
Abstract
Alzheimer’s disease as a consequence of chronic brain inflammation mediated by infectious microbes including the oral microbiome continues to attract support. Taiwan’s National Insurance database was used to evaluate associations between dental health and Alzheimer’s disease; 209,112 new cases of Alzheimer’s disease were matched 1:4 with 836,448 dementia-free controls to test the hypothesis that better dental health would be associated with less occurrence of dementia. Ten year dental records and conditional logistic regression models were used to estimate the odds ratios associated with Alzheimer’s disease. Subgroup analyses compared vascular Alzheimer’s disease and sporadic Alzheimer’s disease. As the population aged, Alzheimer’s disease diagnoses were more frequent with a 10 fold upward inflection after 60. Nearly 56% of sporadic Alzheimer’s disease patients were women but less than 50% had vascular Alzheimer’s disease. Comorbidities were 10–20% higher in the Alzheimer’s disease patients than in controls, but stroke, chronic infection, and pneumonia were 40–45% more common in the vascular Alzheimer’s disease patients. Heart disease, hypertension, diabetes, stroke, peripheral artery disease, pneumonia, and herpetic disease (HSV) were all associated with higher odds of Alzheimer’s disease. HSV was not a factor in the vascular Alzheimer’s disease. Routine dental procedures tended to lower odds ratios. Root canals and extractions that restore oral homeostasis were associated with lower odds of dementia. However, when extractions exceeded four, the odds of Alzheimer’s disease rose. The fact that Alzheimer’s disease was not associated with periodontal procedures per se but with more frequent periodontal emergencies suggested again a chronic issue. Dental health costs suggest that good dental care was associated with lower odds of Alzheimer’s disease except for radiographic costs which were consistently associated with higher odds, independent of oral health. Common comorbid conditions were associated with higher odds of Alzheimer’s disease and oral health care was associated with lower odds, providing support for the hypothesis that the oral microbiome is a factor in the development of Alzheimer’s disease.
Impact statement
This study clearly demonstrates the power and value of a nationally applied digital medical record. Longitudinal studies of gradually developing pathologies like dementia have often been limited by sample size and narrow and incomplete medical histories. The Taiwan National Insurance database provides an unparalleled opportunity for detailed analyses of associations between current medical conditions and a spectrum of prior medical and dental events. The temporal impact of the database will only become more important as the past historical record progressively expands going forward. The inclusion of dental records in assessing the relationship with subsequent dementia is very important because this information is often unavailable or dependent on subject recall. This study clearly establishes associations between a variety of suspected cardiovascular and metabolic factors and the odds of dementia. A critical outcome should include the design of targeted interventions and the subsequent assessment of their efficacy.
Introduction
Dementia comprises a spectrum of progressively degenerative brain disorders that primarily afflict the elderly. In some cases, the disorder can be ascribed to a specific etiology like impaired blood flow or infectious pathogens like those responsible for syphilis and Lyme disease. However, in the majority of cases, the precise cause is unclear and is labeled as sporadic Alzheimer’s disease (SAD) both with and without post-mortem confirmation. Several careful reviews of the salient data have made a strong argument for the hypothesis that SAD is an inflammatory brain disorder that results from an ongoing battle between the body’s immune defenses and a variety of chronic subclinical brain infections.1,2 The progressive loss of neuronal cell numbers and associated cognitive function is presumed to be unfortunate consequences of the host’s immune response, i.e., collateral damage.
A number of potential causative microbes have been cultured from SAD brain samples and they have each demonstrated the ability to produce similar sequela in experimental model systems including the hallmarks of SAD, the accumulation of the proteins Aβ and tau needed for the pathological markers of the disorder, extracellular plaque, and neurofibrillary tangles. Most of these microorganisms are able to evade regular host defenses and persist via latency mechanisms, and/or sequestration in internal reservoirs. These characteristics allow for their periodic emergence or reactivation assuring an ongoing chronic inflammatory process.3,4 Although a number of prime candidates have been proposed, a single causative agent seems unlikely and multiple organisms are routinely isolated from post-mortem brain samples of AD patients. Successful access to the brain by any one microbe seems to facilitate the entry of others, increase their virulence and sensitize the resident immune defenses to produce a more intense and thus, more damaging response.
The source of these microbes and their continuing reservoir is also an open question. While the lung and gastrointestinal tract provide viable reservoirs of potential agents, an increasingly strong case is made for the oral microbiome.5–7 Multiple oral microbes have been isolated from SAD tissues and they clearly have proximate reservoirs within the gingival spaces and regular access to the circulation.8–13 In addition to circulatory access, the oral microbiome may have a more privileged access to the brain via retrograde transit along cranial nerve tracts. In this regard, HSV has been isolated from within the trigeminal ganglia.13–15
These collected observations led to the suggestion that individuals with good oral health should be protected from the development of SAD. The current study was designed to test the hypothesis that good oral health as evident from dental medical metrics would be associated with lower odds of SAD. The Taiwan National Medical and Dental records provide a robust database with which to test the hypothesis. The very large sample sizes with more than 200,000 cases of dementia likewise provides for the prospect of very precise analyses. The diagnostic codes also allow for subgroup analyses comparing those diagnosed with dementia and those with the specific atherosclerotic or vascular dementia (VAD). After partitioning out the VAD group, the much larger remaining group is primarily composed of patients with sporadic Alzheimer’s disease (SAD) and will be labeled as such herein.
Methods
Study population and database
The Taiwan National Health Insurance (NHI) that began in 1995 provides compulsory health insurance for the populace of 23 million with 99% participation. The associated database includes both medical and dental records.
New cases of diagnosed dementia recorded during the years 2011–2015 were identified based on an index hospital admission or after two or more outpatient visits during one year’s time (ICD 9 CM code 290.0–290-4, -331.0) From the database, 209,122 “Cases” were identified and as each was identified four dementia-free controls were selected by incidence density sampling. The resulting 836,448 controls were matched 4:1 with the cases by sex and age within five years. Medical and dental, comorbidities and selected pharmaceutical records including dental and pharmaceutical costs for the decade prior to the index diagnosis were collected for analyses. The Study protocol was approved by the National Taiwan University Hospital Research Ethics Committee.
Statistical analysis
Conditional regression models were used to estimate odds ratios (ORs) and their 95% confidence intervals (CIs). Covariates were based on retrospective data obtained from the decade prior to the index diagnosis of dementia. Sub-group analyses were also conducted for men, women, VAD, and SAD. Differences were deemed significant if their chance probability was less than 0.05.
Two conditional logistic regression protocols and five models based on the case-control matching process were executed as follows: Protocol 1: Logit (probability of dementia) = b0 + b1 (confounding factors) + b2 (dental utilization as exposure variables) + b3 (cost variables). Model 1: Exposure variables and cost variables are all continuous. Model 2: Exposure variables are categorical but cost variables are continuous. Model 3: Exposure variables and cost variables are all categorical. Protocol 2: Logit (probability of dementia) = b0 + b1 (confounding factors) + b2 (cost variables) (dental utilization not considered). Model 4: Cost variables are continuous. Model 5: Cost variables are categorical.
Results
Cases ascertainment and controls selection
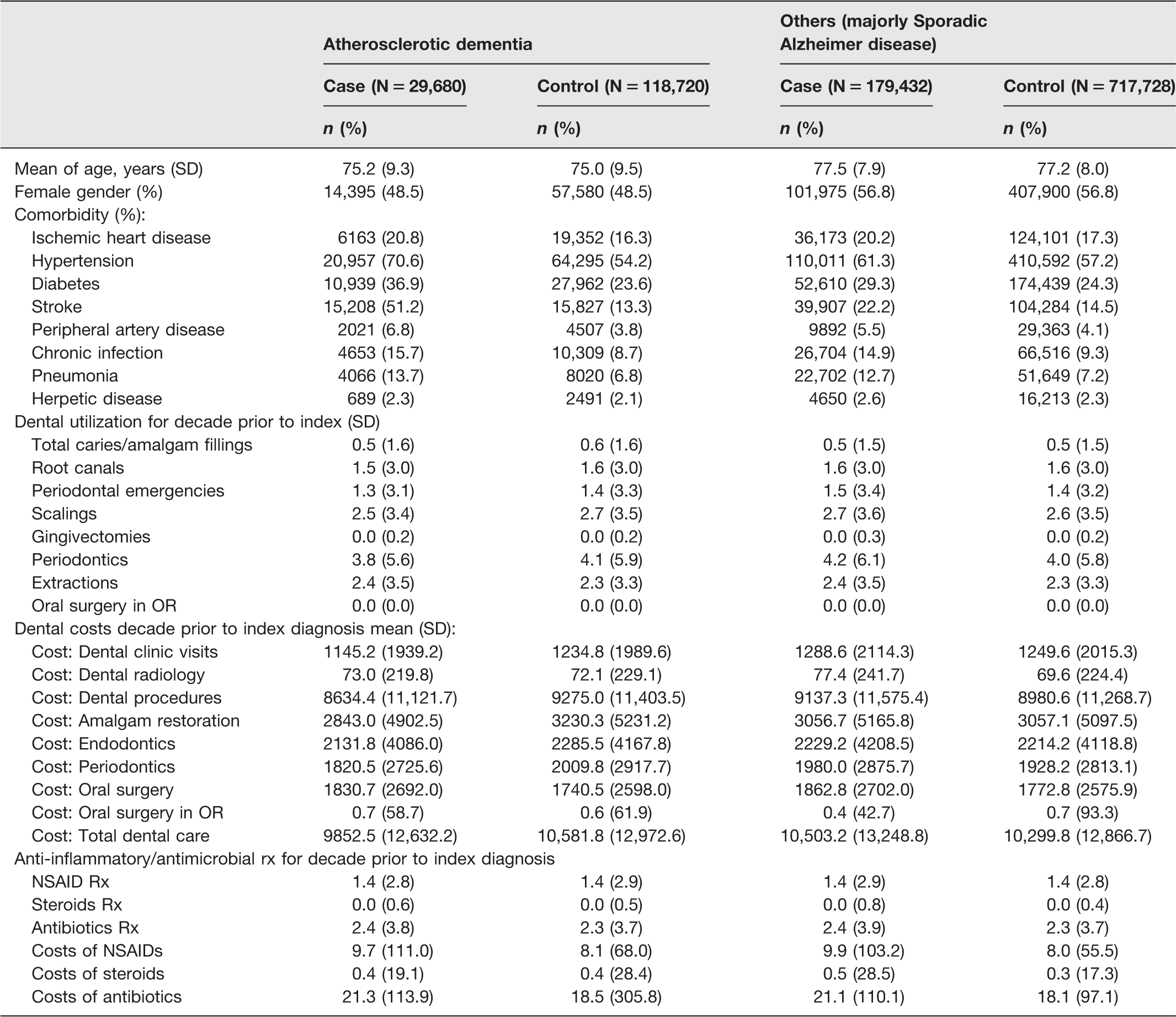
The demographics (Tables 1 and 2) include 209,112 individuals (cases) diagnosed with dementia age matched 1:4 with 836,448 dementia-free control subjects for the years 2011–2015. The dementia group was subdivided into those simply identified as dementia (86%) and those assigned the more specific diagnosis of atherosclerotic dementia (14%). Experience suggests the larger group is primarily comprised of a degenerative process (SAD). The aggregate dementia group had an average age of 77.2 years and was 55.6% female. Diagnosed dementia numbers became higher with age appearing first, late in the fourth decade (Figure 1). Less than 1% of all cases were recorded before age 60. The incidence of dementia accelerated rapidly after age 60, peaking in the early-80s age interval. After 85 years of age, the total incidence declined slightly presumably reflecting a parallel increase in age-associated mortality (survival bias). Dementia was more frequent in women (55.6%) than in men and this gender disparity was entirely due to the higher prevalence of dementia in women in the larger SAD subgroup. Men were more likely to be diagnosed with VAD than women (51.5% vs. 48.5%).
Demographics of all study patients.

Demographics of dementia subgroups.
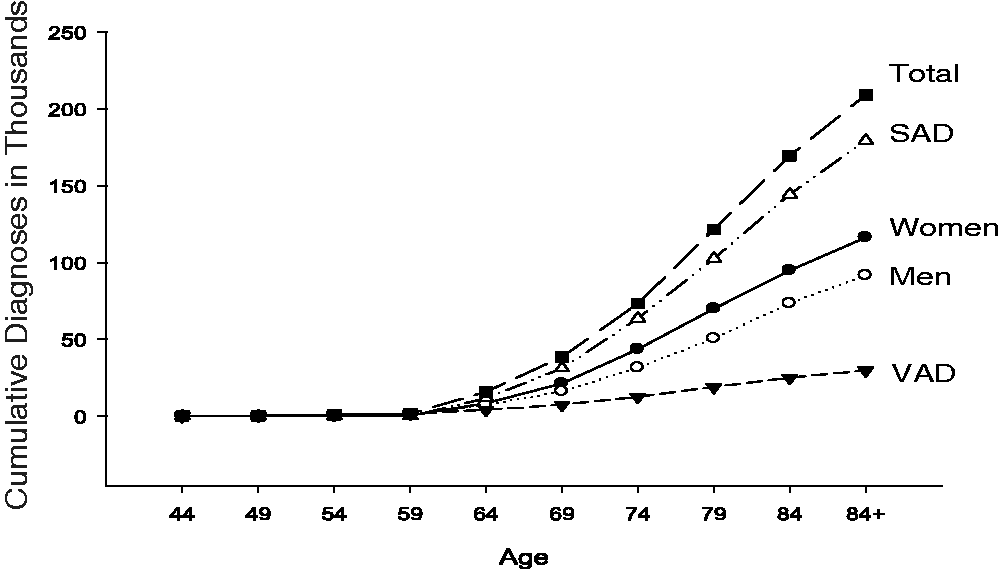
Cumulative diagnosis of dementia by age between 2011 and 2015. Total diagnoses, men, women, sporadic Alzheimer’s disease (SAD), vascular Alzheimer’s disease (VAD).
Comorbidities
The odds of dementia associated with major comorbidities were evaluated. Not surprisingly, any condition that might compromise the healthy perfusion of the brain was associated with higher odds of dementia (Table 3). Ischemic heart disease, hypertension, stroke, peripheral artery disease, and diabetes were all proportionately more prevalent in those diagnosed with dementia compared to their matched controls.
Comorbid diseases adjusted odds ratio by fitting conditional logistic model 3.
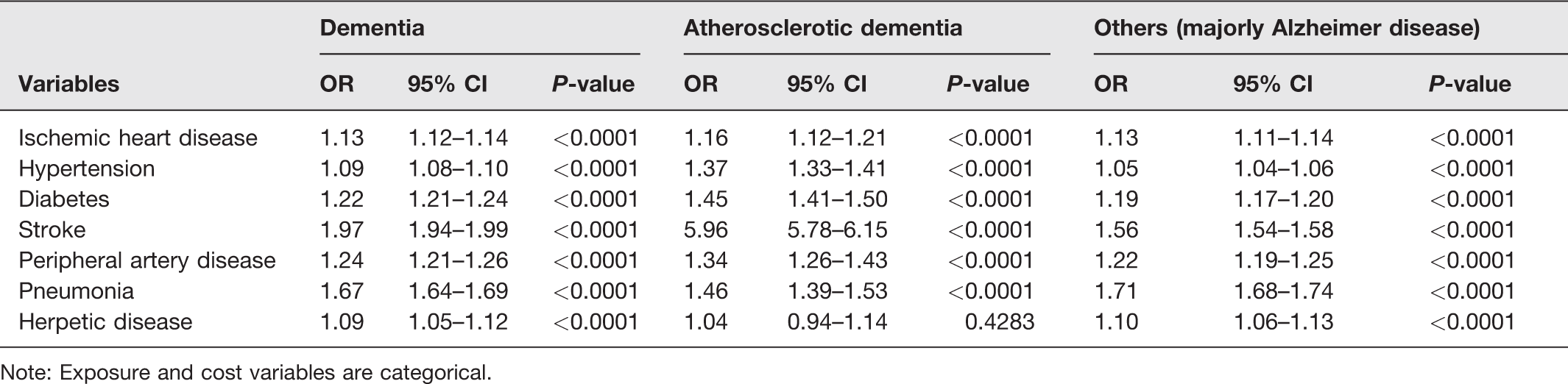
Note: Exposure and cost variables are categorical.
Chronic or recurrent infections were also far more likely among subjects with dementia compared to control subjects (Table 3). The microorganisms associated with two of these disorders, pneumonia and herpetic disease have both been proposed as mediators of dementia. These specific infections were associated with higher odds of subsequent dementia. However, by comparison, the odds associated with pneumonia was clearly much higher than that associated with HSV (OR, 1.67 vs. 1.08) and HSV was not a factor in the VAD variant.
There was no apparent change in the odds of dementia associated with the number of caries filled, gingivectomies, or scalings for the collected group (Table 4). Though not significant, routine tooth restoration and gingival care tended to be associated with lower odds of dementia. Similarly, multiple scalings tended to be associated with higher odds. Self-limiting acute procedures that should rapidly restore oral health like extractions and root canals were significantly associated with lower odds of dementia. However, when the number of teeth extracted in 10 years exceeded four, the odds of dementia reversed course and became higher. These observations suggest that the odds of dementia is associated more with chronic rather than acute, easily corrected, oral health issues.
Oral health factors adjusted odds ratios.
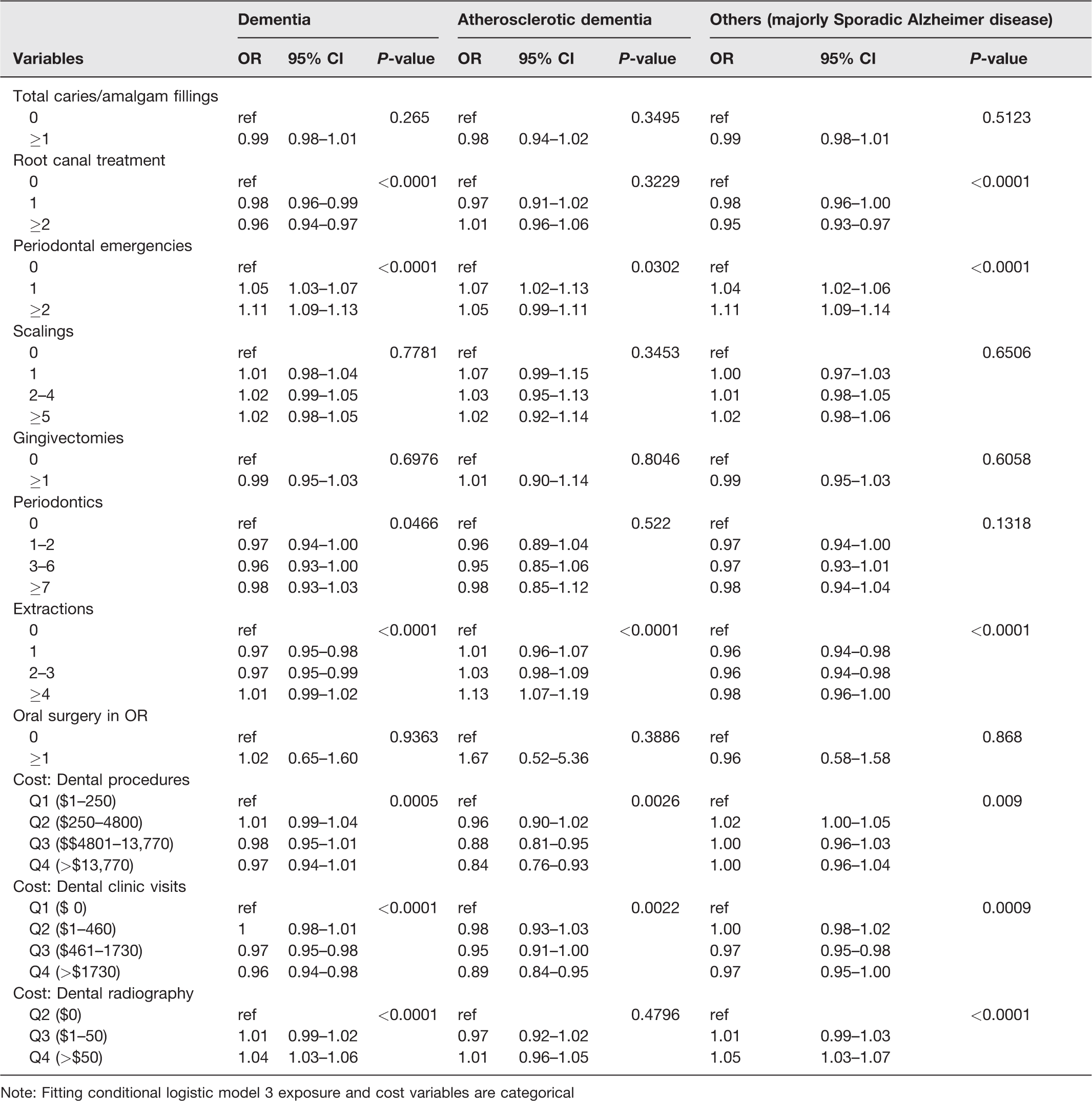
Note: Fitting conditional logistic model 3 exposure and cost variables are categorical
The odds of dementia was negatively associated with the number of periodontics procedures but positively associated with greater cost of periodontics. This higher odds associated with the cost of periodontics (Model 5: P ≤0.0001, OR 1.07) suggests again collectively that the odds of dementia was associated with greater severity, complexity, and/or frequency of the treated problems.
Oral surgery per se, was not associated with altered odds but as the cost increased, the odds became higher (Model 5: P ≤0.0001, OR 1.08), suggesting again that subsequent dementia was associated with chronic or more severe cases.
In contrast, the number of periodontal emergencies, a potential indicator of repeated oral infections, was uniformly associated with higher odds of dementia.
When the overall costs of dental procedures and/or dental clinic visits were examined categorically, the more funds spent collectively on dental care, the lower the odds of dementia. Thus, it appears that those who regularly attended to their oral health were at lower odds of dementia.
In contrast, dental radiography was consistently associated with higher odds of dementia for both the number of exposures and/or cost of dental radiology. This suggests that independent of the positive effect of good oral health care, there may an association between dementia and the exposure of the brain to repeated oral diagnostic radiation.
Based on the hypothesis that microbial inflammation is a proximate cause of dementia, the influences of selected anti-microbial and anti-inflammatory drug therapies were investigated. Collectively across the five models, subjects who required prescribed antibiotics, NSAIDS, or steroids were all associated with higher odds of dementia. This is contrary to the original thesis that these therapies would be protective suggesting that the underlying medical problems that necessitated these therapeutic interventions are causative and outweighed the proposed protective influence of said drug therapies.
Subgroup analyses
Two subgroup analyses were conducted. One specifically examined the role of sex and the other partitioned out VAD and SAD to determine subgroup differences.
VAD included 29,680 cases equivalent to 14% of the diagnosed dementia. Thus, the remaining majority of 179,728 or 86% of cases were presumed to be primarily SAD. The incidence of both forms of dementia became higher with age though the vascular form began to appear as early as late in the fourth decade. This early appearance of VAD still represents less than 1% of all cases and only about 5% of all VAD diagnoses. After age 60, the diagnosis of both forms began to rise quickly in a near parallel fashion. Both forms began to decline after age 85 suggesting again the natural influence of age-related mortalities.
As indicated above, ischemic heart disease, hypertension, diabetes, stroke and peripheral artery disease were all associated with higher odds of dementia. Each of these five comorbidities was at least marginally more prevalent in the VAD subgroup compared to the SAD subgroup. Hypertension (70.6% vs. 61.3%) and stroke (51.2% vs. 22.2%) were each much higher within the vascular dementia group. The OR for dementia associated with stroke was four fold higher (5.98 vs. 1.56) in the vascular dementia group when compared to the much larger SAD group.
Unlike the cardiometabolic issues above, the primary inflammatory disorders identified, pneumonia and herpetic infections were more evenly distributed across the two dementia categories. A history of pneumonia was consistently and substantively associated with higher odds of dementia in each of the two dementia subgroups. However, the higher odds of dementia associated with the herpes virus was consistently limited to the larger SAD group and was not a factor in the VAD group.
Despite the much larger SAD group size, associations between oral health, SAD and VAD were consistently similar to those described above for the two subgroups combined. However, the odds associated with a number of variables were different within the VAD subgroup. Specifically the number of root canals which as a categorical variable was negatively associated with the outcome in the SAD subgroup was not associated within the VAD group. Similarly, the cost of dental radiology was associated with higher odds of dementia within the SAD subgroup but no association was found within the VAD subgroup. This suggests again a specific mechanistic association between ionizing radiation and dementia and particularly within the SAD subgroup.
Finally, the categorical analyses of the selected pharmaceuticals indicate that greater use of NSAIDs and steroids were associated with higher odds within the SAD subgroup, while antibiotics were not associated (Table 5). Contrary to this observation, the opposite was true for the VAD subgroup. NSAIDs and steroids were not a factor among the VAD cases and more prescriptions for antibiotic therapy were associated with higher odds of dementia for VAD. This discrepancy may reflect a more general relationship between microbial infections (e.g. pneumonia), cardiovascular disease, and VAD.
Anti-inflammatory/ antimicrobial pharmaceuticals adjusted odds ratios.
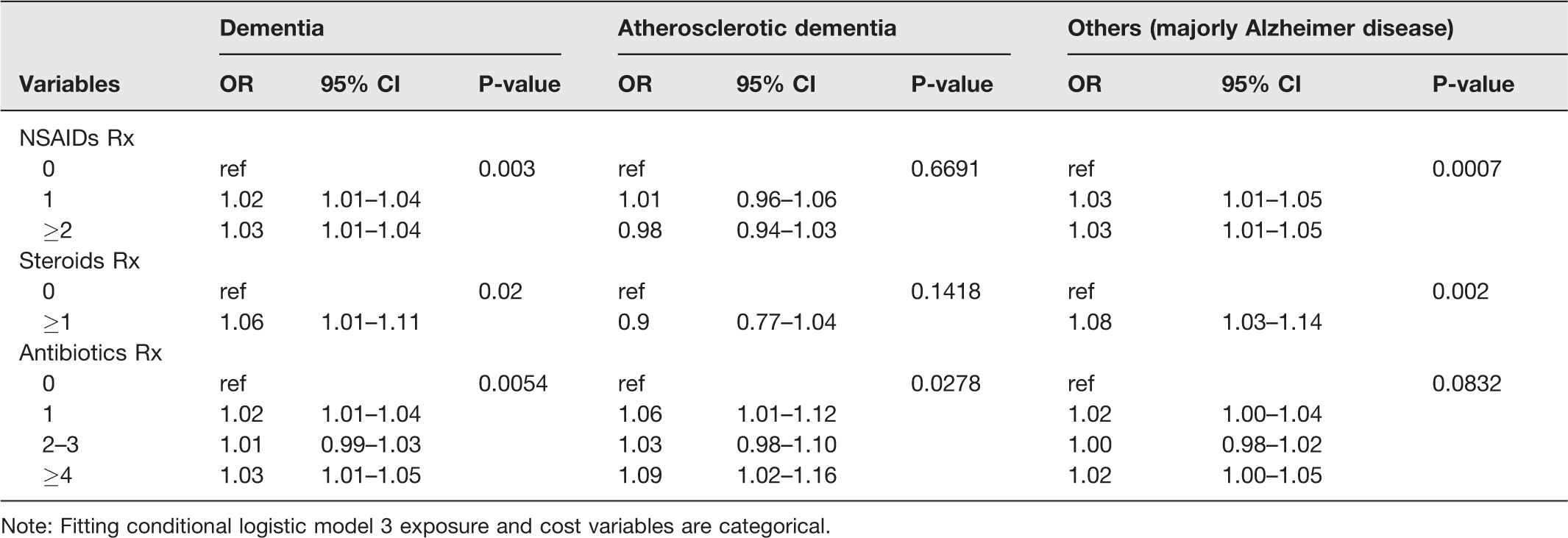
Note: Fitting conditional logistic model 3 exposure and cost variables are categorical.
Sex/gender analyses
The total incidence of dementia in men and women was similar when corrected for age-associated population numbers (Table 6). Plotting the all-case incidence between the age 60 and 85 provided a nearly linear relationship with correlation coefficients r = 0.97 for men and 0.99 for women. The greater total number of diagnoses of dementia in women prompted a reanalysis. In most analyses, the effects of tested variables were again very similar to both subgroups combined. Due to the large volume of data, only key differences will be described here. The cumulative incidence of dementia with age for women and men is illustrated in Figure 1. Approximately twice as many of the cases recorded prior to age 60 are men. As indicted above, these early cases were almost all characterized as VAD. This is a true sex difference in VAD incidence since the population is relatively balanced in these younger age groups. Demographically, the men were more likely to have vascular problems including more ischemic heart and peripheral artery disease. Thirty percent of the men with dementia had a diagnosed stroke. The women were more likely to have high blood pressure and diabetes and remarkably fewer strokes in both absolute numbers and as a fractional percentage (23%). Despite the larger case number, women were less likely to present with VAD (W 12.4% vs. M 16.5%).
Subgroup analyses demographics by sex.

Note: Fitting conditional logistic model 3 exposure and cost variables are categorical.
Stroke was positively associated with dementia in both sexes. The odds ratio for VAD was greater than 5 for women and greater than 6 for men. The odds of SAD associated with stroke, though lower than in the VAD subgroup, was still significant at 1.51 for women and 1.63 for men. Despite the demographic differences in comorbid disease distribution, each of the five disease categories retained higher odds of dementia for men and women.
Men had more diagnosed infections largely due to a higher prevalence of pneumonia. Pneumonia was associated with higher odds for both VAD and SAD for both sexes; higher for men (M 1.82 versus W 1.52) than for women. The distribution of diagnoses for HSV was relatively equal across genders. HSV posed higher odds of SAD for both men and women. Again, HSV did not appear to relate to the odds of VAD in either sex.
The frequency of dental procedures overall was quite similar for men and women. However, the cost of those procedures was consistently 5–10% higher for men including dental radiology (Table 6). Variables for which a sex disparity was observed are listed in Table 7 with male/female differences highlighted as bold P values. Surprisingly, the small number of differences provides few cogent clues as to why so many women are diagnosed with dementia. Women may have more gingival issues (periodontal emergencies; scalings) and inflammation (NSAIDs) compared with men, and men may derive more protection from periodontal procedures and the total costs of dental care than women. The cost of antibiotic and NSAIDs medication was more than 50% higher for men in the study. This greater requirement for antibiotics translates into greater odds of VAD and SAD for men. NSAIDs were associated with higher odds of SAD in women and despite the greater NSAIDs costs for men; the associated odds for men were not altered. The cost of anti-inflammatory steroids was similar between the two subgroups. Thus, NSAIDs and steroids were associated with higher odds of SAD for women. NSAIDs were not a problem for men but steroids and antibiotics were associated with higher odds of SAD for men and antibiotics were associated with higher odds of VAD for men. Thus, collectively, the apparent disparity in SAD between women and men may depend on multiple factors where women suffer more from negative influences and men benefit more from positive influences.
Female/male disparities oral health factors adjusted odds ratios.

Note: Fitting conditional logistic model 3 exposure and cost variables are categorical.
Discussion
The Taiwan National Health Insurance (NHI) database provides a unique opportunity to test for a variety of influences on the development of dementia in a national populace. The large comprehensive sample size allows for the evaluation of very subtle associations with a high degree of confidence and precision. As indicated above, the current analyses selected residents of Taiwan 40 years of age or older diagnosed with dementia within the five-year interval 2011–2015. These were then age matched 1:4 with their dementia-free countrymen and women. Five models were conducted but due to the large volume of data and similar results, the categorical Model 3 was selected for presentation. Model three was also better able to compensate for biphasic variables and dilutive effect of the VAD subgroup. In Model 3, all the variables were categorical. Selected results from the other models were presented. Two subgroup analyses were also conducted to first compare VAD and SAD and second to compare the influences on men and women separately. More than 200,000 new cases were identified during the five-year study interval. Taiwan is an aging society and since the mean mortality rate following diagnosis is 4.48 years, 16 it would appear that the overall prevalence of dementia in Taiwan will continue to increase as we proceed forward.
The primary hypothesis proposed that those with either better oral health or better oral health care would be less likely to develop dementia. This is based on the emerging concept that dementia results at least in part from chronic subclinical infectious processes within the brain.1,2 The actual brain damage then arises from normal host defense mechanisms and the resulting inflammation from the continual struggle to eliminate the foreign microbes. Although the host defense systems should be self-limiting by design, the hypothesis suggests that the offending biome is continually replenished from a natural reservoir. 5 A number of sources have been suggested due to their ready access to the external environment including the normal biome within the lungs, intestinal tract, and the oral cavity. The oral microbiome may first, have an advantage in that several of the cranial nerves serve the mouth and nasal passages and their musculature. There is experimental evidence for the retrograde transport of oral microbes along these nerves based on microbes isolated from associated ganglia and from within the postmortem brains of SAD patients. 4 Second, rough food and the sometimes intense mechanical pressure associated with mastication can easily damage and breech the oral epithelium to allow microbial access to the interstitial spaces and thus the systemic lymph. And finally, in the absence of scrupulous attention to dental hygiene, these same forces regularly create microbial reservoirs between teeth and within the gingival spaces composed of oral microbes and a veritable culture medium of partially digested food.
The data analyses identify a number of suspected factors that might be associated with subsequent dementia. 17 The disease is associated with age and the data illustrate a consistent timeline for the relatively homogenous Taiwanese populace. The numbers of cases prior to age 60 are few but are twice as likely to be men and nearly all are VAD. After age 60, new cases increase rapidly with the incidence in women consistently surpassing men in every age bracket after age 60. The greater number of women mirrors an even greater female/male disparity reported by the Alzheimer’s Association in the United States.18,19 Some smaller studies did not always find a greater prevalence in women throughout the aging process but most found women were at higher risk.20–23 The sex disparity has been attributed in part to a survivor bias which suggests that men succumb to chronic diseases earlier in life than their female counterparts. Thus, following this early attrition, the remaining male populace is then disproportionately comprised of those with superior health and perhaps greater brain reserve providing greater resistance to dementia and delaying its perceived onset. This is not supported in the combined group because when the incidence between ages 60 and 85 is corrected for the national population by age and sex, the incidence rates are not different for men and women. Thus, it seems there are more women with dementia because there are more women in the aging population not because the surviving men are healthier.
The data reinforce significant dementia associations with coronary artery, peripheral artery, and cerebral artery (stroke) disease plus hypertension and diabetes. Since latter two conditions are major contributors to the prior three, cerebral perfusion issues must be considered a major contributing factor for dementia. Impaired perfusion of the brain may compromise the blood–brain barrier and facilitate further the entry of both infectious agents and/or humoral inflammatory mediators.
In addition to the established relationships among hypertension, diabetes and vascular disease, hypertension and diabetes are both associated with a general state of sub-clinical systemic inflammation.24–27 Diabetes and coronary artery disease also have more specific known interrelationships with inflammatory periodontal disease.28,30 In each case, these comorbidities were associated with significant odds for VAD and SAD in both men and women. Of these comorbidities, stroke was most prominently associated with the outcome among the VAD subgroup for both men and women by a similarly wide margin.
Exposure to two of the proposed microbial offenders, pneumonia and HSV, were evaluated. Pneumonia was consistently associated with the outcome across all groups, though 60% more problematic for men. In contrast, HSV was also positively related for men and women but the odds were concentrated in the SAD subgroup and were not significant for VAD. This difference in the distribution of the HSV-associated odds reinforces the distinct etiology of the two dementia variants. One concern in this regard is that the prevalence of diagnosed HSV (2–3%) in the database significantly underestimates the reported prevalence in the population based on random serological sampling. 29 The association between pneumonia and VAD may reflect the added influence of a reported association between pneumonia and cardiopulmonary disease. 31 However, the association between both pneumonia, HSV, and SAD provides additional support for participation by these microbes in the proposed microbial inflammatory hypothesis of dementia. Most discussants believe that a variety of microbes are likely to be involved, though access by a few primary microorganisms, may then facilitate the entry of a spectrum of secondary organisms. 1
The odds associated with dental or oral health are somewhat mixed and open to interpretation. Many routine dental procedures like fillings, scalings, gingivectomies, periodontics, and even oral surgeries were not consistently associated with a change in the overall odds though the odds often trended lower. Although dental amalgam has routinely been deemed safe and unrelated to AD,32,33 a modest trend for the association between AD and oral mercury containing amalgam has been proposed in this population. 34 Though the current analyses did not partition the filling materials by content, an association with the number of fillings was not identified. However, when treated as categorical variables, typical restorative dental care like root canals and limited numbers of extractions appears to be protective, lowering dementia odds ratios. When the recorded problems were frequent and/or severe as in large numbers of extractions or in periodontal emergencies, the odds rose. Perhaps the strongest evidence for better dental care resides with the costs of dental care. Based on a decade of care, the average costs are modest, yet the cost of dental visits and dental procedures were both associated with a significant reduction in odds of dementia.
In dramatic contrast, the cost of dental radiographic procedures appears to positively relate to SAD but again differentially not for VAD. This disparity between the costs of dental care and the costs of dental radiographic procedures strongly suggests the associated X-radiation may be independently associated with SAD. An alternative interpretation might suggest that greater radiology costs reflect more severe/chronic oral health issues. Although plausible, this latter concept seems less likely since the overall cost of dental care directly refutes that logic. Although, modern dental radiographic equipment is better collimated to focus and reduce the exposure, the convenience of the digital equipment may actually increase the number of images routinely acquired.
Based on the inflammatory hypothesis, the roles of three classes of pharmaceuticals were analyzed. These included anti-inflammatory steroids, NSAIDs, and antibiotics. The original thesis was that these drugs would lower the odds of dementia. However, the data do not support that concept. Increasing use or requirement for these drugs rather appears to be a hallmark of repeated infection and/or chronic inflammation. All three classes are associated with higher odds of total dementia. The notable exception was that NSAIDs and steroids were not an issue in the VAD subgroup. Antibiotics were specifically a problem for men especially within the VAD subgroup. This perhaps emphasizes again an underlying relationship between infection and cardiovascular disease. For some antibiotics, their access to the central nervous system may not have been sufficient to alter the resident microbial population within the brain. The analysis of specific antibiotics was beyond the scope of this study. Once again it is unlikely these drug associations are causative but more likely that they are symptomatic of an underlying chronic or repeated condition. High dose steroids may be a potential exception if their immunosuppressive activity is sufficient to allow the pathological biome to evade immune surveillance and thus, flourish.
Limitations
(1) As always, the analyses described here are able only to assess the association and though the data may support a cause and effect relationship, they cannot prove causality. The association with oral health may be mediated by other relationships. In this regard, those with better oral health may be more socially and physically active or enjoy a more nutritious diet. (2) The diagnoses were made based on clinical findings and not confirmed by post-mortem pathology, and thus the clinical diagnosis of SAD may overestimate the actual numbers. In contrast, cultural respect for the elderly in Taiwan may result in an underestimate in the actual incidence.31,35–38 However, given the very large sample size, these errors would presumable be relatively constant across groups. (3) When one makes a large number of comparisons, the probability of false positives rises. Several factors in the current study tend to mitigate this issue including the internally consistent findings across multiple regression models and frequent P-values that would meet much higher stringencies. (4) The study used available dental records for the decade preceding the index diagnoses and thus the assessments might differ if life-long records were available. While the data analyses are very precise, the interpretation of that data is necessarily qualitative given the multifactorial characteristics of Alzheimer’s disease.
Summary
The Taiwan National Insurance database allows for some very precise estimates of associations with dementia. Cardiometabolic and infectious disease are clear and potentially modifiable factors. Serious and/or recurrent oral health problems also appear to be positively associated with dementia. Consistent attention to oral healthcare appears to be associated with lower odds.37,39 These observations are consistent with the hypothesis that resident oral microbes participate in the development of dementia, particularly sporadic Alzheimer’s disease. The NHI dental records do not include the mundane daily hygiene practiced by the populace. Simple measures such as daily brushing, flossing, and using antimicrobial mouthwash are increasingly difficult for cognitively impaired patients and may represent an easy and important point of intervention. Thus, routine oral hygiene may be strategically important with respect to both the development of dementia and its subsequent rate of progression especially for dementia patients who have increasing difficulty with their daily routine. Since prophylaxis is absolutely critical, carefully controlled studies or well-designed retrospective surveys of routine dental hygiene could be very useful for public health advice and planning.
Footnotes
Authors’ contributions
All authors made substantive contributions to the design of the study and construction of the manuscript.
DECLARATION OF CONFLICTING INTERESTS
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
FUNDING
The study was supported by grants from Ministry of Science and Technology, Taiwan (107–2221-E-002–151-), and National Taiwan University Hospital Yunlin Branch, Taiwan (NTUHYL104.A001, NTUHYL106.A001).