
Abstract
This study investigated the effects of hypothermia induced before cardiac arrest or after return of spontaneous circulation (ROSC) on cardiac function and myocardial mitochondrial injury after ROSC in a rat cardiac arrest model. Sixty healthy, male Wistar rats were randomly divided into the Normothermia group, pre-arrest hypothermia (Pre-HT) group, and post-resuscitation hypothermia (Post-HT) group. The rats underwent 8 min of untreated ventricular fibrillation followed by cardiopulmonary resuscitation. Twelve rats in each group were used to evaluate the left ventricular ejection fraction before ventricular fibrillation and 4 h after ROSC. Survival was determined at 24 h after ROSC. The remaining eight rats in each group were used to detect for heart malondialdehyde, reduced glutathione, adenosine triphosphate levels and mitochondrial histology. Oxygen consumption rate and mitochondrial membrane potential were evaluated 4 h after ROSC; 10 of 12 rats in Pre-HT group, 5 of 12 in Post-HT group, and 6 of 12 in normothermia group were successfully resuscitated. The survival rate of each group was 66.7%, 33.3%, and 25%, respectively. Rats in the Pre-HT group showed less alteration of the mitochondrial ultrastructure and oxidative stress injury, better maintenance of adenine nucleotides, and more preservation of the mitochondrial membrane potential and respiratory function when compared with rats in the Post-HT and normothermia groups. Transient hypothermia is an effective preconditioning stimulus to induce ischemic tolerance in a cardiac arrest model and worthy of further evaluation for potential clinical use.
Impact statement
In this paper, we investigated the effects of hypothermia induced before ischemia or after ROSC on cardiac function, oxidative stress damage, and myocardial mitochondrial ischemia–reperfusion injury after cardiac arrest in a rat model with VF. We demonstrated that pre-arrest hypothermia conferred greater cardio-protective benefits than delayed post-resuscitation hypothermia, reduced the number of defibrillations required and dosages of epinephrine during CPR, decreased oxidative stress, ameliorated mitochondrial dysfunction, and subsequently improved survival rate.
Introduction
Despite decades of efforts to improve the prognosis of cardiac arrest patients, the survival rate to hospital discharge remains poor.1,2 Even after successful resuscitation, most patients die due to post-cardiac arrest syndrome (PCAS), secondary to post-cardiac brain injury, myocardial dysfunction, and systemic ischemia/reperfusion response.
Deaths occurring early in hospital admission are often due to persistent hemodynamic instability, leading to multiple organ failure with persistent low cardiac index (CI). A low CI in survivors can be reversed within 24 h, 3 which indicates that the high in-hospital mortality after return of spontaneous circulation (ROSC) is largely attributed to myocardial dysfunction. Thus, alleviating myocardial dysfunction may improve survival. Strategies such as percutaneous cardiovascular intervention, hemodynamic support with fluids, vasopressors, inotropes, and mechanical circulatory assistance devices (i.e. intra-aortic balloon pump (IABP)), can improve myocardial function after resuscitation. However, these efforts have not eliminated the poor survival rate of cardiac arrest.
Therapeutic hypothermia has been used since the 1950s to treat patients with cardiac arrest. However, the optimal timing to initiate hypothermia has not yet been determined. Moreover, evidence of hypothermia improving cardiac performance after cardiac arrest is limited and has not been compared in global ischemic situations.
Hypothermia preconditioning is defined as a stimulus to induce the protection against subsequent ischemic reperfusion injury. Its function is similar to hypoxia, which cannot be used widely in clinical settings due to its inherent risks. Therefore, hypothermia is a promising alternative with relative safety margins. During the past few decades, studies in animals and humans suggest pre-ischemic cooling could extend the brain’s tolerance to ischemic damage, attenuating brain injury.4–7 However, its effect on cardiac function has not yet been fully elucidated.
This study was designed to investigate whether induction of hypothermia therapy would increase post-resuscitation cardiac function in a rat model of cardiac arrest. Mitochondrial abnormalities can cause post-resuscitation myocardial dysfunction,8–10 which is characterized by ischemia–reperfusion injury after cardiac arrest. Thus, mitochondrial structure and function were also examined to investigate the underlying mechanisms.
Materials and methods
This project was approved by the Animal Investigation Committee of Sun Yat-sen University and conformed with the National Institutes of Health Guidelines for Ethical Animal Research. 11 Animal care was in accordance with the recommendations of Guidelines for the Care and Use of Laboratory Animals formulated by the National Research Council.
Experimental design and grouping
Sixty rats were randomly and equally divided into three groups: the NT group, in which rats were placed on an electrically heated blanket to maintain the esophageal temperature in the physiologic range of 36 °C to 38 °C until the study was completed, the Post-HT group, in which the rats were cooled immediately after ROSC was achieved and the esophageal temperature was kept in the range of 32 °C to 34 °C by a constant temperature incubator (Beijing, China), and the Pre-HT group, in which the rats’ esophageal temperature was kept in the range of 32 °C to 34 °C by constant temperature incubator (Beijing, China) before the induction of ventricular fibrillation (VF) for 30 min and were kept on an electrically heated blanket to maintain the esophageal temperature in the physiologic range of 36 °C to 38 °C for 12 h after ROSC.
Animal preparation
Sixty healthy male Wistar rats weighing 350.0 to 416.5 g were obtained from the Experimental Animals Center of Sun Yat-sen University. After overnight fasting, the rats were anesthetized by intraperitoneal injection of pentobarbital (30 mg/kg, Sigma, Natick, MA, USA). Animal preparation was described in our previous study. Ethical institutional protocol number: [2013] A-067.
Induction of VF
The induction of VF has been published in our previous article12–14 and the details can be found in the Supplemental Data 1. Experimental protocols are shown in Figure 1.
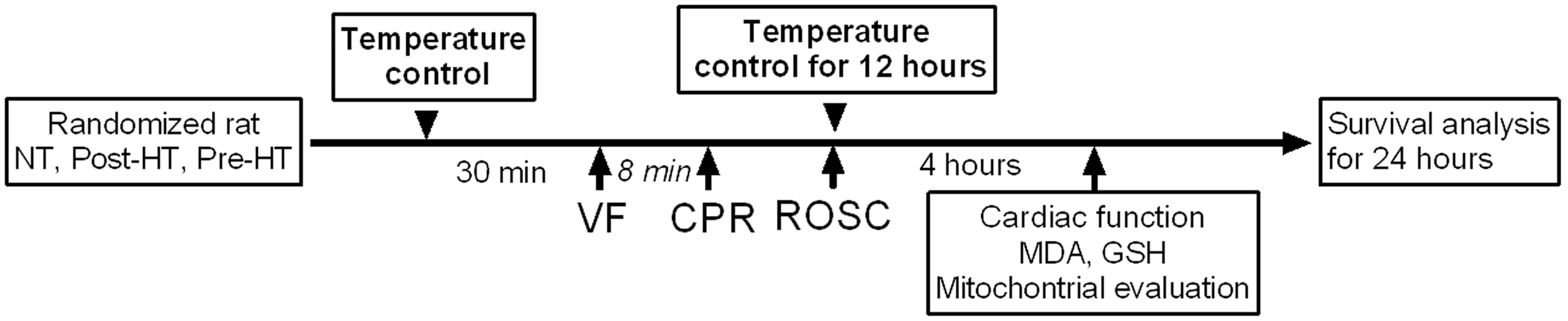
Experimental protocol flow diagram. NT: nomothermic group; post-HT: post hypothermia therapy; pre-HT: pre-hypothermia therapy; VF: ventricular fibrillation; CPR: cardiopulmonary resuscitation; ROSC: return of spontaneous circulation; MDA: malondialdehyde; GSH: reduced glutathione.
Cardiac function and survival study
Twelve rats in each group were used for cardiac function evaluation and survival analysis. Cardiac function was measured with the M-Turbo Ultrasound System 5 to 10 MHz transthoracic echocardiographic transducer (SonoSite, USA) on all animals before induction of cardiac arrest and at 4 h after ROSC. The animals were continuously observed 24 h after ROSC, and the esophageal temperature was kept in respective group target temperature ranges. The survival status was recorded and mortality was confirmed by the cessation of cardiac and spontaneous respiratory movements for 2 min. The survival rates between the different groups were compared.
Myocardial histology and myocardial mitochondrial function evaluation
Eight rats in each group were used to evaluate myocardial histology and mitochondrial function. Three additional rats served as controls.
Myocardial histology
Rats were painlessly euthanized by over-anesthetization at 4 h after ROSC. The hearts were quickly excised. Tissue blocks were taken from the free left ventricle (LV) subendocardium, fixed in cold 2.5% glutaraldehyde with 0.1 mol/L cacodylate buffer (pH = 7.4), postfixed in 1% osmium tetroxide, dehydrated, and embedded in Epon. According to the standard stereologic principle of randomization, ultrathin sections (60–80 nm) were randomly cut regardless of the orientation, mounted on copper grids, and stained with lead citrate and uranyl acetate. Transmission electron microscopy (TEM) was used to examine the structure of myocardium using an FEI Tecnai G2 TEM equipped with a Gatan 832 CCD camera (Gatan, Pleasanton, CA) at a range of magnifications from ×13,500 to ×46,000. Ultrastructural damage was assayed with the Flameng score method. 15
Measurement of malondialdehyde and reduced glutathione concentration and activities in the LV
Measurements were carried out with a malondialdehyde (MDA) detection kit (Nanjing Jiancheng Biological engineering Institute, Nanjing, China) and glutathione (GSH) kit instructions (lot E90294Ge, USCN Life Science Inc., Wuhan, China).
Myocardial mitochondria extraction
Mitochondria were isolated from the LV according to the Mitochondria Isolation Kit for Tissue (ab110168, abcam) protocol. The final pellet was resuspended in ice-cold isolation medium (20 mg protein/mL). The mouse anti-OXPHOS (MitoProfile Total OXPHOS Rodent WB Antibody Cocktail, MS604, 1:250) was used to identify protein expressions in mitochondria by Western blot analysis. Mitochondrial protein concentrations were detected using the Bradford method.
Detection of mitochondrial membrane potential
Mitochondria maintain transmembrane potentials that are important for biogenesis. Mitochondrial membrane potential (MMP) was estimated by JC-1 kit (Sigma-Aldrich, St Louis, MO, USA). All databases were analyzed by Flow Jo software (Tree Star, Ashland, OR, USA).
Measurement of mitochondrial oxygen consumption
Mitochondrial oxygen consumption was detected by using the respiratory control ratio (RCR) detection kit (Genmed Scientifics Inc., USA). After 1 min of equilibration, oxygen uptake by mitochondria was measured with a Clark-type oxygen electrode using a Hansatech Oxygraph Measurement System (Hansatech, Norfolk, UK). RCR was defined as adenosine diphosphate (ADP)-stimulated respiration (state 3) divided by resting respiration (state 4).
Measurement of ATP by high-performance liquid chromatography
Frozen samples of 1 g were homogenized in 0.3 mol/L cool perchloric acid at the ratio of 0.3 mL/50 mg inside a pre-cooling glass beaker followed by centrifugation at 15,000 RCF/min for 5 min. The supernatant was collected with an added proportional ATP/ADP standard mixture and adjusted to pH 7.6–7.8 with 0.5 mol/L KOH. The extracts were centrifuged again for another 5 min. All steps were conducted at 4°C. Adenosine monophosphate (AMP) and ADP were measured by HPLC (Shimadzu Corporation, Kyoto, Japan).
Statistical analysis
A three-group difference was compared by one-way analysis of variance (ANOVA), followed by the Bonferroni test for multiple comparisons. ROSC rates were assessed with the Chi-squared test. Kaplan–Meier survival curve analysis and the log-rank test were used for comparisons of survival between different groups. The general linear model (GLM) was used for detecting dependencies introduced by repeated measurements over time within each group. All analyses were completed by using SPSS Version 22.0 (IBM, Corp, Armonk, NY).
Results
Pre-arrest hypothermia decreased the epinephrine dose and defibrillation times, shortened the basic life support time during CPR, and improved ROSC rate
There were no differences in body weight, temperature, and EF among the groups at baseline, as shown in Table 1. The ROSC rate of rats in the Pre-HT group was higher than in the NT and Post-HT groups. The epinephrine dose, defibrillation times, and basic life support times were higher in the NT and Post-HT groups than in the Pre-HT group (Table 1). The temperatures were controlled according to the protocol (Supplementary Figure 1).
The basal parameters of rat in each group (Mean±SD).
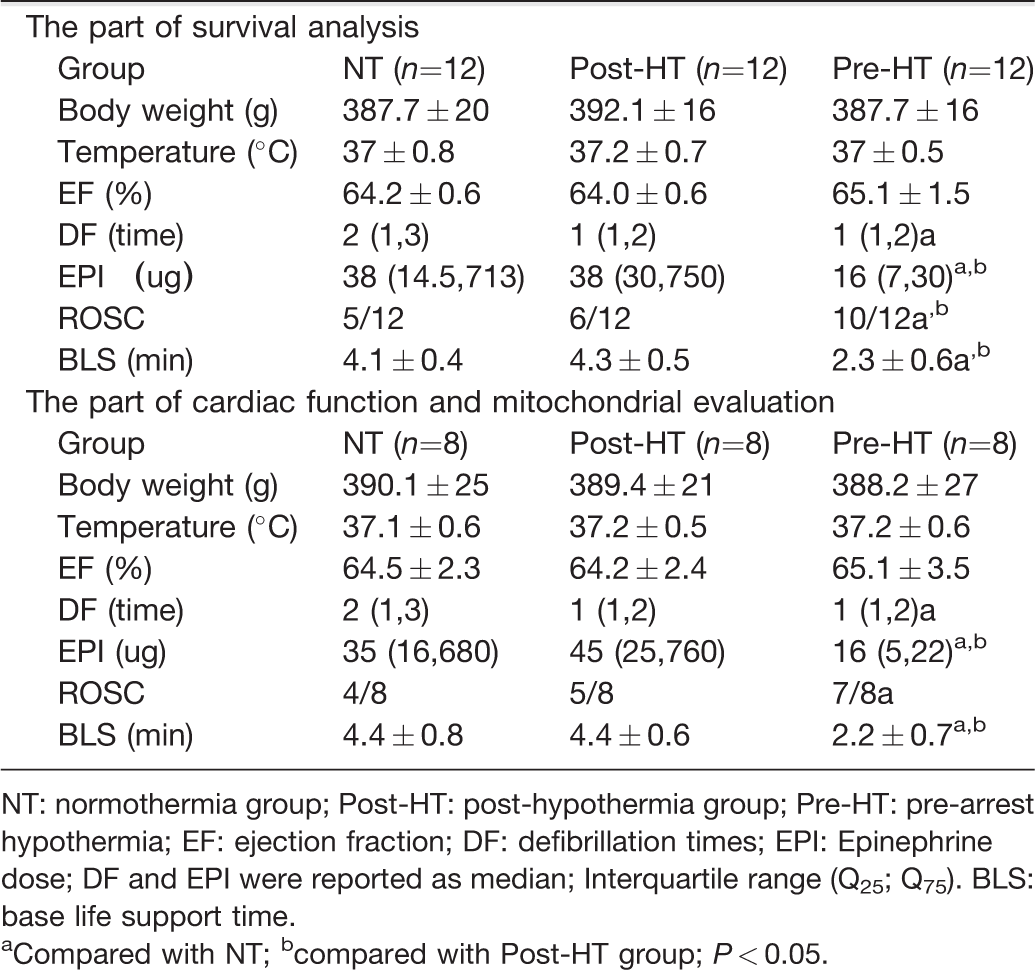
NT: normothermia group; Post-HT: post-hypothermia group; Pre-HT: pre-arrest hypothermia; EF: ejection fraction; DF: defibrillation times; EPI: Epinephrine dose; DF and EPI were reported as median; Interquartile range (Q25; Q75). BLS: base life support time.
aCompared with NT; bcompared with Post-HT group; P < 0.05.
Pre-arrest hypothermia improved LV function after ROSC at 4 h and the 24-h survival rate of rats after ROSC
There were no significant differences between LVEF values among the three groups at baseline. VF for 8 min and subsequent CPR deteriorated cardiac function, and LVEFs were 41.9% ± 4.2% in the NT group, which was lower than the 49.6% ± 3.7% in the Post-HT group (P = 0.006) and 58.7% ± 3.2% in the Pre-HT group (P = 0.001). The difference between Post-HT and Pre-HT groups was also significant, P = 0.003 (Figure 2(a)).
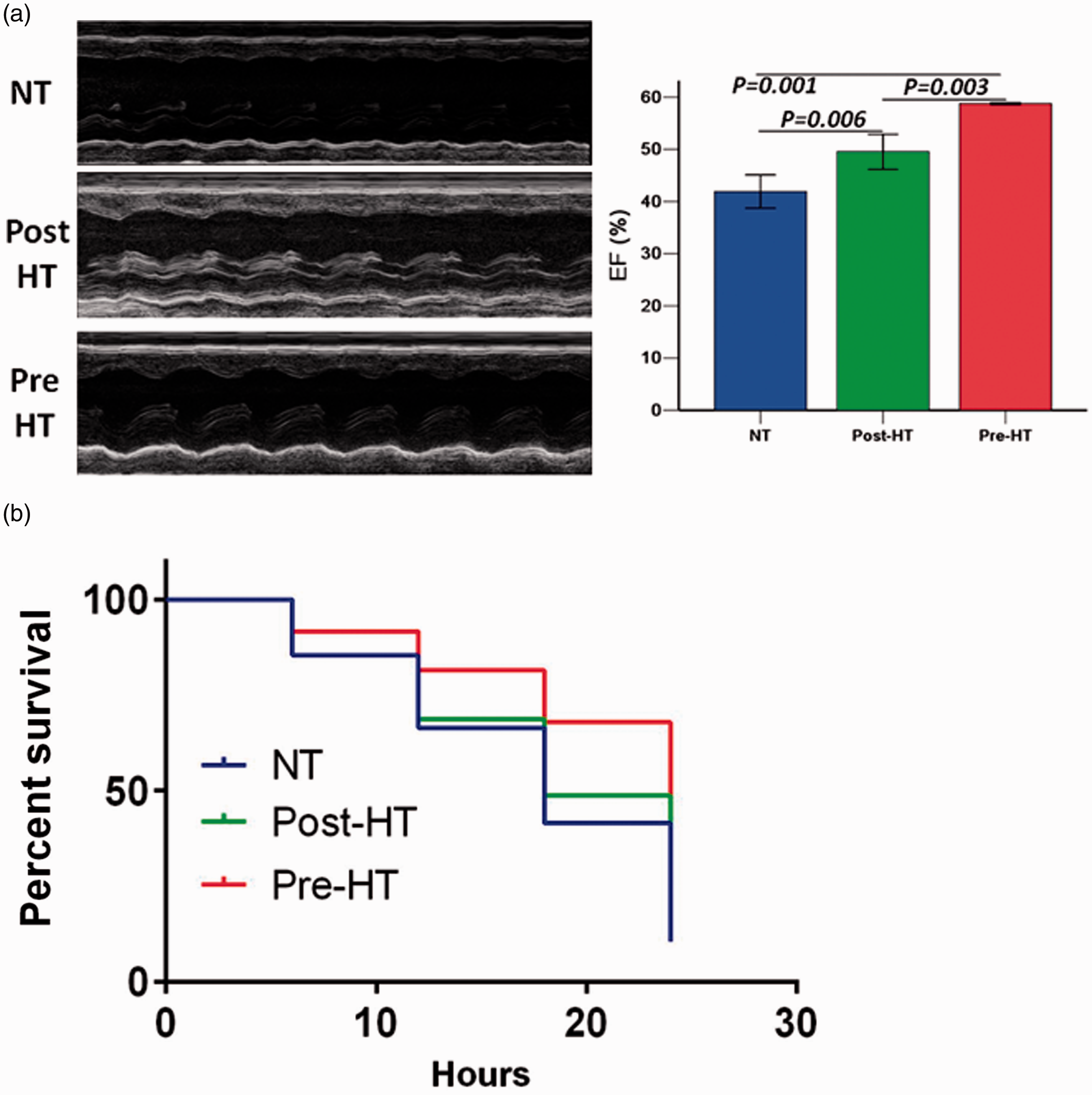
Pre-hypothermia improved the ejection fraction at 4 h and 24 h survival rate of rat after ROSC.
The Kaplan–Meier survival curves are shown for the NT, Post-HT, and Pre-HT groups. The NT and Post-HT groups showed a steep decline in the survival curve after CA and resuscitation for 24 h. Most of the successfully resuscitated animals died of refractory cardiac shock within 16 h in the NT and Post-HT groups. Only 3 of 12 rats in the NT group and 4 of 12 in the Post-HT group, but 8 of 12 rats in the Pre-HT group survived for 24 h (Figure 2(b)).
Pre-arrest hypothermia improved myocardial oxidative stress injury after ROSC for 4 h
GSH concentrations were similar at baseline, and all GSH concentrations reached high levels: 21.84 ± 0.90 μmol/g protein in the Pre-HT group, 12.0 ± 1.84 μmol/g protein in the NT group, and 16.03 ± 3.12 μmol/g protein in the Post-HT group at 4 h after ROSC (Figure 3(a)). MDA is considered to be an index of lipid peroxidation, reflecting oxidative damage to the cell membrane. Concentrations of MDA in Pre-HT group were 0.63 ± 0.085 nmol/mg, which was lower than the 1.0 ± 0.086 nmol/mg in NT group and 0.83 ± 0.057 nmol/mg in Post-HT group (Figure 3(b)).
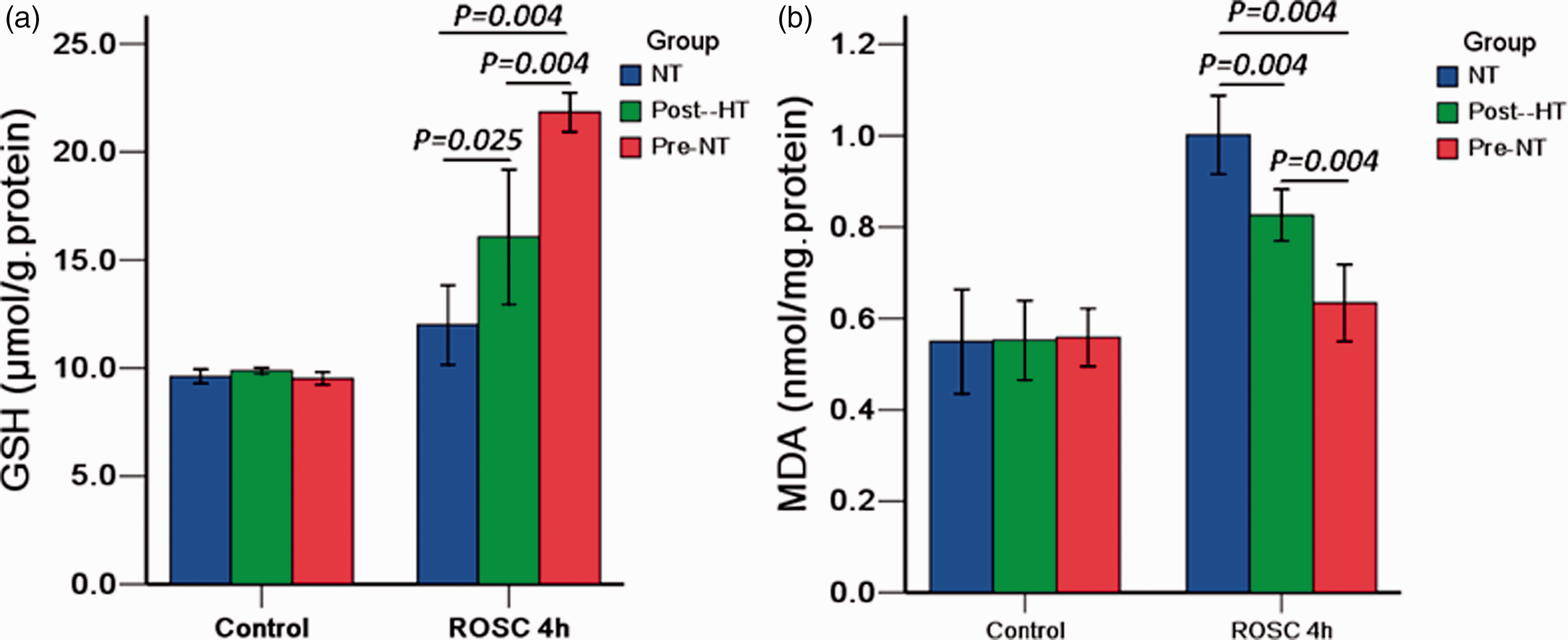
The pre-hypothermia improved myocardium GSH levels and decreased the MDA levels after ROSC for 4 h.
Pre-HT reduced mitochondrial morphologic damage and improved myocardial mitochondrial function
Mitochondria were irregular in shape among all groups after cardiac arrest. At 4 h after ROSC, the majority of mitochondria in the NT group remained severely swollen, with an increase in size, disarrangement of inner membranes, and a great loss of cristae. Whereas, mitochondria in the Pre-HT group showed relatively better ultra-structural integrity with mild swelling, slightly reduced matrix density, and partial fragmentation of cristae. The Pre-HT group had a significantly lower mitochondria damage score (Figure 4(a)).
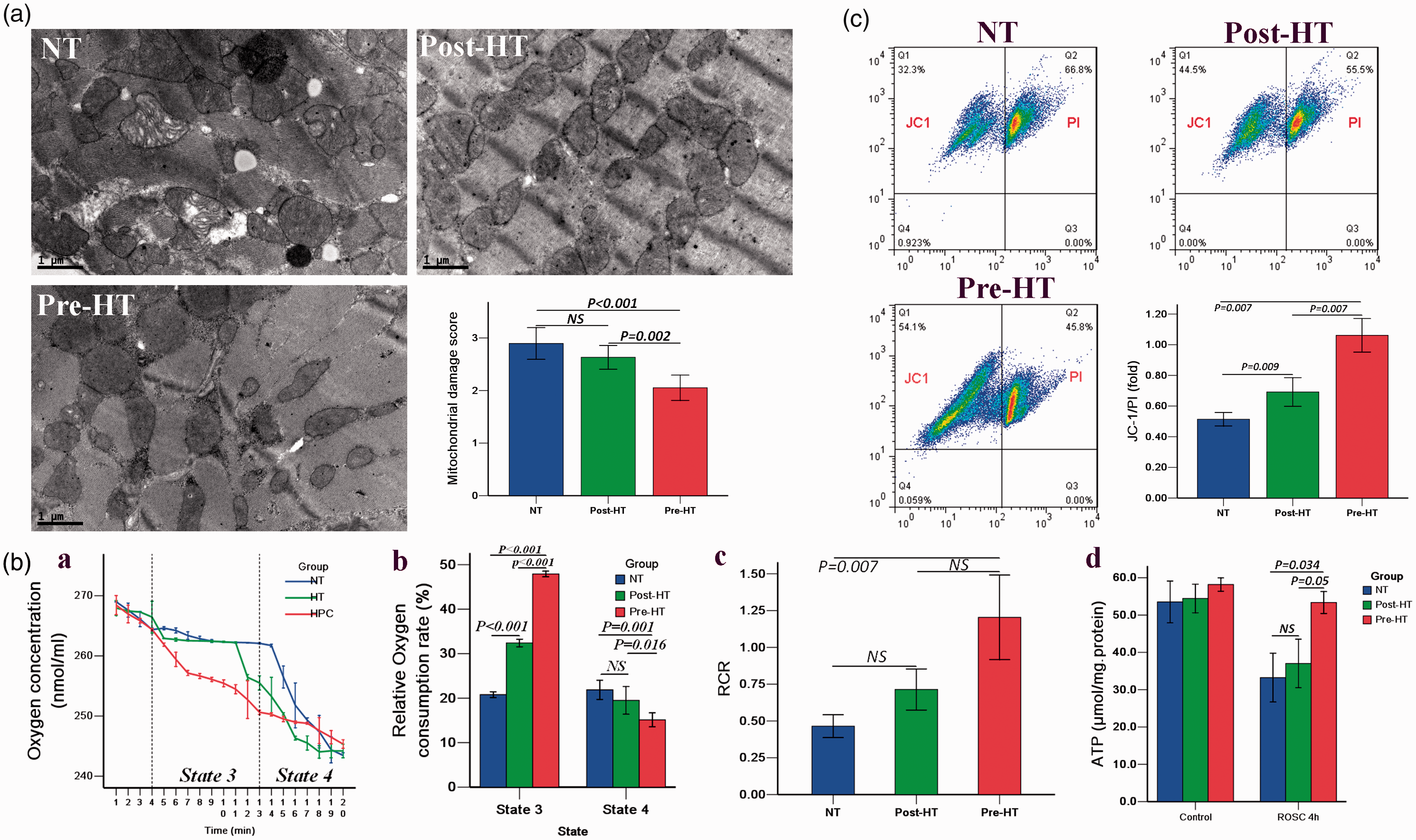
The pre-hypothermia improved mitochondria morphologic damage and mitochondria function after ROSC for 4 h.
Protein levels of OXPHOS complexes exhibited no change between NT, Post-HT, and Pre-HT groups 4 h after ROSC (Supplementary Figure 2).
A dramatically decreased RCR was diagnostic of extensive mitochondrial damage. RCR was highest in the Pre-HT group compared with NT and Post-HT groups (Figure 4(B, a,b,c).
Levels of ATP concentrations were significantly decreased in the three groups after cardiac arrest (Figure 4(B, d). At 4 h after ROSC, ATP levels in NT and Post-HT groups were significantly decreased by 53% and 45%, respectively. In contrast, the Pre-HT group ATP levels were decreased by 25% (P < 0.05). Therefore, Pre-HT treatment maintained intracellular ATP concentrations against ischemia/reperfusion injury.
Loss of MMP leads to the release of apoptogenic substances from mitochondria into the cytoplasm and initiates cell apoptosis. The preservation of MMP was lost after cardiac arrest with the loss of JC-1 red fluorescence. The Pre-HT treatment could provide better protection in order to maintain MMP relative to the other two groups, and the ratio of JC-1 to propidium iodide (PI) was 1.06 ± 0.11, 0.51 ± 0.04, and 0.69 ± 0.09, respectively in Pre-HT, NT, and Post-HT groups (Figure 4(c)).
Discussion/conclusion
Our study demonstrated a strong cardio-protective effect with pre-arrest hypothermia in a cardiac arrest animal model. The potential mechanisms underlying cardiomyocyte protection are related to less oxidative stress injury and better preservation of myocardial mitochondrial function. This includes less severe mitochondrial respiratory dysfunction, maintenance of bioenergetic metabolism, alleviation of the MMP loss, and the sustainability of ultrastructure integrity. Pre-arrest hypothermia could afford a greater cardiac performance and hemodynamic status in rats that were treated with post-resuscitation hypothermia.
Therapeutic hypothermia has been widely used in the setting of out of hospital cardiac arrest (OHCA) patients for post-ROSC management.16,17 However, there are still many questions, including whether or not a patient with cardiac dysfunction will benefit from cooling therapy, the optimal time to implement hypothermia, and its impact on cardiac function. The relevant impact of post hypothermia therapy on cardiovascular function is still controversial.16–21
In our study, we evaluated both pre-hypothermia and post-hypothermia effects on cardiac function and the potential mechanisms behind it. In the NT and Post-HT groups, the total dose of epinephrine before ROSC was higher and more shocks were delivered during CPR. This resulted in increased hemodynamic instability and subsequent poor myocardial performance after ROSC. At 4 h after ROSC, the ejection fraction was significantly lower only in the NT group and partial recovery was observed in the post-HT group. In the Pre-HT group, the ejection fraction almost normalized. We found that cooling therapy prior to arrest was more effective in protecting cardiac performance against subsequent ischemic reperfusion injury instead of implementing it after ROSC. Reversible post-resuscitation myocardial dysfunction in patients after cardiac arrest has been noted in a clinical trial, 3 but our study demonstrated that the cardiac function can be reversible in a relatively short period with hypothermia preconditioning. This was also found in another study where the LV dysfunction was partially improved by 24 h and fully recovered at 48 h. The discrepancy in recovery time is from various VF durations and the implementation of the hypothermia protocol. Finally, among the three groups, we found that pre-hypothermia provided better ROSC rates and survival rates compared with the post-hypothermia group. The improved LV function and circulatory support after reperfusion could increase the survival rate after cardiac arrest.
Another important issue this study addresses is the possible mechanism for ischemic tolerance. Mitochondrial function is key to preserving aerobic metabolism to sustain myocardial function after reperfusion and the release of various pro-apoptotic proteins to signal cell death. The observation of mitochondrial dysfunction progressing during ischemia and reperfusion after cardiac arrest has resulted in interesting pre-clinical experiments.8–10 One study used three cycles of short-term hypothermic 26°C perfusion interspersed by periods of normothermia as temperature preconditioning and confirmed that hypothermia preconditioning could increase pre-ischemic levels of creatine phosphate and ATP before ischemia. After reperfusion, it still preserved myocardial energetic metabolite concentrations and effectively inhibited the mitochondrial permeability transition pore (MPTP) opening, decreasing oxidative stress. Another study showed that temperature preconditioning induced by two brief episodes of profound hypothermia at 16°C showed strong cardio-protection of isolated ventricular myocytes against oxidative stress. These results are similar to our findings. We demonstrated that Pre-HT could alleviate the mitochondrial damage by maintaining the MMP, preserving respiratory function, sustaining energy supply, and decreasing the production of lipid peroxidation compared to Post-HT. It may be attributed to reduced metabolic demand and preserved cellular energy before ischemia, which will further mitigate the detrimental production of reactive oxygen species (ROS) defined as reperfusion injury. In addition, the preservation of structure could play an important role in maintaining its function and inhibiting the release of pro-apoptotic proteins following the ischemic reperfusion damage. These beneficial effects on mitochondria could ensure a better energy supply to cells, sustain adequate myocardial performance, and therefore, explain the preservation of cardiac function and better survival rate provided by hypothermia treatment after cardiac arrest.
Currently, the impact of the timing of hypothermia initiation after cardiac arrest is not completely understood. Our results indicated that the benefits of hypothermia used before ischemia are superior to the delay in application. We chose 30-min of hypothermia prior to ischemia with a target temperature between 32°C and 34°C as our protocol because the short duration of this temperature is tolerated by most patients without the increased likelihood of developing malignant arrhythmia and can be easily performed in a hospital.
Our study has several limitations that should be mentioned. First, it is unknown how low a hypothermic stimulus is needed to elicit a maximum amount of tolerance. Also, we used a healthy animal model in the study and in the clinical setting, many cardiac arrest victims have comorbidities. Lastly, we did not collect data on LV performance and mitochondrial function at 24 h and 48 h, where full recovery might be observed.
This study demonstrates that transient hypothermia is cardio-protective when administered 30 min before a global ischemic event occurs. Using hypothermia as a preconditioning stimulus for inducing cardio-protection is worth further evaluation for potential clinical use.
Supplemental Material
Supplemental material for Pre-arrest hypothermia improved cardiac function of rats by ameliorating the myocardial mitochondrial injury after cardiac arrest
Supplemental Material for Pre-arrest hypothermia improved cardiac function of rats by ameliorating the myocardial mitochondrial injury after cardiac arrest by Yuanzheng Lu, Xiaoyun Zeng, Xiaoli Jing, Meixian Yin, MMS Mary P Chang, Hongyan Wei, Yan Yang, Xiaoxing Liao, Gang Dai and Chunlin Hu in Experimental Biology and Medicine
Footnotes
Authors’ contributions
All the co-authors have made contributions to this study and approved the version to be published. Dr. Lu and Dr. Zeng both are responsible for the acquisition and analysis of the data and drafting of the manuscript. Dr. Hu designed the study, interpreted the data, and revised the manuscript. Dr. Chang was in charge of data analysis and manuscript revision. The rest of the co-authors all participated in the animal experiments, data collection, laboratory tests and revision of the manuscript.
DECLARATION OF CONFLICTING INTERESTS
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
FUNDING
Professor Hu was supported by funding from the National Nature Science Foundation of China (No.81272021, 81571867), and the Fourth Batch of Youth Talent Project in the First Affiliated Hospital of Sun Yat-sen University (No.Y50152). The funders had no role in the study design, data collection, analysis, decision to publish, or the preparation of the manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.