
Abstract
Six million cancer patients worldwide receive radiotherapy, either alone or in combination with other cancer treatments annually. The purpose of this study was to investigate, at the structural and molecular levels, the protective effect of N-acetylcysteine (NAC), a powerful antioxidant, against radiotherapy-induced damage on the intestinal system. Three study groups were constituted: control (group 1: no radiotherapy), radiotherapy (RT; group 2), and RT + NAC (group 3). The NAC group received 300 mg/kg NAC orally for five days before irradiation. At the end of the 5th day, 6 Gy was irradiated once, and 300 mg/kg NAC was administered orally for two days following irradiation. NAC drug administration was maintained for a total of seven days. At the end of the study, the rats were euthanized by the administration of anesthetic agents and sacrificed. The malondialdehyde (MDA) levels and caspase-3 expression increased and glutathione (GSH) levels decreased in RT rats compared to the control group (p < 0.05). NAC reduced MDA levels, and caspase-3 expression, and increased GSH levels in the small intestine caused by RT (p < 0.05). Therefore, NAC may be useful in the prevention of gastrointestinal syndrome in patients undergoing radiotherapy in the treatment of malignancy.
Impact statement
Some six million cancer patients currently receive radiotherapy. Radiotherapy eliminates cancer cells by accelerating their death. However, radiotherapy is not selective, and it therefore harms healthy tissues around cancerous tissue. The latest studies have shown that the irradiation of biological materials causes a rapid increase in reactive oxygen species (ROS) in the tissue as a result of exposure of the target molecule to direct and indirect ionization. N-acetylcysteine (NAC) is an antioxidant that permits the elimination of free oxygen radicals and that contributes to glutathione synthesis. Our study, therefore, examined the effects of radiation resulting from radiotherapy on the small intestine at the molecular level, and prospectively considered the potential protective characteristics of NAC against gastrointestinal syndrome resulting from radiotherapy.
Introduction
The current global number of cancer patients is approximately 25 million, but the number of individuals diagnosed with cancer is expected to rise to 75 million in the next 20 years.1,2 Some six million cancer patients currently receive radiotherapy, either alone or together with other modalities, such as surgery, immunotherapy, chemotherapy, and hormone therapy. 3 Radiotherapy eliminates cancer cells by accelerating their death. 4 However, radiotherapy is not selective, and it, therefore, harms healthy tissues around cancerous tissue.4,5
Previous studies reported that the most significant condition resulting from 6–8 Gray (Gy) irradiation is gastrointestinal syndrome, the effects of which include anorexia, lethargy, infection, fluid and electrolyte loss, and reduced intestinal absorption associated with villus loss and gastric retention.6–8 The latest studies have shown that the irradiation of biological materials causes a rapid increase in reactive oxygen species (ROS) in the tissue as a result of exposure of the target molecule to direct and indirect ionization.9–11 ROS cause cellular damage by causing adverse effects on antioxidant defense mechanisms by reducing glutathione (GSH) levels and increasing malondialdehyde (MDA) levels.12,13 Recent studies have also shown that ROS cause damage to DNA and lead to caspase-dependent apoptosis.14,15 Activation of the caspase-3 cascade plays a highly important role in apoptosis and is regarded as a terminal event prior to cell death and increases under the effect of radiation.16–18
N-acetylcysteine (NAC) is an agent particularly used as an antidote in mucolytic and analgesic drug intoxications.19,20 Additionally, NAC is an antioxidant that permits the elimination of free oxygen radicals and that contributes to GSH synthesis. 21 NAC plays an active role in the elimination of free oxygen radicals by increasing GSH levels in tissues.21,22 In addition, NAC has been reported to inhibit ROS-induced apoptosis by reducing caspase-3 expression. 23
Our study, therefore, examined the effects of radiation resulting from radiotherapy on the small intestine at the molecular level, and prospectively considered the potential protective characteristics of NAC against gastrointestinal syndrome resulting from radiotherapy.
Materials and methods
Experimental animals
Twenty-four male Sprague Dawley rats, 3–4 months old and weighing 280 ± 25 g, were procured from the Recep Tayyip Erdoğan University Animal Care and Research Unit (Rize, Turkey). All animals received humane care as described in the “Guide for the Care and Use of Laboratory Animals” prepared by the National Academy of Sciences and published by the National Institutes of Health.
Before and during the experimental period, all rats were housed in standard plastic cages under optimal temperature conditions of 22 ± 2°C and 55 ± 5% humidity in a 12-h light–dark cycle, with ad libitum access to standard rat chow and tap water. The study protocol was approved by the local animal care committee of Recep Tayyip Erdogan University (Rize, Turkey; No. 2018/37, DATE: 03.05.2018).
Drugs and chemistry
NAC (ASIST 4%, 150 mL, 60 g granules) was obtained from Hüsnü Arsan İlaçları A.Ş. (Istanbul, Turkey). Animals were anesthetized under ketamine hydrochloride (Ketalar®, 50 mg/kg, Pfizer İlaçları Ltd. Şti., Istanbul, Turkey) and xylazine hydrochloride (Rompun®, 5 mg/kg, Bayer, KS, USA). All chemicals used for laboratory experiments were purchased from Sigma Chemical Co. and Merck (Darmstadt, Germany).
Experimental protocol
The animals in this study were randomly assigned into three groups containing eight members: control, radiotherapy, and radiotherapy + NAC. Group 1 received saline per os alone for seven days. Group 2 was irradiated once with 6 Gy over the whole body. Group 3 received 300 mg/kg NAC orally for five days prior to irradiation by the modification of a previously described procedure. 24 NAC was again administered orally at 300 mg/kg for two days following irradiation. Drug administration was completed on the seventh day.24,25
Irradiation procedure
Prior to radiotherapy, rats (groups 2 and 3) were anesthetized with a single intramuscular (IM) dose of 50 mg/kg ketamine and 5 mg/kg xylazine. Rats were placed in the prone position under anesthesia on the radiotherapy table.
Radiotherapy zones were adjusted so as to involve the entire body, including the small intestines. A single fraction of 6 Gy was applied using x-radiation with a linear accelerator device (Elektra, Synergy), at SSD of 98.5 cm at half depth with the installation of a tissue-equivalent bolus to rats’ inferior and superior aspects with a gantry angle of 0° and 180° from the front and rear using the isometric method and an area size of 10 × 40 cm. A 95% volume of the intestine received the entire dose (100%). 26 The calculation was performed with a convolution algorithm on the CMS XIO treatment planning system version 5.0 as an RT planning system 26 (Figure 1).

Ionizing irradiation procedure. (A color version of this figure is available in the online journal.)
At the end of the experiment, rats were sacrificed under high-dose anesthesia. The intestines were carefully removed. One part of the intestines was stored at −80°C for biochemical investigation. The other part was placed in 10% neutral formalin for histopathological and immunohistochemically study.
Biochemical procedure
MDA assay
MDA was measured using the method described by Ohkawa et al. 27 MDA resulting from lipid peroxidation was determined by the optical reading of the pink complex at 532 nm, which forms as a result of heating in Tris-buffered saline solution.
Reduced GSH assay
GSH assay was performed using the method described by Ellman. 28 Total GSH was determined by analyzing the reduced and oxidized GSH. Reduced GSH was measured by the optical reading of the yellow complex resulting from the reduction of 5,5'-dithiobis 2-nitrobenzoic acid by sulfhydryl groups at 412 nm.
Total protein assay
Since GSH and MDA quantitative analysis results were to be expressed as per protein levels, protein levels were determined using the Lowry method. 29
Histopathological analysis procedure
Small intestine specimens from rats from all groups were fixed in a fixator in 10% formalin (Sigma Aldrich, St. Louis, MO, USA) for 48 h. Following fixation and routine histological procedures, small intestine specimens were embedded in paraffin blocks (Merck). Next, 4–5 µm sections taken from the paraffin blocks using a microtome (Leica, RM2125RT, Germany) were stained with hematoxylin (Harris hematoxylin, Merck). The small intestine tissues were examined under a light microscope (Olympus BX51, Olympus Corporation, Tokyo, Japan) and photographed using an Olympus DP71 (Olympus Corporation) camera. 30
Immunohistochemical (IHC) analysis procedure
A caspase-3 immunohistochemistry kit was applied to the small intestine sections in order to determine apoptotic cells. Small intestine sections were incubated with primary caspase-3 antibody (Rabbit polyclonal antibody, ab2302, Abcam, UK) and secondary antibody (Goat Anti-Rabbit IgG H&L, HRP, ab205718, Abcam) in accordance with routine IHC protocols. Next, sections were incubated in anti-digoxigenin-peroxidase. Finally, the sections were counterstained with Harris hematoxylin. 31
Semi-quantitative analysis
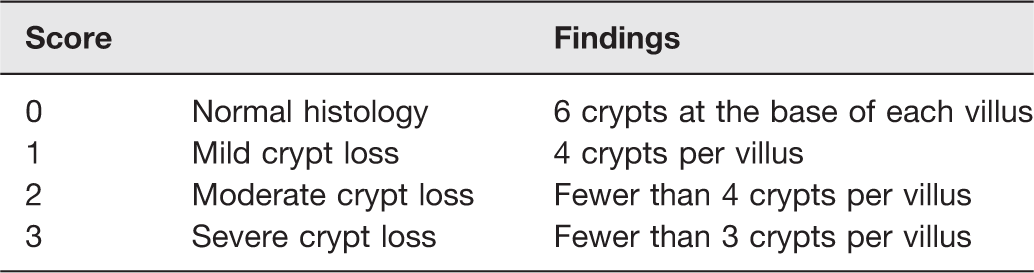
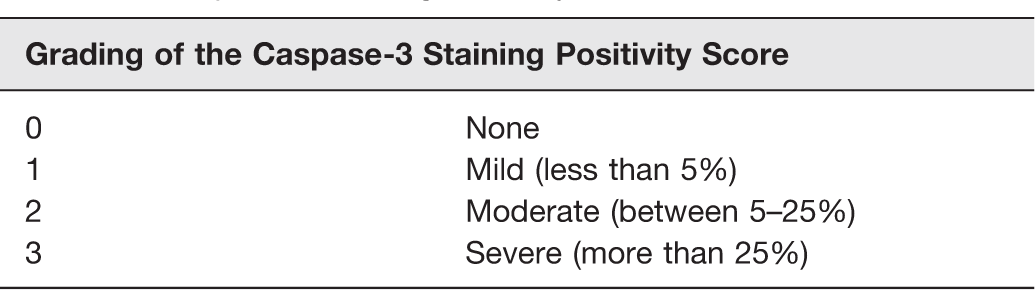
Histopathological changes observed in the villus and crypt in small intestine tissue sections were scored as shown in Table 1, using predefined Elliot’s intestinal mucosal damage score. 32 The histopathologist classifying the small intestine sections was also blinded to all the groups. In addition, the scores of villus and crypt epithelial caspase-3-positive cell are shown in Table 2. The blind semi-quantitative analysis was performed by an independent histopathologist.
Radiation-induced intestinal injury scoring as described by Elliot et al.
Caspase-3 Staining Positivity Score.
Statistical analysis
All data were calculated using SPSS 18.0 statistical software (IBM, Armonk, NJ, USA). Data obtained from semi-quantitative analyses were expressed as a median ± standard deviation and were analyzed using the parametric Kruskal Wallis test. Intergroup differences were analyzed using the Tamhane test. Biochemical data were expressed as mean ± standard deviation. Intergroup differences were analyzed using one-way analysis of variance (ANOVA), followed by the Tukey HSD test. p values <0.05 were regarded as statistically significant.
Results
Biochemical analysis
The mean MDA level in the control group was 0.08 ± 0.008 nmol/mg tissue, rising to 0.13 ± 0.011 nmol/mg tissue in the RT group (p = 0.000; p < 0.05; Table 3). NAC reduced MDA levels after administration of RT from 0.13 ± 0.011 nmol/mg tissue to 0.10 ± 0.011 nmol/mg tissue (p = 0.000; p < 0.05; Table 3). However, NAC increased MDA levels from 0.08 ± 0.008 nmol/mg tissue in the control group to 0.10 ± 0.011 nmol/mg tissue (p: 0.012; p < 0.05; Table 3).
Biochemical analysis results (mean ± standard deviation).
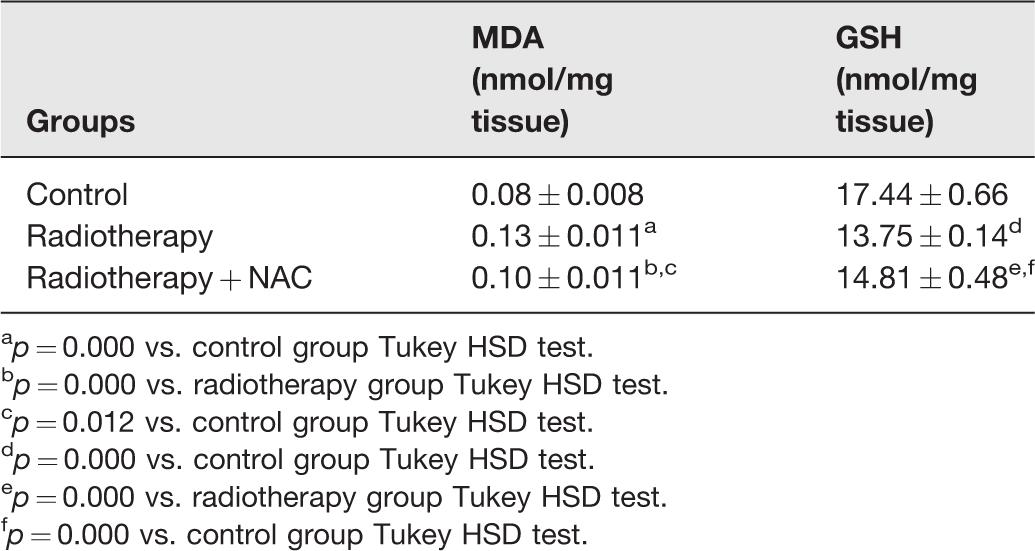
ap = 0.000 vs. control group Tukey HSD test.
bp = 0.000 vs. radiotherapy group Tukey HSD test.
cp = 0.012 vs. control group Tukey HSD test.
dp = 0.000 vs. control group Tukey HSD test.
ep = 0.000 vs. radiotherapy group Tukey HSD test.
fp = 0.000 vs. control group Tukey HSD test.
The mean GSH level in the control group was 17.44 ± 0.66 nmol/mg tissue, compared to 13.75 ± 0.14 nmol/mg tissue in the RT group (p: 0.000; p < 0.05; Table 3). NAC raised GSH levels after administration of RT from 13.75 ± 0.14 nmol/mg tissue to 14.81 ± 0.48 nmol/mg tissue (p: 0.000; p < 0.05; Table 3). On the other hand, NAC reduced GSH levels from 17.44 ± 0.66 nmol/mg tissue in the control group to 14.81 ± 0.48 nmol/mg tissue (p: 0.000; p < 0.05; Table 3).
Histopathological analysis
The intestinal villus and crypt in light microscopic sections taken from the duodenums of the control group exhibited a normal histological structure (Figures 2(a), 3(a),(b)). On the other hand, in sections from the radiotherapy group, we determined a decrease in intestinal villus numbers accompanying widespread fusion in intestinal villi (Figure 2(b)). We observed a decrease in intestinal crypt structure scores. We also observed disintegration in epithelial cells, fibrosis, and diffuse hemorrhagic areas in the lamina propria (Figures 2(b), 3(c),(d)). However, sections from the NAC treatment group revealed a typical intestinal villus and crypt structure. We also observed a regular structure in intestinal epithelial cells (Figures 2(c), 3(e),(f)).

Representative light microscope image of the duodenal tissue. H&E staining. (a: ×200) and (b: ×400) control group: healthy villus (v) and crypts (c) structures of the intestinal tissue. Typical brush border epithelium (arrow) and goblet cell (arrowhead). Regular lamina propria (Lp). Lacteal (L). (IDS median: 0.00 ± 0.41). (c: ×200) radiotherapy group: severe intestinal villus and crypt loss (IDS median: 4.00 ± 0.57). The decrease in intestinal villus and crypts numbers accompanying widespread fusion in intestinal was monitored. Besides, disintegration in epithelial cells (arrow), and diffuse hemorrhagic areas (asterisk) in the lamina propria were observed. (d: ×200) radiotherapy + NAC group: typical villus (v) and crypts (c) structures of the intestinal tissue were observed. Regular brush border epithelium (arrow) and goblet cell (arrowhead). (IDS median: 1.00 ± 0.43). (A color version of this figure is available in the online journal.)
Figures 3. Representative light microscopic appearance of the duodenal tissue. Goldner’s Masson Trichrome staining. (a: ×100) and (b: ×200): control group; healthy villus (v) and crypts (c) structures of the intestinal tissue. (c: ×100) and (d: ×200): radiotherapy group; the decrease in intestinal villus and fibrosis accompanying widespread fusion in lamina propria were monitored. (e: ×100) and (f: ×200): radiotherapy + NAC group; regular villus (v) and crypts (c) structures of the intestinal tissue were observed. (A color version of this figure is available in the online journal.)

IHC analysis
Examination of sections from the radiotherapy group revealed an increase in intestinal epithelial cell caspase-3 positivity compared to the control group (p = 0.00; p < 0.05; Table 4; Figure 4). In contrast, intestinal epithelial cell caspase-3 positivity decreased significantly in the NAC treatment group compared to the radiotherapy group (p = 0.00; p < 0.05; Table 4; Figure 4).

Representative light microscope appearance of caspase-3 stained sections from intestinal tissue. (a: ×400) normal enterocytes were observed on control group sections (Caspase-3 Positivity Score: 0.00 ± 0.41). (b: ×200): apoptotic enterocytes (arrow) were observed in the villus-crypts epithelium in RT group sections (caspase-3 positivity score: 4.00 ± 0.57). (c: ×400): typical enterocytes from RT + NAC group were monitored (caspase-3 positivity score: 1.00 ± 0.43). (A color version of this figure is available in the online journal.)
Caspase-3 Staining Positivity Score results (median ± standard deviation).

ap = 0.00 vs. control group Kruskal–Wallis test.
bp = 0.00 vs. radiotherapy group Kruskal–Wallis test.
Semi-quantitative analysis
We observed an increase in intestinal damage scores (IDS), resulting in severe crypt loss in the radiotherapy group compared to the control group (IDS median: 4.00 ± 0.57; p = 0.00, p < 0.05; Figure 2(b); Table 3). In the NAC treatment group, radiotherapy-induced IDS was significantly reduced (IDS median: 1.00 ± 0.43; p = 0.00, p < 0.05; Figure 2(c); Table 4).
Discussion
Several studies have reported that due to the rapid intestinal epithelial cycle, the small intestine is quite sensitive to acute and chronic toxicity developing in association with radiotherapy.32,33 El-Ghazaly et al. reported that the shedding of intestinal epithelial cells resulting from ionizing radiation led to fusion in the intestinal villi. 34 Elliott et al. reported that ionizing radiation led to dose-dependent decreases in villus and crypt structures. 32 That study also reported that exposure to ionizing radiation led to damage in the crypt, as well as the villus. 32 In our study, similarly to Elliott et al., a single 6 Gy dose of ionizing radiation led to severe villus and crypt loss. In addition, we observed shedding in the villus epithelium. Kiang et al. also reported that a single 8.75 Gy dose of gamma radiation led to edema and thickening associated with hemorrhage in the villus structure. 16 Similarly, in our study, we determined hemorrhage in the lamina propria of the intestinal villi and thickening in villus structure.
Although the mechanism of acute gastrointestinal syndrome developing in association with ionizing radiation is not fully understood, recent studies have implicated oxidative stress developing in association with increased ROS production.14,35–37 ROS lead to cell damage via an adverse effect on antioxidant defense mechanisms by lowering reduced GSH levels and increasing MDA levels. 12 Zhao and Robbins reported that ionizing radiation increased MDA levels. 8 Similarly, in our study, a single 6 Gy dose of radiation increased MDA levels. The second most important parameter of oxidative stress in tissue exposed to ionizing radiation is GSH. Wu et al. also showed that GSH is an important product for the prevention of tissue damage against ROS and decreases due to the effect of damage. In our study, GSH level has been shown to be decreased against radiation damage in accordance with previous studies. 11
Recent studies have reported that radiation-induced gastrointestinal syndrome causes apoptosis, particularly of crypt cells, in the small intestine.38–41 Poindexter et al. reported that 12 Gy full-body radiation caused apoptosis in intestinal cells. 42 Kiang et al. reported that a single 8.75 Gy dose of gamma radiation caused an increase in caspase-3 expression in intestinal cells between the first and seventh days. 16 Similarly, in the present study, we observed an increase in caspase-3 positivity in villus and crypt epithelial cells two days after a single 6 Gy dose of ionizing radiation.
NAC, a drug with no significant side-effects, has been used as a therapeutic agent in the last few decades in respiratory diseases, and in hepatotoxicity developing in association with acetaminophen overdose.15,19,43 NAC plays a role in GSH formation as a precursor of L-cysteine and reduced GSH.15,21,43,44 Weiss and Landauer reported in an early study that NAC affords protection from apoptosis caused by radiotherapy. 45 Reliene et al. reported that NAC exhibited protective effects in healthy cells against radiation-derived genotoxicity. We also determined that NAC increased GSH and reduced MDA levels. Samuni et al. reported that NAC blocked increases in caspase-3 and caspase-7 levels developing in association with radiation. 43 Nonetheless, they also reported that NAC had no effect on caspase-3 and caspase-7 in radiation-related apoptosis. 43 However, in our study, we observed that NAC reduced caspase-3 positivity in villus and crypt epithelial cells.
The limitations of our research include the fact it was designed as an acute study, stress deriving from oral administration, and oxidative stress were assessed using only two parameters. In addition, oxidative stress should also be evaluated using other oxidant and antioxidant enzymes and molecules. Moreover, mucin content should be separately assessed for analysis of small intestine goblet cells.
Conclusion
In conclusion, a single 6 Gy dose of whole-body ionizing radiation caused apoptosis in intestinal villus and crypt cells in association with oxidative stress. NAC suppressed ROS production by increasing GSH levels and reducing those of MDA. Our study needs to be supported by further studies investigating mechanisms such as other oxidative stress enzymes and molecules, inflammation, and intracellular Ca+2 levels.
Footnotes
Authors’ contributions
FM and AT conceived and designed research. FM conducted experiments. AY contributed new reagents or analytical tools. FM, AY, SR, AT, and LT analyzed data. FM and AT wrote the manuscript. All authors read and approved the manuscript.
DECLARATION OF CONFLICTING INTERESTS
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
FUNDING
The author(s) received no financial support for the research, authorship, and/or publication of this article.