens during bone healing, including the participation of the IL-17 family.
Although the influence of OA during wound healing has been described, the influence of this fatty acid on bone healing has not been fully elucidated. Thus, our hypothesis was to evaluate, in vitro and in vivo, the potential therapeutic effect of OA on bone healing response.
PCL has been extensively used as a polymeric matrix in bone tissue engineering due to its biodegradability, biocompatibility, and compressive mechanical properties. 16 The addition of OA on the polymeric matrix did not alter the morphology of the scaffolds, as shown in Figure 1.
Successful scaffolds were fabricated using casting and salt-leaching methods reaching 70% of porosity and the cell migration ability has been proved in previous studies. 17 Likewise, previous data indicated OA as a biocompatible material as a bone tissue engineering agent and primary tests used the U20S cell to provide information about the toxicity and cell spreading on samples with OA addition. Indeed, a similar average cell spreading was noted: 2.17 ± 0.66, 1.82 ± 0.37, 2.56 ± 0.75 and 1.70 ± 0.39, PCL and PCL/OA at one and three days of culture, respectively. 8
In this study, ADSC demonstrated the ability to be cultured in vitro on PCL and PCL/OA scaffolds for extensive periods of 21 days. Data indicate high cellular viability, with detection of calcium by Alizarin Red-S staining. At a porosity of 70%, scanning electronic and fluorescence images elucidated the interconnected porous structures, which can enhance the nutrition and waste diffusion, which are important for the metabolism, proliferation, and osteogenic differentiation of ADSC. 18 For the ADSC differentiation, major phases are known: proliferation, extra-cellular matrix deposition and maturations, and mineralization. 19 Using the staining Alizarin Red-S, it was possible to detect the mineralization phase; calcium was secreted by cells indicating the ADSC differentiation to osteogenic lineage. Findings differ between PCL and PCL/OA data, indicating the potential of OA as a bone induction agent.
According to in vitro results, toxicity in vivo was not observed in all compositions. The integrity of the borders was shown in the histological data; likewise the absence of chronic inflammation phenomena, non-deformities or secondary fractures was also shown. Samples without biomaterial (G1) on critical-defect demonstrated tissue grown from the border to the center, neo-bone was characterized by a thin and non-continuous structure, due to the presence of conjunctive tissue, and a low number of young bone trabeculae was also detected. Samples with biomaterials addition (G2–G3) on defects demonstrated better cell migration than controls. The use of scaffolds has been investigated in multiple tissues and it is well known the benefices of using a biomimetic material in the tissue allow better cell migration and penetration.20,21 Therefore, samples with PCL and PCL/OA had neo-bone structure in all the defect area, with higher volume on areas near the surrounding tissue.Indeed, due to the degradation rate of PCL, around one to two years, tissue invagination inside the porous structures was observed in both groups . OA composition, beside the scaffold structure, also contends OA biomolecules on the surfaces, which induced a better adhesion, proliferation, and migration demonstrated by histological findings. Moreover, it was possible to detect islands of neo-bone not connected with the surrounding tissue, a result of OA induction potential. The detection of collagen fibers was proportional to the neo-bone volume, confirmed by histological data quantification.
Conclusion
Based on our findings, it can be concluded that oleic acid presents as a potential source of osteogenic induction agent. In this study, PCL and PCL/OA scaffolds exhibited porosity and wetting property sufficient to support cell proliferation and adhesion. Additionally, OA had positive effect on ADSC cell differentiation and proliferation, resulting in evident higher calcium deposits, thus benefiting OA–cells interaction. Furthermore, OA addition enhanced tissue growth migration, based on in vivo results. In vitro and in vivo data motivate further studies using larger animal models, so as to develop strategies for bone tissue engineering.
Footnotes
Authors’ contributions
All authors participated in the interpretation of the studies, analysis of the data, and review of the manuscript. GBCC and CACZ wrote the paper and produced the materials and characterizations; EC, PGLC and MRC were responsible for in vivo surgery as well as histological characterizations; PBR, ASSD and STOS were responsible for in vitro stem cell studies
Acknowledgements
The authors thank Espaço da Escrita- Coordenadoria Geral da Universidade – UNICAMP- for the language services provided. This work was funded by the São Paulo Research Foundation (Fapesp 2009/54546-9 and 2013/19472-0) and INCT-Biofabris.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
All authors hereby declare that all experiments have been examined and approved by the appropriate ethics committee and have therefore been performed in accordance with the ethical standards laid down in the 1964 declaration of Helsinki. For in vitro assay, it was approved the project “Differentiation of stem cells obtained from adipose tissue to chondrocytes using collagen type ii as scaffold for cartilage repair” by the research ethics committee of the University of Campinas, CEP/FMC/UNICAMP, number 838/2008. The project “Viability of polymers, bioceramics and natural grafts for bone repair on cases none and smokers in vivo model” was approved by the research ethics committee from the School of Medicine of Jundiai (FMJ), the number is cep 276/2013.