
Abstract
Chronic obstructive pulmonary disease (COPD) is a heterogeneous inflammatory disease and eosinophils (EOS) participate in inflammation process. Acute exacerbation of COPD (AECOPD) is an inevitable trend in the development of the disease and has attracted widespread attention. In the present study, 108 hospitalized patients with AECOPD were collected and the levels of interleukin-13 and eosinophil cationic protein in the serum and sputum were measured to explore their clinical value in eosinophilic AECOPD patients. The patients were divided into an eosinophilic group (52 cases, 48.15%) and a noneosinophilic group (56 cases, 51.85%). The eosinophilic group had fewer acute exacerbations in the past year, shorter average hospitalization days, lower respiratory failure rate, mechanical ventilation utilization rate, and lower CAT and mMRC scores (P < 0.05). The levels of interleukin-13 and eosinophil cationic protein in sputum in the eosinophilic group were higher than those in the noneosinophilic group (P < 0.05), and there was no significant difference in the serum between the two groups (P > 0.05). The receiver operating characteristic (ROC) curves of sputum interleukin-13 and eosinophil cationic protein predicting peripheral blood EOS% ≥2% of AECOPD patients were statistically significant (P < 0.05). The noneosinophilic group had a higher rate of rehospitalization due to acute exacerbation during the one-year follow-up, and there was no significant difference in mortality between the two groups. The results show that eosinophils in peripheral blood are a simple, convenient, and inexpensive index for assessing the condition and prognosis of AECOPD patients. Interleukin-13 and eosinophil cationic protein are involved in the pathogenesis of eosinophilic AECOPD and may be the new targeted anti-inflammatory therapies in the future.
Impact statement
Acute exacerbation of chronic obstructive pulmonary disease (AECOPD) is an inevitable trend in the development of the disease and eosinophils (EOS) participate in inflammation process. It is important to explore some relatively simple biomarkers in AECOPD which are useful to recognize the disease. In the present study, 108 hospitalized patients with AECOPD were collected and the levels of IL-13 and ECP in the serum and sputum were measured. The levels of IL-13 and ECP in sputum in the eosinophilic group were higher than those in the noneosinophilic group. Moreover, the noneosinophilic group had a higher rate of rehospitalization due to acute exacerbation during the one-year follow-up. The results show that eosinophils in peripheral blood are a simple, convenient, and inexpensive index for assessing the condition and prognosis of AECOPD patients. IL-13 and ECP are involved in the pathogenesis of eosinophilic AECOPD and may be the new targeted anti-inflammatory therapies.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is a common disease characterized by persistent airflow limitation that can be prevented and treated. 1 Acute exacerbation of chronic obstructive pulmonary disease (AECOPD) is an inevitable trend in the development of the disease. The disability rate and mortality rate are extremely high, which seriously affects the labor ability and quality of life of patients. Because pulmonary function cannot essentially reflect the pathogenesis of COPD although it is a gold indicator for the diagnosis of this disease, it is particularly important to explore some relatively simple biomarkers that can recognize AECOPD.
Chronic airway inflammation is an important link in the pathogenesis of COPD, and COPD has great heterogeneity in inflammatory mechanisms. EOS has always been previously considered to be the main cell involved in asthma. 2 In recent years, a large number of studies have found that EOS also participates in chronic obstructive pulmonary airway inflammation, so eosinophilic AECOPD is of wide concern in the respiratory community.3,4 IL-13 and ECP are both cytokines related to EOS inflammation. A large number of animal experiments and clinical studies have shown that both IL-13 and ECP are involved in the pathogenesis of COPD.5,6 IL-13 may participate in the pathogenesis of COPD by regulating the expression of proinflammatory cytokines, upregulating adhesion molecules to activate EOS, and inducing B cell proliferation to produce IgE and goblet cells to secrete large amounts of mucus. 7 ECP is released after activation of EOS and then participates in airway inflammation through cytotoxicity. 8 In summary, previous studies have confirmed that the expression of IL-13 and ECP increased in patients with AECOPD and was proportional to the severity of the disease. However, there are few reports about the clinical value of IL-13 and ECP in eosinophilic AECOPD, and its pathogenesis needs to be further explored.
Based on the knowledge from above literatures, we hypothesize that IL-13 and ECP may participate in the pathogenesis of AECOPD, and represent the candidate biomarkers to assess the eosinophilic AECOPD patient’s condition and predict prognosis. The purpose of this study was to investigate the effect of IL-13 and ECP in serum and sputum on the condition and prognosis of hospitalized patients with eosinophilic AECOPD and their possible role in the pathogenesis of eosinophilic AECOPD. We aimed to prove the consistency of the evaluation by various biological specimens in a clinical setting, to further validate the application value of EOS in AECOPD, and to provide a new evaluation method and therapeutic target for eosinophilic AECOPD.
Materials and methods
Ethical approval
This study was reviewed and approved by the ethics committee of the First Hospital of Shanxi Medical University (No. SYDYY20170602). All subjects were informed and signed consent.
Subjects
The diagnosis of COPD met the 2017 Global Initiative for Chronic Obstructive Pulmonary Disease (GOLD) guidelines (http://goldcopd.com): FEV1/FVC <0.70 after inhalation of bronchodilators. Acute exacerbation refers to the acute deterioration of respiratory symptoms, leading to the need for additional treatment. Exclusion criteria were some other diseases, such as bronchial asthma, asthma-COPD overlap, eosinophilic bronchitis, and allergic rhinitis. In addition, patients with severe organic diseases and severe illnesses who cannot cooperate and patients with incomplete clinical data were excluded. We consecutively collected 108 hospitalized patients with AECOPD who met the enrollment and exclusion criteria from the Department of Pulmonary and Critical Care Medicine of the First Hospital of Shanxi Medical University between October 2017 and August 2018. The patients included 85 males and 23 females with an average age of 70.56 ± 9.31 years. According to the EOS % in peripheral blood, the patients were divided into an eosinophilic group (EOS % ≥2%) and a noneosinophilic group (EOS % <2%).
Clinical information
General information of all enrolled patients, including age, sex, smoking index, and body mass index, was collected. Meanwhile, clinical data including the number of acute exacerbations in the past year, the date of this hospitalization, the use of mechanical ventilation during hospitalization, and the symptom scores (CAT, SGRQ, CCQ, and mMRC questionnaire) were recorded. In addition, we followed the patient’s outcomes (rehospitalization due to acute exacerbations and mortality) one year after discharge by telephone.
Observation indicators and detection
The pulmonary function test was measured by the Jaeger Lung Functional Instrument, including the percentage of predicted forced expiratory volume in 1 s (FEV1%), percentage of predicted forced vital capacity (FVC %), and the ratio of FEV1 to FVC (FEV1/FVC). In this study, 47 patients with AECOPD completed pulmonary function tests before discharge.
At admission, radial or femoral artery blood was extracted by heparinized syringe from all subjects (without oxygen inhalation). The data were analyzed by a Danish ABL725 full parameter blood gas analysis. The type of respiratory failure was judged according to the partial pressure of arterial oxygen and partial pressure of carbon dioxide. In addition, the laboratory indicators of all subjects were collected, such as the blood cell count (including neutrophil, eosinophil, and lymphocyte absolute values and their percentages), sputum culture results, and biological indicators, including the neutrophil lymphocyte ratio (NLR), C-reactive protein (CRP), procalcitonin (PCT), and fibrinogen (FIB).
Serum and sputum sample detection
In the early morning, 5 mL of elbow venous blood from all subjects was collected and kept at room temperature for 30 min and then centrifuged at a speed of 3000 r/min for 10 min. The separated serum was withdrawn and placed in Eppendorf tubes and frozen in a freezer at −80°C for testing. Serum IL-13 and ECP levels were measured by enzyme-linked immunosorbent assay (ELISA). The kits were provided by Wuhan Boster Biological Preparations Company. The product numbers were EK0424 and HM10789. The procedures were strictly in accordance with the instructions.
There are two methods for the collection of sputum specimens. Patients who had sputum were instructed to rinse their mouths with clean water and cough deep sputum; patients without sputum were instructed to induce sputum examination formulated by the Chinese Medical Association Respiratory Diseases. First, the patients inhaled 3% hypertonic saline for 7 min with an ultrasonic nebulizer, and then the patient was asked to force a deep cough. If the sputum specimen was qualified, the atomization was terminated, and if not, hypertonic saline was continued until the collected sputum sample was qualified (weigh > 0.2 g, and the ratio of squamous epithelial cells to total cells was < 20% under low magnification). Next, three times the volume of 0.1% dithiothreitol solution was added to the qualified sputum sample, and the mixture was immersed in a water bath at 37°C for 10 min. The filter was filtered through a 300 mesh nylon filter and centrifuged at 3000 r/min for 10 min. Then, the supernatant was collected in an Eppendorf tube and frozen in a freezer at −80°C for testing. The methods for testing IL-13 and ECP in sputum were the same as those in serum. The remaining sediment was mixed, smeared, fixed, and stained. Finally, we classified 400 nonsquamous epithelial cells under light microscopy and calculated the percentage of neutrophils, macrophages, eosinophils, and lymphocytes.
Statistical analysis
SPSS 22.0 was used for analysis. The measurement data were expressed as the mean ± standard deviation. Two groups that met the normal distribution were compared by independent-samples Student’s t test. The count data were expressed as frequencies and percentages, and the rate was compared using the Chi-square test. Pearson correlation analysis was used to describe the correlation between EOS % in peripheral blood and IL-13 and ECP in serum and sputum. The ROC curve was used to analyze the value of sputum IL-13 and ECP in evaluating the prognosis of patients. A value of P < 0.05 was considered statistically significant.
Results
Comparison of clinical characteristics
Among all patients, there were 52 cases (48.15%) in the eosinophilic group and 56 cases (51.85%) in the noneosinophilic group. A comparison of the clinical characteristics between the two groups is shown in Table 1. There were no significant differences in age, smoking index, body mass index, FEV1%, FVC%, FEV1/FVC%, and the length of disease between the two groups (P > 0.05). Compared with the noneosinophilic group, men were more common in the eosinophilic group, with fewer acute exacerbations in the past year, a shorter average number of hospitalization days, a lower respiratory failure rate and mechanical ventilation utilization rate, and lower CAT and mMRC scores (P < 0.05).
Comparison of clinical characteristics.
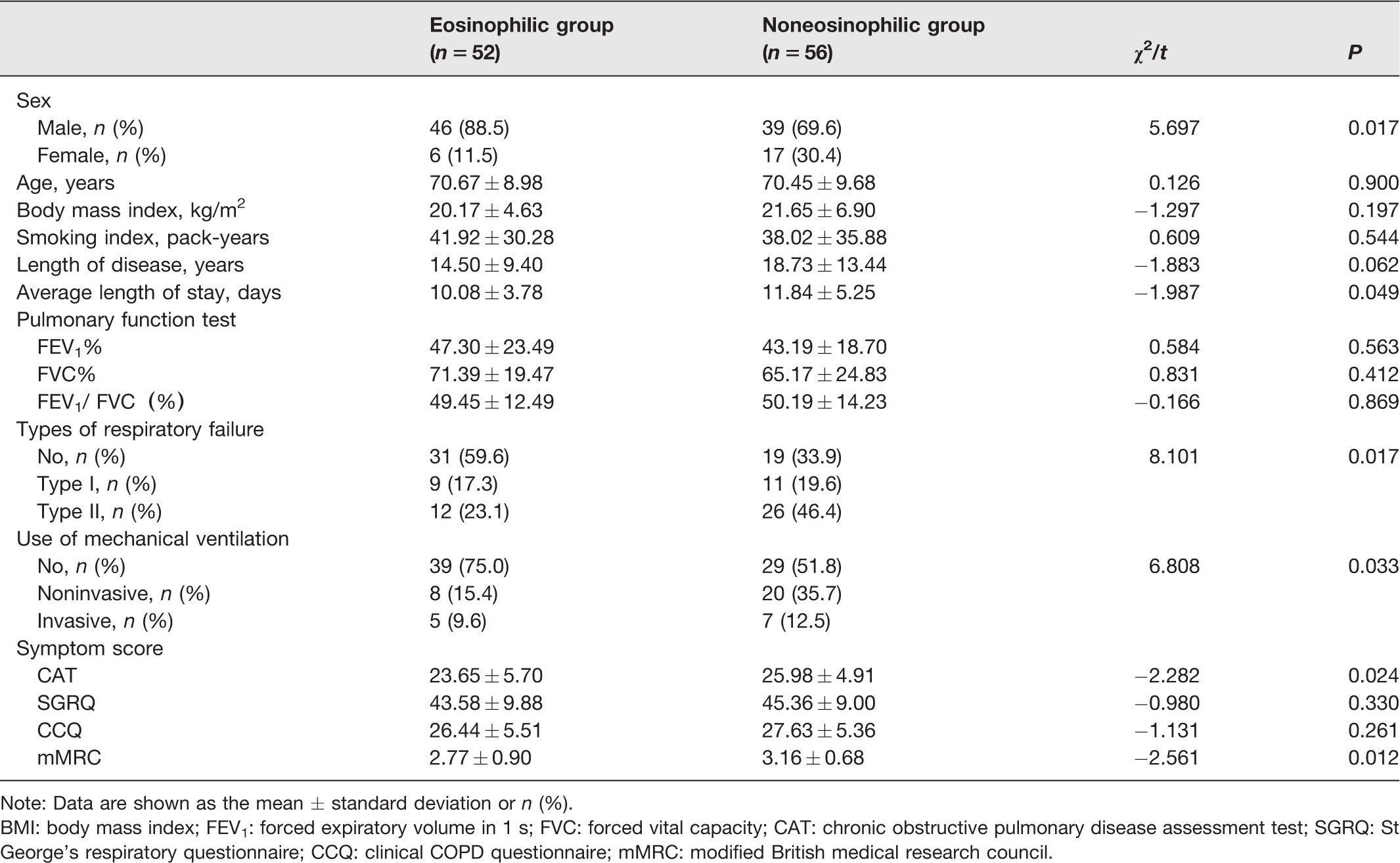
Note: Data are shown as the mean ± standard deviation or n (%).
BMI: body mass index; FEV1: forced expiratory volume in 1 s; FVC: forced vital capacity; CAT: chronic obstructive pulmonary disease assessment test; SGRQ: St George’s respiratory questionnaire; CCQ: clinical COPD questionnaire; mMRC: modified British medical research council.
Comparison of laboratory indicators
Table 2 shows a comparison of the laboratory indicators between the two groups. In the eosinophilic group, the absolute value and percentage of lymphocytes in peripheral blood and the percentage of lymphocytes in sputum were higher than those in the noneosinophilic group (P < 0.05). In the noneosinophilic group, the absolute value and percentage of neutrophils in peripheral blood and the percentage of neutrophils in sputum were higher than those in the eosinophilic group (P < 0.05), and the positive rate of sputum culture and biological indicators (NLR, CRP, PCT, FIB) was also higher than those in the eosinophilic group (P < 0.05).
Comparison of laboratory indicators.
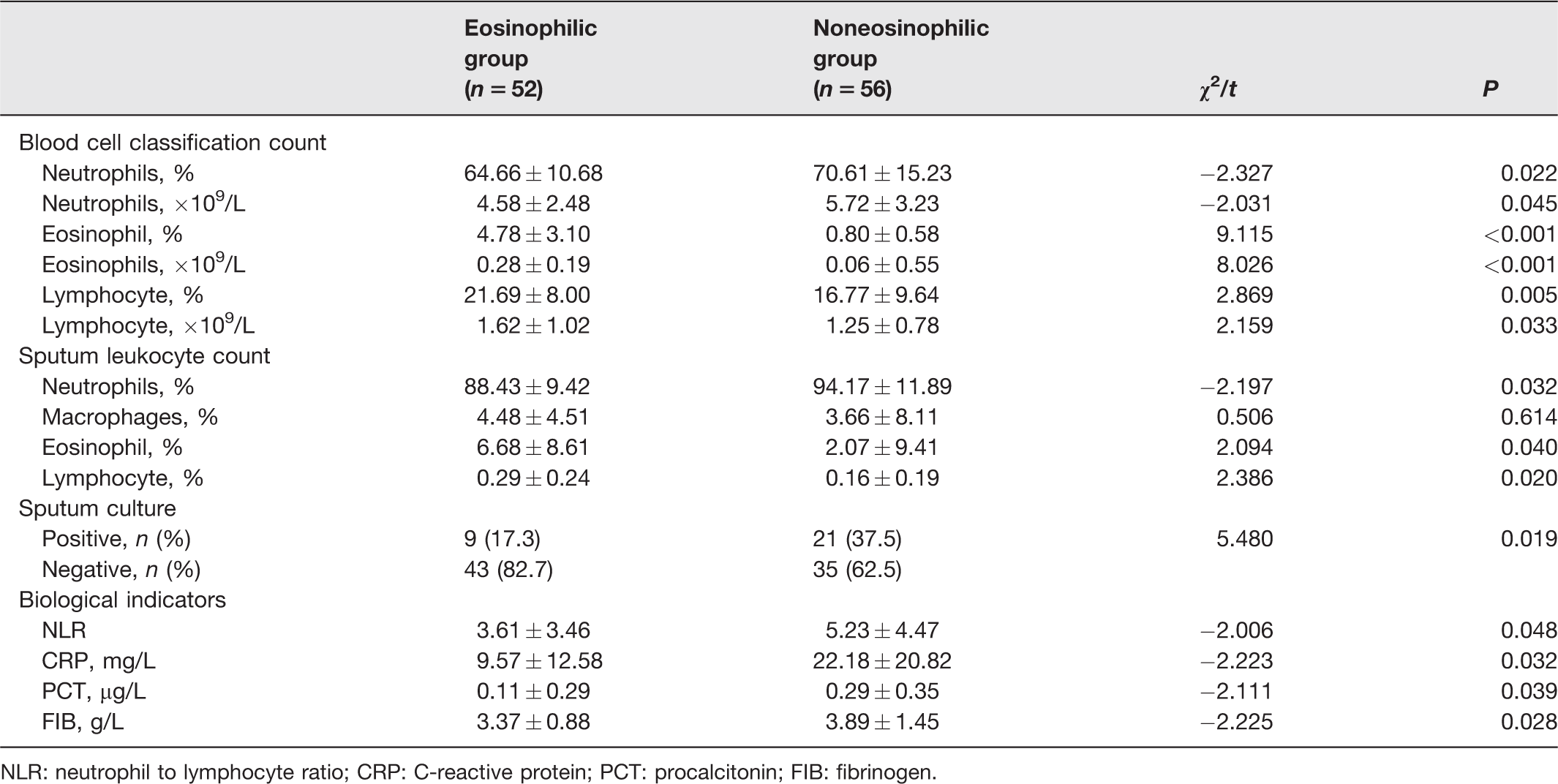
NLR: neutrophil to lymphocyte ratio; CRP: C-reactive protein; PCT: procalcitonin; FIB: fibrinogen.
Comparison of the levels of IL-13 and ECP in serum and sputum
The levels of IL-13 and ECP in sputum in the eosinophilic group were higher than those in the noneosinophilic group (P < 0.05), but there was no significant difference in serum between the two groups (P > 0.05) (Table 3). Moreover, the effect of genders on the levels of IL-13 and ECP was analyzed. As shown in Table 4, there were no significant difference on these two inflammatory factors between male and female.
Comparison of the levels of IL-13 and ECP in serum and sputum.
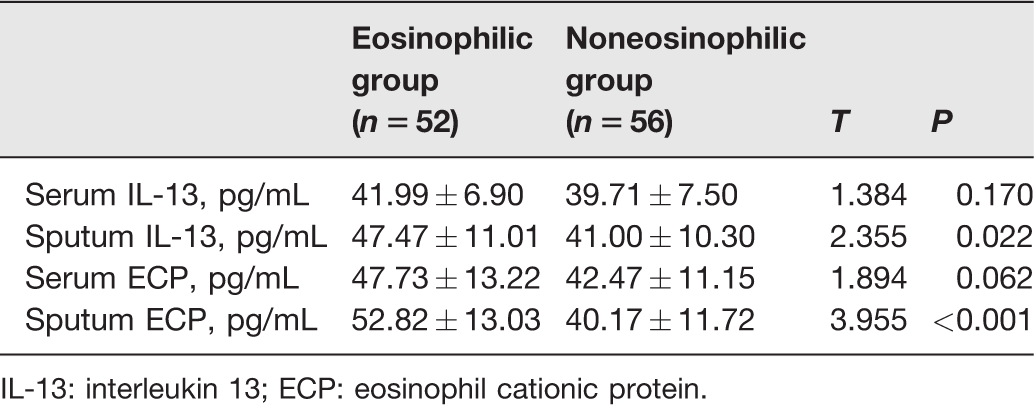
IL-13: interleukin 13; ECP: eosinophil cationic protein.
Comparison of the levels of IL-13, ECP in serum and sputum of different genders.

Correlation between peripheral blood EOS% and IL-13 and ECP in serum and sputum
There was no significant correlation between peripheral blood EOS% and serum levels of IL-13 and ECP (P > 0.05, Figure 1(a) and (c)), while peripheral blood EOS% was moderately positively correlated with sputum IL-13 (P < 0.001, Figure 1(b)) and strongly positively correlated with sputum ECP (P < 0.001, Figure 1(d)). In addition, there was no significant correlation between the serum levels of IL-13 and ECP (P > 0.05, Figure 1(e)), while the sputum IL-13 was positively correlated with sputum ECP (P < 0.05, Figure 1(f)).
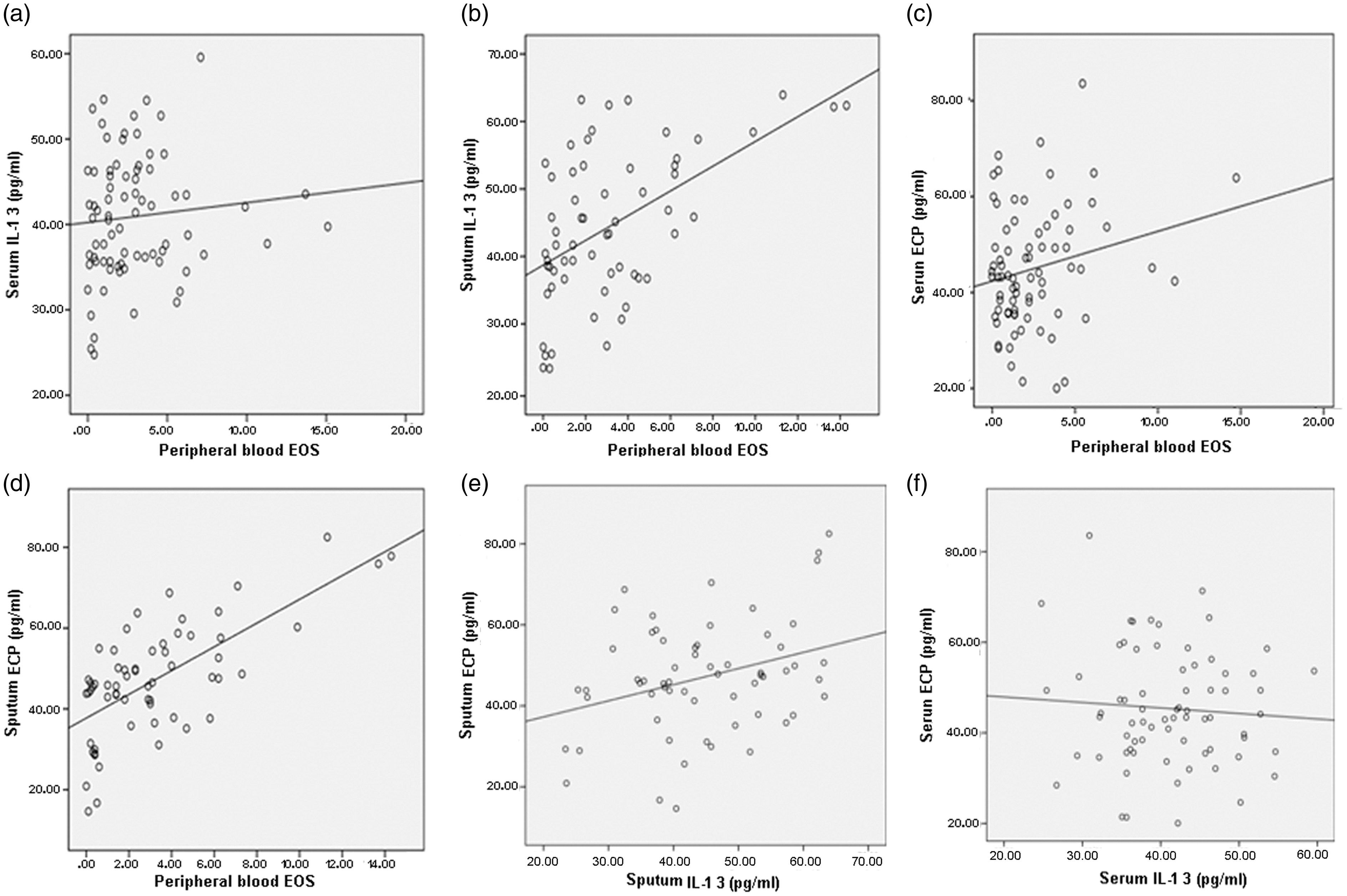
Correlation analysis. (a) Peripheral blood EOS% and serum IL-13 (r = 0.095, P = 0.415). (b) Peripheral blood EOS% and sputum IL-13 (r = 0.531, P < 0.001). (c) Peripheral blood EOS% and serum ECP (r = 0.218, P = 0.059). (d) Peripheral blood EOS% and sputum ECP (r = 0.680, P = 0.000). (e) Sputum IL-13 and sputum ECP (r=−0.071, P = 0.557). (f) Serum IL-13 and serum ECP (r = 0.318, P = 0.012).
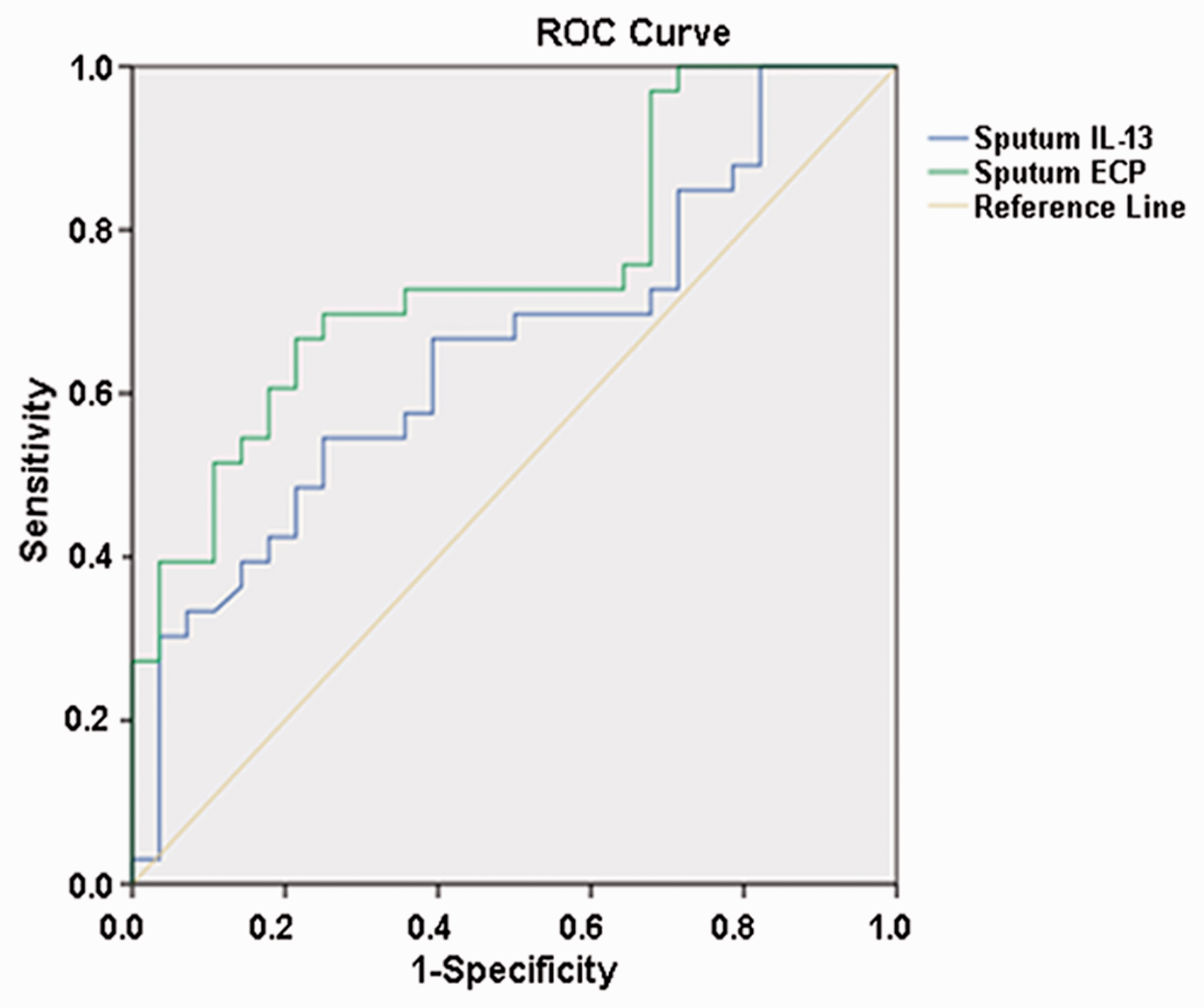
ROC curve of the peripheral blood EOS % ≥2% in inpatients with AECOPD by IL-13 and ECP in sputum. (A color version of this figure is available in the online journal.)
Analysis of the ROC curve of peripheral blood EOS % ≥2% of inpatients with AECOPD by IL-13 and ECP in sputum
The ROC curves of IL-13 and ECP in sputum predicting peripheral blood EOS % ≥2% of inpatients with AECOPD were statistically significant (P < 0.05), and the AUC values were 0.654 and 0.751. The Yoden index was the highest when the best cutoff value of sputum IL-13 was 42.45 pg/mL and sputum ECP was 46.49 pg/mL, the sensitivities were 66.7% and 69.7%, and the specificities were 60.7% and 75.0% (Table 5 and Figure 2).
Analysis of ROC curves of peripheral blood EOS % ≥2% in inpatients with AECOPD by IL-13 and ECP in sputum.

ROC: receiver operating characteristic; AUC: area under the curve; CI: confidence interval.
Comparison of the outcomes at follow-up one year after discharge
We followed-up the patients at one year after discharge by telephone, and seven patients were lost because they could not be contacted. The remaining 49 patients in the eosinophilic group and 48 in the noneosinophilic group were followed-up, and we found that the noneosinophilic group had a higher rate of rehospitalization due to acute exacerbation (P < 0.05), but there was no significant difference in mortality between the two groups (P < 0.05) (Table 6).
Comparison of the outcomes at the one-year follow-up after discharge by telephone.

Discussion
Chronic airway inflammation is one of the main pathogeneses of COPD. It is believed that the inflammatory cells involved in the inflammatory reaction mainly contain CD8+ T lymphocytes, neutrophils, and macrophages. In recent years, EOS has also been found to be involved in COPD airway inflammation. As early as 2006, scholars discovered EOS in 20%–40% of induced sputum specimens and large and small airway tissues of patients with stable COPD, and the increase in EOS in the airway was related to acute exacerbation. 9 The pathogenesis of COPD is heterogeneous and complex in terms of inflammation. In order to further explore the occurrence and development of COPD, it is of great clinical value to identify biomarkers that can be used to guide treatment, evaluate the condition, and predict prognosis.
Numerous studies have shown that peripheral blood EOS is associated with acute exacerbation of COPD and can be used to guide glucocorticoid therapy and predict the prognosis of the disease.10,11 Referring to the results of a large epidemiological survey, 12 we divided 108 inpatients with AECOPD into two groups according to peripheral blood EOS% with a cut-off value of 2%. It was found that the eosinophilic group accounted for 48%, and in this group, male sex was more common, acute exacerbations in the past year were less, the average hospital stay was shorter, the incidence of respiratory failure and the proportion of mechanical ventilation were lower, the symptom scores (CAT and mMRC) were lower, and the overall prognosis was better. These results are basically consistent with previous studies.13,14 Moreover, there was no significant difference in the pulmonary function test between the two groups. However, Bafadhel et al. 15 found that FEV1% and FEV1 in the EOS-positive group were lower than those in the EOS-negative group. This may be related to the fact that there are fewer patients in this study who have pulmonary function tests, and the representativeness was poor. At present, there are few studies on peripheral blood EOS and pulmonary function, and further study is needed to expand the sample size in the future.
The absolute value and percentage of peripheral blood neutrophils and the percentage of sputum neutrophils in the noneosinophilic group were higher than those in the eosinophilic group, and the positive rate of sputum culture and biological indicators such as NLR, CRP, PCT, and FIB was also higher. The NLR is the ratio of neutrophils to lymphocytes, which can reflect both inflammatory reactions and the immune system. Although it is easy to calculate from routine blood tests, it has not received widespread attention. In recent years, it has been found that the NLR can be used to judge the severity and prognosis of AECOPD. 16 CRP is an acute phase protein synthesized by the liver during inflammatory stimulation, such as bacterial infection. There is evidence that CRP can be used as an independent predictor of poor prognosis of AECOPD. 17 A Cox regression analysis demonstrated that an NLR ≥7 (P = 0.001) and CRP ≥19 mg/dL (P = 0.035) in the noneosinophilic group were negatively correlated with the survival rate at the six-month follow-up after discharge. 18 PCT is a protein that reflects systemic inflammation and is elevated when severe bacterial and fungal infections occur but does not increase when allergies and viral infections occur. A significant number of studies have confirmed that PCT can be used to evaluate the severity and prognosis of patients with AECOPD.19,20 FIB is a fibrinogen synthesized mainly by hepatocytes and secreted into the blood. It is expressed in hypoxia, airway inflammation, and tissue damage. It has also been proven to be an independent risk factor for predicting the decline in pulmonary function and frequent acute exacerbations in patients with AECOPD. 21 We discovered that the positive rate of sputum culture in the noneosinophilic group was significantly higher than that in the eosinophilic group, which may objectively reflect that bacterial infection in the noneosinophilic group may be more common than in the eosinophilic group. Therefore, it is further speculated that the pathogenesis of inpatients with eosinophilic AECOPD may be related to viral infection, air pollution, environmental deterioration, allergies, etc. The pathogenesis of inpatients with noneosinophilic AECOPD may be related to common bacterial infections, and the prognosis is relatively poor. Although these biological indicators have been shown to be related to the prognosis of hospitalized patients with eosinophilic AECOPD, there are currently no uniform evaluation criteria, and more studies are needed to delineate clear cut-off values.
At the one-year follow-up, the subjects in the eosinophilic group had a lower rate of rehospitalization due to acute exacerbation, which suggests that the prognosis of the eosinophilic group is more ideal. However, there was no significant difference in mortality between the two groups (P < 0.05). Bafadhel et al. 22 also proved the results. Nevertheless, Holland et al. 23 and Baldwin and Allen 24 reported that the length of hospital stay of patients with severe noneosinophilic COPD was significantly longer and that the mortality was significantly increased. The differences in the results of these studies may be related to the severity of the patient’s illness, compliance with treatment, follow-up time, follow-up method, medical level, economic conditions, and educational level. Compared with eosinophilic AECOPD, noneosinophilic AECOPD patients had more sputum and serum inflammatory cells (leukocytes and neutrophils) and higher levels of inflammatory mediators, lower lung function, longer recovery time and hospital stay, accompanied by more bacterial infection and response poor to standard therapies (steroid treatment). 4 In general, patients in the eosinophilic group have shorter hospital stays and better treatment of glucocorticoids, suggesting that eosinophils can guide the use of systemic glucocorticoids. This further illustrates that peripheral blood eosinophil levels can be used as a prognostic indicator for patients with COPD.
When acute exacerbation of COPD occurs, airway epithelial cells can release a variety of inflammatory cytokines. IL-4, IL-6, and IL-8 are correlated with the severity, and are associated with poor prognosis of AECOPD. There were higher levels of IL-4, IL-6, and IL-8 in serum or sputum from AECOPD than those from the control subjects. 25 However, IL-4 and IL-8 cannot judge the different type of AECOPD as biomarkers. Higher levels of sputum and serum IL-6 were observed in eosinophilic AECOPD than those in neutrophilic AECOPD. While IL-6 had variable statistical significance and caused different outcomes, the nondeterminacy of results limits its use as a biomarker for judging the severity of AECOPD in these populations. 26 In eosinophilic COPD, airway epithelial cells release cytokines (IL-33, IL-25, and thymic stromal lymphopoietin (TSLP)) which stimulate both naive T cells to differentiate into T helper 2 (Th2) cells and type 2 innate lymphoid cells (ILC2). Th2 cells and ILC2 cells then produce IL-5 and IL-13.25,27 IL-5 plays a central role in stimulating the growth, differentiation, and maturation of eosinophils in the bone marrow and also is implicated in the function and survival of eosinophils. 28 Clinical trials have shown that mepolizumab, which is a monoclonal antibody against IL-5, can reduce the exacerbation rate of COPD by inhibiting blood eosinophilia. 29
IL-13 was first recognized in human activated T lymphocyte clones in 1993. 30 It is a T cell-derived cytokine that regulates the functions of human monocytes and B cells. Punnonen et al. 31 found that it can directly induce B cells to produce IgE through the Th2 pathway, and its gene locus is on chromosome 5q23-31, which is close to the position of IL-4. At present, IL-13 is considered to be a multipotential Th2 proinflammatory cytokine that stimulates airway structural changes by regulating mononuclear macrophages, eosinophils, airway epithelial cells, and fibroblasts, thus participating in airway inflammation. Extensive studies have reported that IL-13 participates in the pathogenesis of COPD through a variety of mechanisms, mainly reflected in the following aspects: (1) inducing airway mucus hypersecretion; (2) participating in airway remodeling; (3) inducing airway hyperresponsiveness; (4) regulating the EOS inflammatory response; (5) stimulating airway epithelial fibrosis; and (6) modulating oxidative stress. 32 However, there are few studies on IL-13 in eosinophilic AECOPD, and its specific pathogenesis needs to be explored in the future. ECP is a cytotoxic ribonuclease produced and released by eosinophils which can be activated by IL-13. 33 In turn, ECP triggers the activation of STAT6 with elevated level of p-STAT6 which contributes to the function of IL-13 on promoting maturation into alternatively activated macrophages. 34 Therefore, there may be a IL-13 and ECP loop in some certain cells to regulate the function of IL-13 and ECP. ECP has been proven to be associated with many diseases. In recent years, it was found that ECP is highly expressed in patients with AECOPD and is related to the severity of the disease. 8
Our study illustrated that the levels of IL-13 and ECP in the sputum of the eosinophilic group were significantly higher than those of the noneosinophilic group, but there was no significant difference in serum between the two groups. Moreover, there was no significant correlation between the peripheral blood EOS % and serum levels of IL-13 and ECP, while the peripheral blood EOS % was moderately positively correlated with sputum IL-13 and strongly positively correlated with sputum ECP. Additionally, we also found that there was no correlation between the serum IL-13 and ECP, but the sputum IL-13 was positively correlated with sputum ECP. This may be due to the release of IL-13 and ECP after the increase in EOS levels in peripheral blood, which are partly absorbed into the blood and may thus be insufficient to significantly increase the concentration of IL-13 and ECP in peripheral blood. Alternatively, this study may not have been able to prove the difference between the two groups in serum IL-13 and ECP by grouping with 2% as the threshold. In the future, it is necessary to further explore the threshold values that can make serum IL-13 and ECP meaningful. Because there are many influencing factors in peripheral blood, sputum cytokines are directly secreted by airway cells, which can promote EOS recruitment to local airways and more accurately express EOS inflammation in patients with AECOPD. Similar to previous studies on asthma and chronic bronchitis, it is also believed that ECP in sputum is more likely to reflect eosinophilic-mediated inflammation than ECP in peripheral blood. 35 The ROC curve analysis further showed that IL-13 and ECP in sputum predicting peripheral blood EOS% ≥2% of inpatients with AECOPD were statistically significant, and the AUC values were 0.654 and 0.751. This finding indicated that sputum ECP could predict the prognosis of AECOPD more accurately than IL-13. This further reveals that IL-13 and ECP are involved in the pathogenesis of eosinophilic AECOPD, which may be the basis of new targeted anti-inflammatory therapy and an important direction for future research.
Traditionally, the treatment of COPD has been based on inhaled bronchodilators or in combination with glucocorticoids, which does not completely eliminate the damage from the inflammatory response to the airways. In theory, it can be reduced by inhibiting proinflammatory cytokines, which may have significant clinical implications for the prevention and treatment of COPD. In summary, IL-13 and ECP play an important role in the pathogenesis of eosinophilic AECOPD and may be targets for new anti-inflammatory therapies in the future. Whether these new therapies can benefit patients with eosinophilic AECOPD requires many clinical trials. In the future, we need to find more specific biomarkers to identify different inflammation phenotypes of AECOPD to achieve targeted treatment.
Footnotes
Authors’ contributions
All authors participated in the design, interpretation of the studies and analysis of the data and review of the manuscript; LT, LYH, QKR and WWT conducted the experiments, MHX, WYY and GL collected the serum and sputum samples, PM and WHL wrote the manuscript.
DECLARATION OF CONFLICTING INTERESTS
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
FUNDING
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Natural Science Fund of Shanxi Province (No. 201901D111186).