
Abstract
Diabetes mellitus, particularly type 2 occurs at global epidemic proportions and leads to cardiovascular diseases. Molecular studies suggest the involvement of epigenetic alterations such as histone code modification in the progression of cardiometabolic disorders. However, short chain fatty acids (SCFAs) are recognized as epigenetic modulators by their histone deacetylase inhibitory property. It is therefore hypothesized that cardiac histone deacetylase activity increases in type II diabetes and SCFA, acetate, would inhibit histone deacetylase with accompanying restoration of glucose dysregulation, cardiac lipid deposition, and tissue damage in male Wistar rats. Twenty-four male rats (240–270 g) were allotted into four groups (n = 6 per group) namely: vehicle-treated (p.o.), sodium acetate-treated (200 mg/kg), diabetic, and diabetic+sodium acetate-treated groups. Diabetes was induced by intraperitoneal injection of streptozotocin 65 mg/kg after a dose of nicotinamide 110 mg/kg. The results showed that diabetic rats had, glucose dysregulation, elevated serum and cardiac triglyceride, malondialdehyde, alanine aminotransferase, histone deacetylase, serum aspartate transaminase, cardiac low density lipoprotein cholesterol (LDLc), glutathione/glutathione disulphide ratio (GSH/GSSG), reduced serum and cardiac high density lipoprotein cholesterol (HDLc), and serum GSH/GSSG. Histological analysis revealed disrupted cardiac fiber in diabetic rats. However, sodium acetate attenuated glucose dysregulation and improved serum and cardiac GSH/GSSG. Sodium acetate normalized cardiac triglyceride accumulation, malondialdehyde, serum aspartate transaminase levels and prevented cardiac tissue damage in diabetic rats. These effects were associated with suppressed histone deacetylase activity. Therefore, sodium acetate attenuated but failed to normalize glucoregulation. Nevertheless, it ameliorated oxidative stress- and lipid dysmetabolism-driven cardiovascular complications in diabetic rats by the suppression of histone deacetylase activity.
Impact statement
This study provides evidence that STZ-NA-induced diabetes mellitus is associated with cardiac triglyceride accumulation and tissue disruption with corresponding increase in cardiac HDAC activity. However, sodium acetate suppresses cardiac HDAC activity and normalizes cardiac triglyceride and tissue integrity in diabetic rats. Therefore, the study suggests that sodium acetate is beneficial for cardioprotection in diabetes mellitus.
Keywords
Introduction
Glucose dysregulation by insulin resistance (IR), a condition in which normal insulin level cannot sufficiently maintain normoglycemia due to reduced tissue sensitivity to insulin action. It is classically linked to type 2 diabetes (T2DM) and cardiovascular disease (CVD)1,2 which are the leading causes of death globally. Also, reduction in insulin secretion which can stem from chronic T2DM or autoimmune destruction of pancreatic β-cells (type 1 diabetes mellitus; T1DM) leads to fatal consequences. With underlying glucose dysregulation, both T1DM and T2DM are chronic diseases often associated with macrovascular and microvascular complications including CVD, 3 diabetic neuropathy 4 kidney impairment, 5 and retinal degeneration. 6 The prevalence of diabetes and its associated complications is growing rapidly ranking as the fifth leading cause of death worldwide. The American Diabetes Association reckons that 1.7 million Americans are diagnosed with diabetes yearly and is considered to double by 2030.7,8 Hence, studying the multi-factorial nature of diabetes mellitus and its progression to fatal conditions, especially CVD, with the aim of characterizing novel safer and more effective therapies is of great relevance to its prevalence.
Diabetes is heritable and its incidence may feature compelling family history. However, aside genetics, environmental factors like nutritional challenge, aging, obesity, and sedentary lifestyle are the risk factors for diabetes and are involved in its pathogenesis.9,10 Nevertheless, some people with these risk factors do not develop diabetes or related diseases possibly due to the absence of genetic predisposition. Therefore, an individual’s susceptibility to the development of T2DM is suggested to rely on the activation of intracellular signaling pathways by environmental factors leading to epigenetic modifications that culminate in changes in gene expression. 11 Epigenetics has to do with altered gene function without any change in the nucleotide sequence. 12 An array of data supports the plausible role of epigenetic changes in the process of metabolic disturbance and diabetes-associated complications. 13
Epigenetic mechanisms that modulate gene expression include histone post-translational modifications, DNA methylation, and pathways mediated by non-coding RNA. Histone post-translational modifications, histone acetylation, and methylation control gene expression via chromatin remodeler, transcription co-repressor, and co-activator recruitment and play significant roles in the progression of diabetes. 14 Histone acetyltransferases (HATs) catalyzes the process of histone acetylation with eventual recruitment of co-activators and chromatin remodelers. Conversely, histone deacetylases (HDACs) catalyze the removal of the acetyl group and can associate with co-repressor complexes creating close interactions between the DNA and the lysine-rich histone tails. This leads to inhibition of gene expression. HDAC is located at 6q21 chromosomal region which is linked to both T1DM and T2DM. 15
Products from colonic microbiota fermentation of nutritional digestible fibers, short chain fatty acids (SCFAs),16–18 are constituted largely by acetate, propionate, and butyrate, making up approximately 90% of the SCFAs present in the colon. 16 Acetate is the most abundant SCFA in the colon (65%) and circulation. 19 Ameliorative effects of SCFA on kidney disease, airway disease, and metabolic syndrome in diet-induced obesity have been reported in animals and humans.20–22 Reports also showed that acetate decreased the lipopolysaccharide-induced production of intracellular reactive oxygen species (ROS) concomitant with an increase in glutathione. 23 Sodium acetate comparably with androgen receptor blockade has been shown to inhibit cardiac overexpression of endoglin 24 and improve the deteriorated glucose homeostasis and antioxidant defenses induced by gestational androgen excess in experimental animals. 25 Besides, SCFAs have been reported to affect epigenetic gene regulation in obesity and other insulin resistance-linked complications through activation of transmembrane cognate G protein-coupled receptors which stimulate the release of protein YY and glucagon-like-peptide that maintain energy homeostasis, improve insulin sensitivity, and reduce visceral adiposity.17,18,26 Moreover, its potent anti-inflammatory and anti-oxidant effects on immune cell functions in human and experimental rodents have been recently demonstrated.27,28 Similarly, the beneficial effect of SCFAs may also be through the inhibition of HDAC activity and the activation of olfactory receptors.27–29 These reports and many others elucidate the beneficial effects of SCFAs in obesity, atherosclerosis and renal ischemic reperfusion-induced hypertension. However, considering the dearth of information on the therapeutic effect of acetate in overt diabetes mellitus, the present study was designed to investigate the ameliorative effect of sodium acetate in diabetic rats. The study also evaluated the involvement of HDAC activity and its probable interaction with sodium acetate in diabetes mellitus.
Materials and methods
Animals
Twenty-four male Wistar rats weighing 240–270 g were procured from the animal house of the College of Health Sciences, Afe Babalola University, Ado-Ekiti. Rats had unrestricted access to standard rat chow and tap water. The investigation was conducted in accordance with the National Institutes of Health Guide for the Care and Use of Laboratory Animals. After one week of acclimatization, the animals were randomly assigned to four groups (n = 6/group) namely; control, sodium acetate (SAC), diabetic (DIB), and DIB+SAC groups. Rats were maintained in a colony under standard environmental conditions of temperature, relative humidity, and dark/light cycle.
Induction of diabetes mellitus
Diabetes was induced in overnight fasted rats by the intraperitoneal injection of streptozotocin (STZ; 65 mg/kg) 15 min after a dose of nicotinamide (NA; 110 mg/kg). After 72 h of streptozotocin and nicotinamide administration, glycemic levels were determined and rats with glycemic levels higher than 12 mmol/L were considered diabetic and used for the experiment.
Treatment
Control group received vehicle (0.3 mL of distilled water; p.o.), SAC-treated group received SAC (200 mg/kg; p.o.), DIB group received distilled water, and SAC+DIB received SAC. The treatment was done daily for six weeks. Initial and final body weights were determined, and weight change was estimated as the difference between final and initial body weights.
Oral glucose tolerance test and insulin resistance
The glucose tolerance test was performed 48 h prior to the sacrifice of the rats. The rats had 12-h overnight fast. Animals were loaded with glucose (2 g/kg; p.o.). Blood was obtained from the tail before glucose load and then sequentially at 30, 60, 90, and 120 min. Glycemic levels were determined with a hand-held glucometer (ONETOUCH®-LifeScan, Inc., Milpitas, CA, USA). IR was determined using the homeostatic model assessment for IR (HOMA-IR= fasting glucose (mmol/l)×fasting insulin (µIU/l)/22.5), while pancreatic beta-cell function was assessed by HOMA-β, which is expressed as [20×fasting insulin (µIU/l)/fasting blood glucose (mmol/l) minus 3.5] as previously described.30,31
Sample preparation
At the end of the treatment, the rats were anesthetized with sodium pentobarbital (50 mg/kg, i.p.). Blood sample was collected by cardiac puncture into non-heparinized tube and was centrifuged at 3000 rpm/min for 5 min. Serum was collected and stored frozen until needed for biochemical assay. The heart was excised, cleared of adhering connective tissues, blotted and weighed immediately. After weighing, 100 mg of the heart was carefully removed and homogenized with a glass homogenizer in phosphate buffer solution.
Estimation of cardiac mass
Cardiac mass was determined from heart weight normalized to tibial length.
Biochemical assays
Serum insulin
Serum insulin was determined using ELISA kits obtained from Ray Biotech, Inc. (Georgia, USA) in compliance with the manufacturer’s procedure. This method is based on the direct sandwich technique in which two monoclonal antibodies are directed against separate antigenic determinants on the insulin molecule.
HDAC level
HDAC level was determined from the serum and cardiac homogenate using ELISA kits obtained from Ray Biotech, Inc. (Georgia, USA).
Lipid profile
Triglyceride (TG), total cholesterol (TC), high density lipoprotein (HDLc), and low density lipoprotein (LDLc) were estimated from the cardiac homogenate by the standardized colorimetric methods using reagents obtained from Randox Laboratory Ltd. (Co. Antrim, UK).
Lipid peroxidation and glutathione content
Serum and cardiac malondialdehyde (MDA) were determined by the standard spectrophotometric method using assay kits obtained from Randox Laboratory Ltd. (Co. Antrim, UK) and in adherence to the manufacturer’s instruction. While oxidized glutathione (GSSG) and reduced glutathione (GSH) were determined by the standard spectrophotometric method using the reagent kits obtained from Oxford Biomedical Research Inc. (Oxford, USA). Reduced to oxidized glutathione ratio (GSH/GSSG) was estimated as an indicator of antioxidant capacity. Nitric oxide (NO) was determined using the non-enzymatic colorimetric assay kits from Oxford Biomedical Research Inc. (Oxford, USA).
Tissue injury markers
Aspartate transaminase (AST) and alanine aminotransferase (ALT) activities were determined from serum and cardiac homogenate by the standard spectrophotometric method and the assay reagents were obtained from Randox Laboratory Ltd. (Co. Antrim, UK).
Histology studies
For Masson’s Trichrome and hematoxylin and eosin (H & E) stains, hearts were fixed in 10% formolsaline overnight, dehydrated, and embedded in paraffin. The paraffin-embedded samples were sectioned at 5-μm thickness. The slides were prepared and examined using light microscopy (Nikon Eclipse 80i, Nikon, Japan).
Data analysis and statistics
All data were expressed as means ± SEM. Statistical group analysis was performed with SPSS statistical software 22.0. One-way analysis of variance (ANOVA) was used to compare the mean values of variables among the groups. Bonferroni’s test was used to identify the significance of pair wise comparisons of mean values between the groups. Statistically significant differences were accepted at P less than 0.05.
Results
SAC improved body weight and cardiac mass in streptozotocin–nicotinamide-induced diabetic rats
Diabetes mellitus in this animal model significantly reduced the body weight and cardiac mass when compared with control and these were improved by the SAC treatment (Table 1).
Effects of sodium acetate on body weight and heart weight in streptozotocin–nicotinamide-induced diabetic rats.
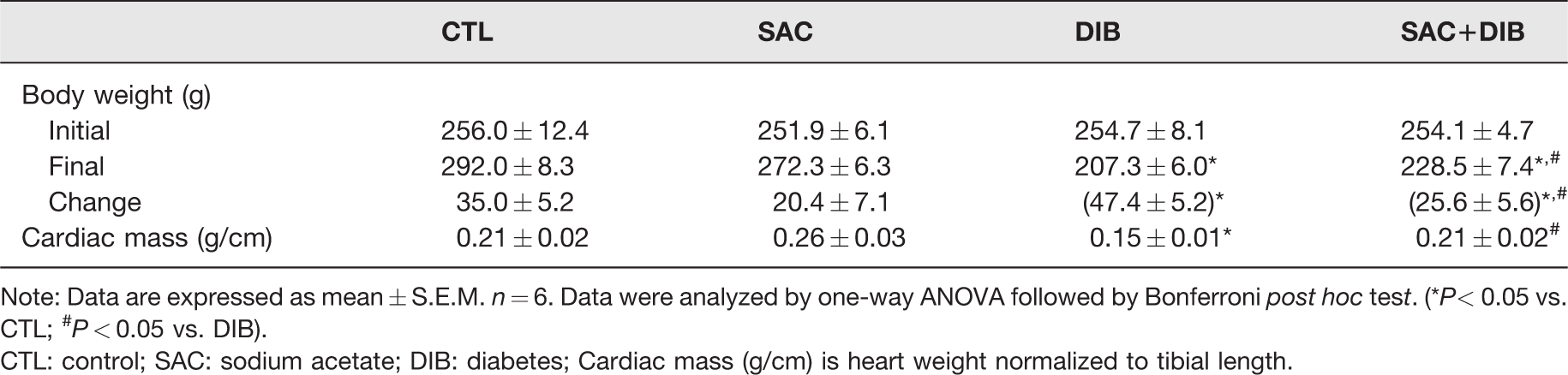
Note: Data are expressed as mean ± S.E.M. n = 6. Data were analyzed by one-way ANOVA followed by Bonferroni post hoc test. (*P< 0.05 vs. CTL; #P < 0.05 vs. DIB).
CTL: control; SAC: sodium acetate; DIB: diabetes; Cardiac mass (g/cm) is heart weight normalized to tibial length.
SAC improved insulin sensitivity but not insulin secretion in streptozotocin–nicotinamide-induced diabetic rats
Fasting blood glucose, 1-h post-load glycemia, serum insulin, and HOMA-IR were increased in diabetic rats when compared with control group. However, treatment with SAC reduced these alterations. In addition, diabetic+SAC-treated rats had increased fasting glycemia, 1-hr post-load glycemia, HOMA-IR but unaltered serum insulin level compared to control group (Figure 1(a) to (c)). This implies that treatment with SAC reduces but does not normalize hyperglycemia, impaired glucose tolerance, insulin resistance in diabetic rats when compared with control group. In addition, pancreatic beta-cell functions as indicated by HOMA-β were reduced in diabetic rats with or without sodium acetate when compared with control rats (Figure 1(d)).
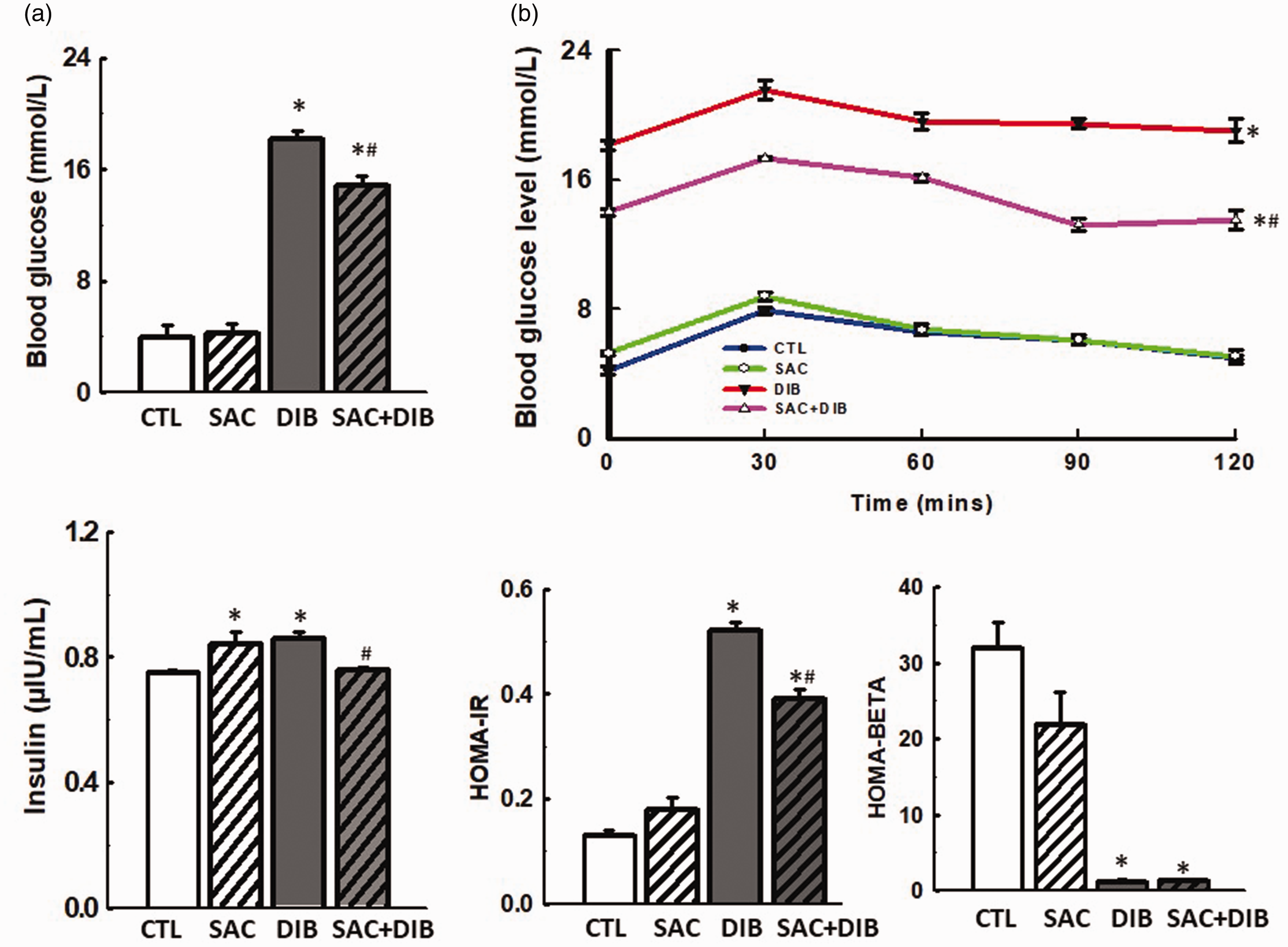
Effects of sodium acetate (SAC) on glucoregulatory parameters (a–d) in streptozotocin–nicotinamide-induced diabetic rats. Diabetes mellitus increased blood glucose, glucose intolerance, plasma insulin, and caused insulin resistance, which were attenuated but not normalized by SAC. However, pancreatic beta-cell functions were reduced in diabetic with or without sodium acetate. Data are expressed as mean ± S.E.M. n = 6. Data were analyzed by one-way ANOVA (a, c, and d) and repeated measures ANOVA (b) followed by Bonferroni post hoc test. (*P < 0.05 vs. control (CTL); #P < 0.05 vs. DIB; diabetes). (A color version of this figure is available in the online journal.)
SAC restored cardiac TG accumulation in streptozotocin–nicotinamide-induced diabetic rats
Serum and cardiac TG but not TC was significantly increased in diabetic rats when compared with control group, which was normalized when treated with SAC. Likewise, serum and cardiac HDL-C significantly decreased but LDLc was unaffected in diabetic rats when compared with control group. The disruption of HDLc was also restored by SAC (Table 2).
Effects of sodium acetate on lipid profile in streptozotocin-nicotinamide-induced diabetic rats.
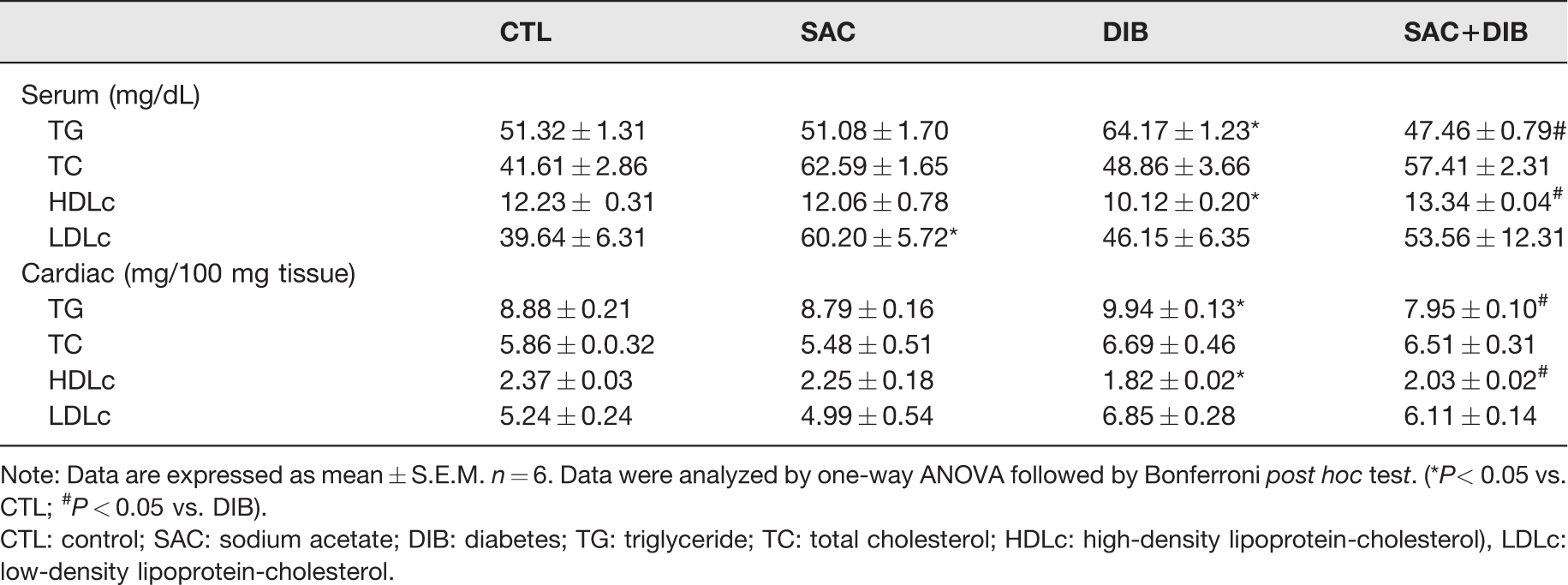
Note: Data are expressed as mean ± S.E.M. n = 6. Data were analyzed by one-way ANOVA followed by Bonferroni post hoc test. (*P< 0.05 vs. CTL; #P < 0.05 vs. DIB).
CTL: control; SAC: sodium acetate; DIB: diabetes; TG: triglyceride; TC: total cholesterol; HDLc: high-density lipoprotein-cholesterol), LDLc: low-density lipoprotein-cholesterol.
SAC attenuated lipid peroxidation and enhanced cardiac antioxidant defense in streptozotocin–nicotinamide-induced diabetic rats
Serum and cardiac MDA and cardiac GSH/GSSG were increased compared to control in diabetic rats, whereas serum GSH/GSSG ratio was reduced in diabetic rats compared to control. The rats treated with SAC only did not show any change in serum and cardiac MDA compared with control (Figure 2(a) and (b)). However, serum GSH/GSSG ratio increased, while cardiac GSH/GSSG ratio reduced in SAC-treated rats compared with control. Diabetic+SAC-treated rats showed lowered cardiac and serum MDA compared with untreated diabetic rats (Figure 2(a) and (b)). SAC treatment also improved GSH/GSSG antioxidant defense in diabetic rats compared with untreated diabetic rats (Figure 2(d)).
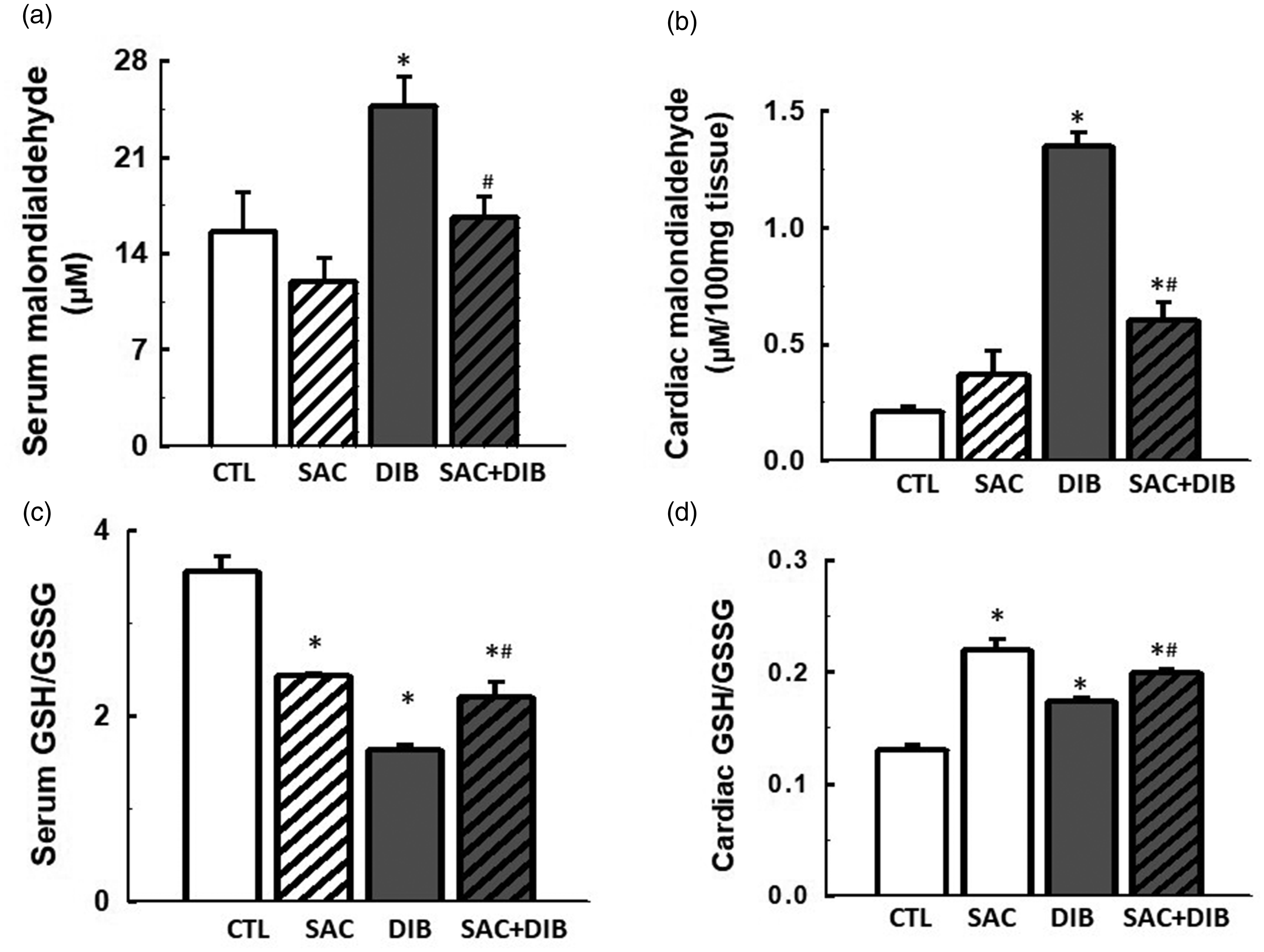
Effects of sodium acetate (SAC) on serum and cardiac lipid peroxidation biomarker (a, b), and glutathione-dependent antioxidant defense (c, d) in streptozotocin–nicotinamide-induced diabetic rats. Diabetes mellitus increased lipid peroxidation marker (MDA) and decreased GSH/GSSG, which were attenuated by SAC. Data are expressed as mean ± S.E.M. n = 6. Data were analyzed by one-way ANOVA followed by Bonferroni post hoc test. (*P < 0.05 vs. control (CTL); #P < 0.05 vs. DIB; diabetes).
SAC attenuated cardiac tissue injury in streptozotocin–nicotinamide-induced diabetic rats
This animal model of diabetes mellitus significantly increased serum and cardiac ALT when compared with control group, which were attenuated by SAC. However, serum AST but not cardiac AST was significantly increased in diabetic rats when compared with control and treatment with SAC improved the alteration (Table 3).
Effects of sodium acetate on tissue function enzyme markers in streptozotocin-nicotinamide-induced diabetic rats.
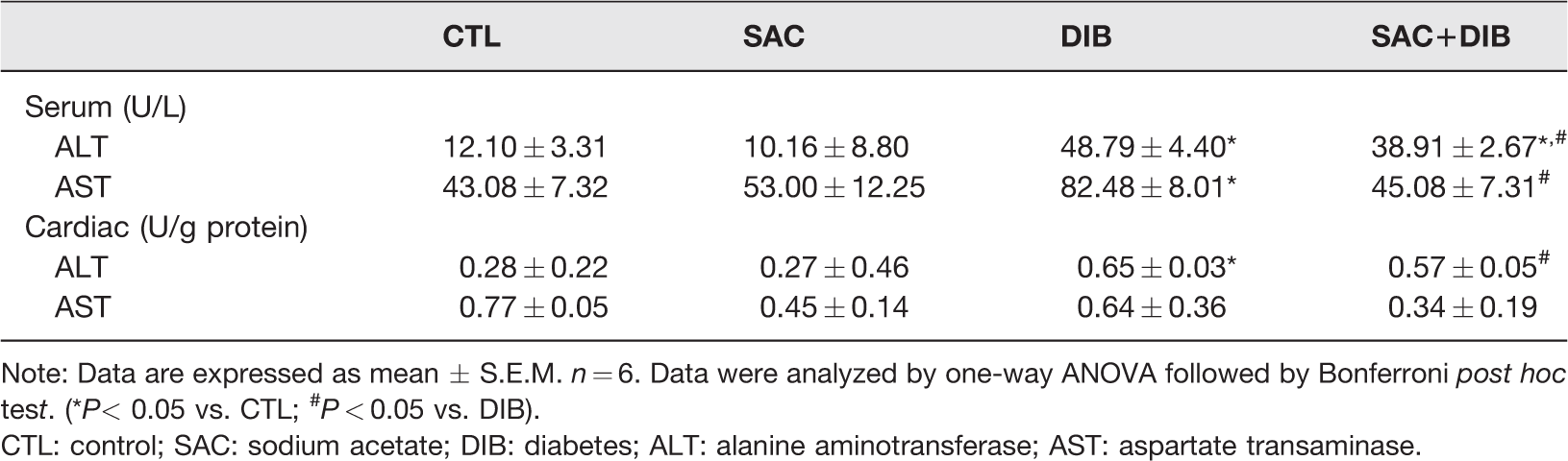
Note: Data are expressed as mean ± S.E.M. n = 6. Data were analyzed by one-way ANOVA followed by Bonferroni post hoc test. (*P< 0.05 vs. CTL; #P < 0.05 vs. DIB).
CTL: control; SAC: sodium acetate; DIB: diabetes; ALT: alanine aminotransferase; AST: aspartate transaminase.
SAC normalized cardiac tissue integrity in streptozotocin–nicotinamide-induced diabetic rats
Histological analysis of the cardiac tissue showed disrupted cardiac muscle fibers with tissue fibrosis and cellular infiltration in diabetic rats (Figure 3(c)) compared with control that showed normal cardiac muscle fibers (Figure 3(a)). Besides, rats treated with SAC only showed normal cardiac tissue architecture (Figure 3(b)), whereas, SAC restored the altered cardiac tissue architecture of diabetic rats (Figure 3(d)). H and E staining technique also confirmed disrupted cardiac muscle fibers in diabetic rats (Figure 4(c)) and restored cardiac muscle fibers with mild cellular infiltration in diabetic rats treated with SAC (Figure 4(d)).
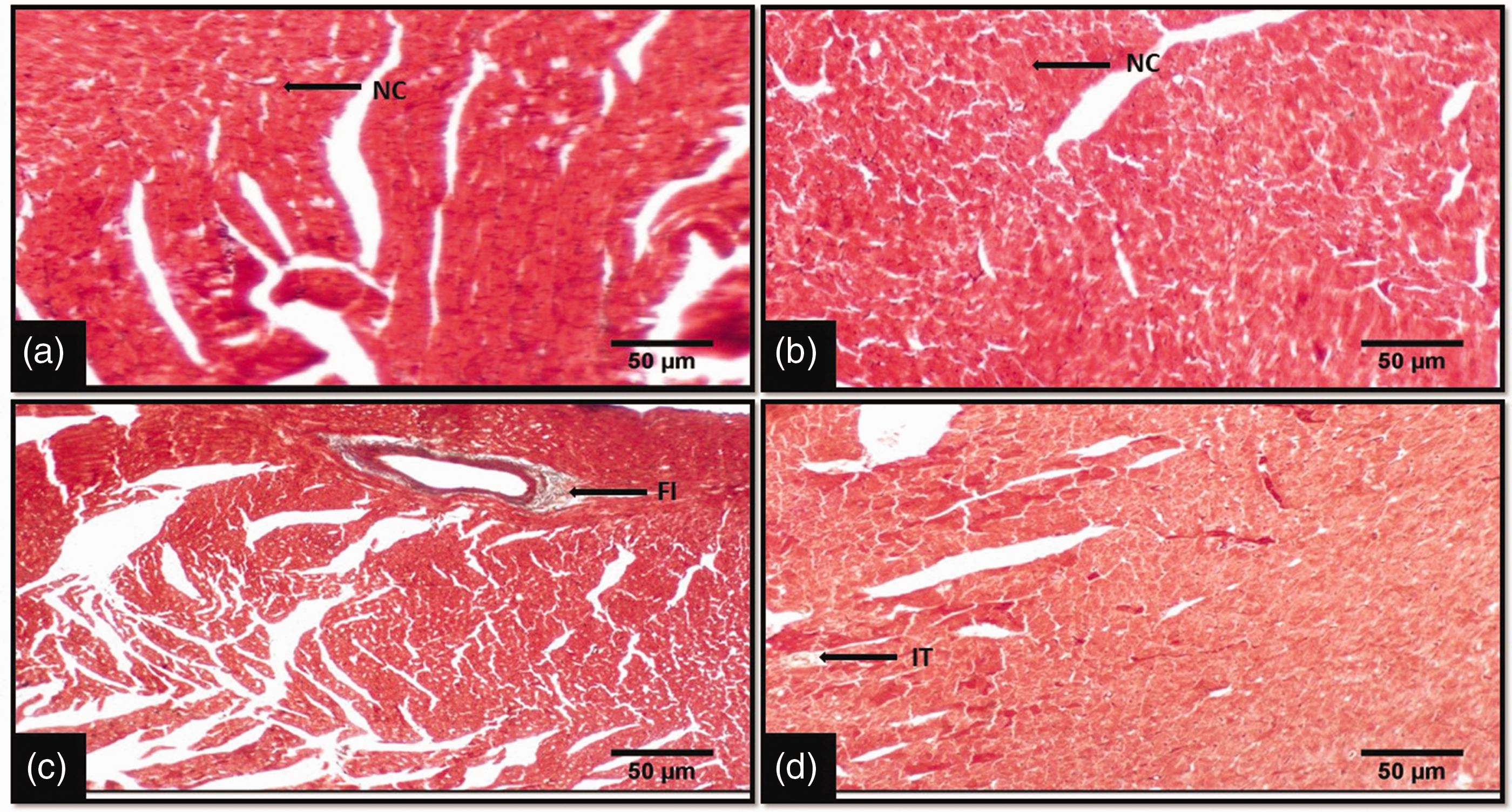
The histology of the heart using Masson’s Trichrome staining technique showed cardiac tissue with normal cardiac muscle fibers in control rat (a), normal cardiac muscle fibers in sodium acetate-treated rat (b), disrupted cardiac muscle fibers with fibrosis and cellular infiltration in diabetic rat (c) and improved cardiac muscle fibers with mild cellular infiltration in diabetic rat treated with sodium acetate (d), (×200, Longitudinal section). NC: normal cardiac muscle; FI: fibrosis; IT: cellular infiltration. (A color version of this figure is available in the online journal.)
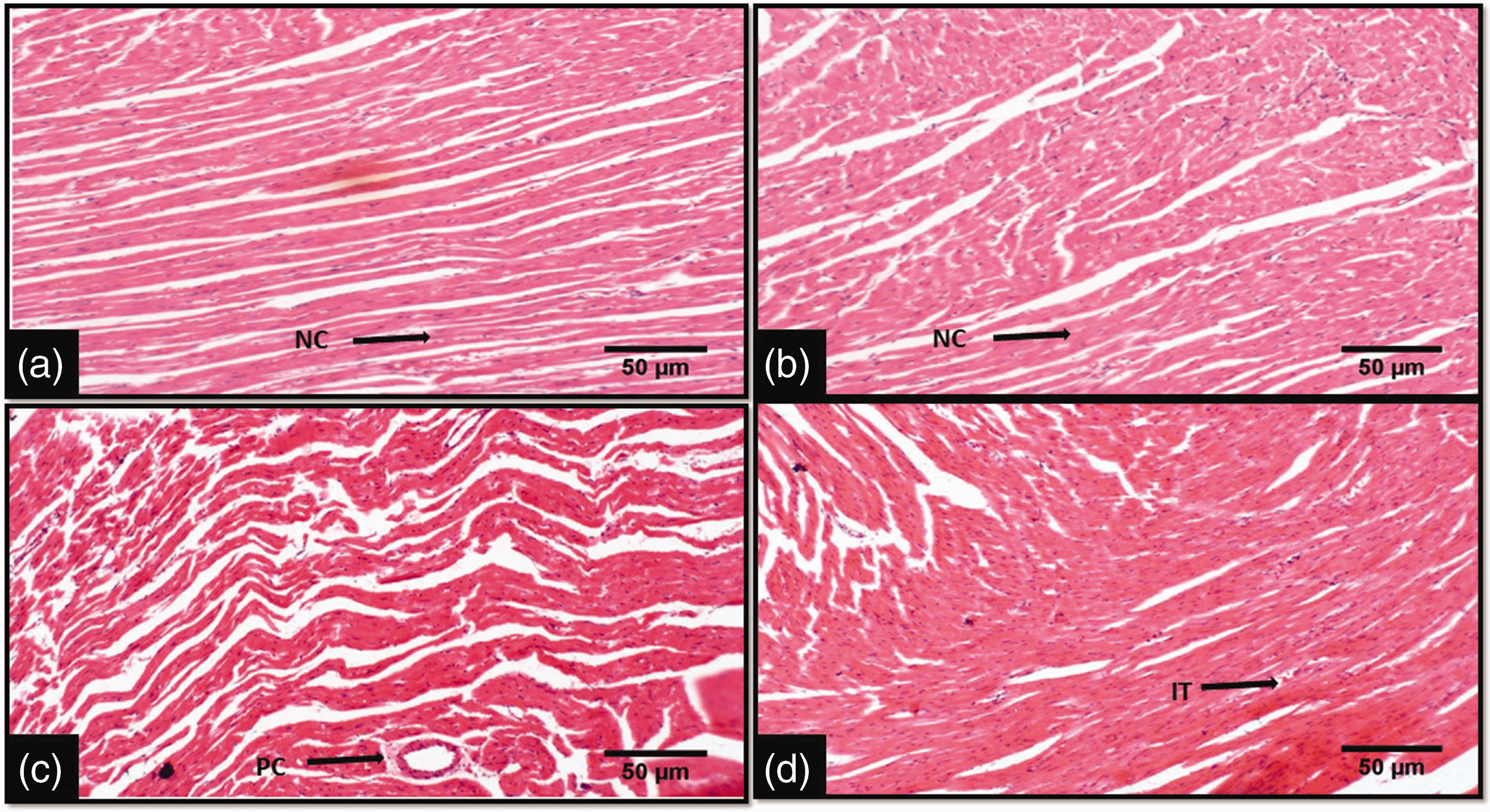
The histology of the heart using H and E staining technique showed normal cardiac muscle fibers in control and sodium acetate-treated rats (a, b), perturbed cardiac muscle fibers with cellular infiltration in diabetic rat (c) and improved cardiac muscle fibers with mild cellular infiltration in diabetic rat treated with sodium acetate (d), (×200, Longitudinal section). NC: normal cardiac muscle; IT: cellular infiltration; PC: perturbed cardiac muscle fibers. (A color version of this figure is available in the online journal.)
SAC reduces cardiac HDAC level in streptozotocin–nicotinamide-induced diabetic rats
Serum and cardiac HDAC levels increased significantly in diabetic rats compared with control (Figure 4). Whereas there was no alteration in both serum and cardiac HDAC in SAC-treated rats compared with control. However, treatment of diabetic rats with SAC reduced serum and cardiac HDAC levels compared with untreated diabetic rats.
Discussion
The present study demonstrated overt diabetes mellitus in Wistar rats showing elevated fasting blood glucose (approximately 3-fold), 1-h post-load glycemia, and HOMA-IR and significant increase in fasting insulin (Figure 1). Hyperglycemia and hyperinsulinemia are critical to the onset of diabetes mellitus-associated complications. They are important metabolic signals that result in severe pathological processes like oxidative stress, inflammatory responses, fibrosis, neuropathy, and eventual CVD. 21 Although, insulin and glucose levels were elevated, while pancreatic beta-cell function was impaired in diabetic rats in the present study. This shows that the STZ-NA-induced diabetes mellitus model features degenerating pancreatic β-cells which cannot adequately respond to glucose-dependent insulin secretion. Therefore, this study achieved a deteriorated β-cell-mediated chronic hyperglycemia which led to evident cardiometabolic derangement. The elevated serum insulin concentration in the diabetic animals may be due to reduced insulin clearance, and hyperinsulinemia has been earlier reported to independently trigger cardiac events in insulin resistance-linked complications.32–34
Aside elevated blood glucose especially due to impaired pancreatic β-cell, IR is associated with increased circulating TG and ectopic TG accumulation. This occurs as a result of increased lipolysis in adipose tissue, leading to increased circulation and influx of lipid into non-adipose tissue. Lipid deposition in non-adipose tissues agreeably culminates in local IR, oxidative stress, mitochondrial dysfunction, inflammatory response, and fibrosis 35 which lead to loss of tissue integrity. In this study, serum and cardiac TG increased in diabetic rats (Table 2). This outcome is accompanied by increased serum and cardiac MDA (Figure 2(a) and (b)), a marker of lipid peroxidation and evidence of oxidative stress with correspondent increased serum and cardiac ALT, a marker of tissue injury (Table 3) and decreased serum but increased cardiac GSH/GSSG ratio (Figure 2(c) and (d)). The elevated cardiac GSH/GSSG ratio might be a compensatory response to protect the cardiac tissue from the progressive oxidative damage. Tissue oxidative stress is injurious and activates inflammatory responses which promote cellular infiltrations, fibrosis, and loss of normal tissue architecture. Histological analysis here shows that diabetic rats demonstrated disrupted cardiac tissue with evidence of cardiac fibrosis and cellular infiltration (Figure 3(c)) and reduced cardiac muscle fibers (Figure 4(c)) compared to normal rats. Collectively, this study shows that in STZ-NA-induced diabetes mellitus model, hyperglycemia and IR-induced lipid dysmetabolism synergistically establishes cardiac metabolic disturbance which is associated with oxidative stress and fibrotic responses.
Hyperglycemic signal and cardiac IR status possibly stimulate gene functions that culminate in a cascade of gene expression and repression which accentuates the epigenetic modifications associated with the initiation of diabetic complications. In line with this thought, increased cardiac HDAC activity was demonstrated in diabetic rats in this study (Figure 5(b)). Previous studies have shown the association of hyperglycemia in diabetes with increased activity of multiple histone acetyl transferase and acetylation leading to DNA transcription and expression of inflammatory genes. 36 Inflammatory molecules play vital roles in the induction of IR by disrupting the insulin signaling pathways, especially the rate-limiting insulin receptor kinase activity. Also, IR, after its onset is associated with reduced expression of glucose transporter 4 (GLUT 4), which has been linked to increased HDAC activity. 37 This glucose deregulation by tissue resistance to insulin worsens hyperglycemia especially when the pancreatic β-cells cannot adequately perform glucose-stimulated insulin secretion. Therefore, the findings here validate the involvement of epigenetic modifications especially HDAC activity in the progression of diabetes mellitus to cardiac metabolic perturbations. This status corresponded with cardiac tissue damage and reduced cardiac mass, which might also be a reflection of retarded cardiac growth in diabetic animals. These findings are in consonance with previous studies.35,36 Hence, inhibition of HDAC activity might prevent or delay the onset of IR/hyperinsulinemia-driven cardiac complications in diabetic animals.
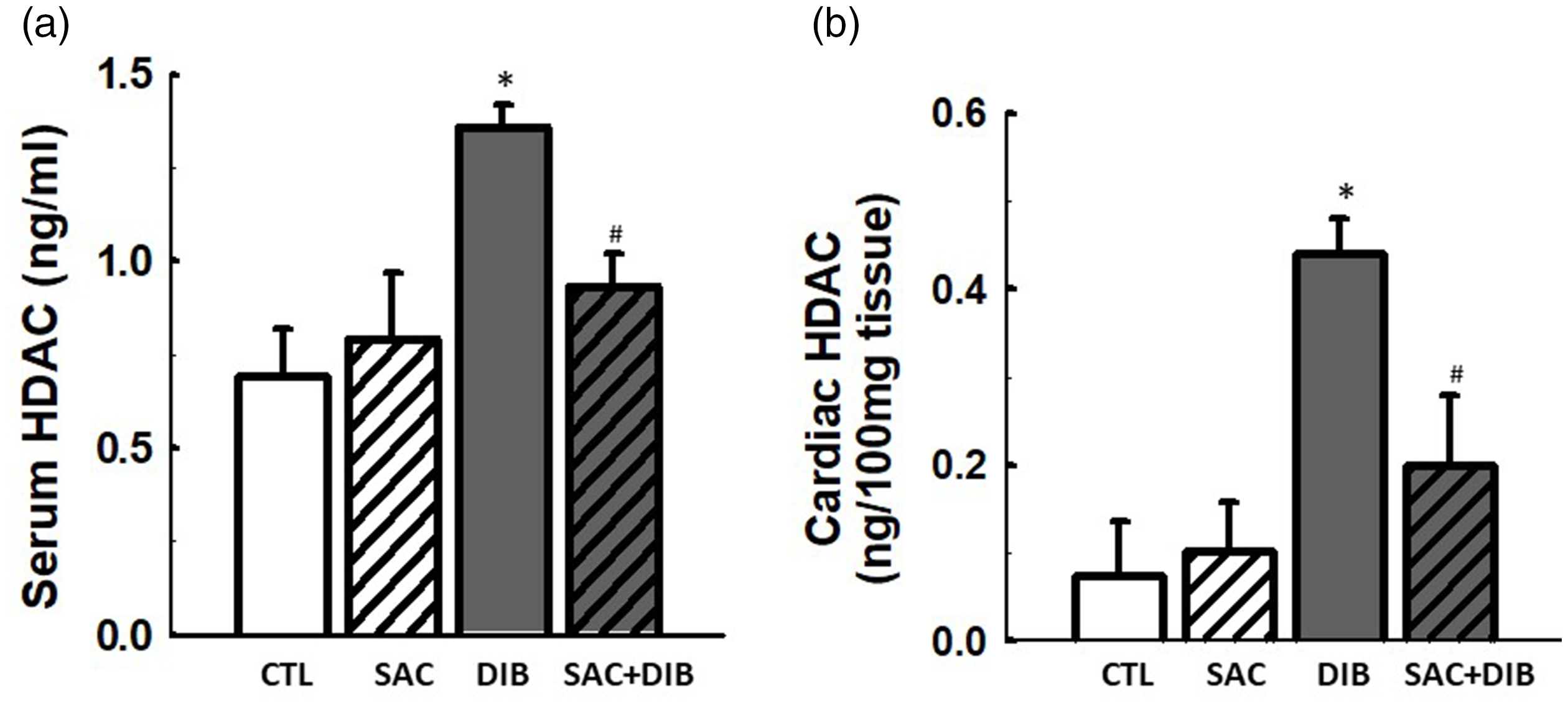
Effects of sodium acetate (SAC) on serum and cardiac histone deacetylase (HDAC (a) and (b)) in streptozotocin-nicotinamide-induced diabetic rats. Diabetes mellitus increased HDAC, which was decreased by SAC. Data are expressed as mean ± S.E.M. n = 6. Data were analyzed by one-way ANOVA followed by Bonferroni post hoc test. (*P < 0.05 vs. control (CTL); #P < 0.05 vs. DIB; diabetes).
Interestingly, nutritional adjustment is a plausible non-pharmacological intervention for metabolic syndrome. Recently, SCFAs are regarded as nutrients of immense beneficial health impact. In the present study, the SCFA, acetate treatment to diabetic rats attenuated glucose dysregulation (fasting glycemia, 1-h post-load glycemia and HOMA-IR) with corresponding improvement in cardiac mass, lipid homeostasis, and tissue integrity. This outcome was accompanied by the suppressed cardiac HDAC activity (Figure 5(b)) which indicates firstly that acetate has considerable HDAC inhibitory property and secondly that HDAC inhibition in diabetes mellitus with deteriorating pancreatic β-cell might only attenuate but not normalize hyperglycemia. Histone deacetylase inhibition has been shown to improve insulin sensitivity by aiding expression of proteins involved in glucose uptake but may not improve glucose-stimulated insulin secretion from the pancreatic β-cell. 13 This may be the physiological basis behind the elevated blood glucose in diabetic rats treated with sodium acetate when compared with control group (Figure 1(a)). This result was accompanied by an insulin level comparable with the control in diabetic rats treated with acetate (Figure 1(c)). Taken together, the results demonstrate that β-cell is deteriorated in diabetic+SAC-treated rats but acetate improved peripheral insulin sensitivity with corresponding increase in glucose uptake as revealed by reduced glycemia compared with diabetic rats without acetate treatment. However, studies have shown that for β-cell function to secrete insulin is not only controlled by histone acetylation but also by histone and DNA methylation .38–40 Therefore, the HDAC inhibitory property of SCFAs can only increase acetylation in β-cells which though is not enough to improve β-cell insulin secretion in overt diabetes mellitus, it may beneficially improve peripheral insulin sensitivity.
Nevertheless, improving peripheral insulin sensitivity in overt diabetes mellitus especially in T2DM is an essential step to delay or prolong local IR and IR-driven complications. In the present study, the peripheral insulin sensitivity and hyperinsulinemia that were improved by acetate in diabetic rats led to improved cardiac mass, lipid homeostasis (Table 2), and tissue integrity (Figure 3). The link between acetate-driven peripheral insulin signaling (secondary to HDAC inhibition) and improved cardiac tissue lipid and structure in diabetic rats might possibly result from its ameliorative effect on lipid peroxidation (an indicator of oxidative stress), TG accumulation, and enhancement of HDLc. High density lipoprotein cholesterol has been shown to improve insulin signaling and glucose uptake through the regulation of adenosine monophosphate activated kinase.41,42 These outcomes show that deleterious cardiac complications associated with diabetes mellitus are accompanied by oxidative stress and lipid dysmetabolism leading to cardiac TG accumulation and SCFA, and acetate ameliorates these effects plausibly by suppression of HDAC activity with considerable improvement in insulin signaling and cardiac events (Figure 6). However, the limitation of the present study was that parameters such as heart rate, blood pressure, mitral flow profile, end systolic and diastolic volume, among others that directly reflect cardiac function was not measured. Nevertheless, cardiac mass and biochemical parameters especially cardiac cholesterol levels (HDLc and LDLc) have been previously documented as surrogate marker of cardiac function.43,44
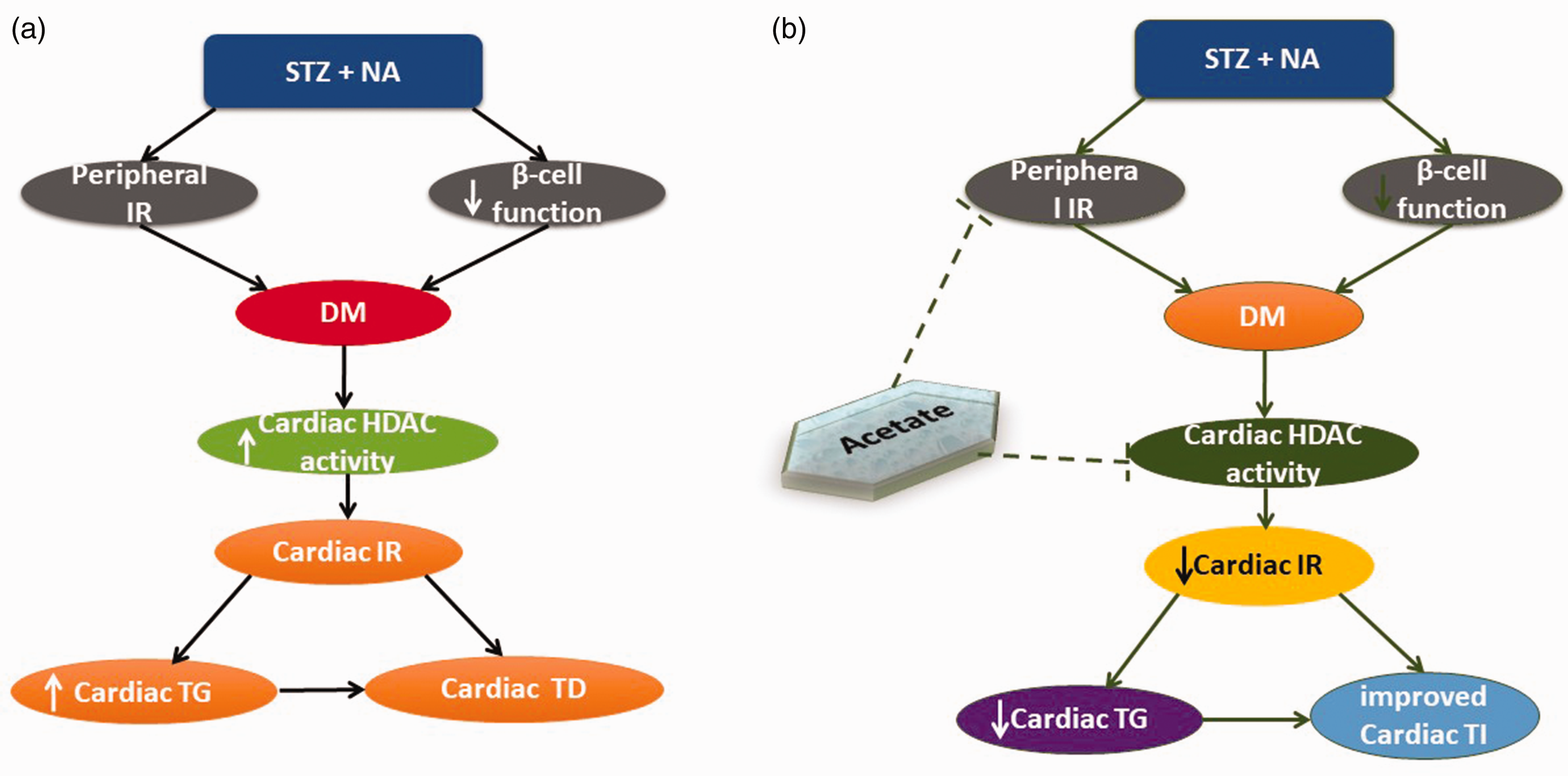
Schematic diagram depicting the pathways involved in the progression of streptozotocin (STZ)–nicotinamide (NA)-induced diabetes mellitus to cardiac metabolic and tissue disruption (a), and the ameliorative effects of sodium acetate on diabetes mellitus-induced cardiac complication by suppression of HDAC (b). Insulin resistance, triglyceride, tissue damage, and tissue integrity are designated as IR, TG, TD, and TI respectively. (A color version of this figure is available in the online journal.)
Conclusion
The present study demonstrates that diabetes mellitus with deteriorated β-cell function is associated with increased HDAC activity, and SCFA, acetate ameliorates cardiac events particularly tissue damage and TG accumulation accompanying diabetes mellitus by the suppression of HDAC activity. Therefore, SCFA, acetate is a plausible dietary therapeutic agent in diabetic conditions by its potential to augment insulin signaling and ameliorate local IR. Hence, nutritional modifications that incorporate acetate generating fiber-rich food intake might be beneficial to diabetic individuals.
Footnotes
Authors’ contributions
KSO and OAA conceived and designed the research. KSO and OAA conducted the experiments. LAO contributed to the new reagents and analytical kit. KSO and OAA analyzed and interpreted the data. KSO and EDA drafted the manuscript. KSO, OAA, EDA and LAO read, revised and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The protocol was approved by the Institutional Ethical Review Committee of Afe Babalola University, Ado-Ekiti, Nigeria.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.